Phys · pharmacological
Salicylate Toxicity
Also known as Salicylate Toxicity · salicylate toxicity
Consultant-physician depth guide to Salicylate Toxicity for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Salicylate Toxicity is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
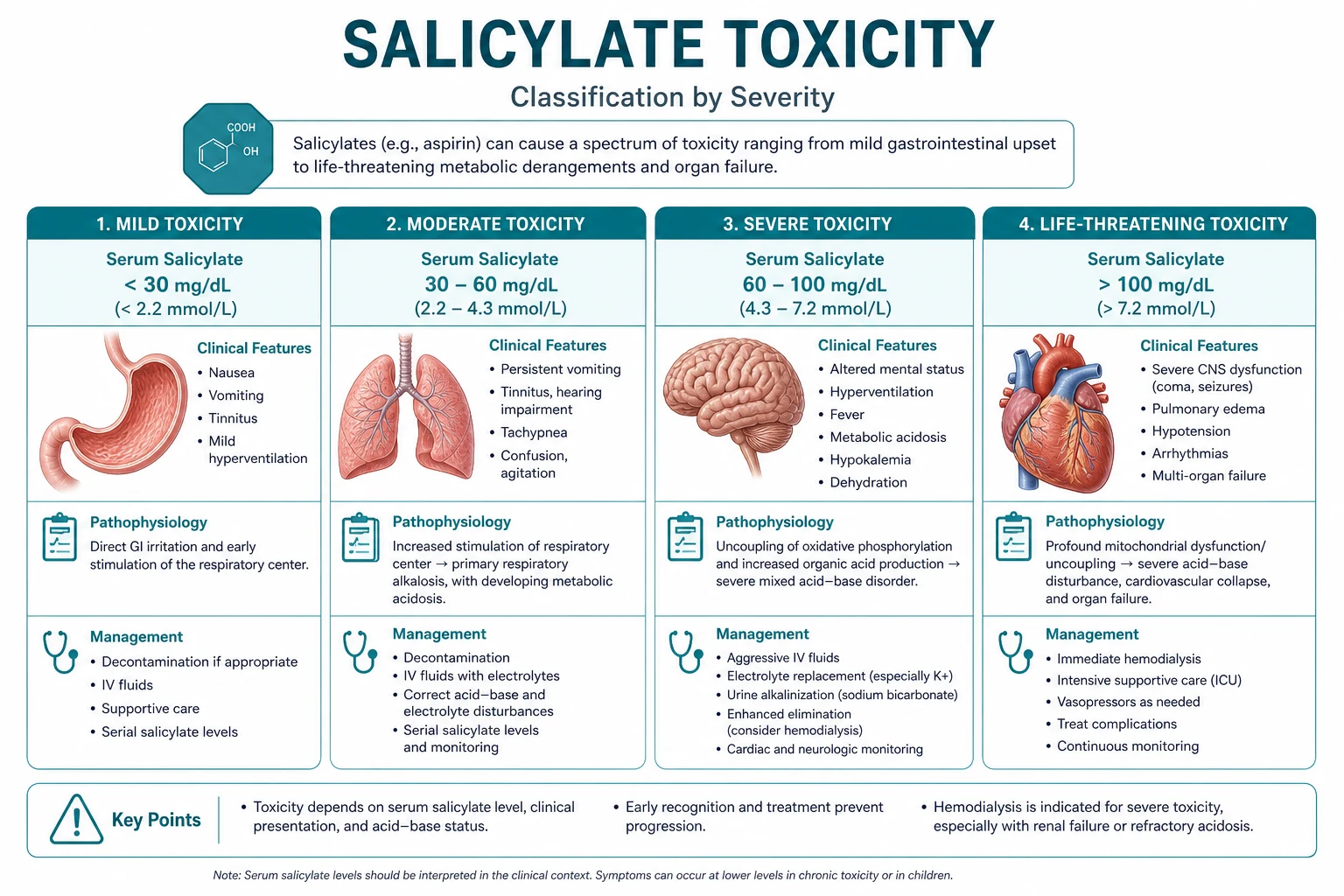
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
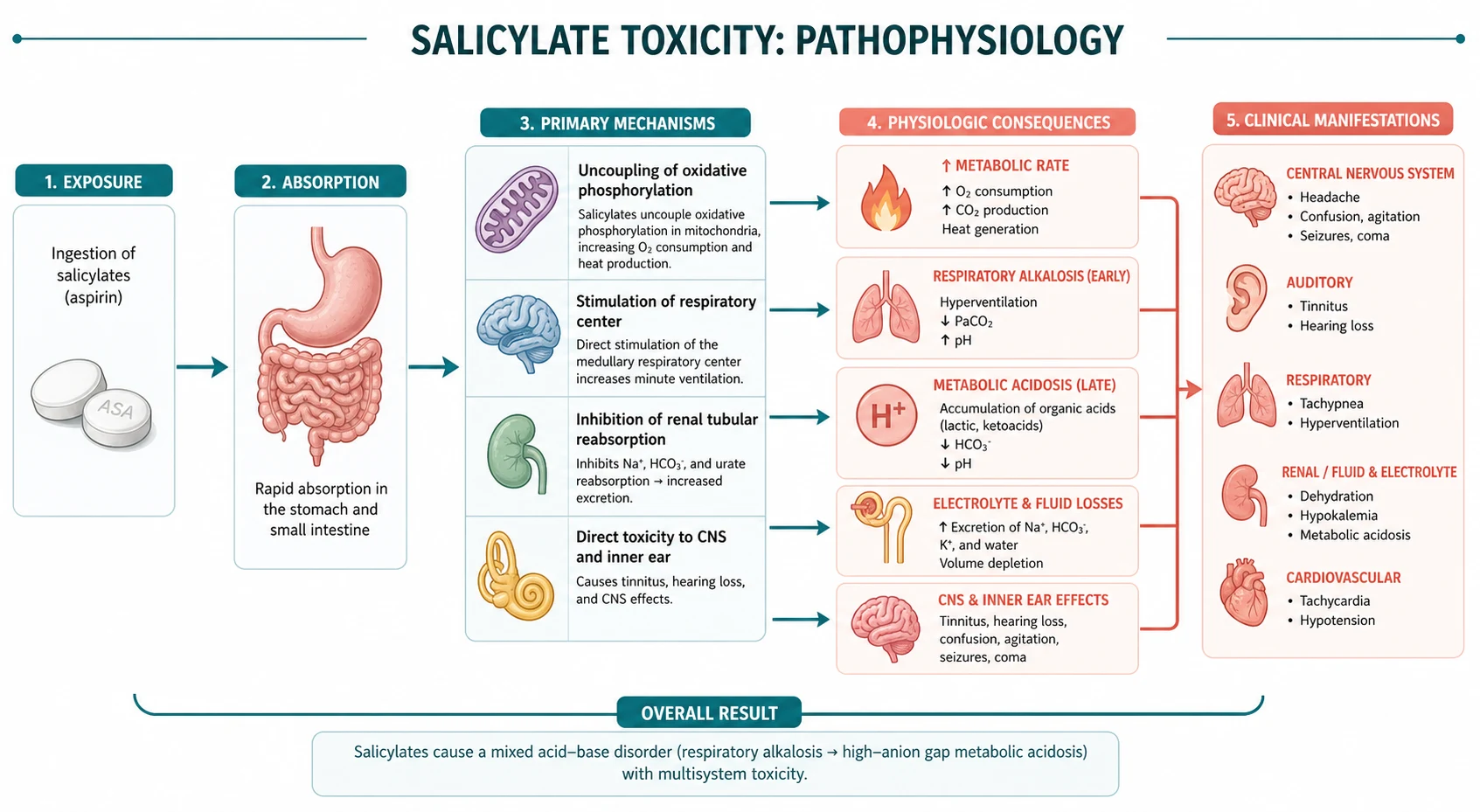
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
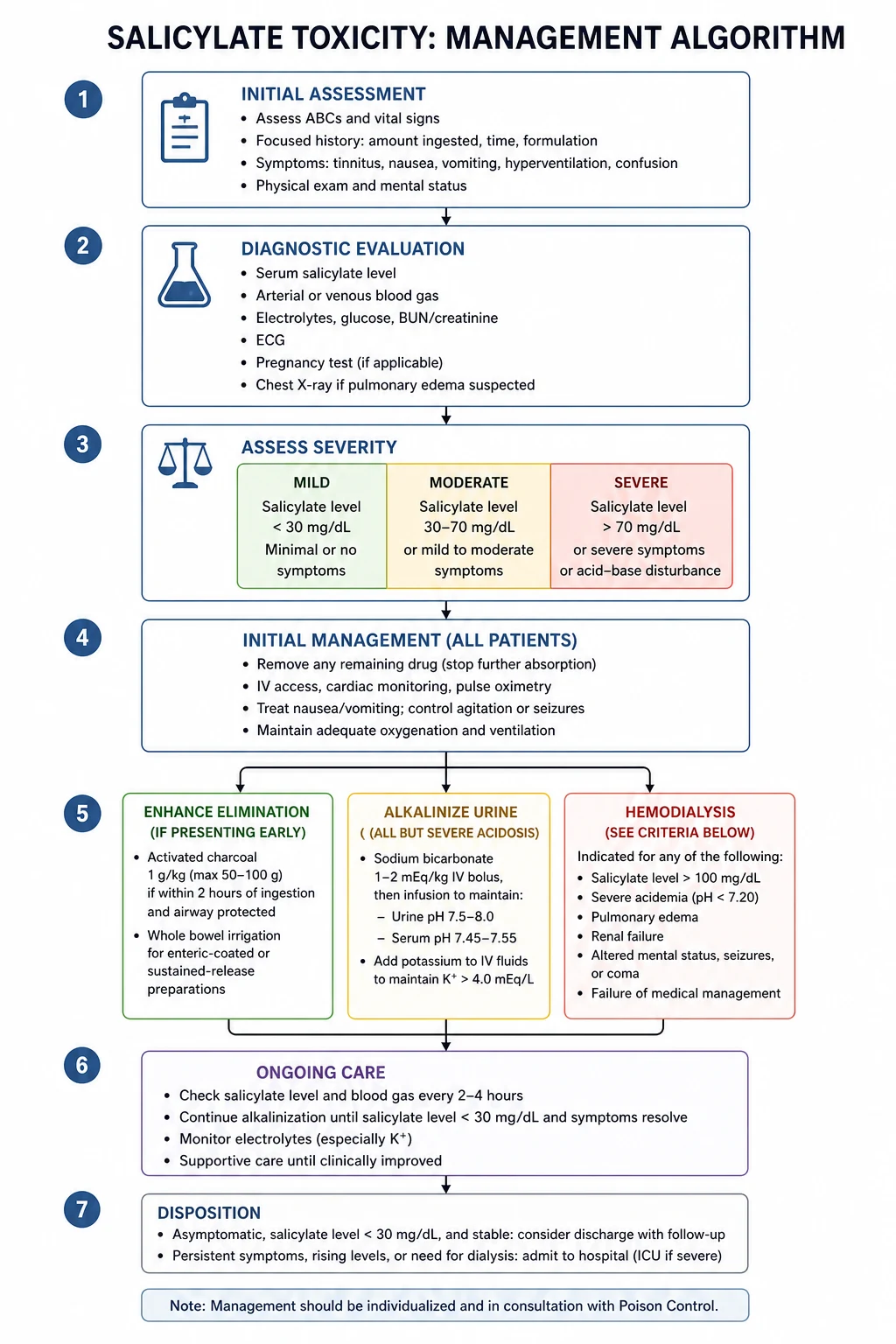
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Salicylate Toxicity to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Megaladevi P, Vadassery J Evolutionary trade-offs in plant immunity: prioritizing antiviral priming by herbivore-induced plant volatiles over defense against herbivores J Biosci, 2026.PMID 42345213
- [2]Palmer BF, Clegg DJ Pathophysiology of Ketoacidosis: Core Curriculum 2026 Am J Kidney Dis, 2026.PMID 42340294
- [3]Rather BA, Mir IR, Mahajan M, Qiao F, et al. Jasmonic acid crosstalk with secondary metabolites and plant growth regulators to maintain redox balance during crop improvement under salt stress Plant Sci, 2026.PMID 42314837
- [4]Hoegberg LCG, Gosselin S, Buckley NA, Wood DM, et al. Recommendations from the Clinical Toxicology Recommendations Collaborative on the administration of activated charcoal in acute oral overdose Clin Toxicol (Phila), 2026.PMID 41906697
- [5]Villanueva E, Carretero M, Aguirre MA, Negro A, et al. [Specific pharmacological treatment guide for transthyretin amyloid cardiomyopathy, 2021] Medicina (B Aires), 2022.PMID 35417392
- [6]Naito C, Yamaguchi T, Katsumi H, Kimura S, et al. Human Induced Pluripotent Stem Cell-Based Skin for Assessing Transdermal Drug Permeability and Irritancy Biol Pharm Bull, 2021.PMID 33390542
- [7]Doan HN, Chang MC Comparative Effectiveness of Unstable Versus Stable Resistance Training on Lower Limb Strength, Mobility, and Fear of Falling in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials Am J Phys Med Rehabil, 2026.PMID 42468010
- [8]Liu HW, Tsai TL Virtual Reality-assisted Physiotherapeutic Training for Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis Am J Phys Med Rehabil, 2026.PMID 42468005
- [9]Osborne AK, Brown RD, Sillence E Effects of Social Media Narratives on Affective and Behavioral Responses to Menopause Content: Randomized Online Experimental Study JMIR Form Res, 2026.PMID 42467962
- [10]Er MY, Karadayi G, Gulsahin Y, Karadayi M, et al. Mitigation of bensulfuron-methyl induced multiple stress responses in Cucumis sativus L. by biostimulants: A comprehensive metabolic and molecular docking approach J Hazard Mater, 2026.PMID 42430926
- [11]Alam NB, Batth R, Mohit AA, Lhamo C, et al. AtGLYI3 and AtGLYI6 play the major role in nickel stress tolerance in Arabidopsis thaliana Plant Cell Rep, 2026.PMID 42319536
- [12]Dai Y, Chen Z, Ren X, Wang S, et al. Salicylate esters inhibit human and rat 11β-Hydroxysteroid dehydrogenase type 2: Mechanistic insights from enzyme kinetics, SPR, and molecular modeling Toxicol Appl Pharmacol, 2026.PMID 42419492