Paeds · fetal-neonatal-and-perinatal
Preterm infant: immediate and longitudinal care
Also known as Premature infant · Preterm neonate · Prematurity · Preterm baby · Preterm newborn
Fellowship guide to the preterm infant: gestational-age-stratified stabilisation, respiratory and nutritional pathways, thermoregulation, complication prevention and structured longitudinal neurodevelopmental follow-up, with regional pathway differences and exam pearls.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the 29-week infant born after spontaneous preterm labour — tiny, fragile, grunting in the delivery suite, skin translucent and heat pouring out of every centimetre of surface area. Your first minutes set the trajectory for a months-long NICU journey and a lifetime of neurodevelopmental risk. That is why preterm care is taught as a whole-of-journey discipline, not a single intervention. [1] [3]
Preterm birth is defined by gestational age at delivery. An infant born before 37 completed weeks is preterm; the lower the gestational age, the higher the risk across every organ system. The 26-week infant is a different patient from the 34-week infant — different respiratory vulnerability, different brain risk, different feeding immaturity, different prognosis — and your plan must reflect that gradation rather than treating all preterm infants as one homogeneous group. [1] [6]
Globally, roughly one in ten live births is preterm, and prematurity remains the leading cause of death in children under five. The burden falls hardest in low- and middle-income settings, but no region is spared — which is why a fellowship answer must be region-aware and equity-literate, not a single textbook pathway. [1] [2] [3]
Classification
Classification by gestational age is the exam vocabulary of prematurity and it drives everything downstream. Extremely preterm means less than 28 weeks; very preterm means 28 to 31 weeks and six days; moderate-late preterm means 32 to 36 weeks and six days. These bands are not arbitrary cut-offs — they map onto quantal leaps in organ maturation, particularly surfactant production, brain vascular stability and gut barrier function. [1] [6]
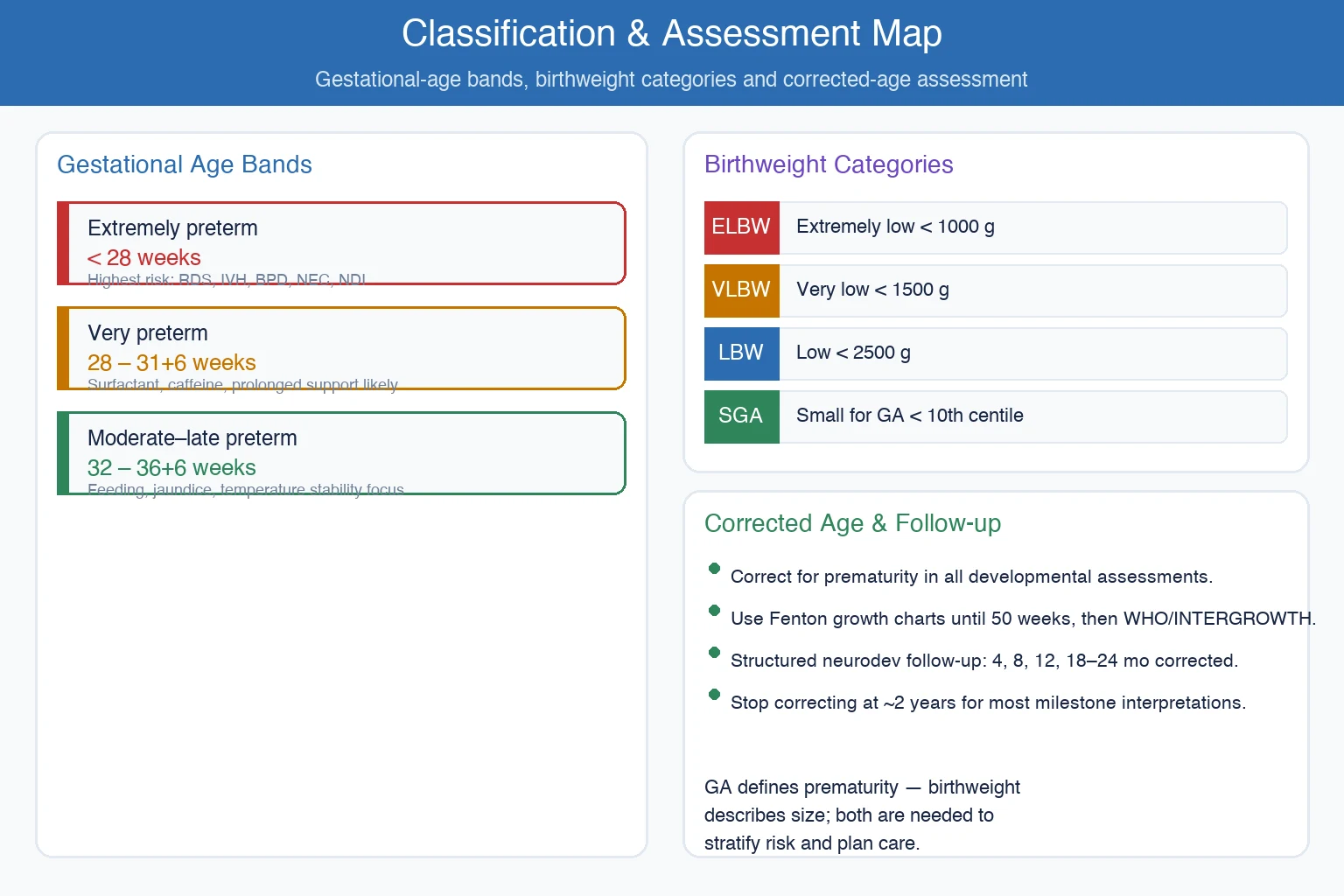
Birthweight categories overlap with but are distinct from gestational-age bands. Low birthweight is under 2500 g, very low birthweight under 1500 g and extremely low birthweight under 1000 g. Small-for-gestational-age describes an infant below the tenth centile for gestational age and signals possible intrauterine growth restriction from placental insufficiency — a different pathophysiology from prematurity but one that amplifies the same risks. [11]
Extremely preterm
< 28 weeks
- Highest RDS, IVH, BPD, NEC and NDI risk
- Requires surfactant, caffeine and prolonged support
- Intensive care and long hospital stay expected
- Follow-up to school age is essential
Very preterm
28 – 31+6 weeks
- Surfactant and respiratory support common
- Caffeine for apnoea and extubation readiness
- Moderate complication risk
- Structured neurodevelopmental follow-up required
Moderate-late preterm
32 – 36+6 weeks
- Often stabilise quickly
- Feeding immaturity, jaundice and temperature issues dominate
- Lower but real risk of readmission
- Corrected-age developmental monitoring still needed
Corrected age trap. When assessing development, you must correct for prematurity by subtracting the number of weeks born early from the chronological age. A baby born at 30 weeks who is 10 months old chronologically is 7 months corrected. Continue correcting until at least two years of age for most milestone interpretations, and use Fenton growth charts until 50 weeks post-menstrual age before transitioning to standard WHO or INTERGROWTH curves. [11] [20]
Epidemiology & Risk Factors
The global preterm birth rate sits near 10 to 11 per cent of live births, though measurement methods and definitions vary. The majority of preterm births occur in South Asia and sub-Saharan Africa, but high-income nations still report rates around 7 to 9 per cent, driven by rising maternal age, assisted reproduction, multiple gestation and medicalised obstetrics. [1] [2]
Headline numbers for viva
Maternal risk factors cluster into spontaneous and indicated pathways. Spontaneous preterm labour and preterm pre-labour rupture of membranes account for the majority, driven by infection, cervical insufficiency, multiple gestation, short interpregnancy interval and socioeconomic disadvantage. Indicated preterm delivery — for pre-eclampsia, placental abruption, fetal growth restriction or non-reassuring fetal status — accounts for the remainder and carries its own counselling implications. [2] [3]
The distinction matters because an infant delivered for pre-eclampsia at 31 weeks may have received full antenatal corticosteroids and be growth-restricted, while an infant born precipitously after spontaneous labour at 29 weeks may have had no antenatal optimisation and chorioamnionitis exposure. Both are preterm, but their risk profiles and early management differ. [4]
Pathophysiology
Organ immaturity is the unifying pathophysiology of prematurity, and it expresses itself differently in each system. The preterm lung lacks surfactant because type II pneumocytes are immature, so high surface tension collapses alveoli at end-expiration and the compliant chest wall cannot sustain functional residual capacity. The result is respiratory distress syndrome — grunting, retractions, increasing oxygen need and a ground-glass appearance on chest radiograph. [6] [21]
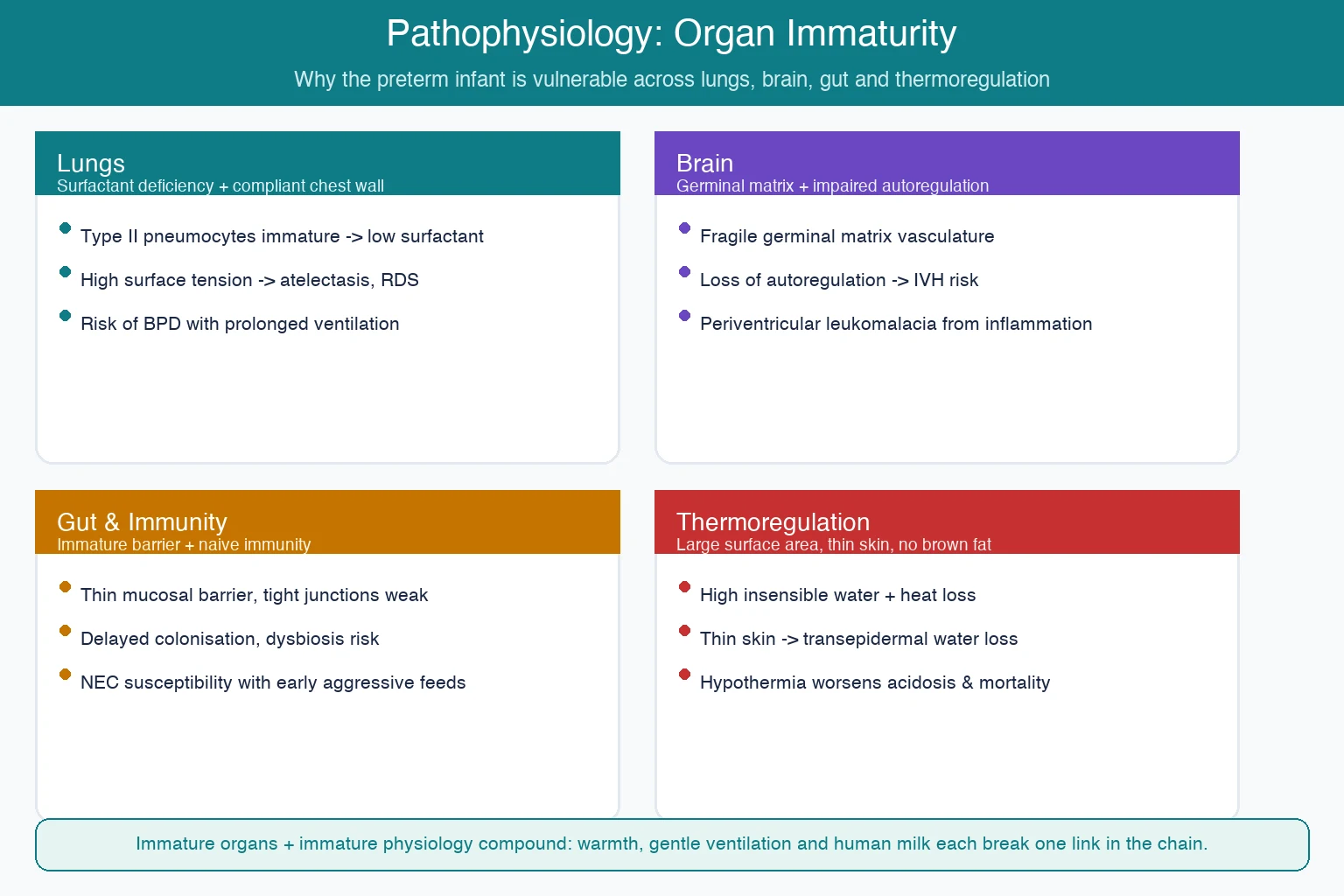
The preterm brain is exquisitely vulnerable because the germinal matrix — a highly vascular, metabolically active region overlying the caudate — is present until around 32 weeks and its fragile capillaries rupture easily under fluctuating cerebral blood flow. The preterm infant also has impaired cerebral autoregulation, meaning changes in systemic blood pressure passively transmit to the cerebral circulation. Together these mechanisms produce intraventricular haemorrhage, and the inflammatory and ischaemic injury that follows can produce periventricular leukomalacia — the white-matter injury that underlies much of the cerebral palsy risk in preterm survivors. [11]
The preterm gut has a thin, immature mucosal barrier with weak tight junctions, limited digestive enzyme capacity and a naive immune system. Combined with altered colonisation patterns from antibiotic exposure and delayed feeding, this creates the substrate for necrotising enterocolitis — the surgical emergency that every paediatrician must recognise. Thermoregulation fails because the preterm infant has a large surface-area-to-mass ratio, very thin skin that allows massive transepidermal water loss, and negligible brown adipose tissue for non-shivering thermogenesis. Hypothermia is not a minor inconvenience — it independently worsens mortality and morbidity. [11]
Clinical Presentation
Respiratory distress is the most common presenting feature of significant prematurity and it evolves over the first hours of life. Watch for tachypnoea above 60 breaths per minute, grunting as the infant fights to maintain functional residual capacity, subcostal and intercostal retractions from the compliant chest wall, nasal flaring, and a rising oxygen requirement. The earlier the gestational age, the more likely the distress is surfactant-deficiency respiratory distress syndrome rather than transient tachypnoea. [6]
Apnoea of prematurity typically emerges after the first day or two, once the infant tires or once sedation and thermal stress accumulate. It reflects immaturity of the central respiratory control centres in the brainstem and usually presents as pauses of more than 20 seconds, or shorter pauses associated with desaturation or bradycardia. Before attributing any apnoea to immaturity, you must exclude secondary causes — sepsis, hypoglycaemia, anaemia, temperature instability, drug effects and intracranial pathology. [10]
Feeding intolerance and abdominal signs demand vigilance. The preterm infant who develops abdominal distension, increased gastric aspirates, bloody stools or bilious residual is a necrotising enterocolitis alert until proven otherwise. A haemodynamically significant patent ductus arteriosus may declare itself through a systolic murmur, bounding pulses, a widened pulse pressure and an unexplained rise in ventilator or oxygen support as pulmonary over-circulation worsens. [15] [16]
Differential Diagnosis
When a preterm infant develops respiratory distress, you must distinguish respiratory distress syndrome from its mimics. Transient tachypnoea of the newborn is more common in late-preterm infants and resolves over 24 to 72 hours. Neonatal pneumonia presents similarly but often with a more pleural effusion and a maternal history of prolonged rupture of membranes or chorioamnionitis. Congenital heart disease — particularly duct-dependent lesions — can present with differential cyanosis, weak pulses or shock as the duct closes. [6]
When a preterm infant deteriorates, sepsis and necrotising enterocolitis are the two diagnoses you must never miss, and they can overlap. Early-onset sepsis presents in the first 72 hours with respiratory distress, temperature instability and lethargy, often linked to maternal colonisation or chorioamnionitis. Late-onset sepsis presents after 72 hours and is usually associated with central venous access, prolonged ventilation and invasive devices. Necrotising enterocolitis adds abdominal signs to the picture and may progress to perforation within hours. [11]
Metabolic disturbance is the silent mimic. Hypoglycaemia presents non-specifically with lethargy, jitteriness, apnoea or seizures, and the preterm infant is at high risk because of limited glycogen stores and immature glucose regulation. Hypocalcaemia, inborn errors of metabolism and electrolyte disturbance can all present as unexplained deterioration, so a metabolic screen belongs in the work-up of any sick preterm infant. [17]
Clinical & Bedside Assessment
Delivery-room assessment is the first and most time-critical bedside encounter. Assess tone, colour, breathing and heart rate within seconds of birth. A preterm infant who is breathing but struggling needs warmth, drying, stimulation and early CPAP — not immediate intubation unless there is apnoea, gasping, a heart rate below 60 despite ventilation, or persistent cyanosis. Use a pulse oximetry target that starts low and rises, and resist the urge to chase 100 per cent saturation in the first minutes. [6]
What does the daily NICU assessment look like?
A structured daily round checks fluid balance and weight trend, glucose and electrolyte stability, respiratory support level and blood gas, feeding tolerance and advancement, sepsis surveillance, central-line necessity, and neurological status including tone, activity and fontanelle. Each day you ask: can we de-escalate respiratory support, advance feeds, remove a line, or narrow antibiotics? That daily stewardship is what prevents iatrogenic harm. [11]
Growth assessment requires corrected-age plotting on Fenton charts for the first weeks, with weight, length and head circumference tracked as separate trajectories. Head circumference is the most sensitive single marker of brain growth, and a flattening head circumference trend after an intraventricular haemorrhage may signal evolving post-haemorrhagic ventricular dilatation. Neurological examination in the preterm infant is limited by immaturity — look for tone symmetry, spontaneous movement quality, primitive reflexes and seizure activity, but recognise that bedside examination alone cannot exclude significant intracranial injury. [11]
Investigations
At admission, a sick preterm infant needs a blood gas to assess oxygenation, ventilation and acid-base status, a glucose level, a full blood count and a C-reactive protein, and blood cultures before antibiotics. Chest radiography confirms surfactant-deficiency respiratory distress syndrome — low lung volumes with a ground-glass or granular appearance and air bronchograms — and excludes air leak, congenital malformation and cardiac enlargement. [6] [21]
Routine surveillance schedule
Cranial ultrasound is the workhorse neuroimaging modality in the preterm infant because it is bedside, radiation-free and sensitive to intraventricular haemorrhage and periventricular leukomalacia. Screen infants below 32 weeks or 1500 g in the first week, repeat at four to seven days to capture evolution, and continue weekly or as clinically indicated to monitor for post-haemorrhagic ventricular dilatation. [11]
Retinopathy of prematurity screening is driven by gestational age and birthweight, not by symptoms. Criteria are typically birthweight below 1500 g or gestational age below 30 to 32 weeks, with the first examination around 31 to 34 weeks post-menstrual age and follow-up every one to two weeks until retinal vascularisation is complete or treatment is indicated. Echocardiography is indicated when a patent ductus arteriosus is suspected, when there is unexplained respiratory deterioration, or to confirm a structural cardiac lesion. [12]
Management — Resuscitation
The three true acute threats in the delivery room are failure to establish ventilation, hypothermia and hypoglycaemia, and the preterm resuscitation algorithm prioritises all three from the first breath. Dry and warm the infant under a radiant heater with a polyethylene wrap for the most immature, provide gentle ventilation with a T-piece or bag at controlled peak pressures, and start with air or low oxygen concentration — 21 to 30 per cent for infants below 35 weeks — titrating upward against pre-ductal saturation nomograms. [6]
For the infant who does not need immediate resuscitation, defer cord clamping for 30 to 60 seconds to allow placental transfusion. Individual-participant-data network meta-analysis shows that deferred clamping — whether short, medium or long — reduces mortality compared with immediate clamping in preterm infants, and cord milking is an alternative when immediate resuscitation precludes waiting. [5] [22]
When an acute deterioration occurs — septic shock, a suspected pneumothorax, pulmonary haemorrhage or metabolic crisis — stabilise the airway and breathing first, then restore circulation with volume and inotropes as indicated, correct glucose and metabolic derangement, and escalate to the appropriate level of imaging and specialist review. Necrotising enterocolitis with suspected perforation is a surgical emergency: fast the infant, decompress the stomach, obtain a surgical opinion and a radiograph, and do not delay surgery for imaging confirmation alone. [11]
Management — Definitive & Stepwise
The respiratory pathway begins with non-invasive support. Start CPAP at 5 to 7 cm of water for any breathing preterm infant with respiratory distress, and use nasal intermittent positive pressure ventilation as an alternative in the most immature. When respiratory distress syndrome is established and the oxygen requirement rises above 30 per cent on CPAP, give rescue surfactant via intubation or less-invasive administration techniques, then extubate back to CPAP as quickly as possible. [6] [7]
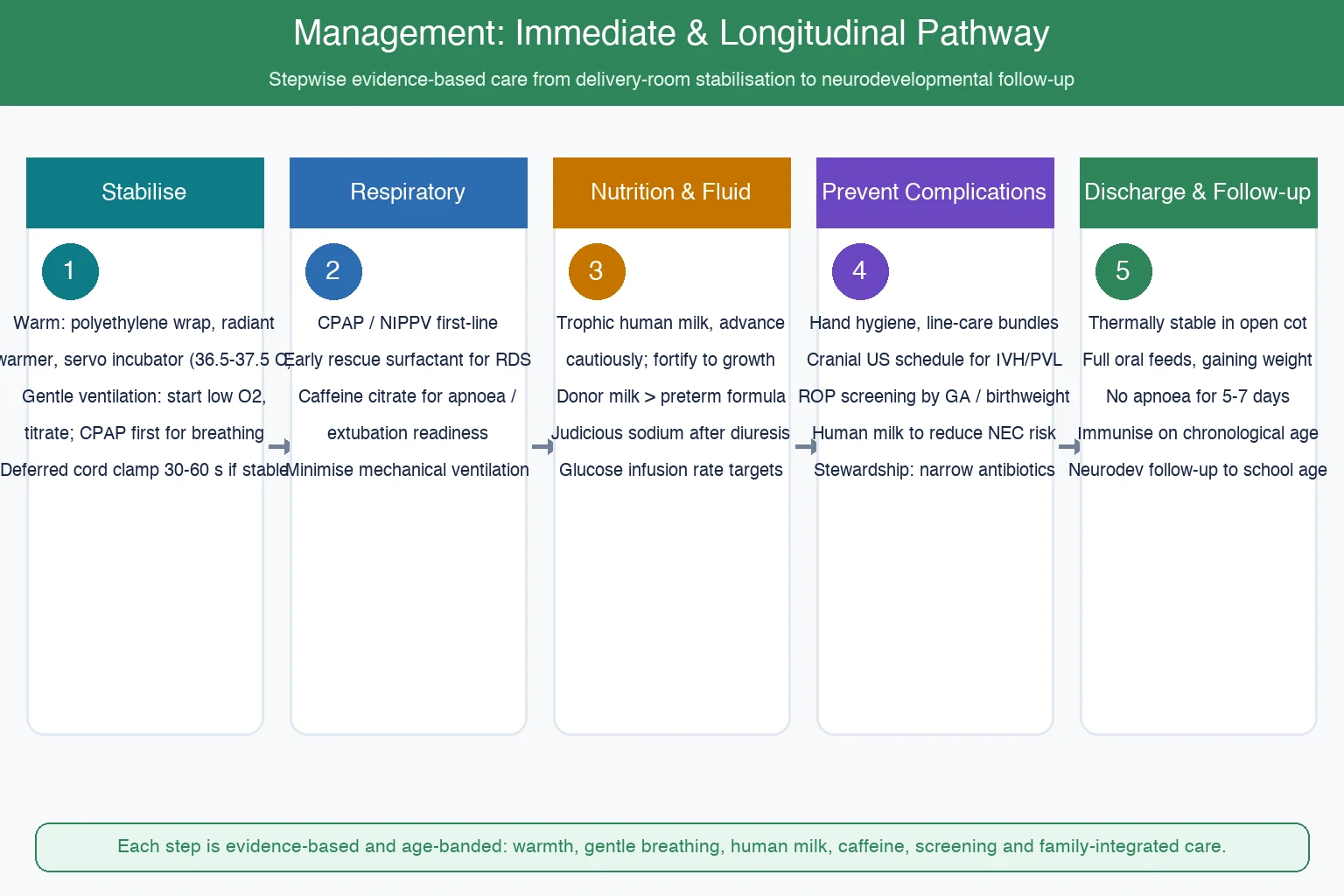
The SUPPORT trial was pivotal in establishing that early CPAP with selective surfactant is a viable alternative to routine intubation and prophylactic surfactant in extremely preterm infants, reducing the need for intubation without worsening outcomes. Caffeine citrate is the pharmacological backbone of apnoea management and extubation readiness — load at approximately 20 mg/kg and maintain at 5 to 10 mg/kg per day — and the Caffeine for Apnoea of Prematurity trial showed improved survival without neurodevelopmental disability at 18 to 21 months, with benefits persisting to age five. [7] [8] [9]
WARMF — the six pillars of preterm daily care
Thermoregulation is non-negotiable. Use a polyethylene wrap or bag for infants below 32 weeks at birth, maintain ambient temperature, use a radiant warmer and then a servo-controlled incubator, and target a core temperature of 36.5 to 37.5 degrees. Hypothermia on admission independently predicts mortality and intraventricular haemorrhage, and it is entirely preventable if the thermal chain — from delivery room to transport to NICU — is intact. [11]
Nutrition drives growth and brain development. Start trophic feeds with expressed maternal colostrum and human milk as soon as possible, advance cautiously in the smallest and sickest infants, and fortify toward growth targets once tolerance is established. When maternal milk is unavailable, donor human milk is preferred over preterm formula because Cochrane evidence shows it reduces necrotising enterocolitis, even though infants on donor milk may grow more slowly and require fortification. Manage fluids by starting with a higher free-water allowance, adding sodium judiciously after the diuresis phase, and targeting a glucose infusion rate of 4 to 8 mg per kg per minute. [14] [17]
The patent ductus arteriosus framework begins with conservative tolerance — fluid restriction, optimisation of oxygen and acid-base status — because many close spontaneously. When the ductus is haemodynamically significant with pulmonary over-circulation or gut hypoperfusion, pharmacological closure with ibuprofen, indomethacin or paracetamol is supported by network meta-analysis, and surgical ligation is reserved for failure or contraindication. [15] [16]
Sepsis prevention is a bundle discipline. Hand hygiene is the single most effective intervention; meticulous central-line care, preferential human-milk feeding, early line removal and antibiotic stewardship together reduce late-onset sepsis and necrotising enterocolitis. Every additional day of a central line is an additional day of risk, so ask daily whether the line can come out and whether antibiotics can be narrowed or stopped. [11]
Specific Subtypes & Scenarios
The very preterm infant of 28 to 31 weeks typically needs early CPAP and often surfactant, a caffeine course for apnoea and extubation readiness, and a feeding progression over two to three weeks with fortification. Cranial ultrasound surveillance and ROP screening are expected, and the discharge timeline is often driven by feeding maturity and weight gain rather than respiratory recovery. [6]
The extremely preterm infant below 28 weeks is the highest-acuity scenario in neonatology. Expect prolonged respiratory support, a high probability of bronchopulmonary dysplasia, significant intraventricular haemorrhage and periventricular leukomalacia risk, and a prolonged hospitalisation measured in months rather than weeks. The multidisciplinary team — neonatology, nursing, allied health and family — must coordinate from the first day, and family-integrated care models improve parental confidence and infant outcomes. [11] [18]
Necrotising enterocolitis at three weeks of age is the classic late complication. The infant presents with abdominal distension, increased gastric residuals, bloody or bilious aspirates, and systemic signs of sepsis. Management is immediate: fast the infant, decompress the stomach, start broad-spectrum antibiotics, obtain surgical review and a radiograph looking for pneumatosis intestinalis or free air. Indications for surgery include perforation, a fixed dilated loop, worsening clinical deterioration despite maximal medical management, or an abdominal mass. [11]
The late preterm infant of 34 to 36 weeks is often underestimated. These infants look relatively mature but have higher risks of feeding immaturity, temperature instability, hypoglycaemia, jaundice and readmission than term infants. Discharge criteria must be met — feeding competence, thermal stability, stable weight gain, no significant apnoea — and parental education and follow-up are essential to prevent the morbidity that falls disproportionately on this group. [11]
Complications & Pitfalls
The major complications of prematurity are concentrated in the lungs, brain, gut and eyes. Bronchopulmonary dysplasia — defined as oxygen need at 36 weeks post-menstrual age — reflects the combined injury of volutrauma, oxygen toxicity and inflammation on the developing lung, and it predicts longer-term respiratory morbidity and readmission. Intraventricular haemorrhage and periventricular leukomalacia are the brain injuries that underlie cerebral palsy and cognitive impairment. [11]
| System | Complication | Key prevention | Surveillance |
|---|---|---|---|
| Lungs | RDS, BPD, air leak | CPAP first, gentle ventilation, caffeine | Blood gas, oxygen weaning, chest radiograph |
| Brain | IVH, PVL, post-haemorrhagic hydrocephalus | Avoid fluctuating BP, gentle handling, deferred cord clamp | Serial cranial ultrasound |
| Gut | NEC, feeding intolerance | Human milk, cautious advancement, line stewardship | Abdominal exam, gastric aspirates, radiograph |
| Eyes | Retinopathy of prematurity | Oxygen targeting, avoid swings | Scheduled ROP screening |
| Infection | Early-onset and late-onset sepsis | Hand hygiene, bundle care, antibiotic stewardship | Blood cultures, CRP, clinical signs |
Retinopathy of prematurity is the blinding complication of disordered retinal vascularisation, driven by immaturity, oxygen exposure and growth factors. Treatment with laser photocoagulation or intravitreal bevacizumab — established by the BEAT-ROP trial for zone I and posterior zone II stage 3 plus disease — prevents progression to retinal detachment, but screening and timely referral are the rate-limiting steps. [12] [13]
The preventable pitfalls are the ones examiners test hardest. Allowing admission hypothermia through a broken thermal chain independently worsens mortality. Over-resuscitating with 100 per cent oxygen and high tidal volumes in the delivery room causes oxidative and volutrauma injury. Attributing feeding intolerance to immaturity and missing evolving necrotising enterocolitis until perforation. Treating all instability as infection and overusing broad-spectrum antibiotics when the problem is metabolic. Failing to screen or follow up retinopathy of prematurity to schedule, and ignoring parental mental health and bonding during a long and stressful admission. [11]
Prognosis & Disposition
Gestational age is the dominant predictor of survival and major morbidity. Modern cohort data show improving survival for the most immature infants, but survival without major morbidity remains challenging below 26 weeks. The EPICure studies comparing 1995 and 2006 cohorts in England demonstrated improved survival for extremely preterm infants over time, with survival to discharge rising across gestational-age bands, and the neurodevelopmental follow-up showed persistent but shifting disability profiles. [19] [20]
Discharge is safe when the infant is thermally stable in an open cot, feeding fully by mouth with sustained weight gain, free of significant apnoea for five to seven days, growing along the expected trajectory, immunised on chronological age, and when the family is ready with a follow-up plan in place. The discharge process is not a single event — it is a structured handover to the medical home, the early-intervention team, and the community services that will support the preterm graduate through childhood. [18]
Structured neurodevelopmental follow-up is expected at corrected ages of approximately 4, 8, 12, and 18 to 24 months, with assessment of motor development using standardised tools, growth plotting on corrected age, hearing and vision surveillance, and school-readiness evaluation closer to age five. Early identification of cerebral palsy, cognitive impairment, sensorineural hearing loss and visual impairment allows timely intervention, and the family must be supported with honest, hopeful and probabilistic counselling throughout. [20]
Special Populations
The extremely preterm infant near the threshold of viability demands the most nuanced decision-making. Antenatal counselling about anticipated outcomes, active versus comfort care, and the limits of viability must be individualised to gestational age, estimated fetal weight, sex, antenatal steroid exposure and parental values — and the paediatrician must be prepared to revisit decisions as new information emerges after birth. This is a distinct topic with its own leaf, but the immediate-care decisions flow directly from that counselling. [19]
The growth-restricted preterm infant carries the combined burden of prematurity and placental insufficiency. These infants are at higher risk of hypoglycaemia, hypothermia, polycythaemia and neurodevelopmental impairment, and they need careful catch-up nutrition with ongoing surveillance for metabolic and cardiovascular consequences of fetal programming. The preterm infant of a mother with perinatal infection or substance use may present with withdrawal, sepsis risk or neurobehavioural dysregulation that complicates the standard pathway. [4] [17]
Rural and remote preterm infants depend on neonatal retrieval networks and telehealth-supported follow-up. The principles of stabilisation are identical, but the logistics of transfer, family separation, and community reintegration add complexity. Indigenous and migrant families require culturally safe, language-concordant care — in the ANZ context, this means Te Tiriti-informed practice and attention to the inequities that drive preterm birth and worsen outcomes for Maori, Pacific and Aboriginal and Torres Strait Islander families. [18]
Multiple-gestation preterm infants share and compete for risk. Twin-twin transfusion, selective growth restriction and preterm labour are more common, and the loss of one twin changes the risk profile for the survivor. Family-integrated care models must account for the practical reality of two or more infants in the NICU simultaneously, with the attendant parental burden and bonding challenges. [11] [18]
Evidence, Guidelines & Regional Differences
The SUPPORT trial was a landmark that established early CPAP with selective surfactant as a viable strategy in extremely preterm infants, reducing intubation without worsening survival or bronchopulmonary dysplasia. The European Consensus Guidelines on Respiratory Distress Syndrome synthesise the delivery-room stabilisation, surfactant strategy and non-invasive support evidence into practical recommendations used worldwide. [7] [6] [21]
ANZ: Neonatal retrieval networks, regional NICU levels, culturally safe family-integrated care, and ANZNN outcome benchmarking. UK: BAPM and NICE frameworks for neonatal stabilisation, discharge criteria and structured follow-up; EPICure cohort data inform prognosis. US: AAP and ACOG guidance on delivery-room management, ROP screening criteria, and Medicaid-funded early intervention follow-up. Canada: Canadian Paediatric Society position statements on preterm nutrition, discharge criteria and community follow-up networks. The principles are converging — the operational details differ. [3] [19]
The Seidler individual-participant-data network meta-analysis transformed cord-clamping practice by demonstrating that deferred clamping reduces mortality in preterm infants compared with immediate clamping. The Caffeine for Apnoea of Prematurity trial and its follow-up established caffeine as a neuroprotective as well as symptomatic therapy. Cochrane overviews on donor milk and patent ductus arteriosus interventions provide the evidence base for nutrition and cardiovascular management. [5] [8] [14] [15]
Controversies persist. Probiotic prophylaxis for necrotising enterocolitis shows promise in meta-analysis but has been complicated by safety signals of bloodstream infection in extremely preterm infants, leading to regulatory caution in some jurisdictions. The routine treatment versus conservative tolerance of the patent ductus arteriosus remains debated. Oxygen saturation targets balance retinopathy risk against mortality — moderate targets around 91 to 95 per cent are widely accepted, but the optimal range for the most immature continues to be refined. [6] [15]
Exam Pearls
Preterm birth is defined by gestational age, not birthweight — moderate-late, very and extremely preterm are the exam vocabulary, and they map onto quantal leaps in organ maturation. Deferred cord clamping for 30 to 60 seconds is the standard for preterm infants who do not need immediate resuscitation, and the Seidler meta-analysis is the citation to quote. [5]
Start resuscitation with air or low oxygen and titrate upward — never routinely with 100 per cent. CPAP is first-line, early rescue surfactant for established respiratory distress syndrome, and mechanical ventilation is a last resort to be minimised. Caffeine citrate treats apnoea, improves extubation success, and improves survival without neurodevelopmental disability — quote the CAP trial and its five-year follow-up. [7] [8] [9]
Retinopathy of prematurity screening is gestational-age-and-birthweight based, not symptom based — do not miss the scheduled examinations, and know that zone I or posterior zone II stage 3 plus disease is treated with laser or intravitreal bevacizumab per BEAT-ROP. Human milk reduces necrotising enterocolitis, and donor milk is preferred over preterm formula when maternal milk is unavailable — quote the Quigley Cochrane review. [12] [14]
Correct for prematurity until at least two years of age when assessing developmental milestones, and use Fenton growth charts until 50 weeks post-menstrual age. Hypothermia on admission is a preventable mortality risk — wrap, warm and use a servo-controlled thermal chain. Necrotising enterocolitis with perforation is a surgical emergency — do not delay surgical review for radiographic confirmation alone. [11]
The discharge criteria are a viva favourite: thermally stable in an open cot, full oral feeds with sustained weight gain, no significant apnoea for five to seven days, immunised on chronological age, and a structured follow-up plan in place. Structured neurodevelopmental follow-up continues to school age using corrected-age assessment. [18] [20]
References
- [1]Chawanpaiboon S Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health, 2019.PMID 30389451
- [2]Walani SR Global burden of preterm birth. Int J Gynaecol Obstet, 2020.PMID 32524596
- [3]Howson CP Born too soon: preterm birth matters. Reprod Health, 2013.PMID 24625113
- [4]Roberts D Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev, 2017.PMID 28321847
- [5]Seidler AL Short, medium, and long deferral of umbilical cord clamping compared with umbilical cord milking and immediate clamping at preterm birth: a systematic review and network meta-analysis with individual participant data. Lancet, 2023.PMID 37977170
- [6]Sweet DG European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology, 2023.PMID 36863329
- [7]SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network Early CPAP versus surfactant in extremely preterm infants. N Engl J Med, 2010.PMID 20472939
- [8]Schmidt B Caffeine therapy for apnea of prematurity. N Engl J Med, 2006.PMID 16707748
- [9]Schmidt B Survival without disability to age 5 years after neonatal caffeine therapy for apnea of prematurity. JAMA, 2012.PMID 22253394
- [10]Eichenwald EC Apnea of Prematurity. Pediatrics, 2016.PMID 26628729
- [11]Stoll BJ Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA, 2015.PMID 26348753
- [12]Fierson WM Screening Examination of Premature Infants for Retinopathy of Prematurity. Pediatrics, 2018.PMID 30478242
- [13]Mintz-Hittner HA Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med, 2011.PMID 21323540
- [14]Quigley M Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev, 2019.PMID 31322731
- [15]Mitra S Interventions for patent ductus arteriosus (PDA) in preterm infants: an overview of Cochrane Systematic Reviews. Cochrane Database Syst Rev, 2023.PMID 37039501
- [16]Mitra S Association of Placebo, Indomethacin, Ibuprofen, and Acetaminophen With Closure of Hemodynamically Significant Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-analysis. JAMA, 2018.PMID 29584842
- [17]Hay WW Jr Knowledge gaps and research needs for understanding and treating neonatal hypoglycemia: workshop report from Eunice Kennedy Shriver National Institute of Child Health and Human Development. J Pediatr, 2009.PMID 19840614
- [18]Patel N Family Integrated Care: changing the culture in the neonatal unit. Arch Dis Child, 2018.PMID 29122741
- [19]Costeloe KL Short term outcomes after extreme preterm birth in England: comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ, 2012.PMID 23212881
- [20]Moore T Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: the EPICure studies. BMJ, 2012.PMID 23212880
- [21]Sweet DG European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology, 2019.PMID 30974433
- [22]Seidler AL Deferred cord clamping, cord milking, and immediate cord clamping at preterm birth: a systematic review and individual participant data meta-analysis. Lancet, 2023.PMID 37977169