Paeds · adolescent-and-young-adult-medicine
Adolescent consultation, HEEADSSS assessment and confidentiality
Also known as HEEADSSS interview · Adolescent psychosocial assessment · HEADSS assessment · Confidential adolescent consultation · Triadic adolescent interview
A fellowship approach to running the adolescent consultation: youth-friendly setup, rapport, time alone, conditional confidentiality with its lawful limits, a full HEEADSSS psychosocial assessment with validated screens, same-visit action on positive screens, and red-flag interrupts across clinic, ED, inpatient and telehealth settings.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old walks in with a parent for a "school medical." The parent starts to answer every question. If you let that continue, you will hear about growth and school, and you will miss the things that can kill this young person — depression, substance use, unsafe sex, abuse. The adolescent consultation is the structured encounter that prevents that miss. [1] [3]
The HEEADSSS assessment is a psychosocial interview that walks through the domains most likely to harbour risk in this age group: home, education and employment, eating, activities, drugs, sexuality, suicide and mood, and safety. It grew out of the original HEADSS instrument described by Cohen in 1991, which covered home, education, activities, drugs, sexuality and suicide. The extra "E" and "S" (eating and safety) are later expansions that many clinicians now use routinely. [1] [10]
Confidentiality in this setting is almost always conditional (sometimes called qualified). You promise to keep what the young person tells you private — except where there is serious risk of harm to themselves or others, where there is abuse, or where the law requires you to act. This promise is what makes the rest of the interview work. If an adolescent believes their parents will hear everything, they simply do not tell you the dangerous things. [2] [4]
The reason this matters in one sentence: most adolescent death and serious illness is preventable, and it is preventable in the conversation you have in this room. Suicide, injury, substance-related harm, unintended pregnancy and sexually transmitted infection are driven by behaviour and risk that a structured, confidential consultation can surface and shift. [1] [4]
What the consultation does
Creates trust
Greet the young person first; set a joint agenda before anything clinical.
Opens disclosure
Time alone plus a confidentiality line lets sensitive topics surface.
Surfaces risk
HEEADSSS walks every domain so none is skipped by accident.
Acts on risk
Positive screens get same-visit assessment, not a filed referral.
Builds a plan
Agree the plan with the adolescent, then rejoin the parent.
Classification
Not every adolescent encounter is the same job. A planned preventive visit has time to do all eight HEEADSSS domains in order. An emergency department attendance does the same domains opportunistically, often with an electronic proforma. A hospital admission is a chance to screen a group known to carry high psychosocial risk, even when the admission diagnosis is medical. The frame changes; the domains do not. [11] [16]
The visit itself runs in three parts, and the order is not optional. You start shared — greeting the young person and parent together and setting an agenda. You move to private time alone for the confidential HEEADSSS. You finish shared — agreeing the plan with the young person first, then rejoining the parent. The confidentiality frame sits around the private middle, which is why the diagram below matters. [3] [15]
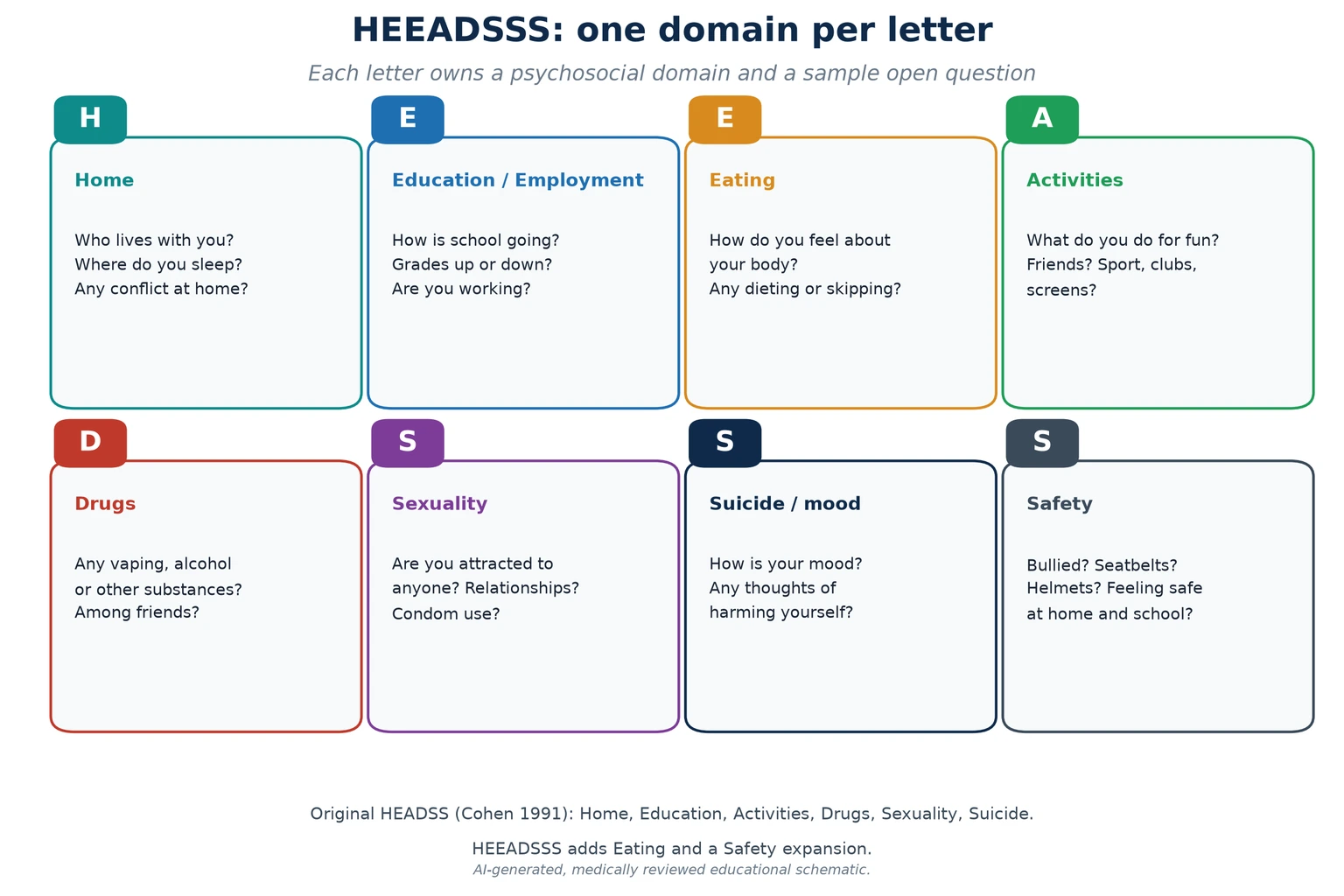
Read the figure like this: each letter is a doorway. If you skip a letter, you skip the doorway, and whatever is behind it stays hidden. The Suicide/mood and Safety letters are last in the acronym but first in safety — you can ask about them at any point if something earlier raises concern. [1] [10]
Shared start
Triadic
- Greet young person first
- Set a joint agenda
- Introduce private time as normal
- Keep it short
Private time
Dyadic, confidential
- Parent waits outside
- State confidentiality line
- Full HEEADSSS + screens
- Where the disclosure happens
Shared close
Plan with parent
- Agree plan with adolescent first
- Rejoin parent for shared plan
- Decide what stays confidential
- Set follow-up and safety-net
Red-flag interrupt
Any step
- Active suicidal intent
- Abuse or assault disclosure
- Medical instability
- Act first, resume later
The instrument also comes in different delivery formats. A skilled bedside interview is the reference standard. A paper or electronic proforma (sometimes written "e-HEEADSSS") standardises the domains, improves completion and documentation, and helps trainees who fear they will forget a letter. It does not replace rapport. An electronic tool in a busy emergency department can reach adolescents a clinician would otherwise miss — but it still needs a human to read the answers and act on them. [10] [11] [12]
Epidemiology & Risk Factors
The leading causes of adolescent death and disability in high-income countries are suicide, injury, substance-related harm, and the consequences of risky sexual behaviour. These are behaviour-driven, which means they are findable and shiftable in a conversation. A consultation that skips the conversation cannot shift them. [1] [5]
Time alone is achieved far less often than guidelines intend, and some adolescents almost never get it. Younger adolescents, boys, and those seen only for acute problems are least likely to have a confidential portion of the visit. When researchers ask young people directly, the gap between what is recommended and what is delivered is wide and consistent across countries. [3] [17]
Failure to state a confidentiality line has a measurable cost. When clinicians do not explain confidentiality, adolescents are less likely to disclose sexual activity, substance use and mental-health concerns. Parents often support time alone once it is explained well — but a meaningful minority are wary, which is why the script matters. [2] [8]
Hospitalised and emergency-attending adolescents carry more psychosocial risk than their presenting complaint suggests, and their screening is often missed. Inpatient HEEADSSS audits repeatedly show that most admitted adolescents are never screened, even though those who are often have positive findings that change the plan. [16] [12]
Who is missed
- Boys and younger teens
- Acute-only attendees
- Hospitalised with medical diagnosis
- Chronic-disease visits crowded by the medical agenda
System barriers
- No time alone built into booking
- Thin walls and shared waiting areas
- Portal and billing that expose sensitive notes
- No chaperone or interpreter pathway
Equity drivers
- Poverty and housing instability
- Out-of-home care and youth justice
- LGBTQ+ minority stress
- Refugee and migrant status
- Rural and remote settings
Family factors
- Parent wary of time alone
- Parent with their own agenda
- Family conflict or violence
- Same-language family interpreter used for sensitive topics
Pathophysiology
Two forces meet in the adolescent consultation, and both push the same way — toward risk that is real but hidden. [1]
The first is brain development. The reward and affect systems mature early in adolescence; the prefrontal systems that put the brakes on impulse mature later. This gap is real biology, and it shows up at the bedside as sensation-seeking, greater reward sensitivity, and a willingness to take a chance that an adult would not. It is also why a calm, non-judgemental counselling style works better than a lecture: you are working with a brain that is wired to feel the pull, not yet fully wired to resist it. [1]
The second is the confidentiality frame. If an adolescent believes that what they say will reach a parent, they stop talking about the things that carry the most shame and risk — sex, substances, mood, abuse. The mechanism is social and emotional, not a personality flaw. A parent in the room is enough to suppress disclosure even of unrelated topics, because the young person is editing everything they say for the audience present. [2] [4]
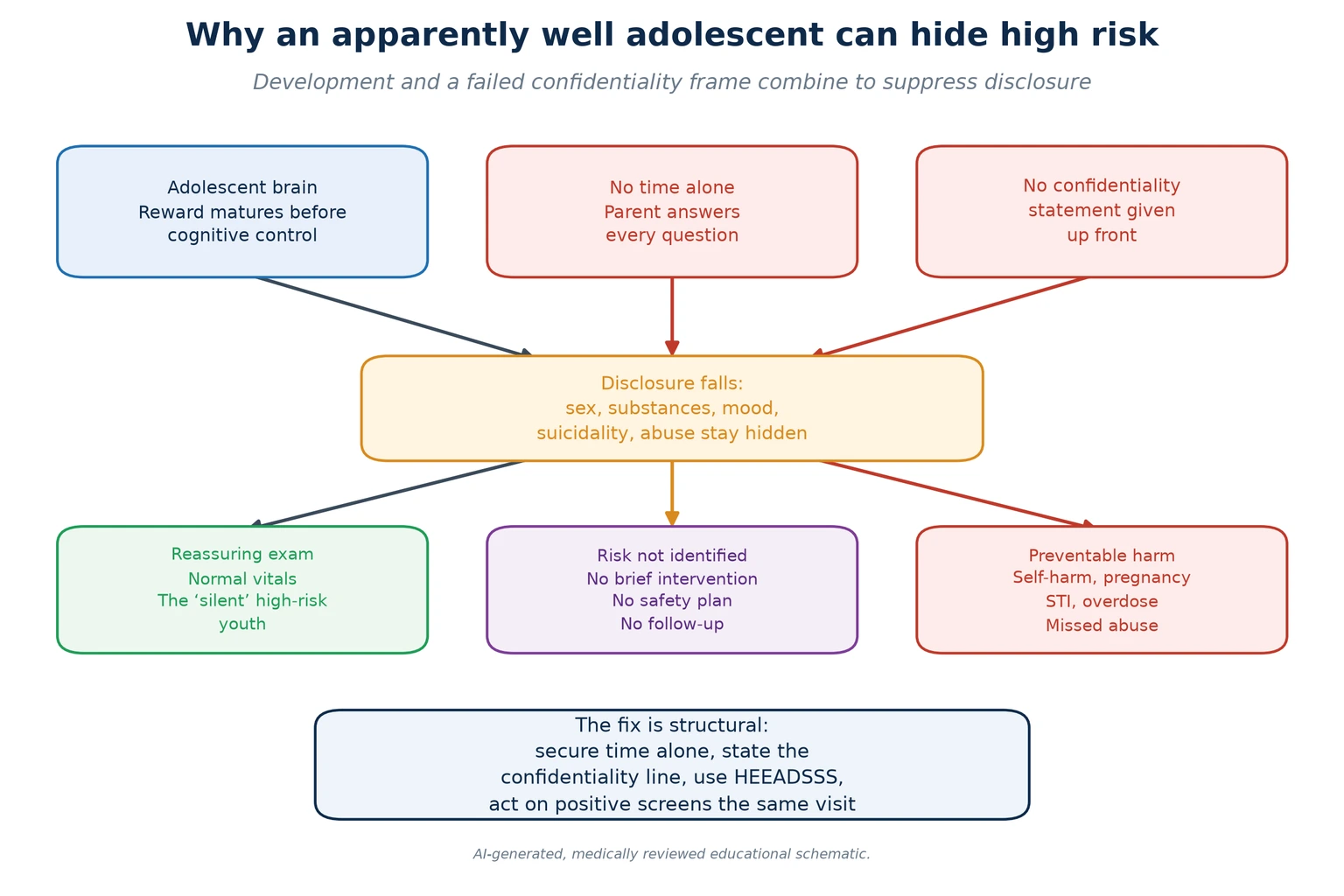
Read the figure like this: the dangerous adolescent often looks well. The physical exam and the vital signs will reassure you, and they will be wrong. That is why you cannot substitute the exam for the HEEADSSS. [16]
Trauma changes the calculation further. Adverse childhood experiences and ongoing family violence alter stress physiology and trust, so a young person who needs care most may be the hardest to engage. A heavy-handed or judgemental approach closes the door; a steady, predictable, confidential frame is the only thing that reopens it. [4]
The same logic applies to minority stress in gender-diverse and sexual-minority youth. The consultation has to be safe enough to hold identity questions without forcing them, while still screening the same domains as for any other adolescent. [4]
Clinical Presentation
A well-run adolescent consultation has a recognisable shape. You greet the young person by name, introduce yourself, and set the agenda together. You explain that some of the visit will be private and that this is normal. The parent leaves for the private part. You state your confidentiality line. You move through the HEEADSSS domains with open questions. You act on anything positive. You agree the plan with the young person, then bring the parent back for the shared plan. [3] [1]
A poorly-run consultation has a shape too, and you should learn to recognise it. The parent answers every question. You never create time alone. You never mention confidentiality. You ask a checklist of closed questions, get one-word answers, and conclude "all well." The dangerous problems were never raised, because you never built the conditions in which they could be. [2] [3]
High-risk problems rarely announce themselves as high-risk. They present as vague somatic complaints, a drop in school marks, a change in sleep, a new friend group, recurrent emergency attendance, or a parent who is worried but cannot say why. The HEEADSSS is how you turn those vague signals into findable risk. [16] [5]
A safeguarding problem may present as a controlling partner in the room, an unexplained injury, a fear of going home, or a reluctance to undress for examination. A failed transition presents at 17 to 19 years with no adult provider, a child-oriented record, and a young person who has dropped out of care. Each of these is a presentation the consultation is built to catch. [4] [7]
Differential Diagnosis
When an adolescent gives you a concerning answer, your first job is to decide whether it is normal development or a problem that needs action. The HEEADSSS does not diagnose; it raises flags that you then interpret. [1]
Separate normative mood variability from a depressive disorder. Every adolescent has bad days and swings. A depressive disorder is persistent low mood or anhedonia for at least two weeks with functional impairment — sleep, appetite, concentration, energy, worthlessness, and suicidality. The PHQ-A or PHQ-9 helps you distinguish them, but the screen is a prompt, not a verdict. [5]
Separate experimental substance use from a substance use disorder. Most adolescents who try alcohol or vaping do not have a disorder. The CRAFFT screen helps you tell the difference: recurrent use in hazardous situations, use to cope, or use despite problems moves the picture toward a disorder needing brief intervention or referral. [6]
Normal variant
Watch + revisit
- Mood swings without impairment
- Experimental single use
- Body-image questions without behaviours
- School anxiety without avoidance
Needs intervention
Brief intervention / referral
- Depression with functional impairment
- Hazardous or recurrent substance use
- Disordered eating behaviours
- Bullying-driven school anxiety
Needs urgent action
Same visit
- Suicidal intent or plan
- Active abuse or assault
- Medical instability (e.g. eating disorder)
- Acute intoxication or overdose
Separate normal body-image concern from an emerging eating disorder during the Eating domain. Concern about appearance is near-universal; behaviours such as skipping meals, vomiting, laxatives, and rapid weight change are not. Separate school anxiety driven by bullying or learning difficulty from school refusal driven by depression or abuse. The differential is not a list you memorise — it is the second question you ask after the first answer worries you. [1] [4]
One differential is easy to forget. A young person who refuses to talk about a topic may be exercising a normal boundary, or they may be protecting a dangerous secret. The way to tell is rapport and time: if you have built the frame, a "not yet" is usually a boundary; a panic at the topic is a reason to come back gently. [4]
Clinical & Bedside Assessment
This is the heart of the topic. The assessment is the intervention — done well, it changes what the young person tells you, what you find, and what you do next. [1]
Open the consultation. Greet the young person first, by name, before the parent. Introduce yourself. Set the agenda together: ask what they want from today, and add what you need to cover. Keep the shared start short. [3] [15]
Create time alone. Say plainly that part of the visit is between you and the young person, and that this is standard at their age. Give the parent a reason to step out — a waiting area, a questionnaire to complete, a clear time. If a parent says "we have no secrets," stay warm and firm: the private time is about the young person's growing independence, not about hiding things from the family. [3] [8]
State the confidentiality line. Say it out loud, early, and to both the young person and the parent. A working script: "What we talk about is between us. The main exception is if I am worried about your safety or someone else's safety, or if someone is hurting you — then I would need to get help, and I would talk with you about that first if I could." This is conditional confidentiality, and it is the engine of the whole interview. [2] [4]
Run the HEEADSSS. Move through each domain with one open, non-judgemental question, then follow the thread. Ask about Home (who they live with, where they sleep, conflict), Education or employment (how school is going, grades, work), Eating (body image, dieting, weight change), Activities (friends, sport, screens, fun), Drugs (vaping, alcohol, other substances, among friends), Sexuality (attraction, relationships, protection), Suicide and mood (mood, self-harm, thoughts of death), and Safety (bullying, seatbelts, helmets, feeling safe). Do not assume the gender of a partner, the young person's orientation, or that they are or are not sexually active. [1] [13]
HEEADSSS in order
Deploy validated screens when indicated. For depression, the PHQ-A or PHQ-9 is a brief, validated self-report that sits inside the Suicide/mood domain; the USPSTF recommends screening adolescents aged 12 to 18 years for depression (grade B). For substance use, CRAFFT is validated for adolescents and a positive result triggers further assessment and brief advice, not an automatic diagnosis. Use screens as prompts, then interpret them with the young person. [5] [6]
Assess suicide risk within the consultation. If mood or any answer raises concern, do not defer. Ask directly about ideation, plan, intent, access to means, prior attempts, protective factors, and whether the young person can stay safe tonight. Direct questions do not increase risk; they reduce it. The same-visit assessment is what separates a pass from a fail in an exam, and a safe plan from a tragedy in practice. [5] [4]
Examine with consent and respect. Explain what you will do and why, ask permission, offer a chaperone, and expose only what you need. A focussed examination — height, weight, body-mass index, blood pressure, pubertal stage if relevant, and any system the history points to — is usually enough in a preventive visit. The exam does not substitute for the HEEADSSS; it complements it. [1]
Document to protect, not to breach. Record enough to provide safe care without exposing sensitive detail to a parent through a portal or an itemised bill. Use your local sensitive-note workflow, and never use a same-language family member as an interpreter for sexual, substance or abuse disclosures. [9] [4]
Investigations
The "investigations" of the adolescent consultation are mostly the screens and the targeted tests that follow the history, not a blanket panel. [1]
Routine measures are height, weight, body-mass index and blood pressure, plus a pubertal assessment when relevant. These are screening observations, not diagnostics, and an abnormality sends you back to the history. [1]
Validated psychosocial screens act as investigations for hidden risk. The PHQ-A or PHQ-9 screens for depression (recommended for adolescents 12 to 18 years, grade B), the GAD-7 for anxiety, and CRAFFT for substance use. The HEEADSSS itself is the universal screen. A positive result is a finding that needs interpretation and action, not a label. [5] [6]
Targeted laboratory testing follows the history, never replaces it. Test for sexually transmitted infections when the history indicates risk — and let the young person know why, how specimens are taken, and how results will be kept confidential. Consider pregnancy testing, a full blood count or iron studies if menses are heavy, and thyroid tests if the picture suggests thyroid disease or an eating disorder. [13]
A urine drug screen has a narrow role. It is indicated only when the result will change management, and it carries real pitfalls — timing of use, false positives and false negatives, consent, and the confidentiality of the result. Do not order it reflexively, and never use it to punish. [6]
If somatic symptoms point more to anxiety or depression than to organic disease, your investigation is the psychosocial screen and a focussed work-up to exclude the dangerous mimics, not an open-ended battery. Positive screens that need action trigger the same-visit response described below. [5]
Management — Resuscitation
Some disclosures cannot wait for follow-up. They need action in the room, now. [4]
Positive depression or suicide-risk screen. Do not file and forget. The same-visit response is to assess suicide risk directly — ideation, plan, intent, means, prior attempts, protective factors, ability to stay safe. Then decide: a crisis or emergency pathway for high risk, or an early outpatient review with a written safety plan for lower risk. A referral to psychology that takes three weeks is not a safe plan for a young person with active intent. [5]
Active suicidal intent. If the young person discloses a plan and intent tonight, override confidentiality as needed to keep them safe. Tell them what must be shared and why. Secure immediate safety — do not leave them alone — and use your local crisis or emergency pathway. Share the minimum necessary with the people who can keep them safe, and preserve their dignity throughout. [4] [5]
Abuse, assault or family violence disclosed. This is a mandatory-action situation in most jurisdictions. Tell the young person what you must do and why. Follow your local safeguarding pathway, escalate to the team trained in child protection, and document carefully. Do not interrogate; do obtain enough to act, and hand over to the specialists. [4]
Medical instability from an eating disorder. If the Eating domain or the examination reveals an unstable picture — bradycardia, postural drop, hypothermia, severe weight loss, or electrolyte disturbance — this is a medical emergency that supersedes the rest of the visit. Stabilise, investigate, and escalate to a service that can refeed safely. The sibling topic on eating-disorder recognition covers this in depth. [1]
Confidentiality override in practice. When you must break confidentiality, say so explicitly: "I am worried about your safety, so I need to share this with [name] to get you help. I will tell you what I am doing and why." Share the minimum necessary. The goal is to keep the young person safe and preserve enough trust that they will come back to you next time. [2] [4]
Same-visit response to a positive screen
Assess
Suicide risk, abuse, instability — directly, now.
Decide
Crisis pathway versus early review with a safety plan.
Share
Override confidentiality only as needed; tell the young person why.
Secure
Do not leave a high-risk young person alone or unsupported.
Hand over
Warm hand-off to crisis, safeguarding or eating-disorder service.
Management — Definitive & Stepwise
Once the red flags are cleared, the consultation moves through a deliberate sequence. Treat it as a procedure with steps. [1]
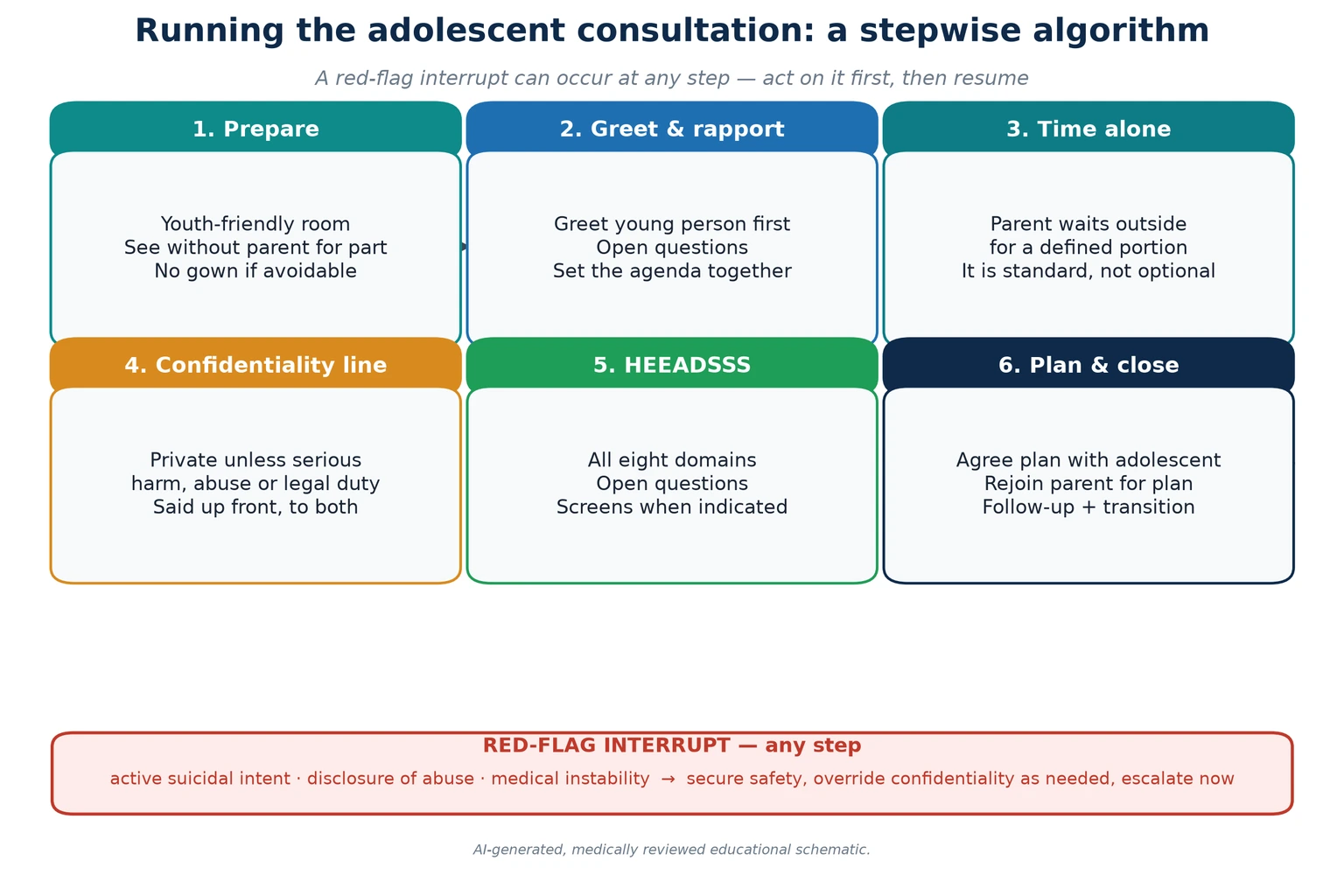
Prepare. Make the room youth-friendly: the young person clothed and seated, no gown unless needed, the door closed, and a plan for where the parent will wait. Preparation is not decoration; it is what makes private disclosure possible. [3]
Greet and build rapport. Address the young person first. Ask something that is not a medical question — school, a hobby, what they did today — before you move to sensitive territory. Rapport is not soft skill in this encounter; it is load-bearing. [3] [15]
Create time alone and state the confidentiality line as described above. These two steps are the hinge of the whole visit. [2] [4]
Run HEEADSSS and deploy screens. Walk every domain with an open question, follow the thread, and use validated screens when indicated. Note positive findings for the same-visit response. [1] [10]
Deliver brief intervention and motivational interviewing. When the screen or the history shows risk, a brief, non-judgemental intervention in the same visit is effective for substance use and other risk behaviour. Motivational interviewing meets the young person where they are, explores ambivalence, and supports their own reasons for change — which works far better than a lecture for an adolescent brain wired to feel the pull of reward. [6]
Make the plan with the young person first. Agree what will happen, who they will see, and when. Then rejoin the parent for the shared plan, deciding together what stays confidential. A plan the young person co-designed is a plan they are more likely to follow. [4]
Close well. Summarise, confirm understanding, give a written safety-net, and set a follow-up interval matched to the risk level. A warm hand-off — telling the next clinician or service directly, with the young person's knowledge — is more reliable than a letter that may never be read. [7]
The full sequence
1. Prepare
Youth-friendly room; plan for the parent.
2. Greet & rapport
Young person first; non-medical opener.
3. Time alone
Private portion is standard, not optional.
4. Confidentiality line
Conditional; stated up front, to both.
5. HEEADSSS + screens
Every domain; PHQ-A, GAD-7, CRAFFT as indicated.
6. Plan & close
Agree with adolescent, rejoin parent, follow-up.
For adolescents with chronic disease, the medical agenda will try to crowd out the psychosocial screen. Protect the HEEADSSS — chronic illness does not protect an adolescent from depression, substance use or unsafe sex, and sometimes it raises the risk. For late adolescents, fold transition preparation into this step: assess readiness, start building a portable summary, and plan the move to adult care as a staged process over years, not a birthday letter. [7]
Specific Subtypes & Scenarios
Younger adolescent (10–13) with a parent who expects to stay. Here the developmental task is emerging autonomy, and the parent's presence is developmentally normal at the start. Introduce private time as a small, age-appropriate step — even five minutes — and frame it as practice for growing independence. Keep the language concrete and the questions shorter. [15] [3]
Gender-diverse and sexual-minority adolescent. Run the same domains, without assuming the gender of partners or the young person's identity. Use the names and pronouns the young person uses. The Sexual Health domain is covered in detail in the sibling topic; here the point is that affirming, non-judgemental care is the precondition for honest answers across every domain, not only sexuality. [4] [13]
Out-of-home care and youth justice. Confidentiality lines are more complex because multiple adults hold legal interests in the young person. Be explicit about who will be told what, and why. These young people carry high rates of trauma and unmet need, and a steady, predictable frame is especially important. [4]
Hospitalised or emergency-attending adolescent. Treat the admission or attendance as an opportunity, not a detour. Hospitalised adolescents have high rates of psychosocial risk that is usually missed, and an opportunistic HEEADSSS — paper or electronic — can change the safety plan and the disposition even when the index diagnosis is medical. [16] [11]
An opportunistic inpatient HEEADSSS
Telehealth consultation. The same domains apply, with new safeguards. Confirm who else is in the room at each end, secure privacy at the young person's location (a parked car or a bedroom with the door closed), and agree how results and notes will reach them without breaching confidentiality through a shared portal. [9]
Adolescent with intellectual disability or neurodiversity. Adapt the interview to the young person's communication, use visual supports and concrete language, assess capacity issue-by-issue, and still screen every domain. Capacity to consent is specific to the decision at hand, not a global label. [14]
Migrant or refugee adolescent. Use a professional interpreter — never a family member — and a cultural broker when available. Explain the confidentiality frame in a way that honours culture, because the boundary between family and clinician is culturally loaded and must be navigated, not ignored. [4]
Complications & Pitfalls
The most damaging pitfall is the promise you cannot keep. If you say "this is completely between us" and then disclose to protect the young person, you have broken trust — and not only with that adolescent, but with every young person they tell. State the limits up front so that an override, when it comes, is not a betrayal. [2] [4]
The modern confidentiality breach usually arrives through a screen, not a conversation. The patient portal, the itemised bill, the pharmacy text, and the open note can all surface a sensitive consultation to a parent who holds the account. In the open-notes era this risk has grown, and it requires active management — sensitive-note workflows, confidential contact details, and billing codes that do not betray content. [9]
Skipping a domain to save time is a false economy. The Eating and Suicide domains are the ones most often dropped, and they are the ones that carry the most danger. A checklist HEEADSSS delivered without rapport produces false-negative disclosure: the boxes are ticked, but the answers are guarded and the risk stays hidden. [10] [16]
Filing a positive screen for delayed psychology review, without a same-visit risk assessment, is the single most common management error. The young person who needed action tonight instead waits three weeks, and the risk is realised in the gap. [5]
Other pitfalls: assuming the parent is a safe historian in a safeguarding case; using a same-language family member as interpreter for sensitive disclosures; reducing transition to a birthday referral letter; and lecturing instead of using motivational interviewing. Each of these closes a door that the consultation is meant to open. [4] [7]
Prognosis & Disposition
The adolescent consultation is not a single event; it is a relationship built over years. The disposition after one visit is almost always another visit, and the quality of the next one depends on the quality of this one. [3]
A confidential, respectful first encounter predicts better engagement and help-seeking over time. Adolescents who experience time alone and a clear confidentiality line are more likely to return, to disclose, and to accept care. Conversely, a breach — a broken promise, an exposed note — can push a young person out of care for years. [2] [9]
The follow-up interval matches the risk. A normal HEEADSSS with no positive screen may need only the next routine preventive visit. A positive screen that did not require the crisis pathway needs early review — often within one to two weeks — with a written safety plan and a clear escalation route. An acute safety concern needs same-day or next-day contact with a crisis service. [5] [4]
For late adolescents, disposition includes transition. Done well — prepare, transfer, integrate in the medical home over years — transition sustains the relationship into adult care and reduces drop-off. Done badly, it produces the 19-year-old with a chronic disease and no provider. [7]
Quality improvement turns the consultation into something you can measure and improve: time-alone rates, HEEADSSS completion, screen-to-follow-up intervals, and the proportion of positive screens that received a same-visit response. These are the metrics that distinguish a service that says it does adolescent care from one that does. [10] [11]
Special Populations
Gender-diverse and sexual-minority youth need the same domains screened in a frame that is affirming and safe. Minority stress raises the stakes of every domain, and a judgemental clinician closes the door permanently. Use the young person's names and pronouns, screen for depression and suicide risk that is elevated in this group, and offer the same confidentiality protections. [4] [13]
Adolescents in out-of-home care and youth justice carry high rates of trauma, mental-ill health and unmet need. Negotiate confidentiality and consent lines explicitly, because several adults may hold legal interests. Steady, predictable, trauma-informed care is the foundation. [4]
Migrant and refugee adolescents need a professional interpreter and cultural broker, never a family member for sensitive topics. Honour cultural meanings of family and confidentiality while still delivering the confidential frame. [4]
Adolescents with intellectual disability or neurodiversity need an adapted interview, concrete language and visual supports, with capacity assessed for each decision. They are screened for the same risks and often for additional ones, such as vulnerability to exploitation. [14]
Aboriginal, Torres Strait Islander, Māori and Indigenous adolescents need a culturally safe consultation that acknowledges the history and determinants shaping their health, and that is delivered in partnership with community-controlled services where possible. [4]
Rural and remote adolescents face thin services and thin privacy — everyone knows everyone. Telehealth, confidential contact details, and clear referral pathways become more important, not less. Adolescents experiencing homelessness or family violence need the consultation to address immediate safety and shelter alongside the usual domains. Pregnant and parenting adolescents need the visit adapted to their developmental stage and their new responsibilities. [4] [9]
Evidence, Guidelines & Regional Differences
The evidence base is mature at the level of the instrument and the principle, and it continues to evolve at the level of delivery and the electronic record. [1]
The HEADSS instrument (Cohen, 1991) gave the field its structure, and the HEEADSSS expansion (adding Eating and Safety) is now the common clinical form taught across training programmes. Studies of paper and electronic proformas — including "HEEADSSS Up," the e-HEEADSSS in a paediatric emergency department, and implementation studies in hospital settings — show that a structured tool improves completion and documentation of the domains, without replacing the value of a skilled interview. [1] [10] [11] [12]
On confidentiality, the AAP/SAHM policy line is consistent and was reaffirmed in the 2024 policy statement: confidential care supports adolescent health, and clinicians should deliver it while respecting the limits set by serious harm, abuse and law. The evidence that a stated confidentiality line increases disclosure is long-standing. [2] [4]
For screening, the USPSTF 2022 statement recommends screening adolescents aged 12 to 18 years for depression (grade B) and notes the co-occurrence of suicide risk. CRAFFT (Knight, 2002) is validated for adolescent substance use, and brief behavioural counselling in primary care has evidence of benefit. [5] [6]
[4] [9] [14]A live controversy is the tension between open-notes transparency for families and the adolescent's right to confidential care. The 21st Century Cures Act, by mandating patient access to notes, can inadvertently expose sensitive adolescent visits through a parent-held account — which is why sensitive-note workflows and confidential contact details now matter operationally, not just ethically. [9]
Controversies over parental notification for contraception, mental health and abortion in minors differ by jurisdiction, and the safe rule for a clinician — and a candidate — is to name the principle (confidential care, with limits for serious harm, abuse and law) and to defer the operational detail to local statute. The capacity to consent is assessed issue-by-issue, and a 2026 systematic review of decision-making capacity tools in minors underlines that no single instrument has displaced careful clinical judgement. [14]
Exam Pearls
The communication station is where this topic is most often examined, and the trap is to recite the letters without demonstrating the frame. Examiners want to see you greet the young person first, negotiate time alone with a resistant parent, state the confidentiality line unprompted, ask one open question per domain, and then — crucially — do something with a positive answer in the room. A candidate who ticks every box but files the positive screen for later fails. [3] [5]
In the long case, expect a chronic-disease adolescent whose psychosocial risk has been neglected because the medical agenda crowded it out. Your job is to show you would protect the HEEADSSS, manage the confidentiality and transition issues, and coordinate care across the medical home and adult services. [7]
In the structured oral, be ready for a branching scenario that moves from a normal visit to a suicide disclosure to an abuse disclosure in a few minutes. The skill is to hold the frame — time alone, confidentiality line, structured assessment, same-visit action — while the stakes rise, and to state plainly when you would override confidentiality and why. [4] [5]
References
- [1]Cohen E HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1991.PMID 1772892
- [2]Ford CA Delivery of confidentiality assurances to adolescents by primary care physicians. Archives of pediatrics & adolescent medicine, 1997.PMID 9158445
- [3]Miller VA Adolescents Spending Time Alone With Pediatricians During Routine Visits: Perspectives of Parents in a Primary Care Clinic. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2018.PMID 29887486
- [4]Chung RJ Confidentiality in the Care of Adolescents: Policy Statement. Pediatrics, 2024.PMID 38646690
- [5]US Preventive Services Task Force Screening for Depression and Suicide Risk in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2022.PMID 36219440
- [6]Knight JR Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of pediatrics & adolescent medicine, 2002.PMID 12038895
- [7]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [8]McKay EA Parents' Perspectives on Confidentiality in Clinical Preventive Services for Adolescents. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2025.PMID 40580168
- [9]Pasternak RH 21st Century Cures Act ONC Rule: Implications for Adolescent Care and Confidentiality Protections. Pediatrics, 2023.PMID 37010402
- [10]Smyth M HEEADSSS Up: Evaluating the Efficacy of a Blank Proforma in the Use and Documentation of an Adolescent Psychosocial Risk Assessment Tool. Adolescent health, medicine and therapeutics, 2024.PMID 41030311
- [11]Wong JW Implementing the electronic HEEADSSS screening tool in a paediatric emergency department. Emergency medicine Australasia : EMJ, 2024.PMID 39327905
- [12]Waller D Psychosocial assessment of adolescents and young adults in paediatric hospital settings: patient and staff perspectives on implementation of the e-HEEADSSS. BMC health services research, 2023.PMID 37349759
- [13]Barrett C Adolescent Sexual Health: A Focus on the Sexual Health Portion of HEADSS Examination. Pediatrics in review, 2025.PMID 40306707
- [14]Adu-Gallant C Evaluation of tools to assess decision-making capacity in minor adolescents in clinical settings: a systematic review with narrative synthesis. BMC medical ethics, 2026.PMID 42363197
- [15]Katzman CL Adolescent Time Alone With a Provider: Adolescent-Mother Dyads' Perspectives on Its Role to Support Emerging Autonomy. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2025.PMID 40838902
- [16]Addison J HEADSS Up! Missed Opportunity for Psychosocial Screening in Hospitalized Adolescents. Hospital pediatrics, 2021.PMID 33789962
- [17]Klein JD Time Alone During Health Visits for Adolescents and Young Adults: Secondary Analysis of a Nonrepresentative Global Youth Consultation. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2026.PMID 42429696