Paeds · growth-development-and-behaviour
Adolescent transition for neurodevelopmental disability
Also known as Health care transition neurodevelopmental disability · Transfer to adult care disability · Transition planning intellectual disability autism CP · Emerging adult disability medical home · Six Core Elements transition disability
Fellowship guide to adolescent transition for neurodevelopmental disability: structured transition frameworks, readiness assessment, portable summaries, warm handoff, legal and family preparation, crisis rescue, and ANZ/UK/US/Canada system differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
T.R.A.N.S.F.E.R. plan
Overview & Definition
A 17-year-old with intellectual disability, epilepsy and gastrostomy still attends only paediatric clinic. No adult GP. No adult neurologist. Mum carries every plan in her head. In six months the hospital “paediatric age policy” may end. That is not a clerical problem. It is health-care transition for neurodevelopmental disability. [1] [15]
Health-care transition is the planned process of moving from child-centred to adult-oriented health care. It is more than sending a letter. Classic adolescent-medicine position papers defined transition as purposeful, planned and continuous. Modern medical-home guidance organises it into policy, tracking, readiness, planning, transfer and adult-care integration. [1] [2] [5] [6]
This page owns the transition process for intellectual disability, autism, cerebral palsy and related complex neurodevelopmental care. Disease-specific treatment algorithms live on dedicated leaves. Cross-link those rather than hiding second chapters here. [14] [17]
Classification
Sort the work by framework stage and readiness domain. [1] [18]
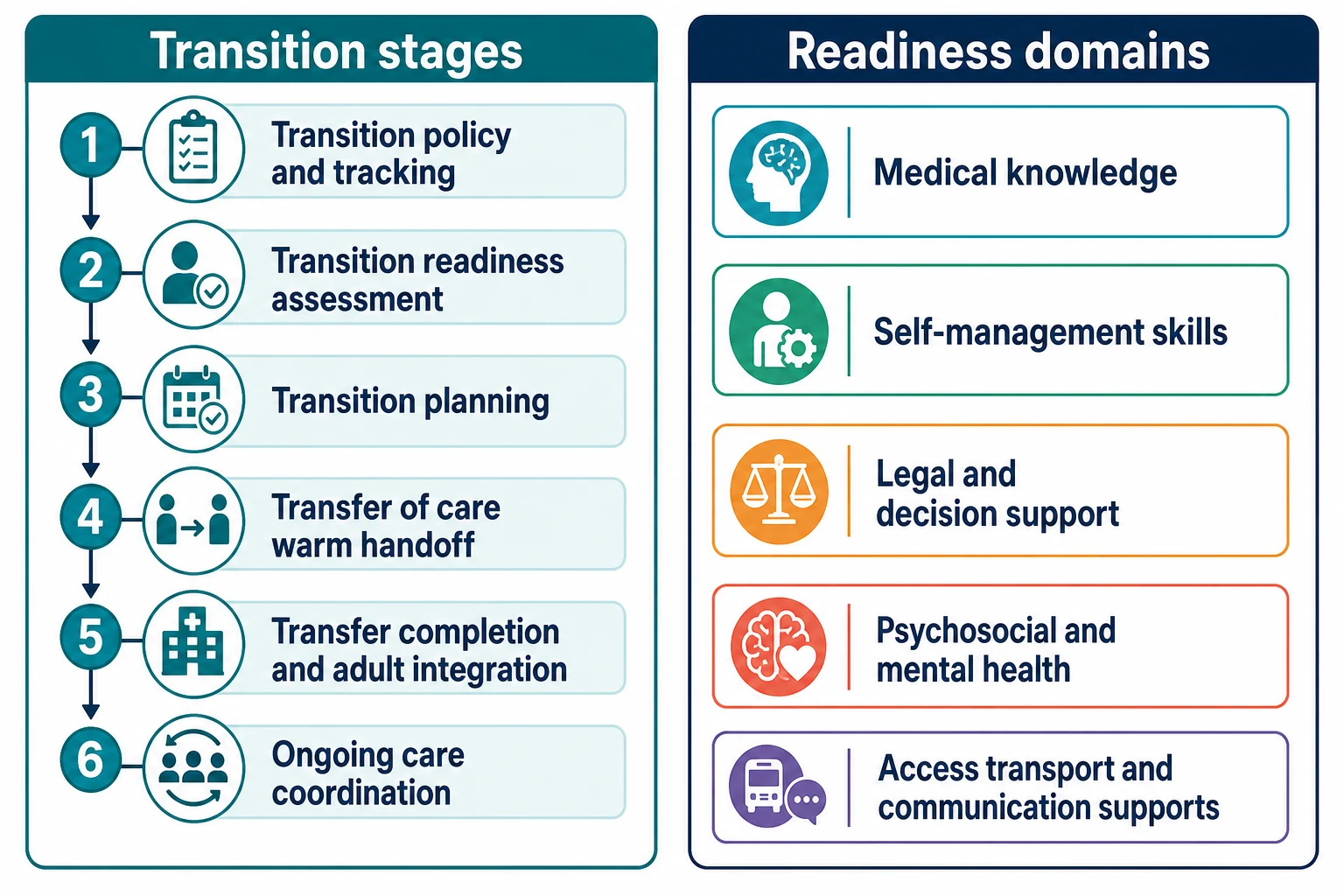
Structured stages (Six Core Elements style). Transition policy and clinic culture. Tracking and monitoring who is approaching transfer. Transition readiness assessment and education. Transition planning with a portable summary. Transfer of care with warm handoff. Transfer completion and adult integration with follow-up. These stages are not a rigid age script; they are a safety checklist. [1] [2] [18]
Readiness domains. Medical knowledge at developmental level. Self-management skills (or supported management). Communication and sensory needs in adult clinics. Legal decision-making supports. Psychosocial and mental-health readiness. Access: transport, funding, interpreters, physical accessibility. [3] [4] [7]
Population subtypes in transition. Intellectual developmental disorder. Autism. Cerebral palsy and other motor disabilities. Technology-dependent complex care. Mixed profiles are common; the process still applies. [15] [17] [20]
Epidemiology & Risk Factors
Many youth with special health care needs reach adulthood without adequate transition preparation. US population data have repeatedly shown incomplete preparation, with worse gaps for some disability and social groups. Newer disparity analyses continue to show unequal preparation. [11] [13]
Neurodisability across adolescence and young adulthood carries measurable health risk. National linked-data work in England highlights mortality risk signals in young people with neurodisability between late childhood and early adulthood — a reminder that this is not a soft administrative interval. [16]
Pediatricians report practical barriers when transitioning adolescents with disabilities: adult provider availability, time, family readiness and system fragmentation. Those barriers are part of the epidemiology of failure. [15]
Risk concentrates where supports are thin: socioeconomic disadvantage, rural services, out-of-home care, complex technology dependence, and families already exhausted by care coordination. [13] [14]
Pathophysiology
Think of mechanisms that turn an age policy into clinical harm. [1] [14]
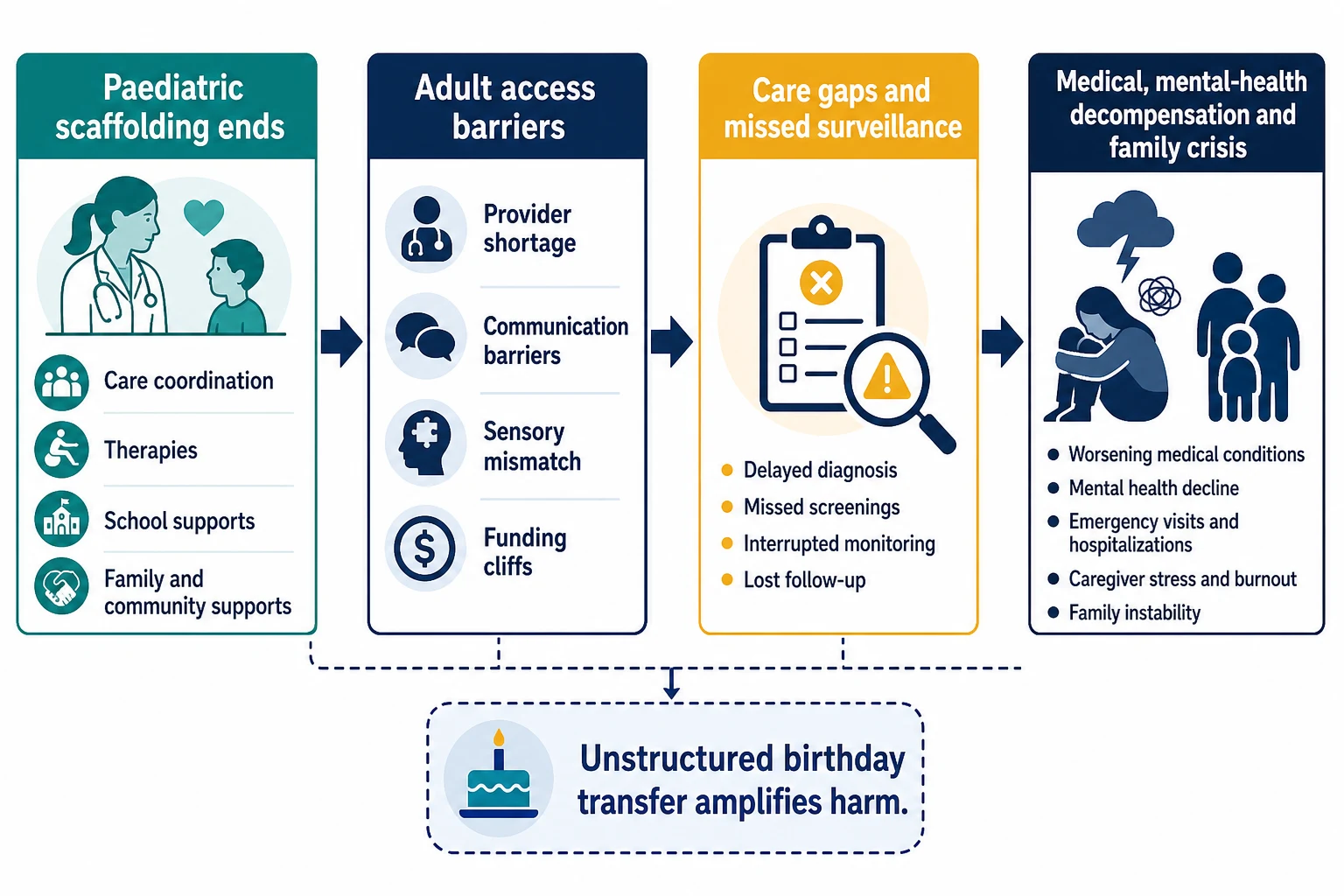
Loss of paediatric scaffolding. Paediatric teams often supply care coordination, therapy links, school medical plans and family-led visits. When that scaffolding ends without replacement, surveillance of seizures, tone, nutrition, mental health and devices fails. [1] [17]
Adult access mismatch. Adult clinics may assume independent history-taking, phone self-booking and short visits. Sensory load, communication differences and behavioural distress block attendance. Structural ableism in adult systems is increasingly named as a barrier. [20] [17]
Medication and device discontinuity. Without a portable emergency plan, missed antiepileptics, failed feeds or unrecognised baclofen/ITB issues present as “new” crises. [1] [14]
Family stress pathway. Parents often remain essential care partners. Abrupt role change without preparation increases anxiety and missed appointments. What helps parents also helps the process. [8]
Clinical Presentation
You will meet transition in ordinary clinics and in crises. [1] [15]
Planned presentation. Annual review of a 14–16-year-old with disability and no transition talk yet. School-exit planning with no adult health home. Request for a guardianship or supported-decision letter. [1] [7]
Failed-transition presentation. Young adult reappears in ED after years without specialist review. Seizure cluster after medication gap. Behavioural crisis when adult services refuse a first appointment without a “compliant” patient. [14] [16]
Legal cliff presentation. Age of majority arrives; parents can no longer consent by default; services demand new paperwork; nobody prepared the family. [1] [5]
Youth voice presentation. A non-speaking young person excluded from planning, or an autistic young person overwhelmed by adult waiting rooms. The presentation is system mismatch, not “non-compliance.” [17] [20]
Differential Diagnosis
Name the true problem before you add tests. [7] [14]
| You see | Prefer this framing | Trap |
|---|---|---|
| Worsening seizures after age 18 | Transition care gap ± disease progression | Blame “non-compliance” only |
| Missed adult clinic | Access, sensory, transport, fear, ableism | “Family not interested” |
| Behavioural escalation | Pain, mental health, communication failure, environment | Pure oppositional label |
| Parent wants full control forever | Need for supported decision-making plan | Assume zero capacity without assessment |
| Stable teen, no plan | Preventive transition work | Wait until crisis at 18 |
Safeguarding versus system failure. Both can coexist. Do not miss maltreatment because the story is “transition chaos.” Do not miss system failure because the story is “difficult family.” [14]
Clinical & Bedside Assessment
See the young person as the patient. Greet them first. Use their communication system. Offer private time when appropriate and safe. Still include caregivers who hold critical history. [1] [17]
Build a functional snapshot. Mobility and transfers. Communication method. Feeding and growth. Seizures. Tone and pain. Sleep. Behaviour triggers. Devices and emergency meds. Mental health. Sexuality and relationships when developmentally relevant. School/work plan. [15] [17]
Readiness assessment. Tools such as TRAQ measure self-management and advocacy skills and have validated structure and reliability in youth with special health care needs. In neurodevelopmental disability, interpret scores with support needs in mind: low independent scores may mean “needs a supported plan,” not “not ready forever.” [3] [4]
Legal and decision-making status. Ask what the young person understands and how decisions are made day to day. Plan for supported decision-making or formal arrangements using local law — do not invent ages or court processes. [1] [5]
Family readiness. Parents need their own transition: from speaking for the child to supporting the young adult. Ask what would make transfer easier for them. [8]
Investigations
Most “investigations” here are system investigations. [1] [14]
Required products before transfer. Up-to-date problem list. Medication and allergy list. Emergency plans (seizure, adrenal if relevant, device failure, behaviour crisis contacts). Baseline function description. Named adult primary and specialty providers. Communication passport. [1] [7]
Optional condition-specific tests. Update only if they change adult management (for example recent EEG relevance, swallow status, hip surveillance status in CP). Do not invent a universal “transition blood panel.” [14]
Harmful delays. Endless paediatric tests used to avoid naming an adult home. Waiting for perfect independence before any adult contact. [1] [12]
Outcome tracking after transfer. Attendance, acute care use, medication continuity, family stress, quality of life — the metrics that show whether transition worked. [9] [12]
Management — Resuscitation
Some transition failures are emergencies. [14] [16]
Act now for clinical instability. Status epilepticus risk, severe dehydration from feed failure, respiratory crisis in technology-dependent youth, suicidal ideation or acute behavioural danger. Stabilise first; repair the transition system second. [14]
Lost-to-follow-up re-engagement. Treat as urgent care coordination if high-risk disability is present. Find the young person, restore meds, book dual paediatric–adult contact if still possible, and write the emergency plan. [1] [14]
Safeguarding. New injuries, unexplained deterioration, or coercive control during the vulnerable transfer window need the same mandatory pathways as at any age. [14]
Management — Definitive & Stepwise
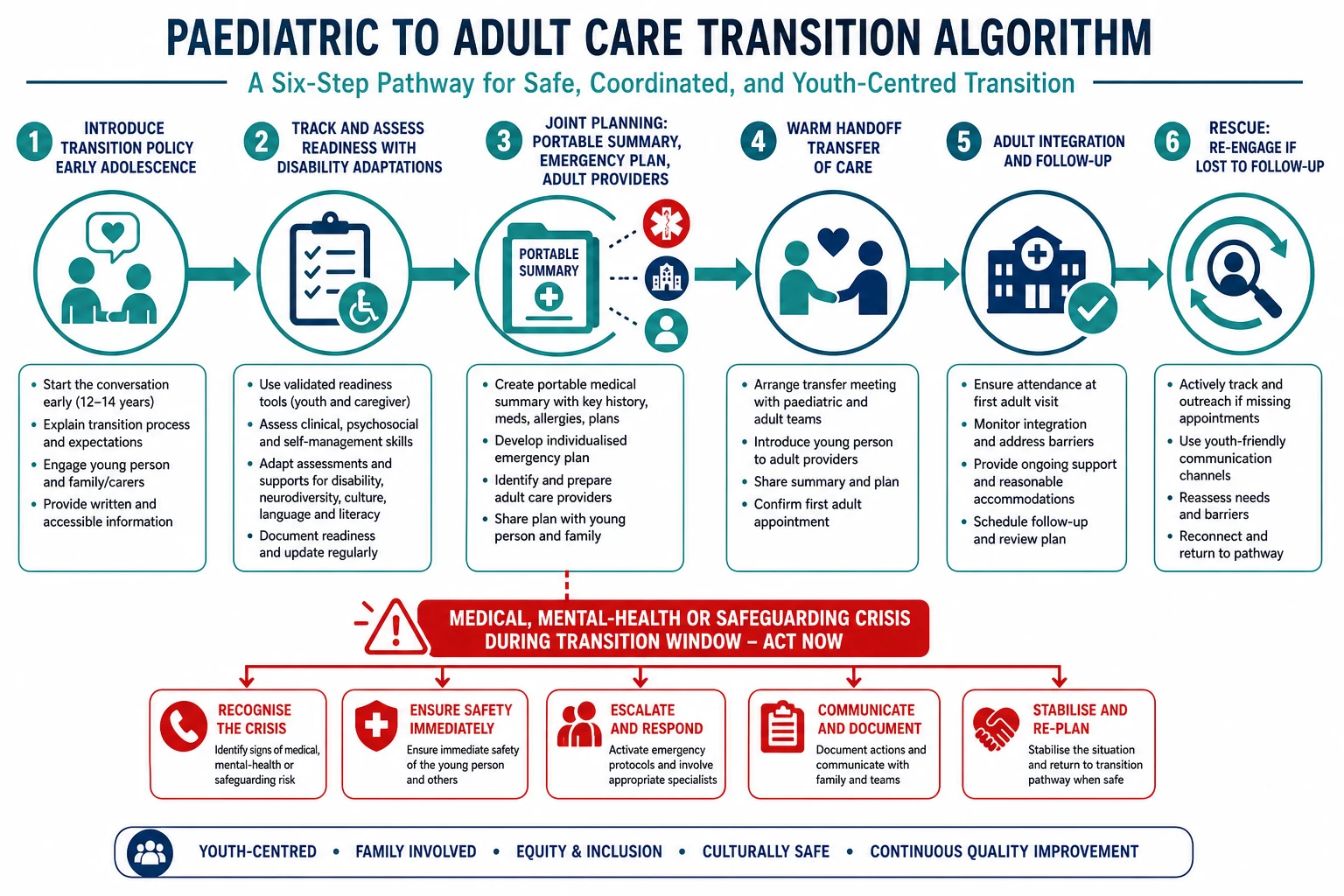
Use a structured pathway adapted from medical-home transition guidance and Six Core Elements practice. [1] [2] [18]
- Start early. Introduce the transition policy in early adolescence. Normalise that adult care is coming. [1]
- Track the cohort. Know who is 12–14, 14–16, 16–18+ and who is high risk. [1] [10]
- Assess and teach readiness. Use structured tools plus disability-specific supports. Practise skills in clinic. [3] [4]
- Plan jointly. Portable medical summary. Emergency plan. Goals for education/work/living. Legal planning timeline. Identify adult primary care and key specialists. [1] [7]
- Warm handoff. Shared visits, phone/telehealth introduction, or joint letters. Transfer when clinically sensible, not only when a birthday arrives. [1] [12]
- Complete and integrate. Confirm first adult visits happened. Offer paediatric rescue contact for a defined period if system allows. Measure outcomes. [9] [10]
What structured interventions can improve. Systematic reviews show structured transition programmes can improve outcomes compared with usual care, though study quality and measures vary. Implementation across large systems is feasible when leadership and process measurement exist. [9] [12] [10]
Digital adjuncts. E-health transition tools for brain-based disabilities are being piloted; they may support preparation but do not replace named adult clinicians or emergency plans. [19]
Specific Subtypes & Scenarios
Intellectual disability. Emphasise communication passport, supported decision-making, medication simplicity, and adult providers experienced with ID. Anticipate annual health checks and sensory-friendly appointments. [20] [15]
Autism. Plan sensory environment, waiting strategies, mental-health co-care, and clear written agendas. Avoid framing stimming or communication differences as non-compliance. [20] [17]
Cerebral palsy. Multi-specialty adult map (neuro, rehab, orthopaedics, urology, pain as needed). Transfer hip, tone, bone health and equipment plans. Youth and parent perspectives stress continuity and being heard. [17]
Technology dependence. Named adult responders for vents, pumps and feeds before transfer day. Device failure plan travels with the young person. [1] [14]
Rural transfer. Telehealth bridges, outreach specialists, and realistic adult local capacity. Do not assume metropolitan adult clinic density. [15]
Out-of-home care / justice interface. Information fragments; name a medical-home owner for the transfer package. [13]
Complications & Pitfalls
- Birthday discharge without adult acceptance. [1]
- Readiness score used as a barrier instead of a teaching map. [3] [4]
- Excluding youth voice when speech is limited. [17]
- No emergency seizure/device plan in the transfer pack. [1]
- Ignoring parent transition needs. [8]
- Assuming adult services will “just cope” with complex disability. [15] [20]
- Missing disparities: some groups get far less preparation. [11] [13]
- Focusing only on medical specialists and forgetting primary care. [1] [2]
- Structural ableism unaddressed in adult pathways. [20]
Prognosis & Disposition
Successful transition looks like continuous care, fewer preventable crises, preserved function and tolerable family stress — not a perfect independence score. Structured programmes and system improvement processes are associated with better process and some clinical outcomes, though residual gaps remain. [9] [10] [12]
Disposition choices. Proceed with transfer when adult homes are named and plans travel. Delay transfer briefly for acute instability, but do not use delay as avoidance. Shared-care bridges help high-risk youth. Re-open paediatric contact if the young person falls through immediately after transfer and local policy allows rescue. [1] [14]
Special Populations
Severe–profound disability and non-speaking youth. Communication supports and caregiver partnership remain central lifelong; adult care must accept supported visits. [17] [20]
Indigenous families. Culturally safe adult services, community-controlled pathways and trusted workers matter as much as the clinical summary. Cross-link dedicated cultural-safety leaves. [13]
Migrant and refugee families. Language access and unfamiliar legal systems amplify transition cliffs. [13]
Gender-diverse disabled youth. Affirming adult services and careful confidentiality planning. [1]
Socioeconomic disadvantage. Funding cliffs for therapies and equipment often hit at the same time as health-care transfer. Name the risk early. [13] [14]
Evidence, Guidelines & Regional Differences
Core anchors are AAP medical-home transition reports (2011 and White 2018 update), SAHM/SAM foundational position papers, TRAQ validation, Delphi key elements, parent-facilitation research, systematic reviews of intervention outcomes, implementation studies, and disparity/preparation epidemiology. Neurodisability-specific perspective and mortality data sharpen why process quality matters. [1] [2] [3] [5] [6] [7] [9] [11] [12] [13] [16]
Transition models vary by state/territory and health board. Use local young-adult disability clinics where they exist, RACP transition principles, and named adult primary care. Do not invent NDIS/benefit ages; prepare documentation early with local disability partners. Support culturally safe pathways for Aboriginal and Torres Strait Islander and Māori young people. [1]
NICE-aligned transition from children's to adults' services emphasises planning, preparation and continuity. Community paediatrics, education health plans and adult learning-disability services interact. Name local trust pathways. [7]
Got Transition Six Core Elements and AAP medical-home reports dominate teaching language. Insurance and Medicaid transitions at 18–26 create practical cliffs. Preparation remains incomplete for many youth with special needs. [1] [11] [13] [18]
Provincial adult disability and primary-care models vary. CanMEDS roles (Communicator, Collaborator, Health Advocate, Leader) map cleanly onto transition work. Use provincial legal frameworks for capacity. [1] [7]
Controversies: ideal chronological transfer age versus readiness; whether readiness scores should gate transfer; adult workforce capacity for complex disability; and how far paediatricians should remain involved after transfer. Exam answers show structured process and local humility. [1] [12] [15]
Exam Pearls
- Transition is a process, not a birthday. [1] [5]
- Start early; transfer with a plan. [1] [2]
- TRAQ-type tools guide teaching; adapt for disability supports. [3] [4]
- Portable summary + emergency plan + named adult home. [1] [7]
- Parents transition too. [8]
- Youth voice even when communication needs support. [17]
- Disparities in preparation are common without structured systems. [11] [13]
- Abrupt discharge without adult acceptance is unsafe. [1] [15]
- Structured interventions can improve outcomes; measure after transfer. [9] [12]
- Ableism in adult systems is a clinical barrier, not a soft issue. [20]
References
- [1]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [2]American Academy of Pediatrics Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics, 2011.PMID 21708806
- [3]Sawicki GS Measuring the transition readiness of youth with special healthcare needs: validation of the TRAQ--Transition Readiness Assessment Questionnaire. Journal of pediatric psychology, 2011.PMID 20040605
- [4]Wood DL The Transition Readiness Assessment Questionnaire (TRAQ): its factor structure, reliability, and validity. Academic pediatrics, 2014.PMID 24976354
- [5]Rosen DS Transition to adult health care for adolescents and young adults with chronic conditions: position paper of the Society for Adolescent Medicine. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2003.PMID 14519573
- [6]Blum RW Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1993.PMID 8312295
- [7]Suris JC Key elements for, and indicators of, a successful transition: an international Delphi study. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2015.PMID 26003575
- [8]Suris JC Transition from paediatric to adult care: what makes it easier for parents? Child: care, health and development, 2017.PMID 27625071
- [9]Schmidt A Outcomes of Pediatric to Adult Health Care Transition Interventions: An Updated Systematic Review. Journal of pediatric nursing, 2020.PMID 31981969
- [10]Jones MR Evaluation of a Health Care Transition Improvement Process in Seven Large Health Care Systems. Journal of pediatric nursing, 2019.PMID 31029928
- [11]McManus MA Current status of transition preparation among youth with special needs in the United States. Pediatrics, 2013.PMID 23669518
- [12]Gabriel P Outcome Evidence for Structured Pediatric to Adult Health Care Transition Interventions: A Systematic Review. The Journal of pediatrics, 2017.PMID 28668449
- [13]Ilango SM Disparities in Health Care Transition Preparation Among US Youth. Pediatrics, 2025.PMID 40953840
- [14]Okumura MJ Improving Health Care Transitions for Children and Youth With Special Health Care Needs. Academic pediatrics, 2022.PMID 35248248
- [15]Houtrow AJ Pediatrician reported experiences of transitioning adolescents with disabilities. Journal of pediatric rehabilitation medicine, 2026.PMID 41860103
- [16]Macaulay L Mortality Risk Between Ages 11 and 22 Years Among Young People With Neurodisability in England: A National Cohort Study Using Linked Health and Education Data. Paediatric and perinatal epidemiology, 2026.PMID 42423521
- [17]Fortune J Transition to adulthood: Perspectives from young people with cerebral palsy, parents, and health professionals. Developmental medicine and child neurology, 2026.PMID 42277597
- [18]Malik FS Incorporating the Six Core Elements of Health Care Transition in Type 1 Diabetes Care for Emerging Adults. Endocrinology and metabolism clinics of North America, 2024.PMID 38272598
- [19]Gorter JW An e-health transition intervention for youth with brain-based disabilities: Pilot and feasibility results from a Randomized Controlled Trial. Health care transitions, 2026.PMID 42317484
- [20]Ehrenberger KA Structural Ableism and Healthcare Transition for Adults with Intellectual and/or Developmental Disabilities. Journal of general internal medicine, 2026.PMID 42151527