Paeds · clinical-assessment-and-reasoning
Continuity of care and the paediatric medical home
Also known as Paediatric medical home · Patient-centred medical home children · Care coordination paediatrics · Relational continuity · Longitudinal primary care children
A fellowship approach to continuity of care and the paediatric medical home: relational, informational and management continuity; care coordination; loop closure after ED and hospital care; foster care and transition; equity and regional models across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Imagine a school-age child with asthma who sees a different doctor every winter flare. Each clinician restarts the story. Inhaler technique is never checked against the last admission. The mother carries a plastic bag of clinic letters. That is not continuity, even if every visit was competent in isolation. [1] [4]
Continuity of care is the degree to which a patient experiences care as connected and coherent over time. Haggerty’s multidisciplinary review separates three domains you must name in exams: relational, informational and management continuity. Relational continuity is an ongoing therapeutic relationship. Informational continuity is the use of information on past events and circumstances. Management continuity is a consistent approach to managing a health condition, especially when several clinicians are involved. [1] [27]
The paediatric medical home is the operational home for that continuity. Historically it grew from care models for children with special health care needs and expanded toward every child. The core idea is a usual source of care that is accessible, continuous, comprehensive, family-centred, coordinated, compassionate and culturally effective. A building with a paediatric sign is not automatically a medical home. [2] [3]
From first contact to a functioning medical home
Name the home
Identify the usual primary clinician or team and confirm the family knows how to reach them.
Map the network
List specialists, hospital teams, school supports, equipment suppliers and legal decision-makers.
Reconcile facts
Align medicines, allergies, outstanding results, growth trajectory and emergency plans.
Coordinate deliberately
Track referrals, close loops after ED or ward care, and share one plan in plain language.
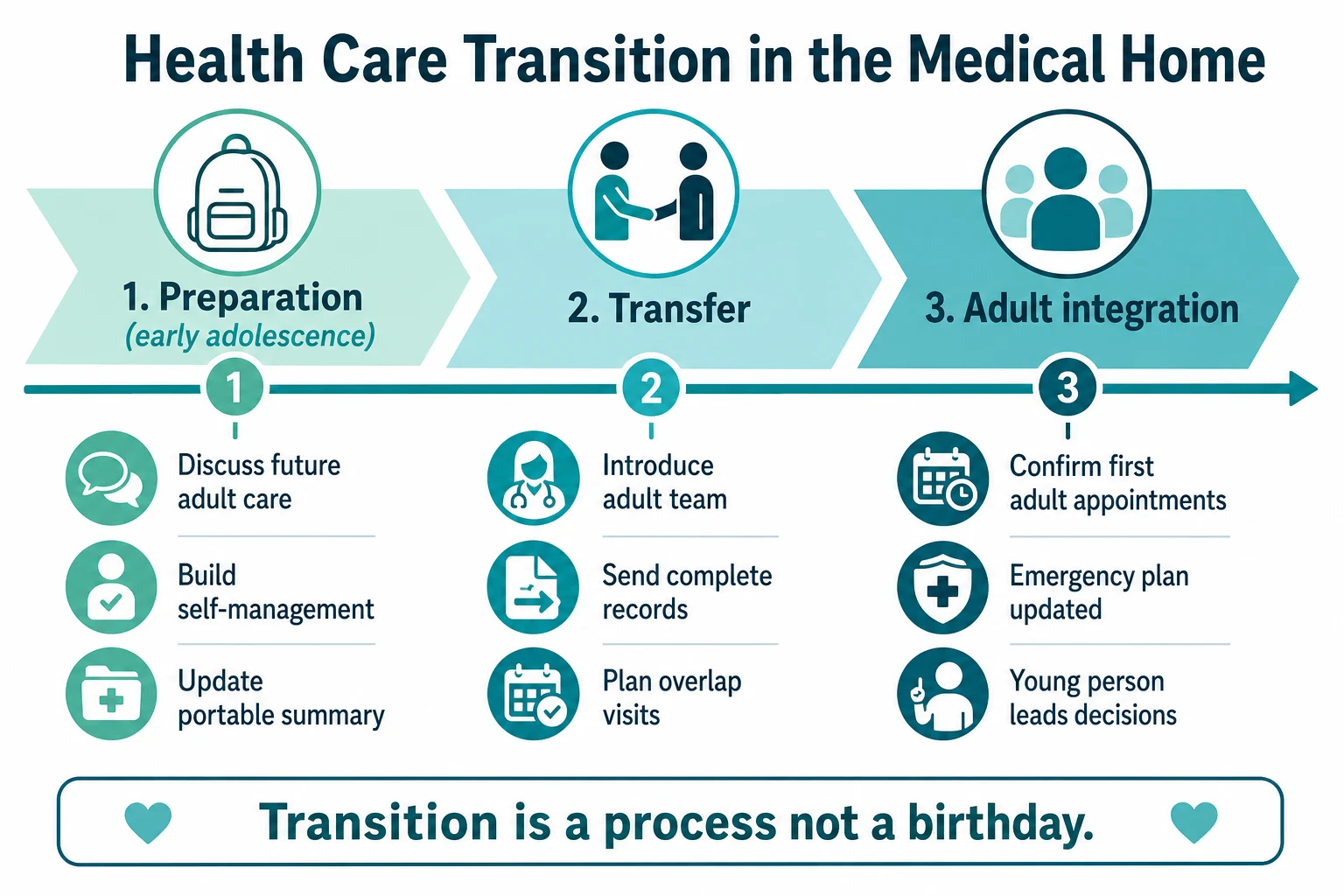
Plan transitions early
Prepare adolescent-to-adult transfer as a process, not a birthday letter.
Classification
Start with the child in front of you, then classify the system problem as carefully as the disease problem. [1] [2]
Continuity domains
Relational continuity is being known. The family does not retell the entire life story at every visit. Trust supports earlier help-seeking and more accurate history. [1] [28]
Informational continuity is usable knowledge. Prior growth charts, discharge summaries, allergy lists and pending tests are available and acted on. Without it, teams repeat investigations and miss delayed results. [1] [7]
Management continuity is one coherent plan. Goals, escalation thresholds and follow-up ownership are shared across primary care, hospital and specialty services. Conflicting advice is a management discontinuity until reconciled. [1] [12]
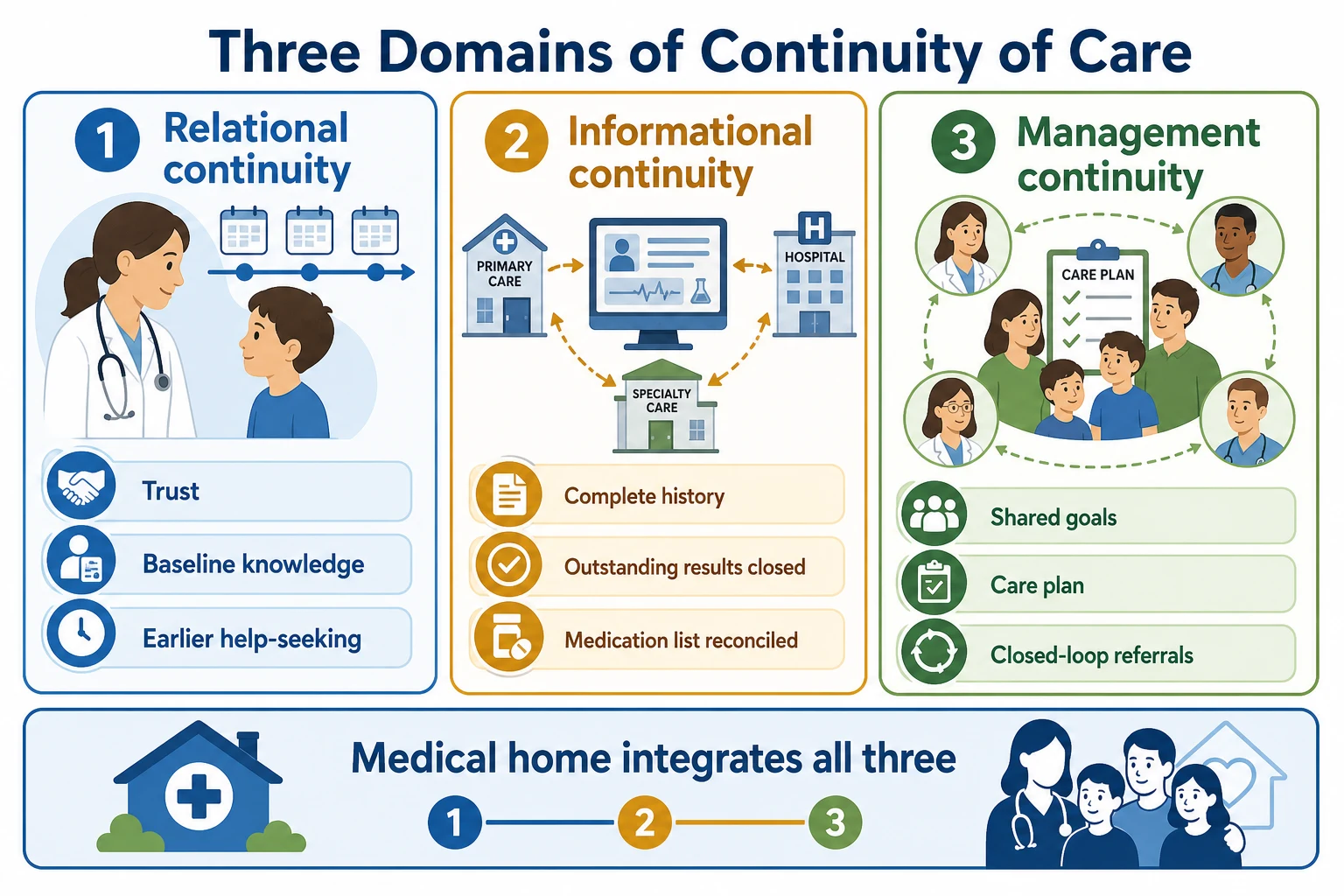
Read the figure like this: if a child “has a GP” but every flare goes to ED with no letter back, relational and management continuity may still be failing. Name the broken domain before you prescribe another clinic appointment. [1] [20]
Medical home versus nearby concepts
| Label | What it means | Common exam trap |
|---|---|---|
| Usual source of care | Family names a place or person they usually go to | Necessary but not sufficient for a medical home |
| Medical home | Continuous, comprehensive, family-centred, coordinated care model | Not guaranteed by clinic branding alone |
| Care coordination | Deliberate organisation of patient care activities between participants | Not the same as “more referrals” |
| Specialty medical home | Specialty team holding intensive co-management for selected conditions | Still needs a primary medical home for whole-child care |
| Complex-care programme | Higher-intensity coordination for children with medical complexity | Evidence is mixed and context-dependent |
Practice-level implementation can be measured with tools such as the Medical Home Index, which rates how fully a practice enacts medical-home processes. That is a service measure, not a bedside severity score for the child. [10]
Relationship-focused activities (knowing the family, continuity with a named clinician) are not identical to structural activities (registries, electronic portals, formal policies). Quality programmes that count only structure can miss whether children are actually known. [23]
Relational
Who knows this child?
- Named clinician or small team
- Baseline behaviour and family context known
- Trust supports disclosure and follow-up
- Roster chaos and temporary staffing erode it
Informational
What travels with the child?
- Reconciled medicines and allergies
- Outstanding results owned
- Discharge and specialty letters received
- Interoperability failures create harm
Management
Is there one plan?
- Shared goals and responsibilities
- Closed-loop referrals
- Emergency information form current
- Conflicting advice is a safety issue
Epidemiology & Risk Factors
There is no single global incidence of “failed continuity.” What matters is which children lose a medical home and what happens next. [21] [3]
Population surveys of children with special health care needs show incomplete access to medical-home attributes, with disparities by income, insurance, race and ethnicity in US data. Treat exact percentages as jurisdiction- and year-specific; the exam point is inequitable distribution, not one universal number. [21] [3]
In paediatric observational work, lower continuity has been associated with greater emergency department use and hospitalisation, and higher continuity with better parent-reported quality and better-coordinated care. These are associations, not pure causal proofs, but they are strong enough to change practice design. [4] [5] [6] [7]
Risk factors for fragmentation cluster in the child, family and system: [17] [13]
- Child factors: medical complexity, technology dependence, multiple specialties, developmental disability, mental health comorbidity. [13] [15]
- Family and social factors: poverty, transport barriers, language discordance, housing instability, racism and prior adverse health-system experiences. [17] [21]
- System factors: no after-hours pathway into the medical home, open-loop referrals, hospitalist models without primary-care partnership, payment that rewards volume over coordination time. [17] [18] [20]
- Placement factors: foster and kinship care create predictable record and provider discontinuity. [29] [30]
Unmet specialty care is more likely when care coordination is weak among children with special health care needs. That is a coordination problem as much as a specialist-supply problem. [22]
Pathophysiology
Continuity fails through mechanisms you can explain at the bedside. [1] [28]
Loss of baseline knowledge raises diagnostic noise. A child with cerebral palsy who is “a bit more sleepy” may be seriously ill, but only a team that knows usual tone and interaction will hear the signal early. Relational discontinuity converts subtle change into late crisis. [1] [28]
Information gaps create missed results, duplicate radiation or blood tests, allergy errors and delayed action on abnormal findings. Each handoff without closed loop is a potential failure point. [1] [7]
Conflicting management plans increase cognitive load. Caregivers receive different feeding, medication or escalation advice from ED, ward and clinic. Adherence falls not only from “non-compliance” but from impossible instructions. [12] [16]
Caregiver overload is a physiological and social stressor. When systems dump coordination labour onto families, sleep, employment and medication safety suffer. Empowerment is not the same as unpaid case management. [13] [16]
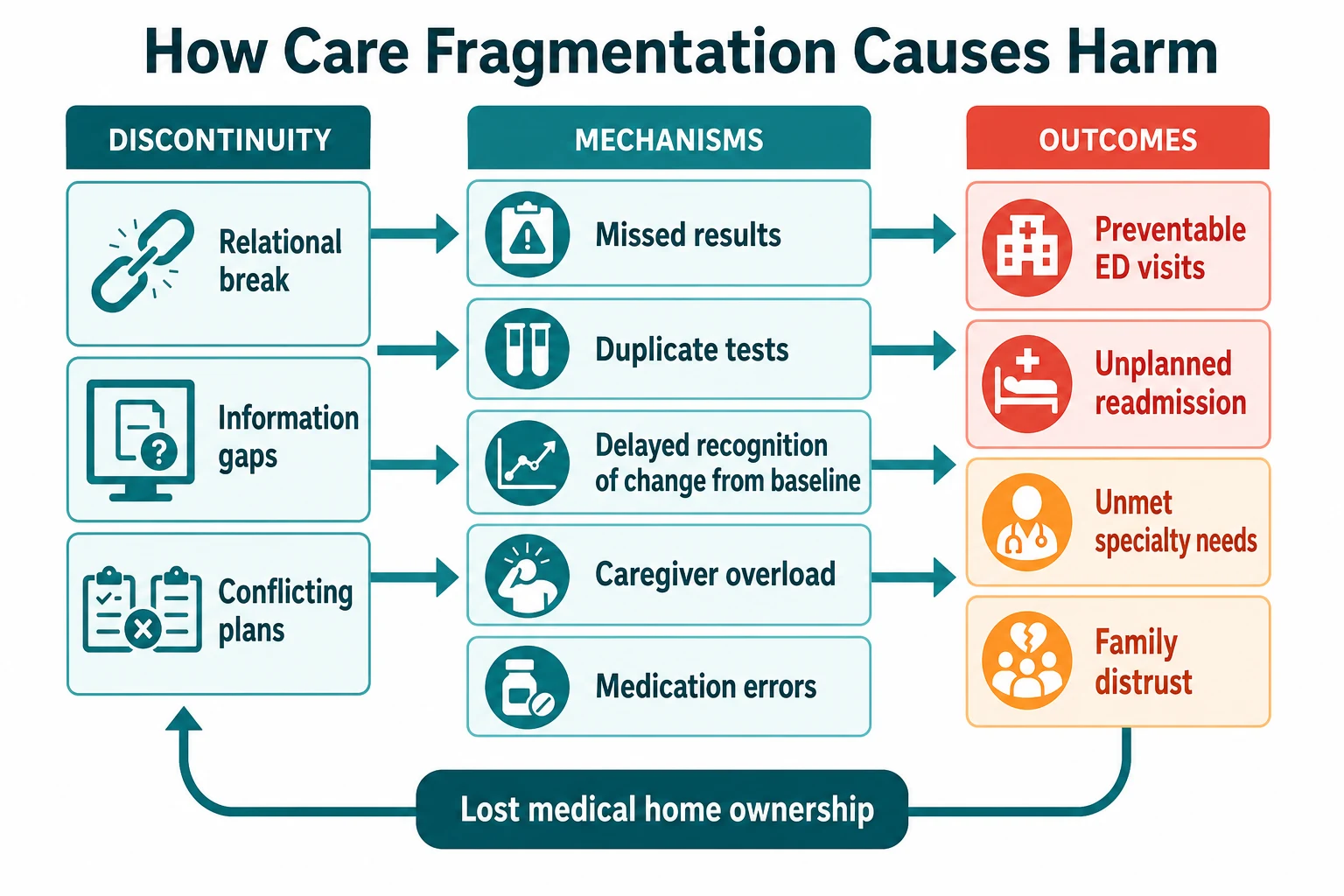
Read the figure like this: when a family says “we are drowning in appointments,” treat that as a system diagnosis. Ask which domain broke, then repair ownership. [13] [16]
Developmental transitions are predictable vulnerability points: newborn hospital discharge, school entry, adolescence and adult transfer. Each transition multiplies new clinicians and new records. Without deliberate bridging, management continuity collapses even if each service is excellent alone. [19] [1]
Clinical Presentation
Continuity problems present as patterns across time, not a single abnormal vital sign. [1] [4]
Well-functioning medical home: the family names their clinician; preventive care is up to date; acute advice is reachable; letters return; the child is recognised as “not themselves” early. [2] [6]
Fragmented care patterns you should recognise: [4] [13]
- Repeated ED attendances for the same chronic issue without primary-care review. [4] [20]
- “Nobody owns this” after multi-specialty involvement. [13]
- Caregiver carries a bag of unsorted letters and cannot state the current plan. [12]
- Outstanding imaging or laboratory results with no responsible clinician. [1]
- School exclusion or missed early intervention because health and education never shared a plan. [31] [33]
- Adolescent with diabetes or epilepsy turning 17 with no adult service named. [19]
- Foster placement change with unknown immunisations and no assigned medical home. [29] [30]
| Life stage | What you often see | What to protect |
|---|---|---|
| Neonates | NICU discharge with incomplete primary-care linkage | Named first medical home before discharge |
| Infants and toddlers | Missed preventive visits; after-hours ED for minor illness | Usual clinician plus safe after-hours advice route |
| School-age | Asthma or ADHD plans not aligned with school | Shared action plans and school communication |
| Adolescents | Drop-out from primary care; confidential needs elsewhere | Medical home that can hold privacy and whole-person care |
| Transition age | Birthday transfer with no adult team | Years-long preparation and transfer process |
| Medical complexity any age | Equipment, polypharmacy, many specialties | Explicit coordinator and emergency information form |
Differential Diagnosis
When care looks chaotic, separate disease, access and continuity. [13] [20]
| Problem that looks similar | Discriminator | First move |
|---|---|---|
| No access at all | Cannot get any appointment or transport | Fix access and safety net urgently |
| Access without continuity | Many visits, no one knows the child | Name a home clinician and reduce team scatter |
| True medical complexity | Multiple active conditions and technology | Escalate coordination intensity |
| System-created complexity | Conflicting plans for a simpler disease | Reconcile plan; stop unnecessary parallel clinics |
| Caregiver capacity limits | Exhaustion, literacy, competing demands | Support and simplify; avoid blame |
| Safeguarding or neglect | Pattern of harm, concealment or unexplained injury | Follow local safeguarding pathway in parallel |
| Appropriate episodic urgent care | Single clear minor illness with loop closed | Acceptable if medical home informed |
| Orphaned specialty care | Only tertiary clinic, no whole-child preventive care | Rebuild primary medical home |
Do not diagnose “non-compliance” until you have tested whether the plan is understandable, affordable, culturally safe and operationally possible. Family-centred care evidence for children with special health care needs supports partnership rather than instruction alone. [35] [16]
Clinical & Bedside Assessment
You can assess continuity in minutes if you ask the right questions. [2] [11]
1. Who is the medical home?
“Who is your usual doctor or nurse practitioner for this child? How do you reach them after hours?” If the answer is “whoever is free” or “we only use ED,” continuity is already impaired. [2] [20]
2. What is the network map?
List active specialties, community nursing, school supports, early intervention, equipment vendors and legal guardians. For complex children, draw it. [12] [13]
3. What information is missing?
Outstanding results, last discharge summary, current medication list, allergy status, growth chart and immunisation registry. Medication reconciliation is a continuity examination. [1] [7]
4. Is there a written plan?
Look for a shared care plan and an emergency information form for complex illness. Check dates and whether the family can use it under stress. [11] [12]
5. Who does the coordination labour?
If the answer is only the mother between midnight feeds, the model is unsafe even if clinics exist on paper. [13] [16]
6. Transition readiness (adolescents):
Can the young person name their conditions and medicines? Is there an adult service pathway? Has a portable summary been prepared? [19]
7. Equity and communication access:
Interpreter need, disability communication method, transport, digital exclusion and cultural safety determine whether continuity is real. [17] [34]
Document sources: who said what, which letter was seen, which result is still pending. Source attribution protects the next clinician. [1]
Investigations
Continuity investigation is often record work, not more blood tests. [1] [12]
High-value “tests” of the system: [1] [11]
- Growth and development trajectories across time. [33]
- Immunisation registry and catch-up needs, especially in foster care. [29] [30]
- Medication reconciliation after multi-provider care. [12]
- Outstanding radiology or laboratory queues. [1]
- Discharge summaries and specialty letters within a defined time window. [11]
- School or early-intervention reports when function is the question. [31]
- Care-coordination quality measures at service level for CMC programmes. [25]
Continuity indices (for example visit-based continuity measures reviewed by Jee and Cabana) are mainly research and quality tools. Do not invent a bedside numeric cut-off for an individual child in an OSCE. Use them to understand service design literature. [9] [8]
Avoid harm: repeating imaging because prior films are inaccessible is an informational failure. Fix retrieval pathways rather than normalising duplication. [1]
Disease-specific investigations remain disease-specific. Continuity language never replaces a septic workup or airway assessment when the child is sick now. [12] [32]
Management — Resuscitation
Continuity work never outranks airway, breathing, circulation, seizure control, glucose or immediate safety. [12] [32]
If the child is critically unwell: [12] [32]
- Call for help and run age-adapted ABCDE.
- Use any available emergency information form, steroid card, device settings or medical-home summary in parallel.
- Ask the caregiver: “What is different from their usual, and what usually works?”
- Notify the medical home after initial stabilisation, not instead of it.
- Preserve later continuity by recording timed interventions, responses and outstanding tasks for handover. [12] [32]
Rural and telehealth teams may hold the only relational knowledge of baseline. Use that knowledge to guide retrieval thresholds, then ensure the written plan travels with the child. [1] [28]
If continuity review uncovers active suicidal intent, assault or other imminent harm, switch to safety and mandatory pathways. Confidentiality has limits when serious harm is imminent; that principle belongs in any medical-home adolescent process. [19]
Management — Definitive & Stepwise
This is the constructive algorithm examiners want. [11] [12]
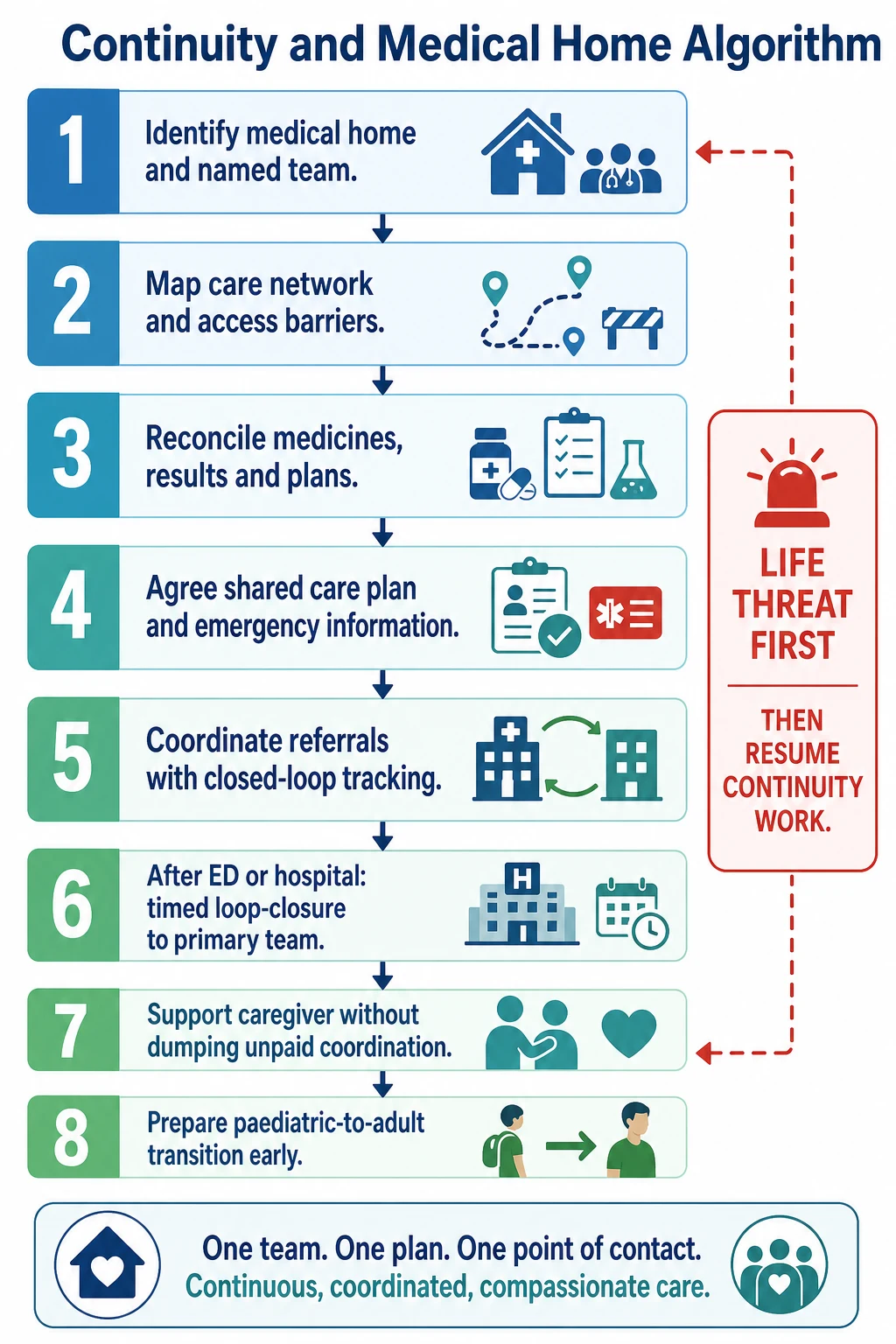
Step 1 — Establish or re-establish the medical home
Assign a named primary clinician or small team. Explain to the family what the medical home will do: preventive care, acute advice route, coordination and advocacy. For children without a usual source of care, disposition from ED or ward must include linkage, not only a discharge script. [2] [20]
Step 2 — Build practice-based care coordination
McAllister and colleagues describe care coordination as a medical-home essential: defined roles, tracking systems, family partnership and proactive planning—not ad hoc heroics. [11]
Turchi’s AAP framework frames patient- and family-centred care coordination across systems, including community services. [12]
Step 3 — Create living documents
- Shared care plan with goals, responsibilities and review date.
- Emergency information form for complex illness.
- Up-to-date medication and device list.
Keep documents short enough to use at 02:00. [11] [13]
Step 4 — Close loops
Every external encounter needs an owner and a time: ED discharge, inpatient discharge, specialty referral, outstanding result. “Faxed somewhere” is not closure. [11] [20]
Step 5 — Match intensity to need
Well children need reliable preventive continuity. Children with special health care needs need scheduled co-management and referral tracking. Children with medical complexity often need dedicated coordination capacity and hospital partnership. [13] [15] [3]
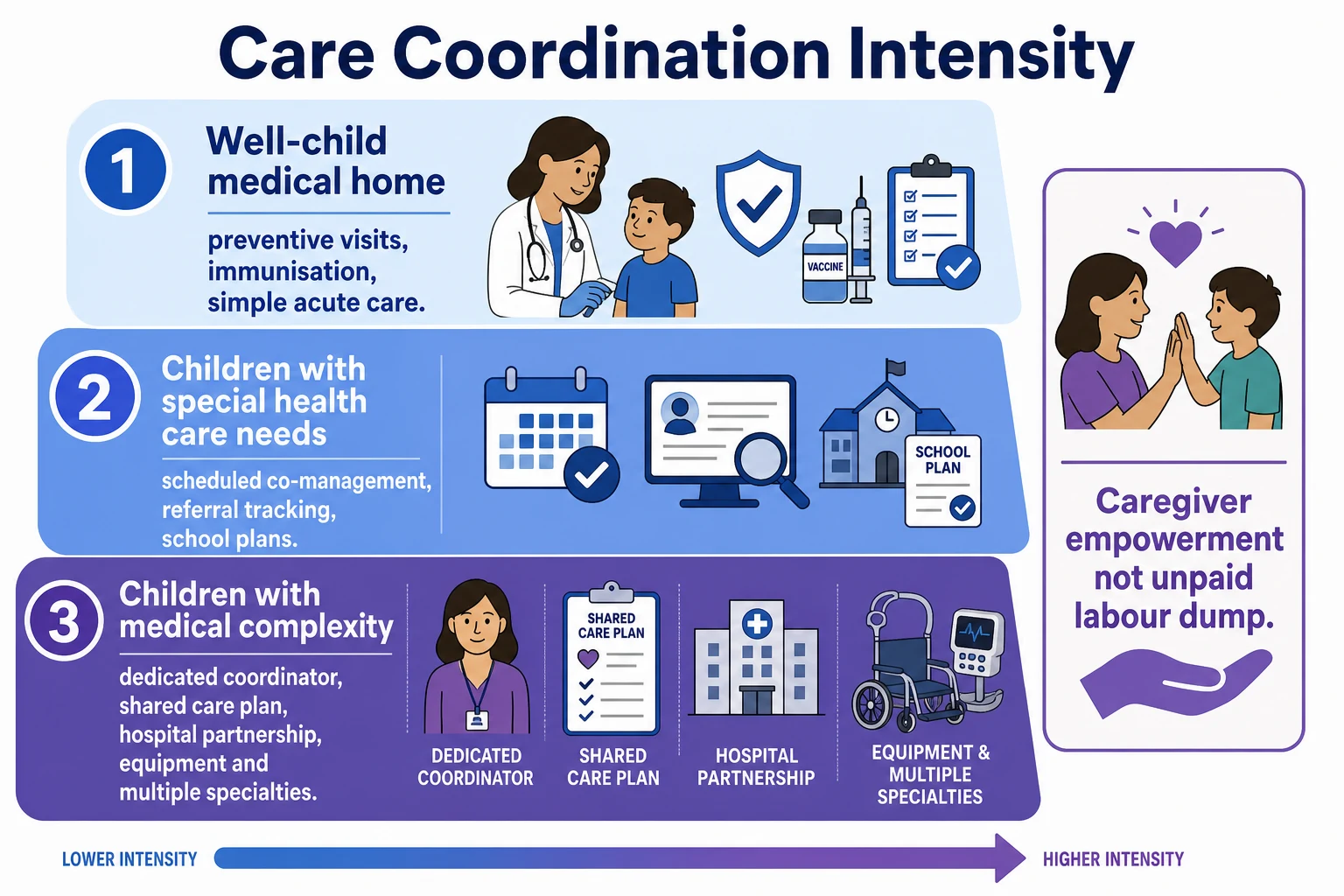
Step 6 — Support caregivers without dumping labour
Invite caregiver expertise. Resource coordination tasks that require system authority. Watch for burnout. Literature on CMC coordination emphasises caregiver empowerment as partnership, not transfer of unpaid clinical work. [16] [13]
Step 7 — Design acute care that feeds the medical home
Non-emergency acute care outside the medical home can be necessary for access. The safety requirement is communication back and alignment with the longitudinal plan. Retail or urgent-care use without loop closure fragments management. [20]
Step 8 — Finance and workforce realism
Sustainable medical homes need payment and staffing models that recognise non-face-to-face coordination time. Price and colleagues outline financing principles for children’s medical homes; local instruments differ by country. Do not invent billing codes in exams—state the principle and the local mechanism. [18] [17]
Step 9 — Measure what matters
Family experience, completed closed-loop referrals, medication reconciliation rates, reduced duplication, continuity with a named clinician, and equity gaps. CMC-specific care-coordination measures exist for programmes that choose formal evaluation. [25] [23] [10]
Specific Subtypes & Scenarios
Newborn and NICU graduate. Book the first medical-home visit before discharge. Transfer growth parameters, pending results, feeding plan and red-flag teaching. [2]
Well child with ED-default behaviour. Explore access barriers and after-hours routes. Rebuild relational continuity rather than only criticising ED use. [20] [4]
Child with special health care needs. Track referrals; unmet specialty care often signals coordination failure. Use family-centred co-management. [22] [35]
Child with medical complexity. Explicit coordinator, emergency form, hospital partnership, polypharmacy review. Kuo frames the “whose care is it?” problem: roles must be explicit across primary, specialty and family. [13] [32]
Hospitalised child. Inpatient teams should identify the medical home on admission day one and send a usable discharge plan, not only a diagnosis list. [32] [11]
Foster and kinship care. Expect incomplete history. Assign a medical home rapidly, catch up preventive care, and communicate with child-protection and caregivers under lawful information-sharing rules. [29] [30]
School-linked care. School-based health centres can expand the medical home if records and plans integrate with primary care; isolated school care can fragment. [31]
Autism and developmental surveillance. Medical-home processes support monitoring and earlier identification pathways when longitudinal observation is organised. [33]
Deaf and hard-of-hearing children. Accessible communication is part of medical-home quality, not an optional courtesy. [34]
Adolescent transition. White’s AAP guidance places structured transition support inside the medical home: preparation, transfer and integration into adult care. [19]
Complications & Pitfalls
- Branding without substance: calling a clinic a medical home while families never see the same clinician. [2] [23]
- Structure without relationship: portals and registries with no continuity person. [23]
- Open-loop referrals: specialty advice that never returns. [11] [22]
- Caregiver as unpaid coordinator for complex care. [13] [16]
- Assuming ED notifies primary care. Build explicit closure. [20]
- Birthday transition without adult service readiness. [19]
- Blaming families for structural barriers. [35] [17]
- Ignoring foster-care discontinuity as expected and therefore acceptable. [30]
- Over-promising complex-care programmes without workforce. [17] [14]
- Duplicate tests and polypharmacy from informational chaos. [1] [12]
Prognosis & Disposition
Paediatric observational data link greater continuity with lower ED utilisation and hospitalisation risk and with better parent-reported quality. Use directional language unless you have the exact study statistics in front of you. [4] [5] [6]
Homer’s evidence review supports medical-home attributes for children with special health care needs, while noting study-quality limits typical of health-services research. [3]
The CCKO randomised trial tested structured care coordination for children with medical complexity in Ontario. Use it as evidence that programme design can be trialled rigorously, and that local implementation details matter; do not over-claim universal outcome magnitudes beyond the paper. [14]
Adult primary-care continuity has been associated with lower mortality in systematic review. Transfer that finding cautiously to paediatrics: it supports the biological and system plausibility of continuity, but children are not small adults in the evidence base. [26] [27]
Disposition rules of thumb: [20] [13]
- Unstable child → acute pathway first.
- Stable child with no medical home → arrange linkage before or at discharge. [20]
- Complex child after admission → timed primary and coordinator follow-up with reconciled plan. [13] [32]
- Transition-age youth → adult service named with overlap plan. [19]
Special Populations
Indigenous children and families. Continuity includes cultural safety, community-controlled services where available, and trust repair after historical and ongoing harm. Do not reduce this to a generic access checklist. [17] [21]
Migrant and refugee families. Interrupted records, catch-up immunisation, interpreter-supported coordination and trauma-aware engagement are medical-home work. [17]
Disability and neurodiversity. Accessible communication, sensory-aware processes and baseline expertise define whether visits are usable. [34] [33]
Out-of-home care and youth justice. High placement mobility demands proactive medical-home assignment and aggressive informational continuity. [29] [30]
Rural and remote. Visiting specialists and telehealth can help only if management continuity and loop closure are designed deliberately. [17]
Socioeconomic disadvantage. Transport, cost, precarious work and after-hours barriers convert theoretically available medical homes into unreachable ones. [21] [17]
Evidence, Guidelines & Regional Differences
Core evidence spine for exams: [1] [3]
- Haggerty continuity domains. [1]
- Christakis paediatric continuity–utilisation associations. [4] [5]
- Homer medical-home evidence for CSHCN. [3]
- Care coordination as medical-home essential and AAP coordination framework. [11] [12]
- CMC coordination roles and CCKO trial. [13] [14]
- Implementation barriers and financing principles. [17] [18]
- Transition in the medical home. [19]
- Non-emergency acute care outside the medical home. [20]
Medical-home language often appears as patient-centred medical home, Health Care Homes, comprehensive GP care, paediatric shared care, Aboriginal Community Controlled Health Services and Māori health models grounded in Te Tiriti and whānau ora. Principles match international continuity science even when programme names differ. State handover and clinical communication standards support informational continuity after hospital care. Avoid inventing current item numbers in an answer; name the local mechanism if known. [1] [17]
GP registration provides a structural usual source of care. Personal relational continuity still varies with rostering and workforce pressure. Named clinician models for vulnerable patients and multidisciplinary primary-care teams map to medical-home functions. MRCPCH tests shared-care reasoning and communication more than US PCMH branding. [1] [27]
AAP policy statements define medical-home, care-coordination and transition expectations. PCMH recognition and Medicaid financing shape implementation. Canadian complex-care programmes, including trial evidence such as CCKO, show that structured coordination can be evaluated. Foster-care medical-home standards and school-based health centres are prominent US extensions. [12] [19] [14] [30] [31]
Controversies to handle cleanly: urgent-care growth versus medical-home ownership; how much outcome gain complex-care teams deliver in which populations; whether structural recognition programmes improve relational continuity; and how far adult continuity–mortality data should influence paediatric policy. [20] [14] [23] [26]
Exam Pearls
- Say relational + informational + management before you say “medical home.” [1]
- A usual source of care ≠ automatic medical home. [2]
- Lower continuity ↔ more ED/hospital use in children—direction matters. [4]
- Care coordination is essential infrastructure, not a soft extra. [11]
- Close every loop: owner, task, time, result route. [11] [20]
- Do not dump coordination onto exhausted caregivers. [13] [16]
- Transition is a years-long process inside the medical home. [19]
- Foster care needs accelerated medical-home assignment. [30]
- Sick now → resuscitate first; continuity second.
- Equity: who never gets a medical home is part of the answer. [21]
References
- [1]Haggerty, Jeannie L Continuity of care: a multidisciplinary review. BMJ (Clinical research ed.), 2003.PMID 14630762
- [2]Sia, Calvin History of the medical home concept. Pediatrics, 2004.PMID 15121914
- [3]Homer, Charles J A review of the evidence for the medical home for children with special health care needs. Pediatrics, 2008.PMID 18829788
- [4]Christakis, D A Association of lower continuity of care with greater risk of emergency department use and hospitalization in children. Pediatrics, 2001.PMID 11230593
- [5]Christakis, D A Is greater continuity of care associated with less emergency department utilization? Pediatrics, 1999.PMID 10103295
- [6]Christakis, Dimitri A Continuity of care is associated with high-quality careby parental report. Pediatrics, 2002.PMID 11927727
- [7]Christakis, Dimitri A Continuity of care is associated with well-coordinated care. Ambulatory pediatrics : the official journal of the Ambulatory Pediatric Association, 2003.PMID 12643780
- [8]Cabana, Michael D Does continuity of care improve patient outcomes? The Journal of family practice, 2004.PMID 15581440
- [9]Jee, Sandra H Indices for continuity of care: a systematic review of the literature. Medical care research and review : MCRR, 2006.PMID 16595410
- [10]Cooley, W Carl The Medical Home Index: development and validation of a new practice-level measure of implementation of the Medical Home model. Ambulatory pediatrics : the official journal of the Ambulatory Pediatric Association, 2003.PMID 12882594
- [11]McAllister, Jeanne W Practice-based care coordination: a medical home essential. Pediatrics, 2007.PMID 17766512
- [12]Turchi, Renee M Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [13]Kuo, Dennis Z Care Coordination for Children With Medical Complexity: Whose Care Is It, Anyway? Pediatrics, 2018.PMID 29496973
- [14]Cohen, Eyal Effectiveness of Structured Care Coordination for Children With Medical Complexity: The Complex Care for Kids Ontario (CCKO) Randomized Clinical Trial. JAMA pediatrics, 2023.PMID 36939728
- [15]de Banate, Mary Ann Care coordination for children with medical complexity. Current opinion in pediatrics, 2019.PMID 31290774
- [16]Van Orne, Julie Care coordination for children with medical complexity and caregiver empowerment in the process: A literature review. Journal for specialists in pediatric nursing : JSPN, 2022.PMID 35671389
- [17]Tschudy, Megan M Barriers to Care Coordination and Medical Home Implementation. Pediatrics, 2016.PMID 27507894
- [18]Price, Jonathan Principles of Financing the Medical Home for Children. Pediatrics, 2020.PMID 31871247
- [19]White, Patience H Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [20]Conners, Gregory P Nonemergency Acute Care: When It's Not the Medical Home. Pediatrics, 2017.PMID 28557775
- [21]Strickland, Bonnie Access to the medical home: results of the National Survey of Children with Special Health Care Needs. Pediatrics, 2004.PMID 15121916
- [22]Boudreau, Alexy Arauz Care coordination and unmet specialty care among children with special health care needs. Pediatrics, 2014.PMID 24864172
- [23]Stille, Christopher J Relationship-focused vs. Structural Activities in Medical Home Measurement in Pediatrics. Maternal and child health journal, 2018.PMID 29926246
- [24]Mohanty, Salini Incorporating Patient- and Family-Centered Care Into Practice: The PA Medical Home Initiative. Pediatrics, 2018.PMID 30135086
- [25]Parast, Layla Validation of New Care Coordination Quality Measures for Children with Medical Complexity. Academic pediatrics, 2018.PMID 29550397
- [26]Baker, Richard Primary medical care continuity and patient mortality: a systematic review. The British journal of general practice : the journal of the Royal College of General Practitioners, 2020.PMID 32784220
- [27]Guthrie, Bruce Continuity of care matters. BMJ (Clinical research ed.), 2008.PMID 18687724
- [28]Haggerty, Jeannie L Experienced continuity of care when patients see multiple clinicians: a qualitative metasummary. Annals of family medicine, 2013.PMID 23690327
- [29]Simms, M D Health care needs of children in the foster care system. Pediatrics, 2000.PMID 11044143
- [30]Szilagyi, Moira A Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416941
- [31]Beem, Angela A School-Based Health Centers as the Pediatric Expanded Medical Home. The Journal of school health, 2019.PMID 31529500
- [32]Russell, Christopher J Care of children with medical complexity in the hospital setting. Pediatric annals, 2014.PMID 24977678
- [33]Barger, Brian Medical Home, Developmental Monitoring/Screening, and Early Autism Identification. Journal of autism and developmental disorders, 2024.PMID 37477840
- [34]Khalsa, Inderpreet Kaur Medical Home Care for Children with Deafness and Hearing Problems. Pediatrics, 2024.PMID 39267599
- [35]Kuhlthau, Karen A Evidence for family-centered care for children with special health care needs: a systematic review. Academic pediatrics, 2011.PMID 21396616