EM · Burn management
Burn management in the emergency department
Also known as Thermal injury · Burn resuscitation · Inhalation injury · Scald
Burn management — the burn-depth classification (superficial, superficial dermal, deep dermal, full-thickness), the TBSA estimation by the rule of 9s and the Lund-Browder chart, the Parkland fluid-resuscitation formula (4 mL per kilogram per per cent TBSA of Ringer lactate in the first 24 hours), the inhalation-injury airway (early intubation), the escharotomy for the circumferential burn, the analgesia (morphine, ketamine), the referral criteria to a burns centre, and the electrical and the chemical burns. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The management of a major burn in the emergency department follows three priorities: the airway (the inhalation injury that closes the airway), the fluid resuscitation (the Parkland formula), and the wound (the depth, the extent, the circumferential compromise). The Fellowship candidate must estimate the depth and the extent at the bedside, start the fluid resuscitation from the time of the burn, intubate the patient with an inhalation injury before the oedema closes the airway, and know the referral criteria for the burns centre.[1][2]
Differential diagnosis — the burn-depth classification
The burn depth is classified clinically by the appearance, the sensation and the capillary refill, and it determines the healing potential and the surgical management. The Fellowship candidate must recognise each depth at the bedside.
[2]Superficial (erythema)
- Red, dry, painful (like a sunburn); no blisters
- NOT counted in the TBSA
- Heals in 3 to 5 days; no scar
- Simple analgesia and a moisturiser
Superficial dermal
- Pink, blistering, very painful; brisk capillary refill
- Counted in the TBSA
- Heals in 10 to 14 days (the adnexa survive)
- Dressings; may need fluid if >10% TBSA
Deep dermal
- Dark red or pale, slow capillary refill, less painful
- Counted in the TBSA
- Heals in 3 to 8 weeks; likely scar; may need a graft
- Referral to a burns centre; surgical assessment
Full-thickness
- White, black or leathery (eschar); dry, painless (nerve destroyed)
- Counted in the TBSA
- Will not heal (no adnexa survive); needs a graft
- Escharotomy if circumferential; surgical debridement
The TBSA estimation — the rule of 9s and the Lund-Browder chart
The contemporary ED approach to burn extent uses the rule of nines and related TBSA tools as a starting estimate, with awareness that crude rules are imperfect in obesity and extremes of body habitus.[4][5][8] Initial assessment and management principles follow current burn reviews.[1] Individualised fluid strategies refine historic Parkland one-size practice and adapted major-burn fluid approaches.[2][3] Smoke-inhalation cyanide care may include hydroxocobalamin when indicated, within broader trauma resuscitation frameworks.[6][7]
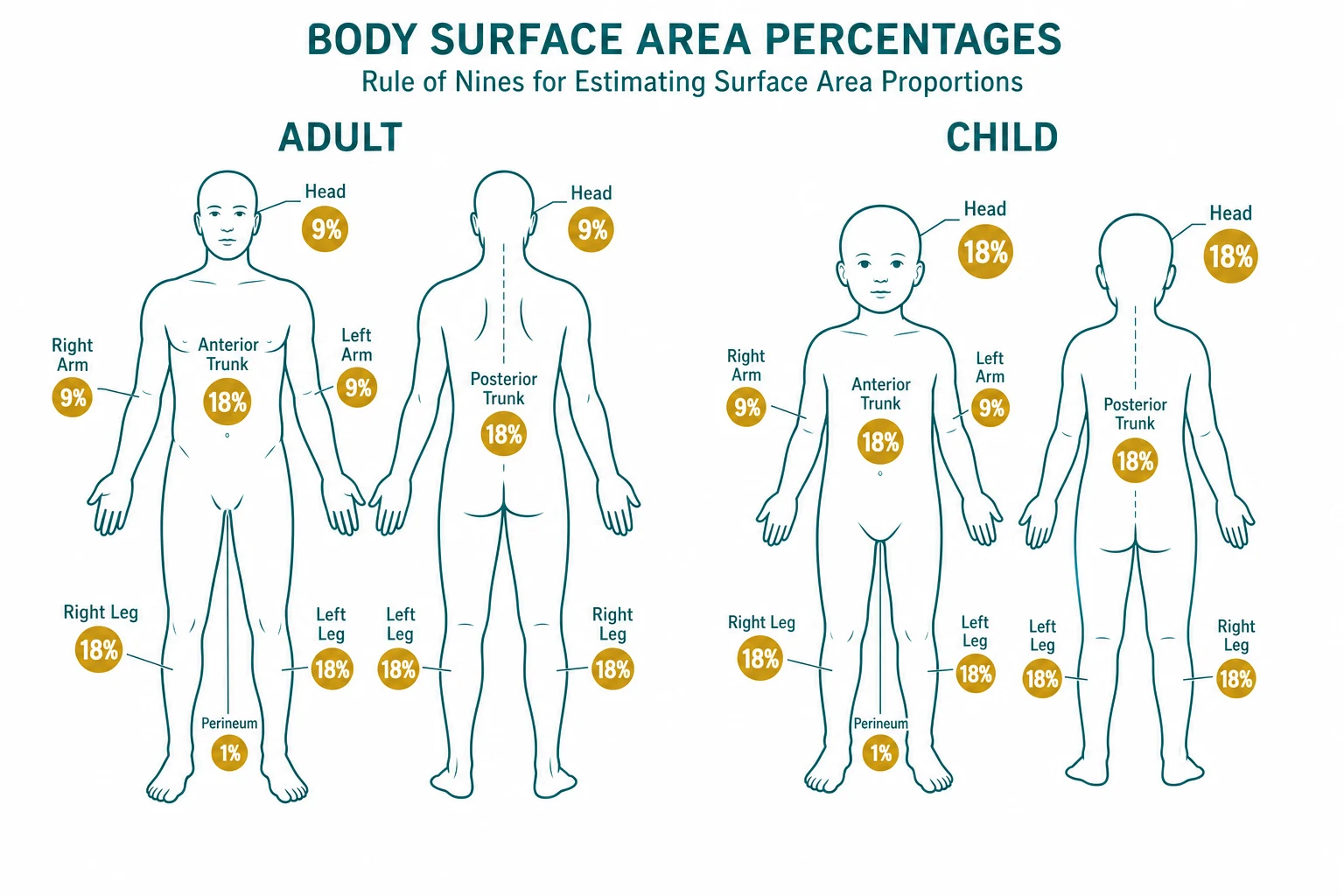
The total body surface area (the TBSA) is estimated to calculate the fluid resuscitation, and only the partial-thickness and the full-thickness burns are counted — the erythema (the first-degree) is excluded. The rule of 9s (the adult): the head and the neck 9 per cent, each upper limb 9 per cent, each lower limb 18 per cent, the anterior trunk 18 per cent, the posterior trunk 18 per cent, and the perineum 1 per cent (a total of 100). The Lund and Browder chart adjusts for the age and is used for the child (whose head is proportionally larger and the limbs smaller). The palm method (the patient's palm, including the fingers, is approximately 1 per cent of the TBSA) is the quick estimator for the small or the scattered burns. The accurate estimation is critical because it drives the fluid calculation, and a 5 per cent error in a 40 per cent burn changes the fluid volume by 800 mL in the first 24 hours.
[5]Rule of 9s (adult)
9s
9% (front 4.5 + back 4.5)
9% (front 4.5 + back 4.5)
18% (chest + abdomen)
18% (back)
18% (front 9 + back 9)
1%
The Parkland formula and the targets
The inhalation injury — the airway first
The inhalation injury is the first life-threatening complication of the burn, and it closes the airway faster than the fluid resuscitation can catch up. The signs are the history of an enclosed-space fire (the smoke, the heat, the toxic gases), the soot in the mouth or the pharynx, the singed nasal hairs, the hoarse voice, the carbonaceous sputum, and the stridor. The management is the early intubation (before the oedema closes the airway), with a low threshold — the window is narrow and narrows fast. The carbon monoxide poisoning (from the smoke inhalation) produces a confusion, a headache and a loss of consciousness; the treatment is the 100 per cent oxygen (which accelerates the carboxyhaemoglobin clearance) and, in the severe case, the hyperbaric oxygen. The cyanide poisoning (from the burning plastics) produces a lactataemia and a refractory shock; the treatment is the hydroxocobalamin.
[6]The fluid resuscitation — the Parkland formula
The fluid resuscitation is the core of the burn management, and the Parkland formula[2][3] is the starting point: 4 mL of Ringer lactate per kilogram per per cent of the TBSA, in the first 24 hours.[2] The first half is given in the first 8 hours from the time of the burn (not from the time of the arrival), and the second half over the next 16 hours. The fluid is titrated to a urine output of 0.5 mL per kilogram per hour in the adult (1 mL per kilogram per hour in the child), which is the most practical endpoint. The formula is a guide, not a rule — the actual fluid is adjusted to the urine output, the blood pressure and the clinical state, and the over-resuscitation (the "fluid creep") causes a pulmonary oedema and a compartment syndrome. The Modified Brooke formula (2 mL per kilogram per per cent) is the alternative for the lighter resuscitation, supported by the recent evidence that the lower volume reduces the complication rate without compromising the tissue perfusion.
Immediate management — the protocol
The management follows the trauma primary survey (the ABCDE), with the burn-specific additions.
[7] [1]The escharotomy — the circumferential burn
A circumferential full-thickness burn of a limb compromises the circulation (the inelastic eschar prevents the swelling, and the compartment pressure rises → a limb ischaemia), and a circumferential chest burn compromises the breathing. The escharotomy is the surgical incision through the full-thickness eschar (the incision is painless — the nerve endings are destroyed) to release the constriction. The limb escharotomy is a longitudinal incision along the lateral and the medial aspects of the limb; the chest escharotomy is along the anterior axillary lines and the subcostal line. A fasciotomy may be needed if the compartment pressure remains high after the escharotomy.
[2]Referral criteria to the burns centre
The referral criteria to a specialist burns centre (the ABA and the ANZBA criteria) include: a TBSA over 10 per cent in the adult (over 5 per cent in the child); any full-thickness burn over 5 per cent; the burns involving the face, the hands, the feet, the genitalia, the perineum or the major joints; the electrical burns (including the lightning); the chemical burns; the inhalation injury; the circumferential burns of the limbs or the chest; the burns in the high-risk patients (the elderly, the diabetic, the immunocompromised); and any burn with the associated trauma. The burns below these criteria are managed as an outpatient or a general-ward admission.
[3]The electrical and the chemical burns — the special cases
The electrical burn has a small surface injury and a deep tissue injury — the current passes through the body, damaging the muscle, the nerve and the vessel along its path. The management includes the ECG (the arrhythmia), the creatine kinase and the myoglobinuria (the rhabdomyolysis — treat with the intravenous fluids to a urine output of 1 to 1.5 mL per kg per hour, and consider the sodium bicarbonate for the myoglobin-induced AKI), the compartment-syndrome monitoring (a fasciotomy may be needed), and the cardiac monitoring for 24 hours (the delayed arrhythmia). The chemical burn is irrigated copiously with the water (for at least 20 minutes — the dilution is the solution), with the specific antidote for the specific agent (the calcium gluconate gel for the hydrofluoric acid). The tar burn is cooled with the water and the tar is removed with a lipid-based solvent (not by force).
[5]Complications and pitfalls
The complications are the airway obstruction from the inhalation injury, the hypovolaemic shock (the under-resuscitation), the compartment syndrome, the infection (the burn wound is a culture medium), the Curling ulcer (the stress ulcer of the severe burn — prophylaxis with a proton-pump inhibitor), and the hyperkalaemia (from the tissue destruction). The pitfalls are the inverse of the management: underestimating the inhalation injury (not intubating early); counting the erythema in the TBSA; starting the fluid clock from the arrival rather than the burn; the fluid creep (the over-resuscitation); not monitoring the urine output; not performing the escharotomy for the circumferential burn; and not referring to the burns centre for the criteria.
[2]Prognosis and disposition
The prognosis depends on the TBSA, the depth, the inhalation injury, the age and the comorbidity. The mortality rises steeply above 40 per cent TBSA in the adult. The patient is admitted to the burns centre or the general ward (by the criteria); the intubated and the fluid-resuscitated to the intensive care. The long-term outcome involves the scar management, the contracture prevention, the psychological support and the rehabilitation.
[6]Special populations
The child has a thinner skin (the scald burns deeper), a larger surface-area-to-mass ratio (the fluid loss is proportionally greater), and the TBSA estimation uses the Lund-Browder chart. The elderly have a thinner skin and more comorbidity. The pregnant patient's burn management is modified (the fetal monitoring, the higher fluid target). The diabetic patient has a higher infection risk and a slower healing. The anticoagulated patient has a higher bleeding risk with the escharotomy.
[5]Evidence and regional guidelines
Bedside assessment and initial management synthesise burn-assessment reviews and fluid-history evidence.[1][2]
The contemporary framework is the ISBI/ABA/ANZBA burns guidelines; the fluid resuscitation follows the Parkland or the Modified Brooke formula, titrated to the urine output.[2] The assessment and the initial management are summarised in the recent reviews.[1] The formula and the airway principles are global; the referral criteria and the dressing choices follow the local burns-centre pathway.
ANZ practice note. The Parkland formula (4 mL per kg per per cent TBSA) and the referral criteria follow the ANZBA guidelines via the local burns-centre pathway; the inhalation injury is intubated early, the fluid clock starts from the time of the burn, and the escharotomy is performed for the circumferential full-thickness burn of the limb or the chest.
[6]Burn depth — the dynamic clinical assessment
The burn depth is dynamic — a superficial burn can deepen over 48 to 72 hours through the progressive microvascular thrombosis, the oedema and the secondary infection, so the definitive depth is often only declared on the third day. The bedside assessment uses the appearance (the colour), the sensation (the pinprick), the capillary refill (the blanching), the adnexa (the surviving hair follicles) and the blistering.
[1] [1]Epidermal (1st degree)
- Erythema only; no blisters
- Painful (the nerves intact)
- Brisk capillary refill
- Heals 3–5 d; no scar
- NOT counted in TBSA
Superficial dermal (2a)
- Pink, blistering, moist
- Exquisitely painful
- Brisk capillary refill
- Heals 10–14 d; minimal scar
- Counted in TBSA
Deep dermal (2b)
- Pale, mottled, dry
- Reduced sensation
- Slow or absent refill
- Heals 3–8 wk; hypertrophic scar
- Often needs a graft
Full-thickness (3rd)
- White, black or leathery eschar
- Anaesthetic (nerves destroyed)
- No capillary refill
- Will NOT heal; needs a graft
- Escharotomy if circumferential
Sub-dermal (4th degree)
- Charred; muscle, tendon, bone exposed
- Anaesthetic
- No refill
- Surgical debridement; amputation possible
- High-voltage contact or prolonged flame
The Lund and Browder chart — the paediatric accuracy
The rule of 9s overestimates the head and underestimates the legs in the small child, in whom the head is up to 19 per cent of the TBSA in the newborn (falling to the adult 9 per cent by 10 years). The Lund and Browder chart apportions the percentages by the age band, and is the standard for any burn in a child under 16 years. The head loses 1 per cent per year of age (from 19 to 9), and each leg gains 0.5 per cent per year (from 13.5 to 18), while the arms, the trunk and the anterior thigh remain fixed.
[8]Lund-Browder paediatric adjustment
CHILD
Use the Lund-Browder chart, never the adult rule of 9s, in the child
Head 19% in the newborn, falls to 9% in the adult
Head loses 1% per year; legs gain 0.5% per year
Each leg 13.5% in the newborn, rises to 18% in the adult
Trace each burned region on the chart and sum the percentages
The Parkland formula — the worked example
Parkland worked example — 70 kg adult, 40% TBSA, burn 2 h ago
Calculate the total 24-hour volume
4 mL × 70 kg × 40 = 11 200 mL of Ringer lactate in the first 24 h.
Set the clock from the BURN
The burn was 2 h ago; only 6 h remain to give the first half.
First half
5 600 mL over the next 6 h = ~933 mL/h.
Second half
5 600 mL over the next 16 h = ~350 mL/h.
Titrate to the urine output
Target 0.5 mL/kg/h = 35 mL/h; up-rate if low, down-rate if high or the urine is rising with the oedema.
After 24 h
Switch to the maintenance fluid and start the colloid (the capillary leak has settled); initiate the enteral nutrition.
The fluid-resuscitation formulas compared
Parkland/Baxter
- 4 mL × kg × %TBSA in 24 h
- Crystalloid (Ringer lactate)
- Half in the first 8 h from the burn
- Most widely used starting point
- Risk of fluid creep
Modified Brooke
- 2 mL × kg × %TBSA in 24 h
- Crystalloid
- Less fluid → fewer complications
- Recommended for the modern resuscitation
- Titrate up if under-perfused
Brooke (original)
- 1.5 mL × kg × %TBSA in 24 h
- Crystalloid plus colloid
- Historical 1953 formula
- Superseded by the Modified Brooke
- Educational reference only
Evans/Muir
- Colloid-containing formulas
- Used in some UK and Japanese centres
- Colloid given early
- Higher cost and blood-product demand
- Not first-line
Rule of 10s
- %TBSA × 10 = initial rate (mL/h) for adults
- Add 100 mL/h for each 10 kg over 80 kg
- Used by the US military for the rapid estimate
- Titrated to the urine output
- Useful in the pre-hospital or the mass casualty
The inhalational injury — the workup and the grading
The inhalational injury has three mechanisms: the supraglottic thermal injury (the hot air, the steam — usually supraglottic because the upper airway is an efficient heat exchanger and the vocal cords shield the subglottis), the supraglottic and glottic oedema (developing over 6 to 24 h), and the toxic gas inhalation (the carbon monoxide, the cyanide, the hydrogen chloride from the burning plastics). The lower-airway injury (the chemical pneumonitis, the ARDS) develops over 24 to 72 hours.
[6]Inhalational injury workup
Recognise the risk
Enclosed-space fire, altered consciousness, soot in the mouth or the nose, singed nasal hairs, hoarse voice, carbonaceous sputum, stridor, facial burns, expiratory wheeze.
Intubate EARLY
A low threshold — the airway obstruction can be rapid and complete; use a smaller tube (the oedema); consider an awake fibre-optic intubation if the airway is difficult.
Bedside tests
Carboxyhaemoglobin level (for the carbon monoxide), the venous lactate (the cyanide surrogate), the arterial blood gas, the chest X-ray (often initially normal — the infiltrate develops over 24 to 72 h).
Bronchoscopy
Diagnostic — soot in the bronchial tree, mucosal erythema, blisters, ulceration; the gold standard for the lower-airway injury.
Treat the toxic gases
100% oxygen (the CO clearance half-life falls from 320 min on room air to 80 min on 100% oxygen at 1 atm); hydroxocobalamin 5 g IV for the cyanide; hyperbaric oxygen for the severe CO poisoning (loss of consciousness, neurological signs, COHb over 25%).
Carbon monoxide and cyanide — the smoke-gas comparison
Carbon monoxide (CO)
- Source: smouldering fire, faulty heater
- Affinity for Hb is 240× that of oxygen
- Lips and skin cherry-red (rare); headache, confusion, coma
- COHb over 25% severe; over 50% lethal
- Treat: 100% oxygen; hyperbaric if neuro signs or COHb over 25%
Cyanide (CN)
- Source: burning plastics, wool, polyurethane
- Inhibits cytochrome c oxidase → cellular hypoxia
- Refractory shock; venous oxygen high (the tissues cannot extract); rapid loss of consciousness
- Lactataemia over 10 mmol/L is the surrogate marker
- Treat: hydroxocobalamin 5 g IV (preferred); avoid the classic nitrite kit (hypotension and methaemoglobinaemia)
Hydrogen chloride
- Source: PVC and other chlorinated plastics
- Direct mucosal irritant → laryngospasm, bronchospasm, ARDS
- Causes a chemical pneumonitis
- Treat: bronchodilators, ventilation, supportive
- Less systemic toxicity than the CO or the cyanide
Escharotomy — the anatomical technique
Escharotomy technique
Indication
A circumferential (or near-circumferential) full-thickness burn of a limb, the chest or the abdomen with a compromised distal perfusion or ventilation.
Time
Performed in the ED or the burns unit; an emergency when the perfusion is lost or the breathing is compromised.
Anaesthesia
The full-thickness eschar is anaesthetic — the incision is performed without anaesthesia in the ED if urgent; the sedation and the analgesia are still given (the patient is in pain from the other burns).
Limb incisions
Mid-lateral and mid-medial longitudinal incisions through the full-thickness eschar down to the subcutaneous fat; extend across the joints to release the constricting bands.
Chest incisions
Bilateral anterior axillary line incisions joined by a transverse subcostal incision — the battery-box pattern — to release the chest wall and restore the ventilation.
Check the perfusion
Reassess the distal pulses, the capillary refill and the oximetry; if still compromised, a fasciotomy is performed.
Electrical burns — the voltage categories and the danger
The electrical injury is classified by the voltage: the low voltage (under 1000 V — a household mains burn, often an oral commissure burn in a child chewing a live lead), the high voltage (over 1000 V — a power-line or a railway-line injury, with the deep muscle damage, the compartment syndrome and the rhabdomyolysis), and the lightning (the mega-voltage, the brief but enormous current, the cardiac arrest, the fixed and dilated pupils that may be transient rather than a death sign).
[1]Low voltage (under 1000 V)
- Small, deep contact burn
- Local tissue injury
- Oral commissure burn in a child (chewing a lead)
- ECG and brief cardiac monitoring
- Local wound care; reconstruct the oral commissure later
High voltage (over 1000 V)
- Small entry/exit wounds; massive deep tissue injury
- Rhabdomyolysis, myoglobinuria, AKI
- Compartment syndrome — early fasciotomy
- Cardiac monitoring 24 h (delayed arrhythmia)
- Massive IV fluid; target urine 1–1.5 mL/kg/h
Lightning
- Brief, massive current — usually a flash-over
- Cardiac standstill (asystole) — prolonged CPR may restore the sinus
- Fixed dilated pupils NOT a death sign
- Lichtenberg figures (fern-like skin markings)
- Tympanic rupture, cataracts, lower-limb paralysis
Chemical burns — agent by agent
The chemical burn continues to injure until the agent is removed or neutralised. The copious water irrigation is the universal first step (at least 20 minutes; longer for the alkali — 1 to 2 hours), and the specific antidote is added for the specific agent. The dry powder is brushed off before the water (the water activates the powder of some agents — the metallic sodium, the phosphorus, the calcium oxide).
[1]Hydrofluoric acid (HF)
- Glass etching, rust removers, semiconductor industry
- Deep painful burns; the fluoride chelates calcium and magnesium → hypocalcaemia, ventricular fibrillation
- Antidote: calcium gluconate 2.5% gel (massaged in); intradermal or intra-arterial calcium gluconate for the deep burn
- Monitor the ECG and the ionised calcium; the systemic hypocalcaemia can be fatal
- Irrigate copiously FIRST, then the calcium gel
Alkali (NaOH, KOH, cement)
- Drain cleaners, oven cleaners, wet cement
- Liquefactive necrosis — penetrates DEEPER than the acid
- Irrigate for at least 1 to 2 hours (longer than the acid)
- No specific antidote; the debridement for the deep burn
- Wet-cement burns are often missed — the patient presents hours later
Sulphuric / hydrochloric acid
- Battery acid, industrial cleaners
- Coagulative necrosis — forms an eschar that limits the penetration
- Irrigate for at least 20 minutes
- No specific antidote; supportive
- Less deep than the alkali at the same concentration
White phosphorus
- Military, industrial, fireworks
- Ignites on the air contact — keeps burning
- Irrigate AND keep wet (the saline-soaked dressing); brush off the particles in the dark (they glow)
- Antidote: copper sulphate 1% (forms the black copper phosphide that does not ignite) — briefly, then wash off
- Systemic phosphorus poisoning — hepatic and renal failure
Tar / bitumen
- Road surfacing, roofing
- Hot sticky mass — burns AND encases the skin
- Cool with the water; do NOT peel by force
- Remove with a lipid-based solvent (the butter, the baby oil, the liquid paraffin)
- Reassess the depth after the tar is removed — the underlying burn is often deeper than it appears
Nutrition — the hypermetabolic burn
The severe burn (over 30 per cent TBSA) triggers a hypermetabolic response — the resting energy expenditure doubles, the muscle catabolism accelerates, and the patient loses up to 25 per cent of the body weight in three weeks without the nutritional support. The enteral nutrition is started early (within 12 to 24 hours — it protects the gut mucosa, reduces the bacterial translocation and the Curling ulcer).
[2]The Toronto formula — the calorie target
TORONTO
Energy = (25 × body weight in kg) + (40 × %TBSA) kcal/day
Titrate the nutrition to the nitrogen balance and the weight
Enteral preferred (gastric or jejunal); parenteral if the ileus
Start within 24 h — early feeding reduces the sepsis and the mortality
High protein — 1.5 to 2 g/kg/day; the burn is a protein-catabolic state
Zinc, vitamin C, vitamin A for the wound healing
Early excision and grafting reduces the metabolic load
Pain management — the burn ladder
The burn pain is severe and biphasic — the background pain (the continuous nociceptive input from the wound) and the procedural pain (the dressing changes, the debridement). The analgesia is layered.
[2] [7]Tetanus prophylaxis
The burn wound is a tetanus-prone wound — the necrotic tissue and the anaerobic environment favour the Clostridium tetani. The immunisation status is checked at the admission and the booster given as per the schedule.
[2] [2]The burn-wound infection and the sepsis
The burn wound is a culture medium — the protein-rich, the devitalised tissue, the impaired immunity of the major burn. The infection is the leading cause of the late mortality, and the signs are subtle: the fever (which is also a feature of the hypermetabolic state), the tachycardia, the ileus, the glucose intolerance, the disorientation, and the change in the wound appearance (the discoloration, the rapid eschar separation, the sub-eschar pus).
[7] [1]Hypothermia and the warming — the forgotten priority
The burn patient loses the thermoregulation (the skin is gone) and arrives cold; the wet dressings, the cold fluids and the exposure during the survey deepen the hypothermia, which worsens the coagulopathy (the trauma triad of death) and the mortality.
[7] [2]The associated trauma — do not miss the second injury
The burn is often associated with the other trauma — the blast injury (the tympanic rupture, the pneumothorax, the lung contusion), the fall during the escape (the long-bone and the spinal fracture), the crush injury (the compartment syndrome), and the assault. The primary survey is the ATLS ABCDE — the burn is addressed in the secondary survey unless it compromises the airway or the breathing.
[7] [7]The special populations — the high-yield pearls
[2] [2]Disposition and the criteria for the transfer
The patient is discharged from the ED if the TBSA is small (under 10 per cent), the depth is superficial or superficial dermal, the pain is controlled with the oral analgesia, the social circumstances are adequate (a responsible adult, a telephone, a return pathway), and the tetanus is updated. The admission to the general ward is for the moderate burn (10 to 20 per cent), the circumferential burn (for the observation), the pain that needs the IV opioid, and the social concern. The burns-centre transfer is for the criteria above; the ICU is for the inhalation injury, the shocked patient, and the over-40-per-cent TBSA.
[6]The evidence base — the trial cards
Baxter (Parkland) — the original fluid formula
Laboratory and clinical work; the basis of the Parkland formula
Key finding
4 mL Ringer lactate × kg × %TBSA in 24 h (half in the first 8 h) restored the intravascular volume
Modified Brooke — the lighter resuscitation
Observational cohort and the consensus revision
Key finding
2 mL × kg × %TBSA gave the equivalent resuscitation with fewer complications (the pulmonary oedema, the compartment syndrome) than the Parkland
Hydroxocobalamin for the smoke-inhalation cyanide
Prospective pre-hospital cohort, the Paris cyanide-antidote study
Key finding
Hydroxocobalamin 5 g IV given pre-hospital reduced the mortality versus the historical placebo
Cooling the acute burn — 20 minutes of running water
Observational and laboratory studies, the Bart's and the NSW cohorts
Key finding
Cooling with the running water (15–20 °C) for 20 minutes within 3 h of the burn reduced the depth, the pain, the healing time and the need for the graft
Exam practice
SAQ — Paediatric scald with TBSA calculation by the Lund-Browder chart
10 minutes · 10 marks
A 2-year-old boy (weight 12 kg) is brought to the emergency department 90 minutes after pulling a saucepan of boiling water from the stove, scalding his anterior trunk, the entire anterior surface of his right arm, and the anterior surface of his right thigh. The burned skin is blistering, moist, pink and exquisitely painful. He also has a patch of erythema on the left forearm. He is alert and tearful: HR 142, BP 92/58, RR 30, SpO2 98 per cent on room air, capillary refill 2 seconds, afebrile. Two large-bore cannulae have been sited by the paramedics.
SAQ — High-voltage electrical burn with rhabdomyolysis and compartment syndrome
10 minutes · 10 marks
A 30-year-old electrician (weight 80 kg) is brought to the emergency department 45 minutes after making contact with an 11,000-volt overhead power line. He was thrown from his ladder and was briefly unconscious but is now alert (GCS 15). He has a small charred entry wound on the right palm and a larger exit wound on the plantar surface of the left foot. He complains of severe deep pain and progressive tightness in the right forearm. The paramedics report his urine is dark brown and tea-coloured. On arrival: HR 108, BP 132/82, RR 22, SpO2 97 per cent on room air. ECG shows sinus tachycardia with non-specific ST-segment changes. Potassium 5.6 mmol/L, creatinine 95 \u00b5mol/L, CK 38,000 U/L, venous pH 7.30, lactate 3.2 mmol/L. The urine is positive for blood on dipstick but has no red cells on microscopy.
Exam pearls
- Airway first: the inhalation injury → early intubation (soot, stridor, enclosed-space fire).
- TBSA: only the partial and the full-thickness burns count (not the erythema).
- Parkland: 4 mL Ringer lactate × kg × %TBSA in 24 h; half in 8 h from the BURN (not the arrival).
- Urine target: 0.5 mL/kg/h (adult); 1 mL/kg/h (child).
- Escharotomy for the circumferential full-thickness burn (limb or chest).
- Electrical burn: small surface, deep tissue → ECG, CK, myoglobinuria, cardiac monitoring 24 h.
- Chemical burn: copious water irrigation for at least 20 minutes.
- Referral: TBSA >10% adult (>5% child), full-thickness >5%, face/hands/feet/genitalia, electrical, chemical, inhalation, circumferential.
Red flags
[6]References
- [1]Kiwan O, et al. What You Need to Know About: Assessment of Burns and Initial Management. Br J Hosp Med (Lond), 2025.PMID 41134176
- [2]Boehm D, et al. A History of Fluid Management-From "One Size Fits All" to an Individualized Fluid Therapy in Burn Resuscitation. Medicina (Kaunas), 2021.PMID 33672128
- [3]Hsiao KH, et al. Adapted approaches to initial fluid management of patients with major burns in resource-limited settings: A systematic review. Burns Open, 2024.PMID 39540031
- [4]Moore RA, et al. Rule of Nines. StatPearls, 2026.PMID 30020659
- [5]García-Ballesteros DI, et al. Evaluation and Optimization of the Wallace Rule of Nines for the Estimation of Total Body Surface Area in Obese and Nonobese Populations. J Emerg Med, 2023.PMID 37709577
- [6]Jin WY, et al. Evidence for Hydroxocobalamin in Cyanide Toxicity Caused by Smoke Inhalation: An Updated Systematic Review. Emerg Med Int, 2025.PMID 41497958
- [7]Rossaint R, et al. The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition. Crit Care, 2023.PMID 36859355
- [8]Williams RY, et al. Does the "rule of nines" apply to morbidly obese burn victims? J Burn Care Res, 2013.PMID 23702858