Paeds · adolescent-and-young-adult-medicine
Obesity and body-image concerns in adolescents
Also known as Adolescent obesity · Teenage overweight and obesity · Body image disturbance in adolescence · Weight-related distress · Disordered eating in higher-weight adolescents · Paediatric metabolic syndrome · Severe obesity in adolescence
A fellowship approach to adolescent obesity and body-image concerns: BMI-based classification with adult crossover, multifactorial aetiology, comorbidity screening, staged and weight-neutral lifestyle-to-surgery management, and concurrent mental-health and body-image care that refuses to reduce a young person to a number on the scale.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A 15-year-old walks into your clinic. Her BMI plots above the 97th percentile, her mother is anxious, and she will not make eye contact. Three things are true at once, and a good clinician holds all of them: she has a chronic metabolic disease that can be staged and treated, she carries a psychological burden that may dwarf the physical one, and the words you choose in the next ten minutes will either build trust or shut it down. This page teaches you to hold all three — to classify, screen for comorbidity, screen for distress, and deliver staged care that refuses to reduce her to a weight. [1] [8]
Overview & Definition
Obesity in adolescence is best understood first as a patient, then as a number. The young person in front of you has a chronic, relapsing disease of excess adiposity in which biological, behavioural, psychosocial and environmental forces have pushed energy balance toward sustained fat storage. The 2023 American Academy of Pediatrics Clinical Practice Guideline reframes it this way deliberately, to move the conversation away from blame and toward long-term, treatable disease. [1]
Clinically you define the physical dimension with body mass index plotted against age and sex on a growth reference. Obesity is a BMI at or above the 95th percentile for age and sex from ages 2 through 19, and severe obesity carries stricter thresholds that change management. The Endocrine Society guideline sits alongside the AAP framework and gives the same percentile-based definition. [1] [2]
Running alongside the physical disease is a psychological dimension — body-image concern. This is the gap between the body a young person perceives and the body they feel they ought to have, amplified by peers, family, media and clinicians. Body-image concern ranges from a healthy, accepting relationship with one's body through mild dissatisfaction to clinically significant disordered eating. Crucially, distress does not map neatly onto BMI: a young person in a larger body can feel fine, and a young person in a slim body can be devastated. [8] [11]
The headline numbers matter, but they exist to orient you, not to summarise a person. The tracking figure tells you why adolescence is a strategic window: intervention here changes the adult trajectory. [5] [8]
Classification
Classification answers two questions at once: how heavy is the body, and how heavy is the psychological burden? You need both, because they do not predict each other. [1] [2]
These tiers come from the CDC and WHO growth references for ages 2 to 19 and are reproduced in both the AAP and Endocrine Society guidance. [1] [2] [7]
The severe-obesity threshold matters because it is the gateway to escalation. Severe obesity is defined as a BMI at least 120 percent of the 95th percentile, or an absolute BMI of at least 35, whichever is lower. Once an adolescent crosses into severe obesity, the AHA scientific statement and the AAP guideline agree that lifestyle alone is unlikely to suffice, and you should plan toward pharmacotherapy and, where eligible, surgery. [7] [1]
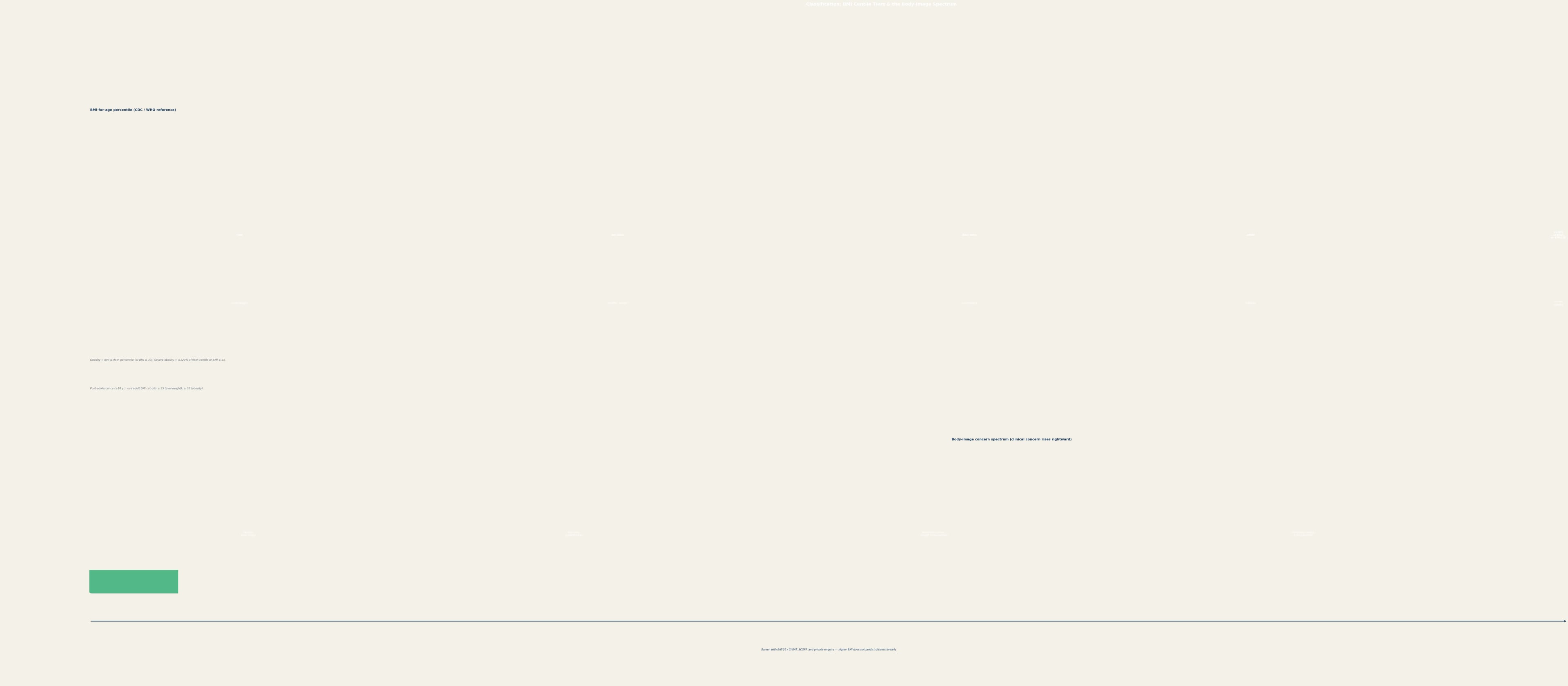
When the adolescent turns 18 you switch to adult cut-offs: overweight is BMI at least 25, and obesity is BMI at least 30. The crossover matters because a young person who looked "obese" on paediatric centiles at 17 may appear only "overweight" on adult cut-offs at 18, yet carry the same comorbidities and the same need for care. [1]
Epidemiology & Risk Factors
Globally, adolescent obesity has risen steeply over two decades, and the severe obesity category is growing fastest of all. Prevalence varies widely by region, ethnicity and socioeconomic position, and Indigenous, Pacific Islander, South Asian and Hispanic adolescents often carry a higher burden that reflects upstream environmental and historical drivers rather than individual behaviour. [1] [8]
The risk factors that cluster around an adolescent are familiar, but worth naming so you can act on them: family history of obesity or type 2 diabetes, socioeconomic disadvantage, food insecurity, high recreational screen time, short sleep duration, and exposure to weight-based teasing. Several of these are modifiable, and the lifestyle section returns to each of them. [12] [1]
Weight-based victimisation is strikingly common. Depending on the study, upward of half of adolescents with higher weight report teasing or bullying about their body, and that experience independently predicts depression, disordered eating, lower physical activity and worsened obesity trajectory. Treat it as a clinical problem in its own right, not background noise. [8] [14]
The single most useful prognostic statistic is tracking. The systematic review by Simmonds and colleagues found that a child or adolescent with obesity is roughly five times more likely to become an adult with obesity than a peer without, and that the probability rises with the severity and persistence of the adolescent obesity. This is why adolescence is not just a window for management — it is the window. [5] [6]
Pathophysiology
The simplest truthful sentence about adolescent obesity is that sustained positive energy balance expands adipose stores, and that the expanded adipose tissue then becomes metabolically and hormonally active in ways that reinforce the disease. But that sentence hides the real teaching, which is why the energy balance tilts and why it tilts more for some young people than others. [1] [2]

On the biological side, obesity is substantially polygenic, and the hypothalamic systems that regulate appetite through leptin and ghrelin signalling do not simply obey a person's intentions. This is why 'willpower' is a biologically inaccurate and clinically harmful frame — it blames a young person for a regulated system that is set against them. [2] [1]
The behavioural drivers are the ones lifestyle intervention targets: an energy intake that exceeds expenditure, a diet shifted toward ultra-processed foods, sedentary behaviour and high recreational screen time, and short sleep. The AHA scientific statement on sedentary behaviour documents that each of these is independently associated with adiposity in youth. [12]
The psychosocial drivers are where obesity and body image fuse. Depression and obesity are bidirectional — the prospective meta-analysis by Mannan and colleagues shows that adolescent depression predicts later obesity and adolescent obesity predicts later depression, in both sexes. Emotional eating and chronic stress reinforce the cycle, and weight-based teasing accelerates it. [15] [8]
The environmental drivers are upstream and powerful: food insecurity that paradoxically links to obesity through cheap energy-dense food, an obesogenic built environment, and socioeconomic disadvantage that constrains every 'choice' a young person appears to make. Naming these protects the young person from blame and directs advocacy as well as clinical care. [1] [8]
Finally, adipose tissue dysfunction produces low-grade systemic inflammation and insulin resistance, which is the engine of the comorbidities — type 2 diabetes, non-alcoholic fatty liver disease, dyslipidaemia and hypertension. The body and the mind are damaged by the same disease, through different routes, and you treat both. [2] [7]
Clinical Presentation
Most adolescents with obesity present at a routine health-supervision visit, a self-referred weight or body-image concern, or a visit for an unrelated problem where the BMI is noted. The presentation you must not miss is the one where the adolescent's real concern is psychological — distress about their body, bullying, or low mood — disguised behind a physical complaint. [1] [8]
Symptoms that point toward a comorbidity rather than simple obesity deserve targeted questioning: polyuria and polydipsia suggest hyperglycaemia or type 2 diabetes; snoring, witnessed apnoea and daytime sleepiness suggest obstructive sleep apnoea; headache and blurred vision suggest hypertension; right-upper-quadrant or diffuse abdominal discomfort can accompany fatty liver. Each of these changes the work-up and the urgency. [1] [13]
Disordered eating travels with higher weight more often than clinicians expect. Binge eating, loss-of-control eating and restrictive 'dieting' can all coexist with a larger body, and restrictive eating in a higher-weight adolescent can constitute atypical anorexia with the same medical danger as classic anorexia. Ask directly and without assumption. [10] [14]
On examination, look for the markers of insulin resistance and comorbidity: acanthosis nigricans (velvety hyperpigmentation in neck folds and flexures), blood pressure taken with an appropriately sized cuff, central adiposity and waist circumference, striae, hepatomegaly, and in females any hirsutism or menstrual irregularity that overlaps with polycystic ovary syndrome. [2] [1]
Features that should prompt you to look for a secondary or syndromic cause rather than primary obesity include short stature, developmental delay, dysmorphic features, Cushingoid fat distribution, and a history of cranial irradiation or hypothalamic tumour. These are the minority, but missing them delays treatable disease. [2]
Differential Diagnosis
The differential splits into two questions: is this obesity primary or secondary, and is the distress a body-image problem or a formal eating disorder? Both questions change the pathway. [1] [2]
Secondary causes are the minority, but the cost of missing them is high. Short stature, a falling growth velocity, developmental delay or hyperphagia out of proportion to the family all lower your threshold to investigate. [2] [1]
The psychiatric differential is equally important. Body dissatisfaction is common and treatable; binge eating disorder and bulimia nervosa require specific eating-disorder care; and atypical anorexia in a higher-weight adolescent is a medical emergency that masquerades as 'successful dieting'. Use screening tools and trust them. [10] [14]
Depression must be separated from 'just obesity'. The bidirectional relationship means both can be present, and treating one without the other fails the patient. A positive depression screen changes the management plan regardless of the BMI. [15]
Clinical & Bedside Assessment
The assessment is where you earn or lose the adolescent's trust for the next five years. Use the HEeadsss framework to structure the interview — Home, Education and employment, Eating, Activities, Drugs, Sexuality, Suicide and mood, Safety — so that weight and body image sit inside the young person's whole life rather than dominating it. Confidentiality and consent are foundational here; explain their limits and their protections explicitly at the start. [1] [8]
Measure height, weight and BMI and plot them on the correct age- and sex-specific reference. Calculate the percentage of the 95th percentile when you approach severe obesity, because that number drives escalation. Waist circumference adds risk stratification beyond BMI and is worth recording. Take blood pressure with a cuff that fits — a too-small cuff falsely elevates the reading in a larger arm. [1] [2]
Then see the adolescent alone. Ask about body image, dieting behaviour, teasing, mood and self-harm using validated, non-stigmatising questions. The Eating Attitudes Test (EAT-26, or ChEAT for younger adolescents), the SCOFF questionnaire, and the PHQ-A depression screen are practical, brief and sensitive. A positive screen in a higher-weight adolescent is never dismissed as 'expected'. [10] [14]
SCOFF
Two or more 'yes' answers raise concern for an eating disorder. Remember that SCOFF screens for eating-disorder pathology across the weight spectrum, including in higher-weight adolescents. [10]
Examine for acanthosis nigricans, striae, hepatomegaly, hirsutism, central adiposity and blood pressure, and ask the comorbidity-focused questions — snoring, polyuria, headaches, menstrual pattern, joint pain. Use motivational interviewing to gauge readiness to change: ask open questions, reflect rather than advise, and let the adolescent set the agenda. Language matters at every step — use person-first, weight-neutral phrasing ('a young person with obesity', never 'an obese kid') and never make the scale the headline. [1] [8]
Investigations
Investigations serve two goals: detect comorbidity, and exclude secondary causes when the clinical picture demands it. The baseline metabolic panel is for every adolescent with obesity. [1]
These four — glucose metabolism, lipids, liver enzyme, and blood pressure — catch most of the modifiable comorbidity early. Abnormal results direct referral and treatment. [1] [2]
For non-alcoholic fatty liver disease, the NASPGHAN guideline recommends ALT as the first-line screen, with liver ultrasound and gastroenterology referral when ALT is persistently elevated or other risk factors accumulate. Ultrasound alone is insensitive for early steatosis, so a normal scan does not exclude disease. [13]
Tests to exclude secondary causes are not universal — they are triggered by clinical features. Check TSH when thyroid dysfunction is suspected (short stature, bradycardia, cold intolerance); consider a morning cortisol or low-dose dexamethasone suppression test for Cushingoid features; and measure IGF-1 and pursue genetic testing (Prader-Willi, MC4R pathway) when hyperphagia, developmental delay or dysmorphism are present. [2]
A sleep study (polysomnography) is indicated when an obese adolescent snores, has witnessed apnoea, daytime sleepiness or unexplained pulmonary hypertension, to evaluate obstructive sleep apnoea. Untreated sleep apnoea worsens metabolic and cardiovascular outcomes and impairs learning and mood. [1] [7]
Mental-health screening is an investigation in its own right. Administer the PHQ-A for depression, the GAD-7 for anxiety, the EAT-26 or SCOFF for disordered eating, and ask directly about self-harm and suicidality. Repeat these at intervals, because the picture changes and the stakes are high. [10] [15]
Management — Resuscitation
There is no traditional resuscitation phase in adolescent obesity, because the disease is chronic rather than acute. But several scenarios demand urgent action, and you must recognise them. [1]
First is active suicidal ideation disclosed during a body-image or weight assessment. Assess ideation, plan, intent and protective factors in detail; formulate a safety plan; involve mental-health services and the family where safety requires it; and document your reasoning. A disclosure of suicidality always outranks a discussion of BMI. [15]
Second is medical instability from a restrictive eating disorder — atypical anorexia in a higher-weight adolescent. Bradycardia, orthostatic vital-sign changes, hypothermia or electrolyte disturbance are emergencies that belong on an eating-disorder pathway, not a weight-loss pathway. [10] [14]
Third is symptomatic or markedly deranged type 2 diabetes discovered on screening — significant hyperglycaemia, ketosis, or features of hyperosmolarity. This needs same-day diabetes-team involvement, fluid and electrolyte assessment, and consideration of insulin. Severe hypertension with target-organ features, and obstructive sleep apnoea with desaturation or cor pulmonale, are further urgent scenarios that redirect the entire visit. [1] [7]
Beyond these, escalation to paediatric endocrinology, gastroenterology, sleep medicine or a specialist weight-management service is appropriate when comorbidities are complex, when severe obesity needs intensification, or when primary-care management is not succeeding. [1]
Management — Definitive & Stepwise
Definitive management is staged, and the staging is the structure examiners reward. Each stage builds on the last, escalation is deliberate, and a parallel body-image and mental-health track runs alongside every stage rather than being bolted on at the end. [1]
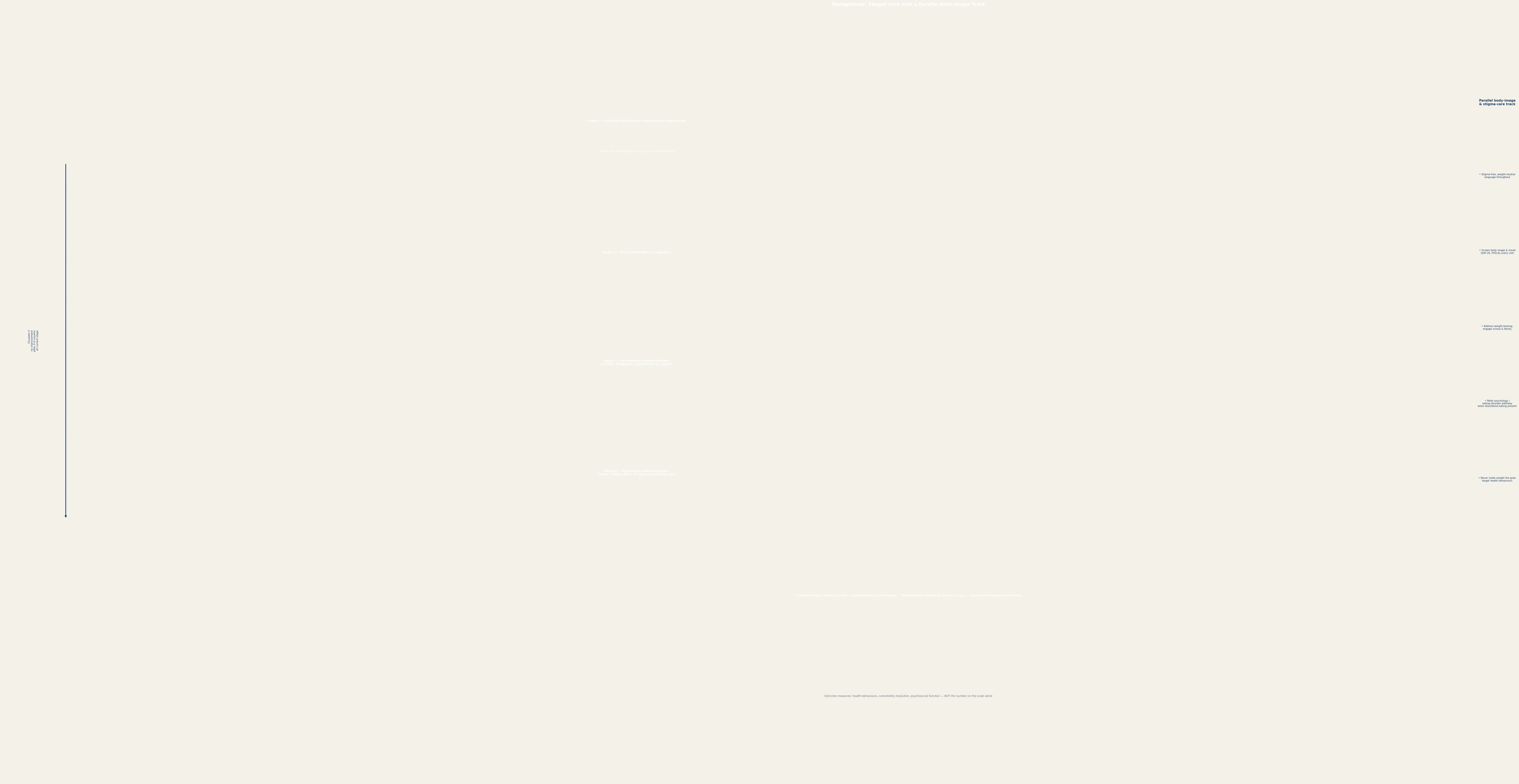
Stage 1 — Lifestyle (all patients). Lifestyle modification is the foundation for every adolescent with obesity, regardless of severity, and the Cochrane reviews by Mead and Ells confirm that diet, physical activity and behavioural interventions produce modest but real benefit. Frame it around health behaviours, not weight: at least 60 minutes of moderate-to-vigorous physical activity daily, a sustainable healthy eating pattern, sleep optimisation, and limiting recreational screen time. Deliver it with motivational interviewing. [3] [4] [1]
Stage 2 — Structured multidisciplinary paediatric weight management. When Stage 1 is insufficient, intensify to a structured programme with dietetics, psychology, exercise physiology and medical input. This is team-based care, still behaviour-anchored, with more structure and closer follow-up. [1] [4]
Stage 4 — Tertiary care interventions including anti-obesity pharmacotherapy. For moderate-to-severe obesity, escalate to medication alongside continued lifestyle. Options vary by region and include orlistat (which inhibits pancreatic lipase; a typical adolescent dose is orlistat 120 mg three times daily with fat-containing meals, with fat-soluble-vitamin monitoring), phentermine (short-term, region-dependent), and GLP-1 receptor agonists such as liraglutide (subcutaneous, titrated up to a maximum of 3 mg daily where approved, with attention to gastrointestinal effects and nutritional adequacy). The recent review by Fox and colleagues summarises the expanding pharmacological landscape. [16] [1]
Stage 4 — Metabolic and bariatric surgery. Surgery is now endorsed for carefully selected adolescents with severe obesity. Typical eligibility is a BMI at least 35 with a significant comorbidity such as type 2 diabetes, or at least 40 without comorbidity, performed at a specialist adolescent centre with lifelong follow-up. The Teen-LABS data show that bariatric surgery can achieve remission of type 2 diabetes and substantial comorbidity improvement, dramatically outperforming medical therapy in severely obese adolescents. [9] [7]
Escalation logic
Stage 1 lifestyle for every patient, delivered with motivational interviewing and weight-neutral language.
Escalate to Stage 2 structured multidisciplinary care if no improvement after 3–6 months at Stage 1.
Add Stage 3 pharmacotherapy for moderate-to-severe obesity; choose agent by region, adherence and side-effect profile.
Refer for Stage 4 surgery when BMI thresholds are met and the adolescent understands lifelong follow-up.
At every stage, run the parallel body-image and mental-health track: screen, address teasing, refer psychology when needed.
The trigger to escalate is failure to improve after three to six months at the current stage, combined with comorbidity burden and the adolescent's readiness. Never escalate a young person who is not engaged. [1] [7]
Throughout, treat the comorbidities alongside the weight: metformin for insulin resistance or type 2 diabetes, positive airway pressure for obstructive sleep apnoea, dietary and statin management of dyslipidaemia per regional paediatric lipid guidance, and liver-directed care for NAFLD. And measure success with health behaviours, comorbidity resolution and psychosocial function — the scale is one datum among many, never the verdict. [1] [13]
Specific Subtypes & Scenarios
Severe obesity changes the conversation. Once the BMI reaches 120 percent of the 95th percentile or an absolute 35, lifestyle alone rarely suffices, and you should plan early toward pharmacotherapy and surgical referral rather than waiting through cycles of unsuccessful lifestyle attempts. The AHA statement is explicit about this. [7] [1]
Obesity with binge eating or loss-of-control eating is common and needs integrated care. Address the eating behaviour with psychology before or alongside weight-management pharmacotherapy, because some weight-loss medications can themselves interact with eating-disorder pathology. A higher-weight adolescent with atypical anorexia belongs on an eating-disorder pathway first, with any obesity treatment held until medical and psychiatric stability is achieved. [10] [14]
Culturally and linguistically diverse adolescents bring ethnicity-specific body ideals, dietary patterns and health beliefs that shift both the BMI-risk relationship and the threshold at which body-image distress becomes clinical. Use a professional interpreter, ask about family and community body norms, and avoid transplanting one culture's body standard onto another. [8] [1]
A gender-diverse adolescent on gender-affirming hormone therapy presents a particular challenge: body composition changes with hormones, body-image concerns may relate to gender dysphoria as much as weight, and the young person may be especially alert to scrutiny of their body. Coordinate with the gender service and keep weight-neutral, affirming language central. [8]
Indigenous adolescents (Aboriginal, Torres Strait Islander, Maori, Pacific Islander) carry a higher metabolic severity and carry the weight of historical and ongoing determinants. Culturally safe care, family and community engagement, and explicit attention to the social determinants are not optional refinements — they are core management. [1] [8]
The adolescent in out-of-home care, or facing food insecurity or socioeconomic disadvantage, often has disrupted food security, fragmented records and care discontinuity. Prioritise practical support, care coordination and follow-up continuity over idealised lifestyle prescriptions that assume a stable environment. [1] [8]
Complications & Pitfalls
The most damaging complication of adolescent obesity care is often the weight stigma the young person encounters in clinical settings, including from clinicians. Stigmatising language and framing reduce engagement, worsen mental health, and paradoxically worsen the obesity. Puhl and colleagues' work is unambiguous on this. [8] [14]
A close second is the pitfall of triggering or worsening a restrictive eating disorder through weight-centric lifestyle advice. Overemphasising weight loss in a vulnerable adolescent can tip them into atypical anorexia with real medical danger. Frame every lifestyle conversation around behaviours and function, never around the weight number. [10] [14]
Missing a comorbidity because attention stayed fixed on the BMI is a recurring failure. Type 2 diabetes, NAFLD, obstructive sleep apnoea and hypertension are all treatable, and all are easy to overlook if the only metric discussed is weight. Screen systematically at baseline and repeat. [1] [13]
Under-treatment of severe obesity — leaving a young person on lifestyle alone when the evidence supports pharmacotherapy and surgery — is the mirror image of over-treatment and is equally a failure. The guideline endorsement of intensification exists precisely because lifestyle is insufficient for severe disease. [7] [9]
Pharmacotherapy has its own pitfalls: orlistat causes fat-soluble-vitamin deficiency and gastrointestinal effects; GLP-1 receptor agonists cause nausea and require attention to nutritional adequacy and, in the context of pregnancy planning, cessation given teratogenicity concerns. Surgery carries perioperative risk and lifelong nutritional and adherence requirements. [16] [9]
Finally, deferring transition to adult care until the adolescent is lost to follow-up leaves comorbidities unmanaged. Plan transition deliberately, with a structured handover, from late adolescence. [1]
Prognosis & Disposition
The long-term cardiometabolic prognosis of an adolescent with obesity is shaped by severity, comorbidity, engagement and the social determinants that surround them. The tracking evidence is stark: childhood and adolescent obesity is a strong predictor of adult obesity and adult morbidity, and the risk scales with how severe and persistent the adolescent disease is. [5] [6]
Comorbidity trajectories matter. Untreated type 2 diabetes in adolescence carries a high lifetime burden of complications; NAFLD can progress to steatohepatitis and fibrosis; hypertension and dyslipidaemia seed adult cardiovascular disease. Treating the comorbidities early and well is among the most consequential things a clinician can do for the adult this adolescent will become. [1] [13]
Psychosocial prognosis is just as important. Untreated depression and body-image distress worsen every other outcome — engagement, adherence, lifestyle success, quality of life. Conversely, sustained, family-centred, weight-neutral care that addresses stigma and builds body acceptance can substantially improve function and wellbeing even when the BMI moves modestly. [8] [15]
Follow-up frequency is higher during active management (often every few months) and relaxes to annual health-supervision once the plan is stable and comorbidities are controlled. Comorbidity resolution — diabetes remission after surgery, NAFLD regression with weight loss — measurably improves long-term outlook and should be tracked explicitly. [1] [9]
Transition to adult care is planned, not drifted into. For a young person with chronic obesity, comorbidities and an established multidisciplinary team, a structured handover to adult endocrinology, hepatology or a weight-management service preserves continuity and protects the gains made in adolescence. [1]
Special Populations
Culturally safe obesity and body-image care for Indigenous adolescents means engaging family and community, acknowledging the historical and structural determinants of the higher metabolic severity, and refusing individualistic framing of a population-level problem. [1] [8]
For migrant, refugee and asylum-seeking adolescents, language barriers, food insecurity, trauma exposure and different cultural body norms all shape the assessment and the plan. Use professional interpreters, screen for the psychological consequences of displacement, and adapt dietary advice to culturally familiar foods rather than imposing unfamiliar prescriptions. [8]
Adolescents in out-of-home care often arrive with incomplete records, disrupted food security and care discontinuity. Prioritise coordination, continuity and practical support; a perfect lifestyle prescription is useless if the young person has no stable kitchen or schedule. [1]
Socioeconomic disadvantage shapes every layer — access to healthy food, safe places for physical activity, specialist services, pharmacotherapy and surgery. Recognising these constraints is not making excuses; it is diagnosing a real part of the disease and directing advocacy alongside clinical care. [1] [8]
A gender-diverse adolescent requires integrated obesity and gender-affirming care: body composition shifts on hormone therapy, body-image distress may interweave with gender dysphoria, and weight-neutral, affirming communication is essential. Coordinate with the gender service and the mental-health team. [8]
Adolescents with intellectual disability or neurodevelopmental conditions, and those with medical complexity or technology dependence, need integrated care that accounts for communication, feeding, mobility and the baseline condition, and in which obesity or faltering growth is interpreted against that baseline rather than in isolation. [1]
Evidence, Guidelines & Regional Differences
The 2023 AAP Clinical Practice Guideline (Hampl and colleagues) is the current landmark. It reframes obesity as a chronic disease, endorses immediate and intensive treatment rather than watchful waiting, and lays out a staged approach from lifestyle through pharmacotherapy to surgery, with concurrent behavioural and mental-health support. [1]
The 2017 Endocrine Society guideline (Styne and colleagues) sits alongside the AAP framework and offers complementary detail on assessment, comorbidity screening and prevention, with broadly concordant percentile-based definitions and management principles. [2]
The Cochrane reviews (Mead on diet, physical activity and behavioural interventions; Ells on the overview of interventions) establish the evidence base for lifestyle: the benefit is real but modest, which is precisely why severe disease needs escalation beyond lifestyle alone. [3] [4]
Surgical evidence comes from the Teen-LABS cohort and related studies; Inge and colleagues showed that bariatric surgery achieved markedly better type 2 diabetes outcomes than medical therapy in severely obese adolescents, supporting surgery as a legitimate option for selected patients. The AHA scientific statements (Kelly on severe obesity; Barnett on sedentary behaviour) and the NASPGHAN NAFLD guideline (Vos) round out the guideline landscape for comorbidity-specific management. [9] [7] [12] [13]
Puhl and colleagues have quantified the prevalence and harm of weight stigma in youth, and Hooper, Puhl and Eisenberg have shown longitudinally how family and parenting factors modify the impact of stigma on disordered eating. The Mannan meta-analysis establishes the bidirectional depression-obesity relationship. Together these underpin the insistence on parallel psychological care. [8] [14] [15]
Teen-LABS — Inge 2018
Key finding
Bariatric surgery achieved far higher glycaemic remission and comorbidity improvement than medical therapy, supporting surgery for selected severely obese adolescents.
Practice change
Do not leave severe obesity with diabetes on lifestyle and metformin alone — surgery is evidence-based.
In Australia and New Zealand, pharmacotherapy availability and surgery pathways vary by jurisdiction and funding; RACP and RCH guidance emphasise family-centred, multidisciplinary care and culturally safe practice for Aboriginal, Torres Strait Islander and Maori adolescents.
Emerging GLP-1 receptor agonist evidence in adolescents is promising but evolving; regional formularies, surgery thresholds and school-nutrition policies differ, so name the principle and check local guidance before prescribing.
Evidence controversies remain: the modest magnitude of lifestyle benefit, the long-term safety of newer pharmacotherapy in growing adolescents, the optimal timing of surgery, and how best to measure success beyond BMI. Fox and colleagues review the current and future pharmacological landscape. [16] [9]
Exam Pearls
The high-yield points a fellowship candidate must hold: screen every adolescent with obesity for comorbidities (fasting glucose or HbA1c, lipids, ALT, blood pressure) and for body-image distress, disordered eating, depression and weight-based victimisation. [1] [8]
Lifestyle is the foundation for every patient — but lifestyle language targets health behaviours, never the weight number, to avoid triggering eating disorders. [3] [10]
Escalate to pharmacotherapy and surgery for severe obesity; do not leave severe disease on lifestyle alone. Bariatric eligibility commonly runs at BMI at least 35 with a comorbidity or at least 40 without, at a specialist centre. [7] [9]
Atypical anorexia occurs in higher-weight adolescents and carries the same medical risk as anorexia at low weight — recognise it and escalate to eating-disorder care, not a weight-loss pathway. [10] [14]
Weight stigma worsens every outcome; addressing it with weight-neutral, person-first language is core management, not an optional courtesy. And the depression-obesity relationship is bidirectional — treat both concurrently. [8] [15]
Outcome measures are health behaviours, comorbidity resolution and psychosocial function — the scale is one datum among many, never the verdict on a young person's worth or your care. [1]
References
- [1]Hampl SE, Hassink SG, Skinner AC Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics, 2023.PMID 36622115
- [2]Styne DM, Arslanian SA, Connor EL Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. Journal of clinical endocrinology and metabolism, 2017.PMID 28359099
- [3]Mead E, Brown T, Rees K Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database of Systematic Reviews, 2017.PMID 28639319
- [4]Ells LJ, Rees K, Brown T Interventions for treating children and adolescents with overweight and obesity: an overview of Cochrane reviews. International journal of obesity, 2018.PMID 30301964
- [5]Simmonds M, Llewellyn A, Owen CG Predicting adult obesity from childhood obesity: a systematic review and meta-analysis. Obesity reviews, 2016.PMID 26696565
- [6]Llewellyn A, Simmonds M, Owen CG Childhood obesity as a predictor of morbidity in adulthood: a systematic review and meta-analysis. Obesity reviews, 2016.PMID 26440472
- [7]Kelly AS, Barlow SE, Rao G Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation, 2013.PMID 24016455
- [8]Puhl RM, Lessard LM Weight Stigma in Youth: Prevalence, Consequences, and Considerations for Clinical Practice. Current obesity reports, 2020.PMID 33079337
- [9]Inge TH, Laffel LM, Jenkins TM Comparison of Surgical and Medical Therapy for Type 2 Diabetes in Severely Obese Adolescents. JAMA pediatrics, 2018.PMID 29532078
- [10]Neumark-Sztainer D, Wall MM, Chen C Eating, Activity, and Weight-related Problems From Adolescence to Adulthood. American journal of preventive medicine, 2018.PMID 29937114
- [11]Quick V, Eisenberg ME, Bucchianeri MM Prospective Predictors of Body Dissatisfaction in Young Adults: 10-year Longitudinal Findings. Emerging adulthood, 2013.PMID 25045599
- [12]Barnett TA, Kelly AS, Young DR Sedentary Behaviors in Today's Youth: Approaches to the Prevention and Management of Childhood Obesity: A Scientific Statement From the American Heart Association. Circulation, 2018.PMID 30354382
- [13]Vos MB, Abrams SH, Barlow SE NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children. Journal of pediatric gastroenterology and nutrition, 2017.PMID 28107283
- [14]Hooper L, Puhl RM, Eisenberg ME Can Family and Parenting Factors Modify the Impact of Weight Stigma on Disordered Eating in Young People? A Population-Based Longitudinal Study. Journal of adolescent health, 2023.PMID 36914449
- [15]Mannan M, Mamun A, Doi S Prospective Associations between Depression and Obesity for Adolescent Males and Females- A Systematic Review and Meta-Analysis of Longitudinal Studies. PLoS one, 2016.PMID 27285386
- [16]Fox CK, Kelly AS, Reilly JL Current and future state of pharmacological management of pediatric obesity. International journal of obesity, 2025.PMID 38321079