Paeds · ent-hearing-and-oral-health
Neck masses in children
Also known as Cervical lump · Thyroglossal duct cyst · Branchial cleft cyst · Cystic hygroma · Cervical lymphadenopathy · Paediatric neck mass
Fellowship guide to the paediatric neck mass framed around the two questions that drive every assessment — is this congenital, inflammatory or neoplastic, and where does it sit (midline versus lateral, anterior versus posterior triangle, supraclavicular)? Most cervical masses in children are benign reactive lymph nodes, but the discipline is to never miss the malignant one: a hard, fixed, painless, progressively enlarging node, a node in the supraclavicular fossa or posterior triangle, or a node that persists or grows beyond four to six weeks or fails to respond to antibiotics. The congenital midline mass that moves up with swallowing and tongue protrusion is a thyroglossal duct cyst (Sistrunk procedure); the lateral mass is a branchial cleft cyst until proven otherwise; the soft, transilluminating posterior-triangle mass in an infant is a lymphatic malformation. Suppurative lymphadenitis needs antibiotics covering Staphylococcus aureus and group A streptococcus with incision and drainage if an abscess forms; non-tuberculous mycobacterial lymphadenitis needs surgical excision. Ultrasound is the first-line imaging test because it is radiation-free and tissue-characterising; persistent or suspicious masses need ultrasound-guided biopsy and urgent paediatric oncology referral. The red flags that shift a reassuring node into an emergency are airway compromise, drooling, a rapidly enlarging mass, constitutional B symptoms, and any supraclavicular node.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the three-year-old whose mother has found a pea-sized lump in the neck, or the anxious family of a teenager with a month-old node that will not go away. The fellowship task is to resist the two opposite errors — reassuring everything as a reactive node, and over-investigating every benign lump — by applying a disciplined structure that sorts the mass by location and behaviour and identifies the small number that are dangerous. The single skill that anchors the whole topic is knowing which neck mass is benign and self-limiting, and which needs ultrasound, biopsy and a paediatric oncology referral today. [1] [3]
A paediatric neck mass is any palpable swelling in the neck, whether a lymph node, a congenital cyst, a vascular malformation, a salivary or thyroid lesion, or a neoplasm. Cervical lymphadenopathy alone is extraordinarily common — it affects as many as nine in ten children between the ages of four and eight years — and the great majority of these nodes are benign reactive responses to viral upper respiratory infections. The minority that are not benign are what the clinician must find. The most common cause of cervical lymphadenopathy in a child is reactivity to a viral agent; the next most common is bacterial infection (pyogenic, anaerobic or mycobacterial); and the most concerning cause is malignancy. [3] [4]
What makes this a fellowship topic rather than a routine referral is that the same lump can be a self-limiting reactive node in one child and a lymphoma in another, and the bedside assessment — not a blood test — is what separates them at first contact. The candidate who walks to the viva able to classify a mass by location and behaviour, name the congenital and acquired causes, and articulate the red flags for biopsy will handle any neck-mass scenario the examiner can construct. [1] [10]
Classification
Classify a paediatric neck mass by location first, then aetiology, because location alone narrows the differential more than any other single feature and prevents the commonest error of grouping all neck lumps together. Keeping midline and lateral separate, and anterior triangle and posterior triangle separate, is the move that turns an undifferentiated lump into a focused differential in seconds. [1] [2]
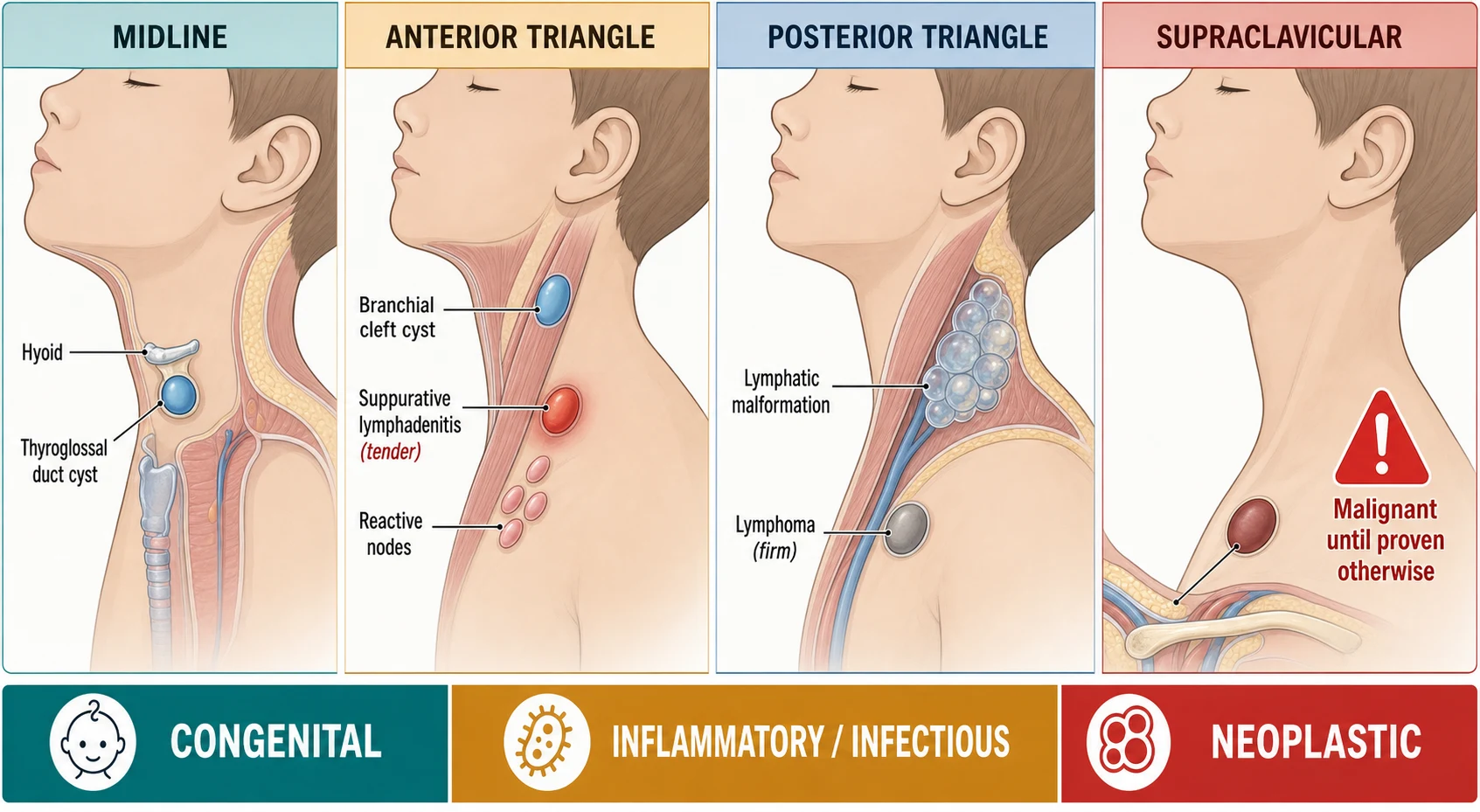
By location, four zones matter. Midline masses are thyroglossal duct cysts (the commonest congenital midline neck mass, typically just below the hyoid), dermoid or epidermoid cysts (more superficial, do not move with swallowing), and thyroid lesions (move with swallowing, lie low in the anterior neck). Lateral masses in the anterior triangle are branchial cleft cysts (the commonest lateral congenital neck mass, classically along the anterior border of the sternocleidomastoid), reactive and suppurative lymph nodes, and enlarged neoplastic nodes. Lateral masses in the posterior triangle include the lymphatic malformation or cystic hygroma (soft, cystic, transilluminating, often present from infancy), lymphoma (especially Hodgkin lymphoma in the adolescent), and in the very young child neuroblastoma. Supraclavicular masses are the zone of highest alarm — a node here is pathologic until proven otherwise, with a high probability of lymphoma or metastatic disease from a thoracic or abdominal primary. [1] [2]
By aetiology, the three buckets are the spine of the topic. Congenital or developmental masses are present from birth even if they declare themselves later, and include the thyroglossal duct cyst, the branchial cleft cyst, the lymphatic malformation, dermoid and epidermoid cysts, teratoma, laryngocele and thymic cyst. Inflammatory or infectious masses are acquired, and span reactive viral lymphadenopathy, suppurative bacterial lymphadenitis, deep neck space abscess, tuberculous and non-tuberculous mycobacterial lymphadenitis, cat scratch disease, Epstein-Barr virus mononucleosis, toxoplasmosis and Kawasaki disease. Neoplastic masses divide into benign (lipoma, neurofibroma, pilomatrixoma) and malignant (lymphoma, leukaemia, rhabdomyosarcoma, thyroid carcinoma, neuroblastoma, nasopharyngeal carcinoma). The congenital-versus-acquired split maps onto behaviour: congenital cysts are painless and slowly growing, inflammatory masses are tender and often acute, and malignant masses are firm, fixed and relentlessly progressive. [3] [4]
The numbers that anchor your viva
Epidemiology & Risk Factors
Cervical lymphadenopathy is one of the most common reasons a child is brought for medical assessment, and the epidemiology is the foundation of the reassurance you offer most families. Palpable cervical nodes are found in up to ninety per cent of children between four and eight years of age, reflecting the intense immunological activity of the cervical lymphatic tissue during the years of greatest viral exposure. Most of these nodes are small (under one to two centimetres), soft, mobile, bilateral and located in the anterior triangle, and they resolve as the intercurrent viral illness resolves. [3] [4]
The risk factors that shift a node from the benign majority into the worrying minority are the epidemiological backbone of the red-flag assessment. Age matters: in infants and young children, congenital lesions (lymphatic malformation, branchial cleft cyst, teratoma, fibromatosis colli) and infections dominate, whereas in adolescents, Hodgkin lymphoma and thyroid carcinoma rise in incidence. Duration and behaviour matter: a node that is hard, fixed, painless, enlarging, located in the supraclavicular fossa or posterior triangle, or that persists beyond four to six weeks or fails to respond to a course of antibiotics is in the high-risk group. Systemic features matter: unexplained fever, drenching night sweats, weight loss, fatigue, pallor, bruising or hepatosplenomegaly are the constitutional B symptoms of lymphoma and leukaemia. Exposure history matters: a kitten scratch suggests cat scratch disease, tuberculosis contact suggests mycobacterial disease, and rural or outdoor exposure in endemic areas brings specific zoonoses into the differential. [3] [9]
Pathophysiology
Understanding why each kind of neck mass arises is the fastest route to remembering its location and behaviour, because embryology and lymphatic drainage predict where a lesion will appear and how it will feel. The three aetiological groups have three different mechanisms, and the candidate who can recite the embryology of the thyroglossal duct and the branchial apparatus, and the lymphatic spread pattern of a supraclavicular node, has the topic by its roots. [5] [6]
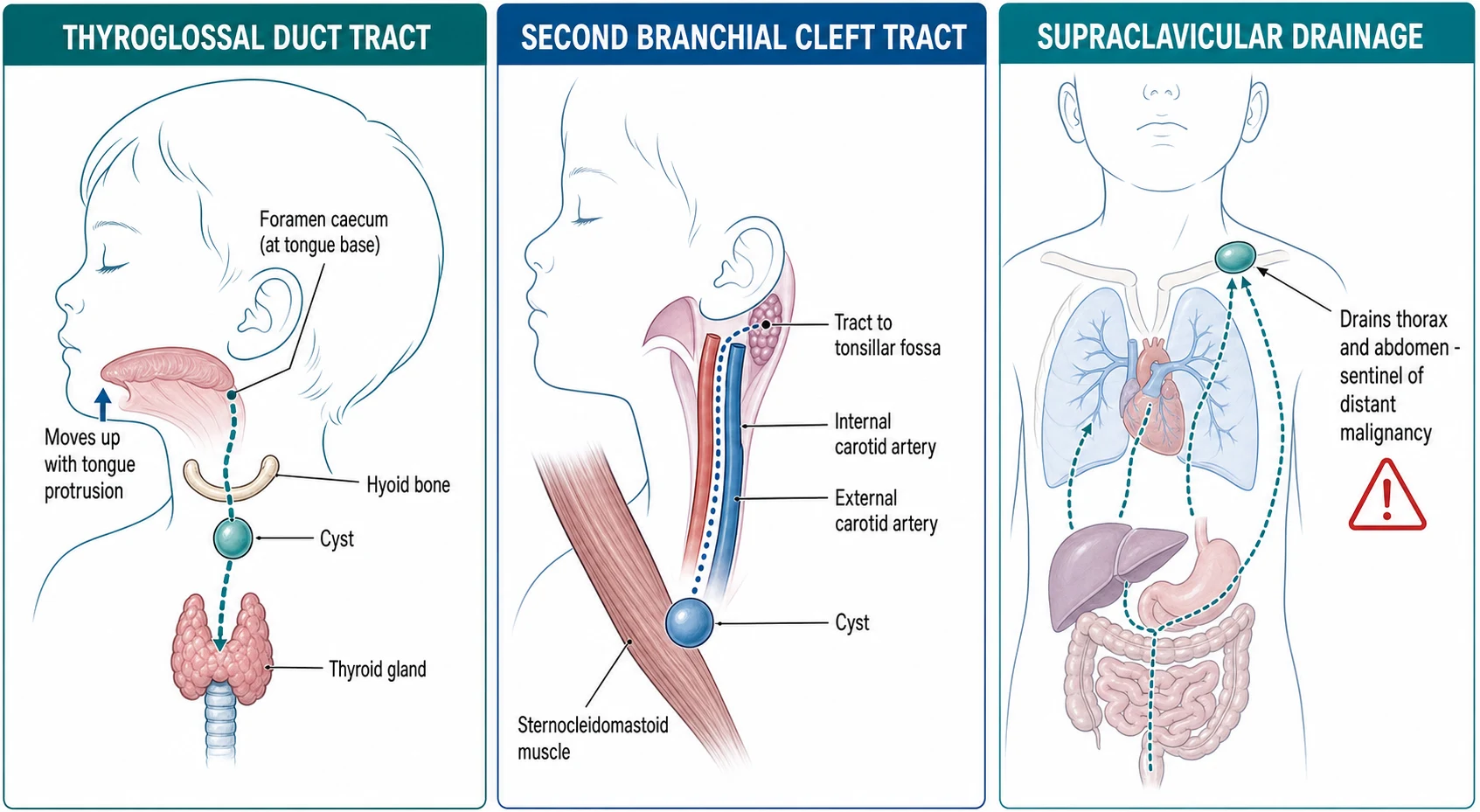
The thyroglossal duct cyst arises from a remnant of the thyroglossal duct, the tract along which the thyroid anlage descends from the foramen caecum at the tongue base to its final pretracheal position during embryogenesis. Because the tract passes through the hyoid bone, a thyroglossal duct cyst classically sits in the midline at or just below the hyoid and moves upward when the child protrudes the tongue or swallows — the single bedside manoeuvre that distinguishes it from a dermoid cyst or a thyroid nodule. Excision must remove the cyst, the tract and the central portion of the hyoid bone up to the foramen caecum (the Sistrunk procedure) or recurrence is likely, because residual tract epithelium will form a new cyst. [5]
The branchial cleft cyst arises from incomplete obliteration of a branchial cleft or pouch. The second branchial cleft accounts for the great majority, producing a smooth, painless, fluctuant swelling along the anterior border of the sternocleidomastoid, with a tract that runs between the internal and external carotid arteries to open into the tonsillar fossa. First branchial cleft anomalies are rarer and present around the ear, the parotid or the angle of the mandible, and can be intimately related to the facial nerve — the International Pediatric Otolaryngology Group consensus stresses careful imaging and surgical planning to protect the nerve. Branchial cysts often present for the first time when they become infected in a school-aged child. [6]
The lymphatic malformation (formerly cystic hygroma) is a benign vascular malformation arising from a developmental error of the lymphatic system, producing dysplastic lymphatic channels that fail to connect to the venous system. They are categorised by cyst size into macrocystic, microcystic and combined forms, which predicts both the clinical feel (the large soft transilluminating mass of a macrocystic lesion in the posterior triangle of an infant) and the treatment (sclerotherapy works well for macrocystic disease, while microcystic and combined disease are harder to treat and may need sirolimus or surgery). They grow with the child, can enlarge suddenly with viral illness or intralesional bleed, and in the neck can compromise the airway or the great vessels. [7]
Inflammatory masses follow the lymphatic drainage of the head and neck. Reactive viral lymphadenopathy reflects the normal immune response of the cervical nodes to viral antigens; suppurative bacterial lymphadenitis follows pyogenic infection (most often Staphylococcus aureus and group A streptococcus) that overwhelms the node to produce pus and abscess; and mycobacterial lymphadenitis reflects chronic granulomatous infection of the node, with non-tuberculous mycobacteria producing the characteristic unilateral, chronic, violet-grey, painless node in a young, otherwise well child. Neoplastic masses arise either primarily in the node (lymphoma, leukaemia) or by metastatic spread along lymphatic drainage — which is why a supraclavicular node, draining the thorax, abdomen and pelvis, is the classic sentinel of distant malignancy. [8] [10]
Clinical Presentation
The presentation of a neck mass is the story that lets you sort it before you touch it. A reactive node comes with the cold, sits in the anterior triangle, is tender and bilateral and resolves in two weeks; a congenital cyst has been there for months, is painless and slowly growing; a malignant node is hard, fixed and painless and is getting bigger. Training the history to extract these features is how the bedside assessment earns its keep. [3] [4]
Reactive and infectious masses present acutely. Viral reactive lymphadenopathy accompanies an upper respiratory infection with tender, mobile, bilateral anterior-cervical nodes of under two centimetres that resolve over one to three weeks. Suppurative bacterial lymphadenitis presents more dramatically with a unilateral, tender, enlarged, erythematous node, fever and systemic upset, and may progress to a fluctuant abscess. A deep neck space abscess — retropharyngeal or parapharyngeal — presents with fever, neck stiffness, torticollis, drooling, a muffled voice and a toxic child, often following a sore throat. Cat scratch disease presents with a tender regional node (classically axillary or cervical) appearing one to three weeks after a kitten scratch, with mild systemic symptoms. Non-tuberculous mycobacterial lymphadenitis presents chronically in an otherwise well child aged one to five years as a unilateral, painless, enlarging cervical node with characteristic violet-grey overlying skin discolouration. [9] [8]
Congenital masses present painlessly and progressively. A thyroglossal duct cyst presents as a midline or paramedian cystic mass at or below the hyoid that moves upward with tongue protrusion and swallowing, often first noticed after an upper respiratory infection, and it may become infected and discharge. A branchial cleft cyst presents as a painless fluctuant mass along the anterior border of the sternocleidomastoid, often presenting acutely when it becomes infected. A lymphatic malformation presents in infancy as a large, soft, cystic, transilluminating mass in the posterior triangle or floor of the mouth that can compromise the airway. Fibromatosis colli (sternocleidomastoid tumour of infancy) presents in the first weeks of life as a firm, painless mass within the sternocleidomastoid with ipsilateral head tilt and restricted rotation — congenital muscular torticollis. [5] [7] [11]
Neoplastic masses present in ways the clinician must not miss. Lymphoma presents with a firm or rubbery, painless, progressively enlarging node — Hodgkin lymphoma in the adolescent, typically contiguous spread from cervical to supraclavicular to mediastinal nodes, with or without the B symptoms of fever, drenching night sweats and weight loss; non-Hodgkin lymphoma including Burkitt lymphoma in younger children, often with rapid growth and extranodal disease. Leukaemia presents with adenopathy alongside pallor, bruising, fatigue and hepatosplenomegaly. Rhabdomyosarcoma and thyroid carcinoma present as firm masses that may grow rapidly; a thyroid nodule in a child is more likely to be malignant than in an adult and needs thorough evaluation. [10] [3]
Differential Diagnosis
The differential of a paediatric neck mass collapses quickly once you apply location, behaviour and age — the skill is to keep the must-not-miss causes at the top of the list rather than buried in a long recitation of cysts. The table below organises the differential by location so the bedside assessment can be converted into a focused list. [1] [2]
Differential diagnosis by neck location
The discriminating features worth memorising are the ones that separate benign from malignant at the bedside. A node that is soft, mobile, tender and bilateral in a child with a viral illness is benign; a node that is hard, fixed, painless, unilateral and enlarging is malignant until proven otherwise. A midline mass that moves with tongue protrusion is a thyroglossal duct cyst; one that does not is a dermoid or thyroid lesion. A lateral mass that is soft and transilluminates in an infant is a lymphatic malformation; one that is fluctuant and along the sternocleidomastoid is a branchial cleft cyst; one that is tender and erythematous is suppurative lymphadenitis. [3] [5]
Clinical & Bedside Assessment
The bedside assessment of a neck mass is a structured examination that converts location and behaviour into a triage decision, and it is the single most examined skill in this topic. Approach it in the same order every time — look, feel, move, then look at the rest of the child — so that no zone is missed and the malignant features are actively sought rather than stumbled upon. [1] [3]
Begin with inspection: note the site, size, overlying skin (erythema suggests infection; violet-grey discoloration suggests non-tuberculous mycobacteria; a punctum suggests a dermoid; dilated veins suggest a mediastinal component or superior vena cava compression), and whether the child holds the neck stiff (suggesting a deep neck abscess or retropharyngeal collection). Position the child sitting up and expose the whole neck, the supraclavicular fossae and the axillae. [12]
On palpation, characterise every mass systematically: site (midline versus lateral, anterior versus posterior triangle, supraclavicular), size, consistency (soft, rubbery, firm or hard, cystic or solid), fixation to skin or deep structures, fluctuance and transillumination, tenderness, and whether nodes are discrete or matted. Then examine the regional and distant node groups — submental, submandibular, preauricular, occicular, axillary, supraclavicular, infraclavicular and inguinal — because generalised lymphadenopathy with hepatosplenomegaly points to a systemic process such as leukaemia or lymphoma, while a single, isolated, hard node points to a primary neoplasm. [3] [4]
Two provocative manoeuvres complete the bedside exam. Ask the child to protrude the tongue and to swallow: a thyroglossal duct cyst moves upward with both, confirming its attachment to the hyoid and the foramen caecum. Examine the oropharynx and look for a tonsillar or pharyngeal primary, and palpate the thyroid and salivary glands. Always take the temperature and look for systemic features — fever, pallor, bruising, weight loss, night sweats — because these shift the assessment from a likely-benign node to a mandatory work-up for malignancy or systemic infection. A child who looks well with a small, soft, tender node has a reactive node until proven otherwise; a child who looks unwell, or who has a node in the supraclavicular fossa or posterior triangle, has a serious disease until proven otherwise. [3] [10]
Investigations
The investigation of a paediatric neck mass is guided by the bedside assessment and is deliberately conservative for the benign majority and decisive for the worrying minority. Ultrasound is the first-line test because it avoids radiation, characterises cystic versus solid tissue, defines vascularity and is well tolerated; cross-sectional imaging and tissue sampling follow only when the ultrasound or the clinical picture demands it. [2] [3]
Ultrasound is the cornerstone of the paediatric neck-mass work-up. It distinguishes cystic from solid lesions (thyroglossal and branchial cysts are cystic; neoplastic nodes are solid), defines the size, shape, internal architecture and vascularity of a node, and identifies abscess formation. It is the test to request for any neck mass that is not a straightforward reactive node in a well child — congenital cysts, suspicious or persistent nodes, and lesions in the supraclavicular fossa or posterior triangle all warrant ultrasound as the first step. [2]
Cross-sectional imaging with contrast-enhanced computed tomography or magnetic resonance imaging is reserved for the deep neck space abscess, for the complex vascular malformation, and for staging a confirmed or suspected malignancy. Contrast CT of the neck is the test of choice for a suspected retropharyngeal or parapharyngeal abscess, where it defines the collection and guides drainage; MRI is preferred for a lymphatic or vascular malformation and for tumour staging because it defines the relationship to vital structures without radiation. [2] [12]
Tissue sampling and laboratory tests are driven by the clinical picture. For a suspicious node — firm, fixed, painless, enlarging, persistent beyond four to six weeks, supraclavicular, or accompanied by B symptoms — the pathway is ultrasound-guided fine-needle aspiration or core biopsy, and if lymphoma is suspected, excisional biopsy of an intact node for histology, flow cytometry and molecular studies, with urgent paediatric oncology referral. For suspected infection, a full blood count, inflammatory markers and blood cultures support the diagnosis of suppurative lymphadenitis; for mycobacterial disease, tuberculin skin test or interferon-gamma release assay, chest radiograph and aspiration or biopsy for acid-fast bacilli, culture and polymerase chain reaction distinguish tuberculous from non-tuberculous disease. For a midline mass, thyroid function tests and a thyroid ultrasound locate and characterise any thyroid component before surgery. [8] [3]
Management — Resuscitation
Most paediatric neck masses are not emergencies, and the resuscitation skill in this topic is recognising the small number that are — the deep neck abscess threatening the airway, the rapidly enlarging mass, and the lymphatic malformation with airway compromise — and acting on them first. The resuscitation priority is always the airway, then sepsis, then the mass itself. [12]
For a child with a deep neck space abscess (retropharyngeal or parapharyngeal), the airway is the first concern. Keep the child sitting upright in a position of comfort, do not force oropharyngeal examination, and involve anaesthetics and otolaryngology urgently. Obtain intravenous access, take blood cultures and inflammatory markers, and start broad-spectrum intravenous antibiotics covering group A streptococcus, oral anaerobes and Staphylococcus aureus (for example ceftriaxone plus metronidazole, or clindamycin). Arrange urgent contrast-enhanced CT of the neck once the child is stabilised, with a low threshold for surgical drainage if the abscess is large, if there is airway compromise, or if the child fails to improve on antibiotics. [12] [4]
For a child with a rapidly enlarging mass, stridor, or superior vena cava syndrome — a haemorrhage into a lymphatic malformation, a rapidly growing tumour, or a mediastinal mass with airway compression — the priority is airway protection in a controlled setting with anaesthetic and otolaryngology or oncology input, followed by urgent imaging. Do not sedate or lie the child flat if the airway is precarious. For a child with suspected severe infection or sepsis from suppurative lymphadenitis, follow paediatric sepsis pathways with fluid resuscitation, intravenous antibiotics and source control. [12]
Management — Definitive & Stepwise
Definitive management maps onto the aetiological buckets, and the fellowship candidate should be able to state the first-line treatment for each cause. The stepwise principle is to treat infection with antibiotics and drainage, to remove congenital cysts electively once infection is controlled, and to refer every suspicious or confirmed malignancy to paediatric oncology for staging and protocol therapy. [1] [3]
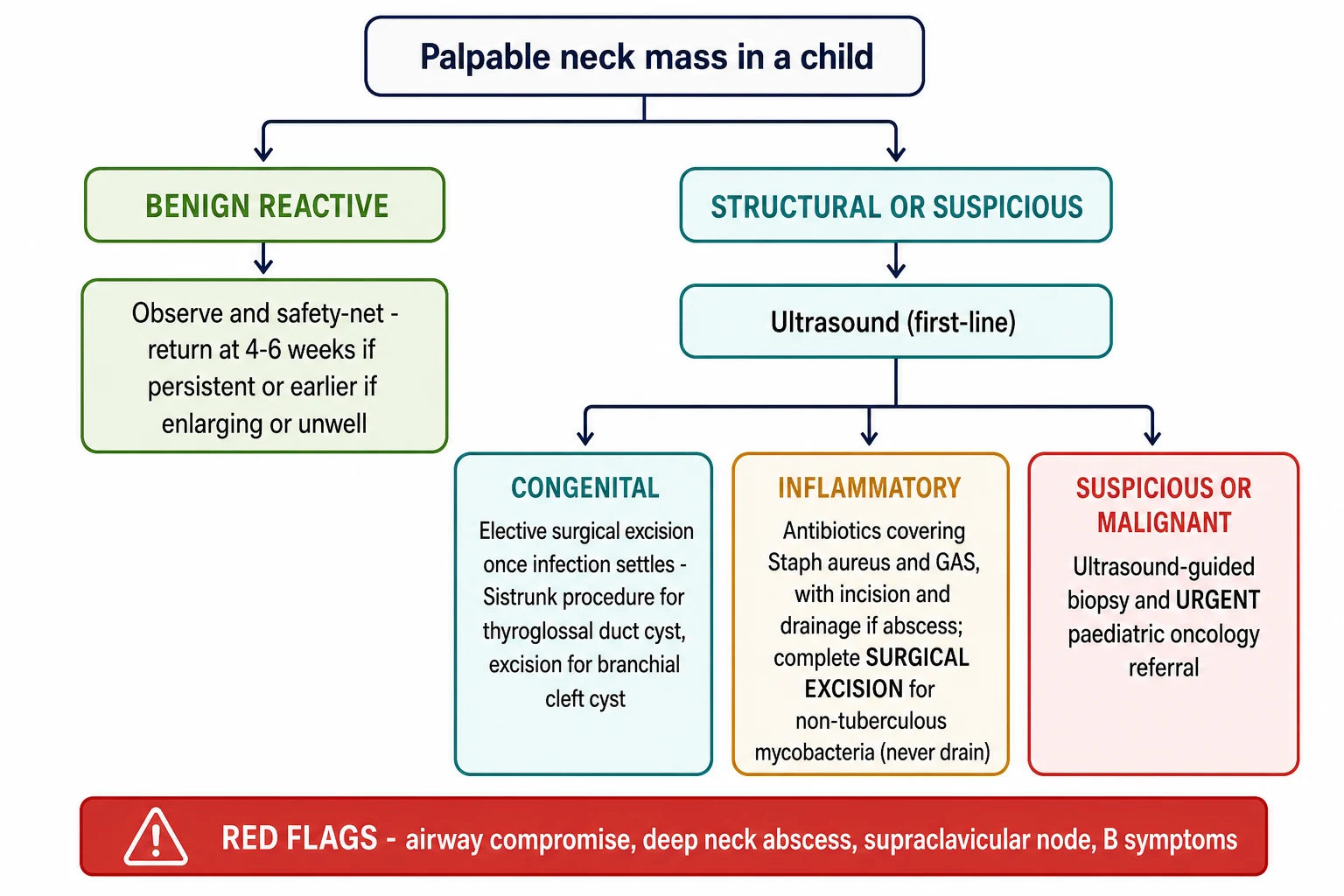
For reactive viral lymphadenopathy, no specific treatment is needed beyond reassurance, analgesia and a clear safety-net to return if the node enlarges, persists beyond two to four weeks, or the child becomes systemically unwell. Over-investigation and antibiotic prescribing for uncomplicated viral nodes is a stewardship error. [3]
For suppurative bacterial lymphadenitis, first-line treatment is an oral antibiotic active against Staphylococcus aureus and group A streptococcus — for example cephalexin, dicloxacillin or clindamycin (the latter covering methicillin-resistant Staphylococcus aureus where prevalence is high) — with intravenous antibiotics for a toxic child or a child who fails oral therapy. If an abscess has formed, incision and drainage is the definitive source control, with culture of the pus to guide therapy. [4]
For non-tuberculous mycobacterial lymphadenitis, the International Pediatric Otolaryngology Group consensus recommends complete surgical excision as definitive treatment, because incision and drainage or inadequate excision risks a chronic discharging sinus and recurrence, and medical therapy alone is less effective. When complete excision is not possible because of the risk to the facial nerve or skin, a course of clarithromycin-based multidrug therapy may be used. For tuberculous lymphadenitis, the treatment is standard antitubercular therapy, with excision reserved for refractory disease. For cat scratch disease, most cases are self-limiting and need only symptomatic care; azithromycin is considered for severe or systemic disease or painful adenopathy. [8] [9]
For congenital cysts, the principle is elective surgical excision once any acute infection has been treated and settled, both to prevent recurrent infection and to obtain histological confirmation. A thyroglossal duct cyst is removed by the Sistrunk procedure — excision of the cyst together with the central portion of the hyoid bone and the tract up to the foramen caecum — because leaving tract behind is the main cause of recurrence. A branchial cleft cyst is excised in its entirety, with care for the tract to the pharyngeal wall and for the facial nerve in first cleft anomalies. A lymphatic malformation is managed according to type and symptoms: macrocystic disease responds to image-guided sclerotherapy (for example doxycycline, bleomycin or OK-432), microcystic and combined disease may need sirolimus (oral mTOR inhibition) or surgery, and a lesion compromising the airway is an emergency needing a multidisciplinary vascular-anomalies team. Fibromatosis colli is managed conservatively with physiotherapy and stretching, which is effective in the great majority of infants; the American Physical Therapy Association guideline supports early, structured conservative management. [5] [6] [7] [11]
For a suspected or confirmed malignancy, the definitive management is urgent referral to paediatric oncology for staging biopsy, imaging and risk-stratified protocol therapy — chemotherapy for lymphoma and leukaemia, and combined-modality therapy as guided by national cooperative-group protocols. The first-contact clinician's job is not to stage the tumour but to recognise it, obtain tissue safely, and refer without delay. [10]
Specific Subtypes & Scenarios
Several presentations recur in exams and in practice because they crystallise a decision, and the candidate should be able to walk through each as a scenario. These are the subtypes that examiners reach for because each tests a different skill — congenital recognition, infection management, or malignancy triage. [1] [3]
The infant with a posterior-triangle mass is a lymphatic malformation until proven otherwise. A soft, cystic, transilluminating mass present from early infancy, growing with the child and enlarging with intercurrent viral illness, raises a lymphatic malformation; the urgency is the airway, because a large malformation in the floor of the mouth or neck can compromise it. Ultrasound and MRI define the lesion, and management is by a vascular-anomalies team using sclerotherapy, sirolimus or surgery according to the cyst type and symptoms. [7]
The toddler with a chronic unilateral node is the classic non-tuberculous mycobacterial scenario. An otherwise well child aged one to five years with a unilateral, painless, slowly enlarging cervical node, often with the characteristic violet-grey overlying skin discolouration and minimal systemic upset, has non-tuberculous mycobacterial lymphadenitis. The pitfall is incision and drainage, which creates a chronic sinus — the correct management is complete surgical excision. Distinguish this from tuberculous lymphadenitis (which needs antitubercular therapy) using the tuberculin test, interferon-gamma release assay and culture. [8]
The school-aged child with an infected midline cyst is a thyroglossal duct cyst that has become infected. Treat the infection first with antibiotics (and drainage if there is an abscess), let it settle, and then plan the Sistrunk procedure as an elective operation. Confirming thyroid function and a normally located thyroid gland beforehand is essential, because a thyroglossal duct cyst can occasionally be the only functioning thyroid tissue. [5]
The adolescent with a supraclavicular node is the must-not-miss scenario. A painless, firm, fixed, progressively enlarging node in the supraclavicular fossa or low posterior triangle, with or without night sweats, fever and weight loss, is Hodgkin lymphoma until proven otherwise. The pathway is urgent ultrasound-guided biopsy and paediatric oncology referral; a chest radiograph is obtained early to look for a mediastinal mass, and the biopsy and staging are coordinated by the oncology team. [10]
The neonate with a sternocleidomastoid mass and head tilt is fibromatosis colli (congenital muscular torticollis). A firm, painless mass within the sternocleidomastoid in the first weeks of life, with ipsilateral head tilt and restricted rotation, is confirmed by ultrasound; management is conservative physiotherapy and stretching, with the great majority resolving without surgery. Examine the hips and the spine, because developmental dysplasia of the hip and skeletal anomalies are associated. [11]
Complications & Pitfalls
The complications and pitfalls of this topic are the ways a child comes to harm when the assessment is not disciplined — by missing a malignancy, by draining a mycobacterial node, or by being reassured about an enlarging cyst. Naming these errors is how a fellowship candidate shows depth, because the examiner is testing whether you know where the topic fails as well as where it succeeds. [3] [8]
The most dangerous pitfall is reassuring or re-prescribing antibiotics for a persistent, enlarging, firm or supraclavicular node, thereby delaying the diagnosis of lymphoma or leukaemia. The defence is the four-to-six-week rule and the biopsy threshold: any node that persists, grows, fails to respond to a course of antibiotics, or sits in the supraclavicular fossa or posterior triangle is investigated with ultrasound and tissue sampling, not treated empirically a second time. [3] [10]
A second classic pitfall is incising and draining a non-tuberculous mycobacterial node under the impression that it is a pyogenic abscess. Incision and drainage in NTM disease produces a chronic discharging sinus that is then far harder to manage; the correct treatment is complete surgical excision. The clue is the otherwise well child, the chronic unilateral course, the minimal systemic upset, and the violet-grey overlying skin — features that distinguish it from the tender, erythematous, febrile child with suppurative bacterial lymphadenitis. [8]
Further pitfalls include missing the airway in a deep neck abscess or a large lymphatic malformation by forcing examination or lying the child flat; treating a thyroglossal duct cyst with simple enucleation rather than the Sistrunk procedure, which leaves tract behind and leads to recurrence; treating a branchial cleft cyst during acute infection rather than after it has settled, which increases the risk of nerve injury and incomplete excision; and forgetting to check thyroid function and thyroid position before excising a thyroglossal duct cyst, in case the cyst contains the only functioning thyroid tissue. Each of these is prevented by applying the structure of the topic rather than acting on a single impression. [5] [6] [12]
Prognosis & Disposition
The prognosis of a paediatric neck mass depends almost entirely on its cause, and the disposition decision — observe, refer electively, or escalate urgently — is where the bedside assessment pays off. Most children do well because most masses are benign; the few who do not are the ones the disciplined assessment identifies early. [1] [3]
The prognosis of reactive viral lymphadenopathy is excellent, with resolution over weeks and no sequelae. Suppurative lymphadenitis resolves with antibiotics and drainage, though recurrent or atypical infection should prompt reconsideration of an underlying congenital cyst or immunodeficiency. Non-tuberculous mycobacterial lymphadenitis resolves with complete surgical excision, with a good cosmetic and functional outcome when the facial nerve is preserved. Congenital cysts are cured by complete surgical excision, with recurrence confined largely to inadequate excision of a thyroglossal duct tract. Lymphatic malformations have a variable prognosis depending on type and extent: macrocystic disease responds well to sclerotherapy, while microcystic and combined disease may need multimodal therapy over years, and airway compromise at presentation is the major determinant of early outcome. Lymphoma and leukaemia carry a prognosis determined by histology and stage, and contemporary risk-stratified paediatric protocols have made survival excellent for most paediatric lymphomas, provided the diagnosis is not delayed. [8] [7] [10]
Special Populations
Several populations need a different threshold for investigation and referral, because their pre-test probability of serious disease is shifted by biology, exposure or access. Recognising these groups is part of equitable care and is rewarded in the exam as an awareness of context. [8] [10]
Immunocompromised children — those on chemotherapy, after transplant, with primary immunodeficiency, or with advanced HIV infection — can present with an opportunistic cervical mass (fungal, mycobacterial, or malignant) that would be rare in an immunocompetent child. The threshold to image and biopsy is lower, and the differential is broader. Infants carry a higher probability that a neck mass is congenital (lymphatic malformation, branchial cleft cyst, teratoma, fibromatosis colli) or a serious infant tumour (neuroblastoma, rhabdomyosarcoma), so ultrasound is early and the index of suspicion is high. Adolescents carry a higher probability of Hodgkin lymphoma and thyroid carcinoma, so a persistent node or thyroid nodule is investigated promptly. [3] [10]
Evidence, Guidelines & Regional Differences
The evidence backbone for paediatric neck masses is built on clinical-review and consensus sources rather than single randomised trials, because the strength of this topic lies in structured assessment and in the consensus of paediatric otolaryngology and oncology groups. The candidate who can name the consensus statements and the key review shows depth by anchoring the practice in named evidence. [1] [2]
The overview and classification evidence rests on the Curtis and Edwards review of paediatric neck masses, which frames the topic around location and aetiology, and the Ho review of imaging guidelines, which establishes ultrasound as the first-line modality. The lymphadenopathy evidence rests on the Weinstock and the Rosenberg reviews of paediatric cervical lymphadenopathy, which establish the epidemiology (up to ninety per cent of children aged four to eight), the viral-reactive majority, the bacterial minority and the malignancy alarm features. [1] [2] [3] [4]
The disease-specific consensus evidence is the strength of the topic. The International Pediatric Otolaryngology Group consensus on first branchial cleft anomalies sets the standard for the classification and facial-nerve-aware surgical management of these rare lesions. The IPOG consensus on non-tuberculous mycobacterial cervicofacial lymphadenitis establishes complete surgical excision as the definitive treatment and warns against incision and drainage. The Elluru review of lymphatic malformations defines the macrocystic, microcystic and combined classification that drives sclerotherapy versus sirolimus versus surgery. The APTA clinical practice guideline on congenital muscular torticollis supports early structured conservative physiotherapy for fibromatosis colli. The Kelly and Friedberg review frames the contemporary management of classic Hodgkin lymphoma in adolescents and young adults. [6] [8] [7] [11] [10]
The live areas of nuance are the precise biopsy threshold (most guidelines converge on persistence beyond four to six weeks, or earlier for supraclavicular or otherwise suspicious nodes), the role of sirolimus for complex lymphatic malformations (an expanding evidence base from the slow-flow-malformation trials), the choice between sclerotherapy agents for macrocystic disease, and the balance of surgical excision against medical therapy for NTM disease when complete excision would endanger the facial nerve. A fellowship candidate shows depth by naming the guideline and the trade-off rather than reciting a single line. [7] [8]
Exam Pearls
The single discipline that keeps children safe is the same one that earns fellowship marks: classify the neck mass by location and behaviour at the bedside, ultrasound the ones that are not straightforward reactive nodes, biopsy and refer urgently the ones that are persistent, firm, fixed, supraclavicular or accompanied by B symptoms, and never miss the malignant node behind the reassurance that most lumps are benign. [1] [3]
And when you teach this topic, teach it as a model of structured clinical reasoning — a common complaint where the default is reassurance for the majority, but where the rare child whose node is a lymphoma depends on you having looked at the location, felt the consistency, and recognised the shift from routine to urgent. [10] [8]
References
- [1]Curtis WJ, Edwards SP. Pediatric neck masses. Atlas Oral Maxillofac Surg Clin North Am, 2015.PMID 25707561
- [2]Ho ML. Pediatric Neck Masses: Imaging Guidelines and Recommendations. Radiol Clin North Am, 2022.PMID 34836558
- [3]Weinstock MS, Patel NA, Smith LP. Pediatric Cervical Lymphadenopathy. Pediatr Rev, 2018.PMID 30171054
- [4]Rosenberg TL, Nolder AR. Pediatric cervical lymphadenopathy. Otolaryngol Clin North Am, 2014.PMID 25213279
- [5]Amos J, Sutton AE, Shermetaro C. Thyroglossal Duct Cyst. StatPearls, 2026.PMID 30085599
- [6]Heilingoetter AL, See GB, Brookes J, et al. Comprehensive management and classification of first branchial cleft anomalies: an International Pediatric Otolaryngology Group (IPOG) consensus statement. Int J Pediatr Otorhinolaryngol, 2024.PMID 39278130
- [7]Elluru RG, Balakrishnan K, Padua HM. Lymphatic malformations: diagnosis and management. Semin Pediatr Surg, 2014.PMID 25241095
- [8]Roy CF, Balakrishnan K, Boudewyns A, et al. International Pediatric Otolaryngology Group: consensus guidelines on the diagnosis and management of non-tuberculous mycobacterial cervicofacial lymphadenitis. Int J Pediatr Otorhinolaryngol, 2023.PMID 36764081
- [9]Klotz SA, Ianas V, Elliott SP. Cat-scratch Disease. Am Fam Physician, 2011.PMID 21243990
- [10]Kelly KM, Friedberg JW. Classic Hodgkin Lymphoma in Adolescents and Young Adults. J Clin Oncol, 2024.PMID 37983570
- [11]Sargent B, Coulter C, Cannoy J, et al. Physical Therapy Management of Congenital Muscular Torticollis: a 2024 evidence-based clinical practice guideline from the American Physical Therapy Association Academy of Pediatric Physical Therapy. Pediatr Phys Ther, 2024.PMID 39356257
- [12]Esposito S, De Guido C, Pappalardo M, et al. Retropharyngeal, parapharyngeal and peritonsillar abscesses. Children (Basel), 2022.PMID 35626793