Paeds · fetal-neonatal-and-perinatal
Apnoea of prematurity
Also known as Apnea of prematurity · Neonatal apnoea · Prematurity apnoea · Caffeine-responsive apnoea · Mixed neonatal apnoea
Fellowship guide to apnoea of prematurity — the definition and the three physiological types, the immature brainstem and chemoreceptor pathophysiology, the caffeine-first stepwise management, and the pitfalls that turn a self-limiting developmental phenomenon into a missed sepsis or an unsafe discharge.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Walk onto the neonatal unit at three in the morning and the question is almost always the same. A baby born at 26 weeks, now four days old, has set off the alarm — the monitor shows a flat breathing trace and a heart rate falling toward 70. The team moves through it from memory: a flick of the foot, a gentle rub, and the numbers climb back. This is apnoea of prematurity, the most common breathing disorder of the very preterm infant, and the skill lies not in the rescue but in deciding when the pause is benign immaturity and when it is sepsis in disguise. [4]
The definition examiners want is precise and worth memorising word for word. Apnoea of prematurity is a cessation of breathing lasting 20 seconds or longer, or a shorter pause accompanied by bradycardia (a heart rate below 80 beats per minute), central cyanosis, or an oxygen desaturation below roughly 80 to 85 percent. It is a diagnosis of developmental immaturity, made in an infant born before 37 weeks, emerging after the first 24 hours of life, and expected to resolve by 43 to 44 weeks postmenstrual age. Crucially, it is a label you can only apply once you have excluded the things that mimic it. [4] [12]
The distinction that catches candidates is the one between apnoea and periodic breathing. Periodic breathing is a benign immature pattern of at least three pauses, each lasting more than three seconds, separated by less than 20 seconds of normal breathing, with no bradycardia and no colour change. You reassure the parents and do not treat it. Apnoea, by contrast, carries physiological consequences and warrants intervention, because the recurrent dips in oxygen that accompany it are what you are really trying to prevent. [4]
Epidemiology & Risk Factors
Picture the gradient and you will never confuse the common with the rare. Apnoea of prematurity affects nearly every infant born before 28 weeks, around half of those born at 29 to 32 weeks, and fewer than one in ten at 34 to 35 weeks. The relationship is inverse and relentless — the earlier the gestational age and the lower the birth weight, the more frequent, severe, and prolonged the events. A 24-week infant is expected to apnoeise; a 36-week infant is not, and when they do, you reach for the septic screen before the caffeine. [4]
Onset typically falls in the first two to three days after birth, and resolution tracks the maturation of the brainstem. Most infants are free of events by 34 to 36 weeks postmenstrual age, though the most extremely preterm may continue to 43 or even 44 weeks. The duration of treatment is therefore individual — you wean and stop when the infant is developmentally ready, not when a fixed number of days has passed. [1]
What turns a self-limiting phenomenon into a crisis is the secondary cause that superimposes itself on an immature drive. Sepsis, hypothermia, hypoglycaemia, anaemia, intraventricular haemorrhage, a patent ductus arteriosus, and central nervous system depressants — opiates, magnesium sulphate, anaesthetics — all depress a respiratory centre that is already struggling. Reflux is invoked far more often than the evidence justifies. When the apnoea pattern changes, the question to ask is not how much caffeine to give but what has gone wrong in the last 12 hours. [4]
Pathophysiology
To understand why caffeine works, picture the preterm brainstem as a conductor who has not yet learned to keep the beat. The respiratory centre fires with an irregular rhythm and weak central drive, so the apnoeic threshold for carbon dioxide sits perilously close to the resting level — a tiny shift and breathing stops. This immaturity of central pattern generation is the engine of central apnoea, the purest form in which effort simply ceases. [4]
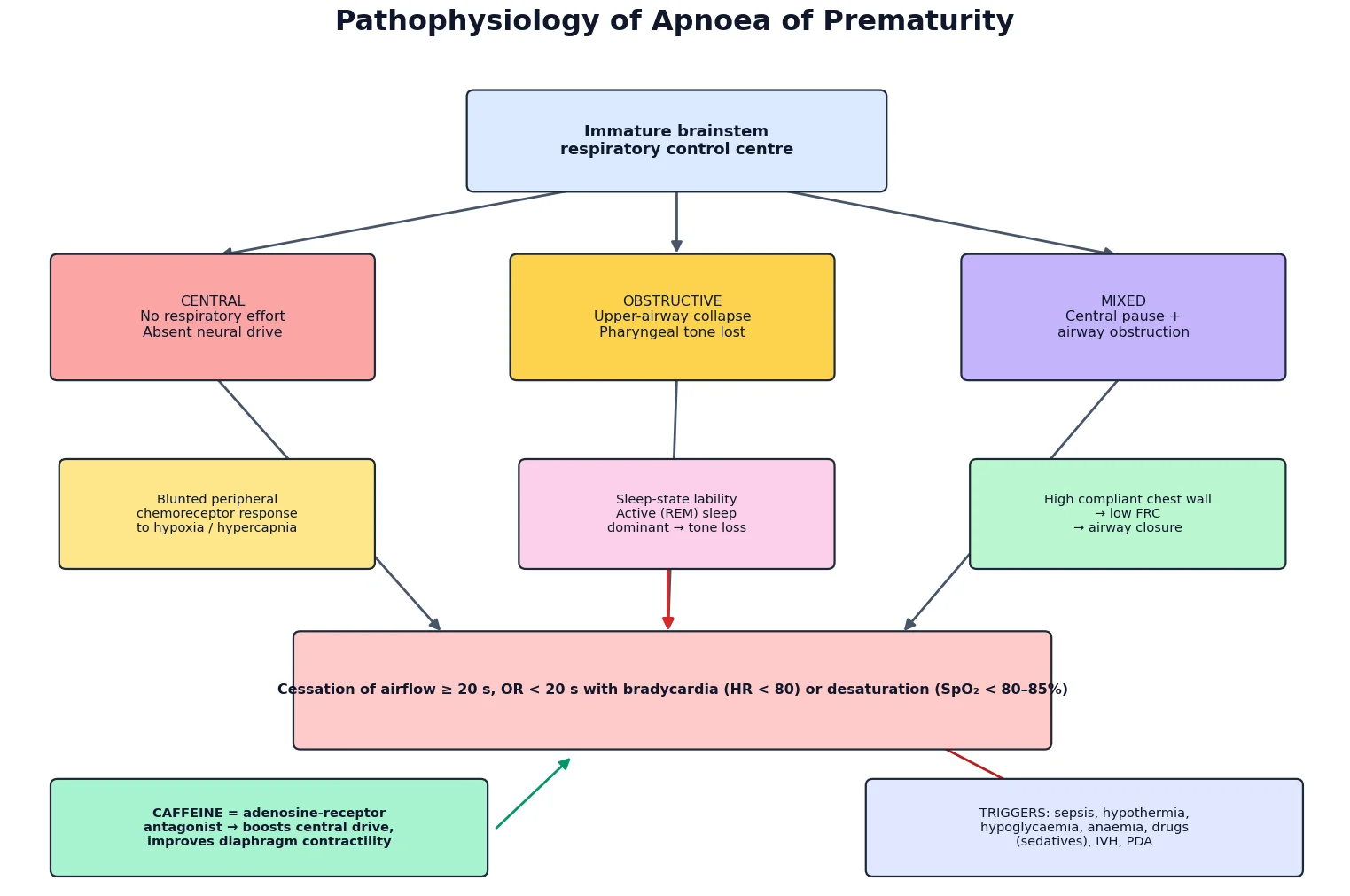
The peripheral chemoreceptors add a second problem. In a mature infant, hypoxia stimulates breathing; in the very preterm infant, the response is blunted and even paradoxical, so that a fall in oxygen further depresses rather than drives respiration. Layer onto this a chest wall that is highly compliant and a lung with a low functional residual capacity, and the stage is set for airway closure, atelectasis, and rapid desaturation the moment effort falters. [4]
The obstructive and mixed forms arise from the upper airway. Premature infants spend most of their time in active, or rapid-eye-movement, sleep, during which the dilator muscles of the pharynx lose their tonic tone and the airway collapses. The result is continued chest-wall motion against a closed airway — obstructive apnoea — or a central pause that is then prolonged by obstruction, the mixed pattern that accounts for most events. This is the mechanism that explains why continuous positive airway pressure works: it stents the airway open. [4]
Caffeine intervenes at exactly these points. By antagonising adenosine A1 and A2a receptors, it increases central respiratory drive, sharpens the response to carbon dioxide, and improves diaphragmatic contractility — three effects from a single, well-tolerated molecule. That mechanism, the receptor pharmacology, is a favourite viva question, so hold it ready. [5]
Classification
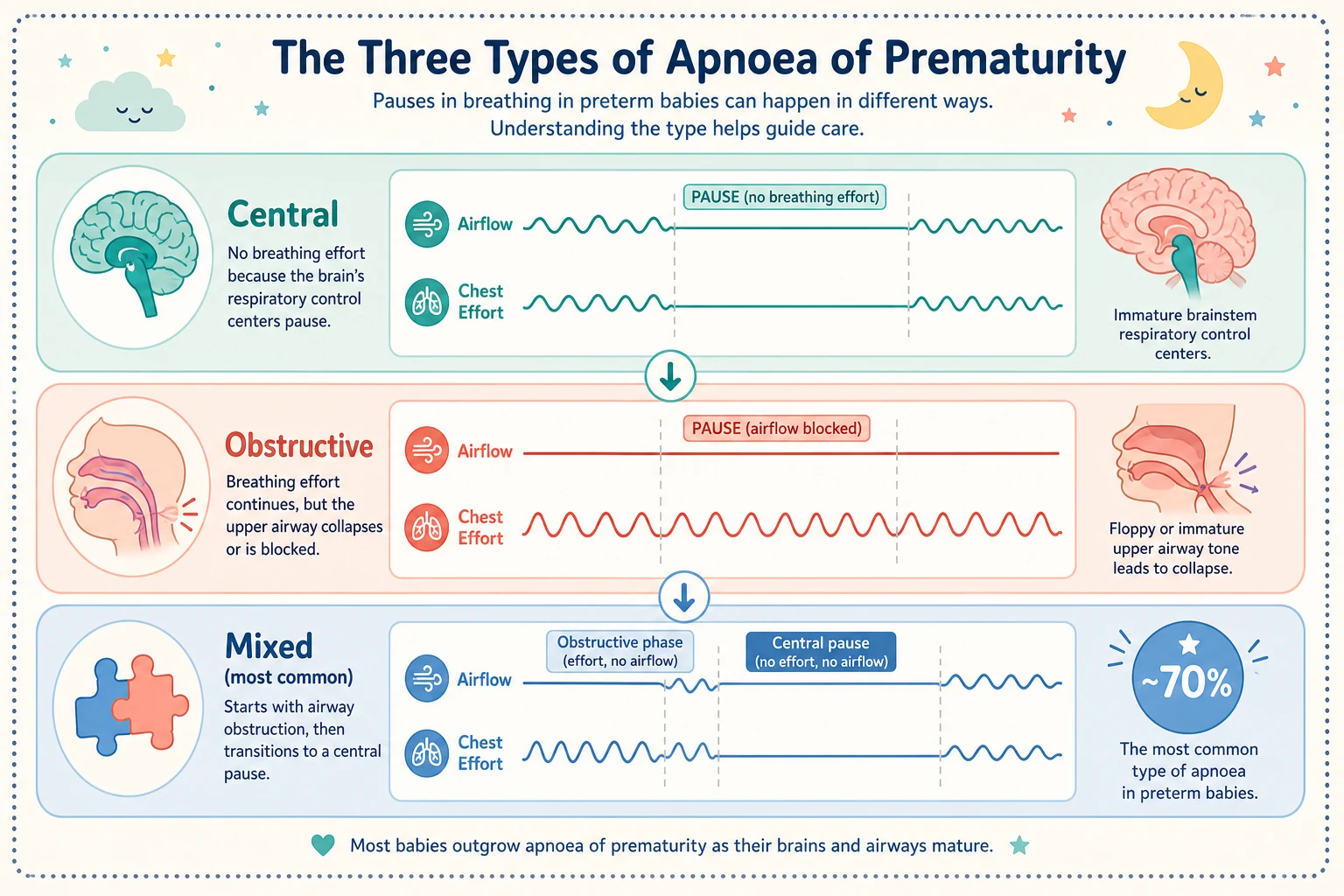
Apnoea of prematurity separates into three physiological types defined by what the chest and the airflow are doing during the pause. Central apnoea is pure loss of drive — no respiratory effort and no airflow, the brainstem simply failing to command a breath. Obstructive apnoea preserves effort but loses airflow, because the upper airway has collapsed against itself. Mixed apnoea is a central pause followed by obstruction, and it is the most common form, which matters because it tells you that a single drug will not always be enough. [4]
The separation from periodic breathing is the classification decision that changes management. Periodic breathing is a rhythm — short pauses in clusters, separated by bursts of normal breathing, without bradycardia or colour change — and it is a sign of an immature but healthy brain. Treat it with reassurance. Apnoea, with its accompanying bradycardia and desaturation, is a sign that the immature brain is failing to protect oxygenation, and it warrants treatment. [4]
Clinical Presentation
The bedside picture is rarely subtle. A nurse sees the colour drain — pallor or a dusky cyanosis — feels the infant go limp, and hears the alarm announce a bradycardia. Most events happen during sleep, especially active sleep, and many cluster around handling or feeds in the smallest infants in the first week of life. The episode usually resolves with gentle stimulation, which is itself diagnostic: if a brief touch restarts breathing, you are watching immaturity rather than catastrophe. [4]
The features that surround the apnoea tell you whether to reach for caffeine or for the blood-culture bottles. Temperature instability, poor perfusion, abnormal tone, respiratory distress, abdominal distension, or feed intolerance all point away from simple immaturity and toward a secondary cause. A septic infant apnoeising is an infant asking to be investigated, not sedated with a methylxanthine. [4]
The character of the event itself is worth documenting precisely. An obstructive event shows the chest continuing to move while the flow trace goes flat; a central event shows no respiratory effort at all. The mixed event, the commonest, shows both in sequence. This detail is not academic — it predicts which infants will need airway support in addition to pharmacotherapy. [4]
Differential Diagnosis
Hold the differential as two lists — the developmental and the dangerous — and the discipline is to prove the second before settling on the first. The single most important mimic is sepsis, with or without meningitis, and it is the one you cannot miss. New or worsening apnoea in any infant warrants a septic screen, because the cost of treating immaturity while infection smoulders is too high. [4]
The metabolic list is short but mandatory: hypoglycaemia, hypocalcaemia, and hyponatraemia all depress the respiratory centre, and an inborn error of metabolism may announce itself with apnoea before any other sign. A blood gas, glucose, and electrolytes at the bedside resolve most of these within minutes. [4]
Respiratory causes — respiratory distress syndrome, pneumonia, pulmonary haemorrhage, or a patent ductus arteriosus overloading the lungs — produce apnoea through fatigue and hypoxia. Neurological causes include intraventricular haemorrhage, periventricular leukomalacia, and seizures, any of which may present with apnoeic spells as the only sign. Gastro-oesophageal reflux is the diagnosis everyone reaches for and the evidence rarely supports; treat it only when the link is objective, not reflexive. [4]
Clinical & Bedside Assessment
Start at the monitor, not the infant. Confirm the episode against the continuous cardiac and oxygen-saturation traces: measure how long the pause lasted, and document whether bradycardia or desaturation travelled with it. A great deal of apparent apnoea dissolves on close inspection — the probe slipped off, the infant was moving, or a brief self-limiting dip was flagged as an event. Before you act, be certain the event was real. [4]
Then examine the infant, because the body tells you what the monitor cannot. Check the temperature, feel the perfusion, count the work of breathing, listen for a murmur, feel the abdomen, and assess the tone and level of consciousness. A cold, mottled infant with a tense abdomen is sending a very different message from a warm, pink, sleeping baby who startled into a pause. [4]
Weigh the event against the gestational and postmenstrual age. A 27-week infant apnoeising at five days of age is doing what 27-week infants do; a 36-week infant apnoeising on day three is a case waiting for an answer. The same pause, at different gestations, demands completely different responses. [4]
Investigations
Investigation is targeted, not blanket, and it is guided by the clinical question. When the apnoea is typical of gestational age, well-controlled on caffeine, and following the expected course, extensive testing adds noise. When it is early, severe, atypical, or occurring in a relatively mature infant, you investigate to find the cause. [4]
The septic screen leads: blood culture, full blood count with differential, and C-reactive protein, with a lumbar puncture added if there are central signs or no alternative source to explain the deterioration. Run the metabolic panel in parallel — glucose, electrolytes, and calcium — and take an arterial or capillary blood gas to assess ventilation and acid–base balance. A chest X-ray excludes pneumonia, respiratory distress, and air leak; a cranial ultrasound is reserved for infants in whom intraventricular haemorrhage or a structural lesion is plausible. [4]
Polysomnography and pneumograms are not routine. They earn their place in the atypical, the refractory, or the pre-discharge infant whose pattern does not fit the expected trajectory, where defining the type and burden of events changes the plan. For the typical case, the bedside monitor and a targeted blood panel are enough. [9]
Management — Resuscitation
The immediate response is graded to the severity of the event. Most pauses resolve with the gentlest possible intervention — a flick of the foot, a soft rub of the chest, a repositioning of the head — and the rule is to avoid vigorous stimulation, which is unnecessary and distressing. If the infant remains apnoeic, bradycardic, or desaturating, provide positive-pressure ventilation with a bag and mask or a T-piece, using blended oxygen targeted to the preterm saturation range. [1]
At the same moment, correct anything reversible that the bedside reveals. Warm the hypothermic infant, treat the hypoglycaemia, and, if sepsis is even a possibility, take the cultures and start antibiotics — the antibiotic is faster than the regret. The resuscitation and the hunt for a cause are not sequential; they happen together. [4]
Reserve escalation to non-invasive or mechanical ventilation for the infant whose events are frequent, severe, or unresponsive to stimulation and pharmacotherapy. The aim of resuscitation is to restore oxygenation and circulation within seconds, then to hand the problem over to the definitive plan. [1]
Management — Definitive & Stepwise
Definitive management is a ladder, and caffeine sits on its first rung. Caffeine citrate is the methylxanthine of choice: a loading dose of 20 mg/kg followed by a maintenance dose of 5 to 10 mg/kg given once daily. The Caffeine for Apnea of Prematurity trial used a 20 mg/kg load and 5 mg/kg per day and demonstrated not just fewer apnoeas but improved survival without neurodevelopmental disability at 18 to 21 months. [1]
Caffeine is preferred over theophylline for sound reasons — a wider therapeutic index, once-daily dosing, faster onset, and fewer side effects — and Cochrane review confirms that methylxanthines as a class reduce apnoea and the need for mechanical ventilation. Theophylline demands level monitoring that caffeine does not, which is why caffeine has displaced it in nearly every neonatal unit. [6] [7] [12]
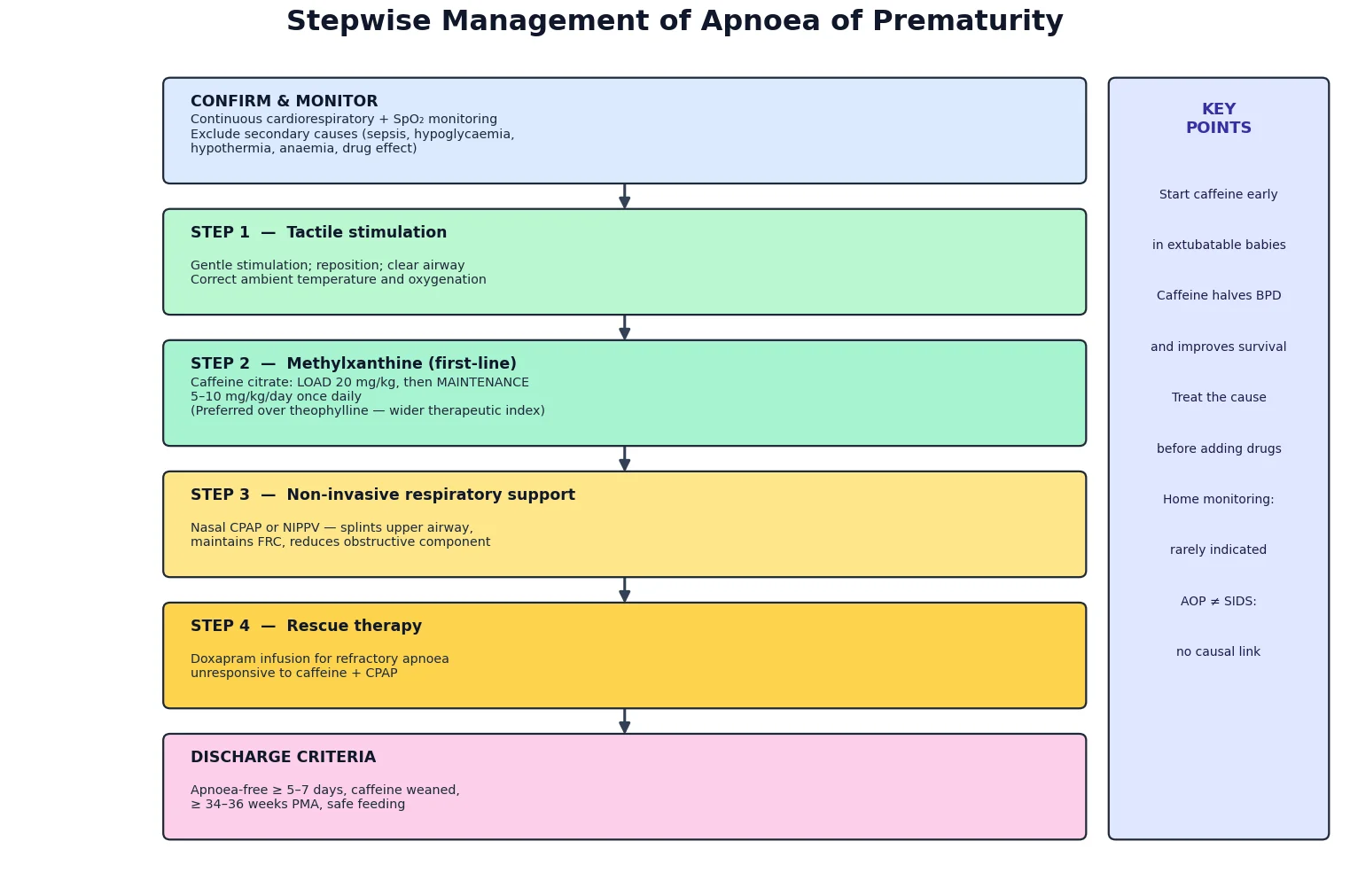
Stepwise management of apnoea of prematurity
Confirm and monitor on continuous cardiorespiratory and SpO2 traces; exclude secondary causes
Gentle tactile stimulation and repositioning; correct ambient temperature and oxygenation
Caffeine citrate — loading dose then once-daily maintenance
Nasal CPAP or NIPPV for obstructive or mixed events
Doxapram infusion as rescue for refractory apnoea
Wean caffeine once apnoea-free, approaching 34 to 36 weeks postmenstrual age
When caffeine alone is insufficient, add non-invasive respiratory support. Nasal continuous positive airway pressure, or nasal intermittent positive-pressure ventilation, splints the upper airway, maintains functional residual capacity, and directly addresses the obstructive component that a drug cannot reach. This is the step for the mixed apnoeic infant who keeps desaturating despite a therapeutic caffeine level. [4]
Doxapram is the third-line rescue agent, reserved for refractory apnoea that has not responded to caffeine and non-invasive support. The evidence base is thinner than for caffeine and the side-effect profile broader, so it earns its place only when the alternatives have been exhausted — never as a substitute for caffeine, which remains the first and usually the only drug the infant needs. [8]
Throughout, treat the cause in parallel with the symptom. Give antibiotics for sepsis, correct the electrolytes, manage the patent ductus, and transfuse only at the restrictive haemoglobin thresholds the trials support. Anaemia contributes to apnoea, but a liberal transfusion strategy carries its own harms, so the trigger is the haemoglobin, not the alarm. [4]
APNOEA — the causes to exclude
Specific Subtypes & Scenarios
Not every apnoea behaves as the textbook promises, and the exceptions are where the marks live. Apnoea that persists beyond 43 to 44 weeks postmenstrual age, or that emerges for the first time in a term infant, is no longer apnoea of prematurity — it is a signal to investigate neurological, airway, or metabolic disease. The label is developmental; when the development is complete, the explanation must be sought elsewhere. [9]
The prophylactic use of caffeine has become standard in the extremely preterm. Starting caffeine early, before events accumulate, facilitates extubation, reduces the need for mechanical ventilation, and is associated with better outcomes — a practice now embedded in the care of the infant under 28 weeks or below 1000 g. [1] [2]
Apnoea with feeds raises the question of reflux, and here the discipline is restraint. Gastro-oesophageal reflux is common in preterm infants and frequently coincidental rather than causal. Thicken the feeds or adjust the positioning only when the temporal link is objective; reserve acid suppression for proven disease, because the evidence that reflux causes apnoea is weak and the drugs are not without harm. [4]
Complications & Pitfalls
The harm of apnoea is not the pause itself but the recurrent desaturation that surrounds it. Intermittent hypoxaemia — the repetitive cycling of the oxygen down and back — is associated with worse neurodevelopmental outcomes and, in observational data, a link to severe bronchopulmonary dysplasia. This is the reason you treat: not to silence the alarm, but to flatten the hypoxaemic burden that the brain and the lung cannot tolerate. [10] [11]
The first pitfall is the false positive — treating every desaturation alarm as apnoea. Many alarms in extremely preterm infants reflect a displaced probe, a moving limb, or a brief self-limiting dip, and over-treating them exposes the infant to unnecessary intervention. Confirm the event before you escalate. [4]
The second pitfall is the false negative — attributing new apnoea to immaturity and missing the late-onset sepsis or necrotising enterocolitis underneath it. The safest reflex, when the pattern changes, is the septic screen, not the dose increase. The third is the reflexive treatment of reflux that is coincidental rather than causal, and the fourth is the assumption that a home monitor prevents sudden infant death syndrome — it does not, and it is not indicated for uncomplicated apnoea of prematurity. [9]
Prognosis & Disposition
The prognosis for the infant who outgrows their apnoea is excellent. Most infants are event-free by 36 weeks postmenstrual age, and even the most extremely preterm resolve by 43 to 44 weeks. The Caffeine for Apnea of Prematurity trial reinforced the upside of treatment — improved survival without neurodevelopmental disability at 18 to 21 months — which is why early caffeine is now the standard, not the exception. [1] [2]
Apnoea of prematurity is not, in itself, a risk factor for sudden infant death syndrome, and the two conditions should be kept firmly apart. The fear that an apnoeic preterm infant will go on to die of SIDS is a fear the evidence does not support, and it should not drive monitoring decisions at discharge. [9]
Safe discharge rests on three things: an apnoea-free interval of five to seven days, a successfully weaned or stable caffeine regimen, and reliable feeding with adequate weight gain, typically achieved around 34 to 36 weeks postmenstrual age. An infant sent home on caffeine needs a clear weaning plan, growth monitoring, and follow-up to confirm that cessation is safe. [9]
Special Populations
The extremely preterm infant, born under 28 weeks, carries the heaviest burden and reaps the greatest benefit from early, prophylactic caffeine. Their course is the most severe and prolonged, and the maturation of their respiratory control is the slowest, so expect events to 43 or 44 weeks and plan the wean accordingly. [1] [2]
The late-preterm infant, at 34 to 36 weeks, sits at the other end of the gradient. Significant apnoea is uncommon at this gestation, and when it appears it is more often a sign of pathology than of immaturity. Investigate these infants aggressively — sepsis, metabolic disturbance, and neurological disease are the diagnoses to chase, not a developmental label to apply. [4]
A term infant does not have apnoea of prematurity. Apnoea in a term baby implies seizure, sepsis, metabolic disease, or airway obstruction, and the work-up must reflect that. Holding the developmental label in reserve until the dangerous list is exhausted is the discipline that protects these infants. [9]
Evidence, Guidelines & Regional Differences
The evidence base centres on the Caffeine for Apnea of Prematurity trial, published in the New England Journal of Medicine in 2006. In this landmark randomised study of over 2000 infants weighing 500 to 1250 g, caffeine reduced the rate of death or survival with neurodevelopmental disability at 18 to 21 months, alongside fewer apnoeas and less need for mechanical ventilation. It is the trial that made caffeine the standard of care. [1]
Cochrane reviews frame the broader pharmacology. Methylxanthine treatment as a class reduces apnoea and the use of mechanical ventilation, and caffeine is preferred over theophylline on the grounds of efficacy, tolerability, and convenience. Recent reviews have turned to dosing — whether higher maintenance doses of caffeine outperform the standard 5 mg/kg per day — and the evidence, while growing, has not yet displaced the standard regimen. [3] [6] [7]
Controversy persists in three places: the optimal dose of caffeine, the best time to start, and the relationship between intermittent hypoxia and later neurodevelopment. The randomised evidence that caffeine reduces intermittent hypoxia, and the observational link between such hypoxaemia and bronchopulmonary dysplasia, frame the argument that flattening the desaturation burden matters as much as silencing the apnoea. [10] [11]
The American Academy of Pediatrics and the Canadian Paediatric Society converge on the message that home cardiorespiratory monitoring is not routinely indicated for uncomplicated apnoea of prematurity and does not prevent sudden infant death syndrome. Their shared emphasis at discharge is on safe-sleep practice and on parental confidence, rather than on a monitor. [9]
Exam Pearls
The definition is the question you will be asked, so hold it exactly: a pause of 20 seconds or more, or a shorter pause with bradycardia below 80, cyanosis, or desaturation. The caffeine doses follow close behind — load 20 mg/kg, maintain 5 to 10 mg/kg once daily — and the mechanism of caffeine, adenosine receptor antagonism, is the pharmacology point that distinguishes a pass from a distinction. [1] [4]
Remember the three structural distinctions that examiners love. Mixed apnoea is the most common type, which is why continuous positive airway pressure earns its place alongside the drug. New or worsening apnoea is sepsis until proven otherwise. And apnoea of prematurity resolves by 43 to 44 weeks postmenstrual age, with no causal link to sudden infant death syndrome — a reassurance you will offer to every anxious parent. [4] [9]
Finally, separate apnoea from periodic breathing at every opportunity. Periodic breathing is the benign immature pattern — short pauses in clusters, no bradycardia, no colour change — and it is treated with reassurance, not methylxanthines. Confusing the two is the error that turns a well infant into a medicated one, and naming the difference cleanly is the mark of a candidate who has spent time on the neonatal unit. [4]
References
- [1]Schmidt B, Roberts RS, Davis P, et al Caffeine therapy for apnea of prematurity. N Engl J Med, 2006.PMID 16707748
- [2]Oliphant EA, Hanning SM, McKinlay CJD Caffeine for apnea and prevention of neurodevelopmental impairment in preterm infants: systematic review and meta-analysis. J Perinatol, 2024.PMID 38553606
- [3]Bruschettini M, Brattstrom P, Russo C, et al Caffeine dosing regimens in preterm infants with or at risk for apnea of prematurity. Cochrane Database Syst Rev, 2023.PMID 37040532
- [4]Erickson G, Dobson NR, Hunt CE Immature control of breathing and apnea of prematurity: the known and unknown. J Perinatol, 2021.PMID 33712716
- [5]Atik A, Harding R, De Matteo R Caffeine for apnea of prematurity: Effects on the developing brain. Neurotoxicology, 2017.PMID 27899304
- [6]Henderson-Smart DJ, Steer PA Caffeine versus theophylline for apnea in preterm infants. Cochrane Database Syst Rev, 2010.PMID 20091506
- [7]Henderson-Smart DJ, Steer P Methylxanthine treatment for apnea in preterm infants. Cochrane Database Syst Rev, 2000.PMID 10796304
- [8]Evans S, Avdic E, Pessano S, et al Doxapram for the prevention and treatment of apnea in preterm infants. Cochrane Database Syst Rev, 2023.PMID 37877431
- [9]American Academy of Pediatrics Committee on Fetus and Newborn Apnea, sudden infant death syndrome, and home monitoring. Pediatrics, 2003.PMID 12671135
- [10]Rhein LM, Dobson NR, Darnall RA, et al Effects of caffeine on intermittent hypoxia in infants born prematurely: a randomized clinical trial. JAMA Pediatr, 2014.PMID 24445955
- [11]Jensen EA, Whyte RK, Schmidt B, et al Association between Intermittent Hypoxemia and Severe Bronchopulmonary Dysplasia in Preterm Infants. Am J Respir Crit Care Med, 2021.PMID 34428130
- [12]Kreutzer K, Bassler D Caffeine for apnea of prematurity: a neonatal success story. Neonatology, 2014.PMID 24931325