Paeds · infectious-diseases
Brain abscess and intracranial suppuration
Also known as Cerebral abscess · Intracranial abscess · Subdural empyema · Epidural empyema · Intracranial suppuration
Fellowship guide to brain abscess and intracranial suppuration in children: the febrile child with evolving focal neurology, the cyanotic-heart-disease and sinus-otitis sources, the polymicrobial anaerobe-heavy microbiology, the contrast CT and MRI with diffusion-weighted imaging strategy, empiric third-generation cephalosporin plus metronidazole, the aspiration-versus-excision neurosurgical decision, the corticosteroid controversy, subdural empyema as a neurosurgical emergency, and the ANZ, UK and ESCMID guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the nine-year-old with a week of frontal headache and low-grade fever, treated as sinusitis, who this morning cannot name his sister and is dragging his right leg. The headache that would not settle, the fever, and the new focal sign together reframe a "simple" sinus infection as something far more dangerous — a collection of pus forming behind his eye. That is the clinical heart of brain abscess: a focal, space-occupying infection whose neurological signs often arrive late and whose mortality is governed by how quickly you image and act. [1] [4]
An abscess is a localised region of suppurative cerebritis that has progressed through inflammation and necrosis to a walled-off collection of pus within the brain substance. Intracranial suppuration is the umbrella term that also covers pus in the subdural (subdural empyema) and epidural (epidural empyema) spaces, which differ sharply in behaviour — the subdural space offers no barrier to spread, so subdural empyema is fulminant and is treated as an emergency. [1] [9]
The condition is uncommon in children but not rare, and it is one of the few diagnoses in paediatrics where hours change outcomes. Cyanotic congenital heart disease, chronic sinus or ear disease, penetrating head injury and immunocompromise are the classic settings, but a substantial minority are cryptogenic, so the absence of an obvious source never excludes the diagnosis. [6] [11]
Classification
The most useful way to think about intracranial suppuration is to map it by anatomical compartment, because the compartment dictates the urgency and the surgical approach. A parenchymal brain abscess sits within the brain substance and matures over days to weeks; a subdural empyema lies between the dura and the arachnoid, spreads rapidly and threatens herniation within hours; an epidural empyema sits between skull and dura and is often tethered by sinus or skull infection. [1] [9]
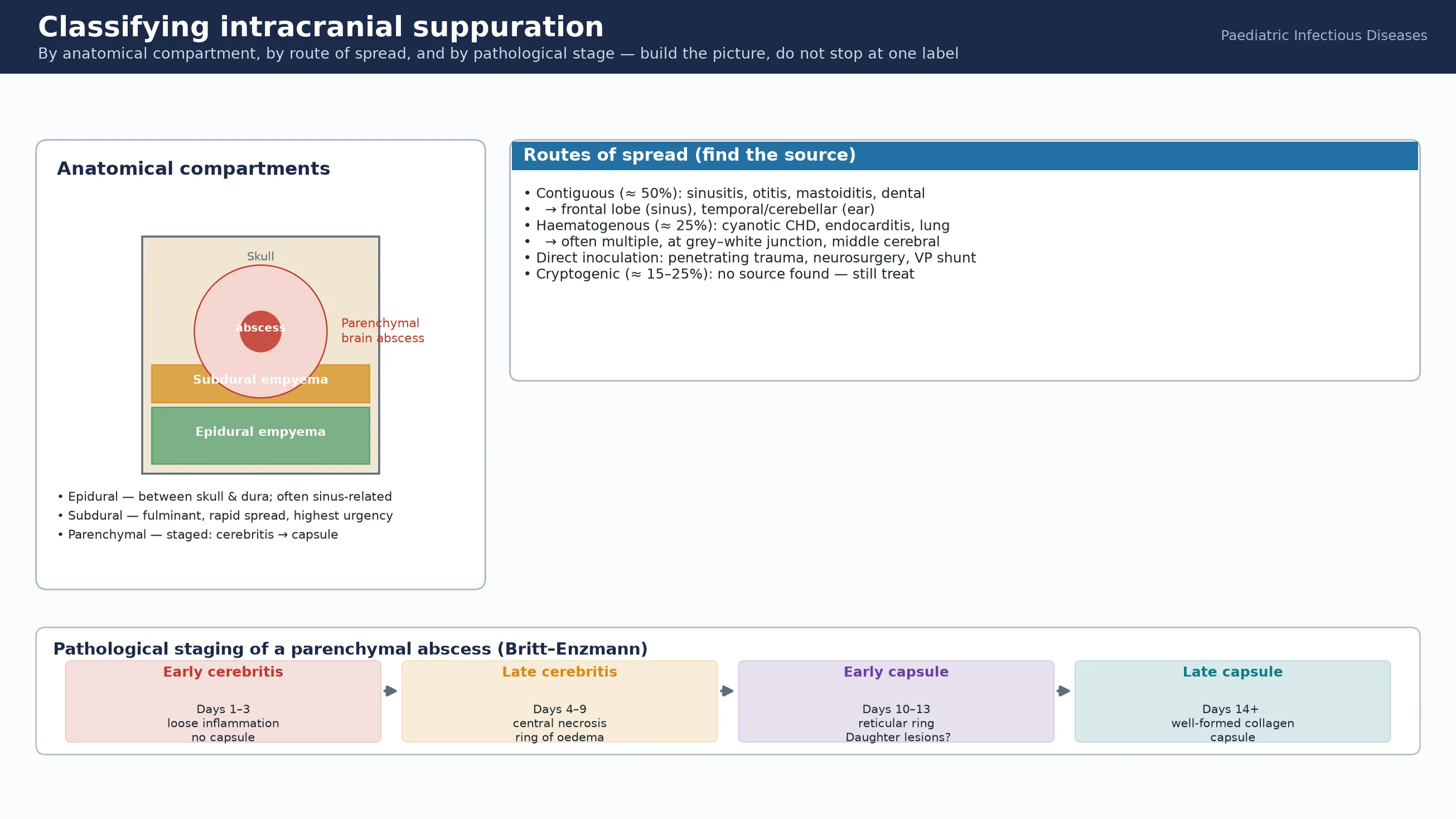
A second axis is the route of spread, which points you to the source you must treat. Contiguous spread from sinus, ear, mastoid or dental infection accounts for roughly half of cases and tends to seed the frontal lobe (sinus) or the temporal lobe and cerebellum (ear). Haematogenous spread — classically from cyanotic congenital heart disease, endocarditis or pulmonary infection — produces abscesses at the grey–white junction, often multiple and in the territory of the middle cerebral artery. Direct inoculation follows penetrating trauma, neurosurgery or a ventriculoperitoneal shunt, and around a fifth remain cryptogenic. [1] [8]
Parenchymal abscess
within brain substance
- Stages: early/late cerebritis → early/late capsule (Britt–Enzmann)
- Single or multiple; grey–white junction if haematogenous
- Matures over 1–2 weeks; capsule collagenises
- May rupture into the ventricle — catastrophic
Subdural empyema
subdural space
- No anatomical barrier → rapid spread
- Septic cortical venous thrombophlebitis
- Neurosurgical emergency — urgent evacuation
- Often from sinusitis or meningitis in infants
Epidural empyema
epidural space
- Tethered by skull sutures — more localised
- Often accompanies osteomyelitis or sinusitis
- Better prognosis than subdural
- Surgical drainage plus source control
Cerebritis
pre-suppurative
- Earliest, potentially reversible stage
- Poorly demarcated inflammation, no capsule
- May respond to antibiotics alone
- Diagnosed and tracked on MRI with contrast
Epidemiology & Risk Factors
Brain abscess is uncommon in children but is over-represented in specific risk groups, which is why a targeted history matters more than population incidence. Cyanotic congenital heart disease remains the single most important paediatric predisposing factor, because right-to-left shunting lets bacteria bypass the pulmonary capillary filter; the risk is highest in the unrepaired or palliated lesion and in children with residual shunts, and it persists across childhood. [11] [12]
The numbers that anchor your viva
Contiguous spread from paranasal sinus, middle-ear or mastoid infection is the most common source overall, and the location of the abscess follows the source — frontal from the frontal sinus, temporal or cerebellar from the ear. Dental sepsis is an under-recognised contributor. Penetrating head trauma, recent neurosurgery and the presence of a ventriculoperitoneal shunt raise the probability of staphylococcal infection and should widen the empiric cover. [8] [10]
Pathophysiology
The teaching model connects the source, the brain's response and the clinical syndrome in a single chain. A pathogen reaches the brain, lodges in a poorly perfused region, and provokes a sequence of inflammation, necrosis and walling-off that takes roughly two weeks to complete — the Britt–Enzmann staging that you can read on contrast MRI. [1] [14]
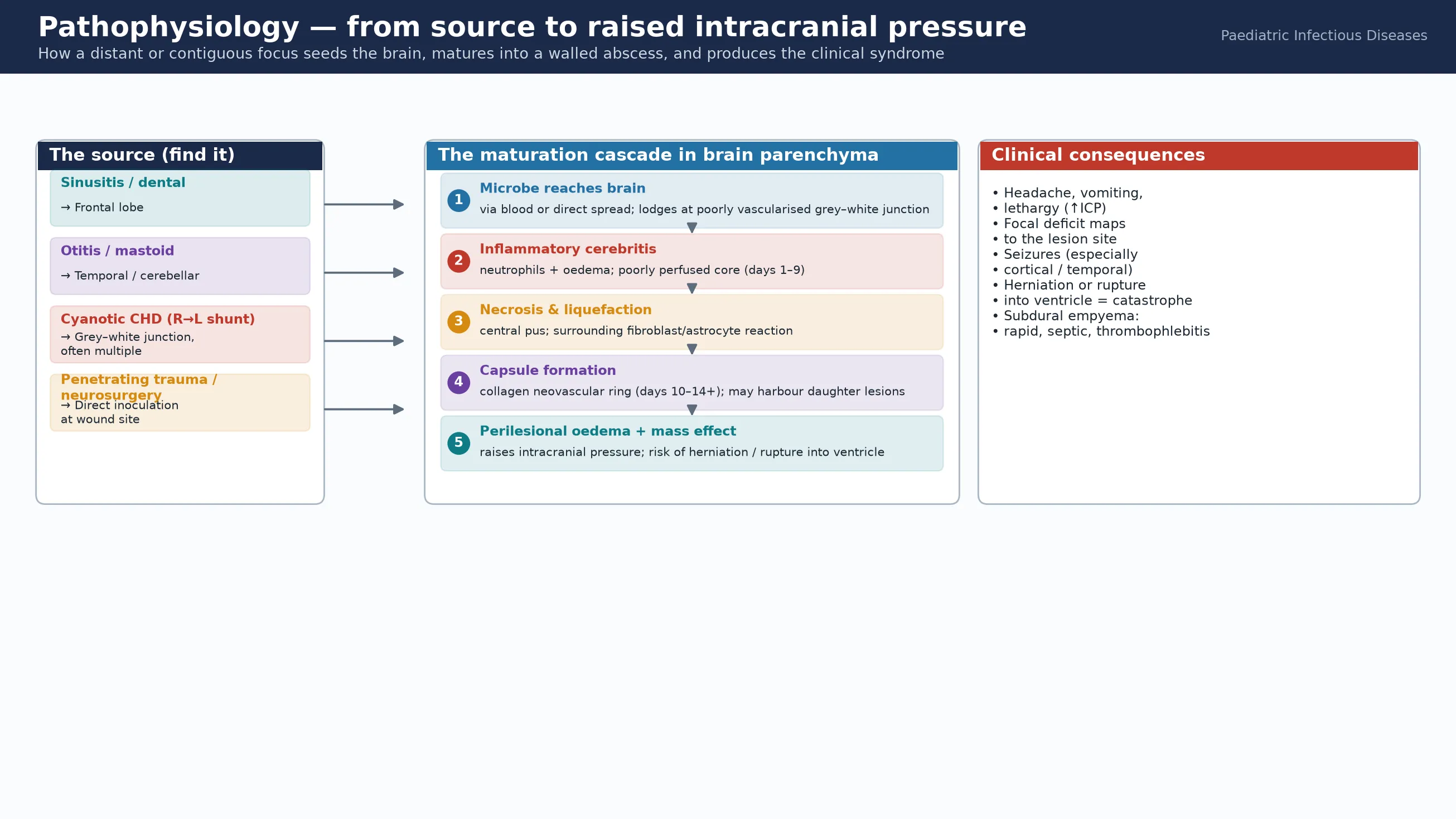
In early cerebritis (days 1–3) the area is loose, oedematous and poorly demarcated, with neutrophil influx and no capsule; in late cerebritis (days 4–9) a necrotic core appears surrounded by inflammatory oedema. By days 10–13 a reticular ring of fibroblasts and new vessels forms, and over the following week it matures into a collagenous capsule. The danger is that the capsule is never as complete on the side nearest the ventricle, which is why abscesses rupture preferentially inwards — a catastrophe. [1] [15]
The clinical syndrome has three drivers. The expanding collection and its surrounding oedema raise intracranial pressure, producing headache, vomiting, lethargy and papilloedema; the lesion's location produces a focal deficit mapped to its anatomy (hemiparesis, ataxia, aphasia, visual field defect); and the infection itself produces fever and inflammatory markers, which may be modest or even absent. Perilesional oedema and mass effect can progress to herniation, and the metabolic and vascular consequences of nearby inflammation explain the high rate of seizures. [1] [7]
[9]Clinical Presentation
The child in front of you rarely arrives with a label, and the presentation is often indolent and non-specific — which is the central diagnostic trap. Headache is the most common symptom, followed by fever, vomiting and lethargy, but any one of these may be absent, and infants in particular may show only irritability, poor feeding, a bulging fontanelle or increasing head size. The classic triad of fever, headache and a focal neurological deficit is present in fewer than a quarter of cases, so waiting for it costs time you do not have. [1] [7]
The focal signs map to the site of the lesion and are the strongest clue that this is not simple meningitis or a viral illness. A frontal abscess may produce subtle personality change or hemiparesis; a temporal-lobe lesion may cause aphasia or a visual-field defect; a cerebellar abscess produces ataxia, nystagmus and signs of raised pressure from obstructive hydrocephalus. Seizures occur in a substantial minority and may be the first sign, especially with cortical or temporal-lobe disease. [4] [6]
| Feature pattern | Likely site / process | Act |
|---|
A crucial point for the viva: the neurological deficit frequently lags behind the infection, so a febrile child with even a vague new neurological complaint warrants imaging rather than reassurance. Subdural empyema in particular can evolve over hours, with rapid progression from headache to coma, so any suggestion of meningeal signs plus a focal deficit in a septic child is an imaging emergency. [9] [5]
Differential Diagnosis
Build the differential in layers so you neither anchor on abscess nor miss a mimic. The imaging differential of a ring-enhancing lesion is the classic starting point, but the clinical differential begins with the other causes of fever plus headache plus evolving neurology in a child. [1] [14]
Ring-enhancing mimics
- Tumour (low-grade glioma, metastasis — rarer in children)
- Resolving haematoma or infarct
- Demyelination (tumefactive MS — very rare in children)
- Neurocysticercosis or tuberculoma in endemic regions
- Radiation necrosis after prior treatment
Other CNS infection
- Bacterial meningitis (no focal mass, LP may be safe)
- Viral encephalitis (HSV — temporal predilection, diffusion change)
- Tuberculous meningitis / tuberculoma
- Fungal abscess in immunocompromised
- Subacute/chronic subdural effusion in infants
Non-infectious
- Venous sinus thrombosis with infarct
- Posterior reversible encephalopathy
- Migraine with neurological aura
- Demyelinating or autoimmune encephalitis
- Recurrent or chronic headache syndromes
The discriminator is imaging combined with the clinical context: diffusion-weighted MRI is decisive, because a pyogenic abscess restricts diffusion (appears bright on DWI) whereas a tumour or cystic necrosis usually does not. Fever, an identifiable source, raised inflammatory markers and a compatible DWI signal together make the diagnosis; the absence of fever does not exclude it. [1] [3]
Clinical & Bedside Assessment
The assessment runs in parallel with resuscitation, because a deteriorating child cannot wait for a neat sequence. Secure the airway, breathing and circulation, treat seizures, and lower raised intracranial pressure if there are signs of impending herniation, while you take a focused history and examine. [1] [6]
The history targets three questions: where might the source be (sinus, ear, dental, heart, lung, trauma, surgery, shunt, immunocompromise), how has the child evolved (the tempo of headache, fever, vomiting, personality change and any focal sign), and what is the child's baseline and risk profile (congenital heart disease, immune status, recent travel or exposure). In adolescents, ask about IV drug use and dental hygiene; in infants, probe feeding, fontanelle and head circumference. [4] [12]
[1] [9]Examination looks for the focal deficit, signs of raised intracranial pressure (papilloedema, bulging fontanelle, declining conscious state, Cushing's response), the source (sinus tenderness, otoscopy, dental abscess, cardiac murmur, skin or scalp wound), and a general assessment of sepsis. A careful, documented neurological examination is also your baseline for tracking response to treatment. [4] [7]
Investigations
The investigation strategy has three aims: to confirm and characterise the collection, to identify the organism so therapy can be tailored, and to find and stage the source. Contrast imaging is the cornerstone; lumbar puncture is contra-indicated when a mass lesion is suspected; and microbiology hinges on obtaining pus, because cultures and molecular methods guide weeks of treatment. [1] [3]
Contrast MRI is the preferred modality when the child is stable enough, because it characterises the capsule, dates the lesion, detects small or multiple abscesses, and — critically — shows diffusion restriction that distinguishes abscess from tumour. A contrast CT is the immediate test in an unstable or rapidly deteriorating child, because it is fast and available and will identify a mass and the need for surgery. Magnetic resonance venography is added when venous sinus thrombosis is suspected, and diffusion-weighted imaging is essential for the differential. [1] [3]
Microbiology comes from blood cultures (two sets, before antibiotics when feasible) and, decisively, from pus obtained at aspiration or surgery — sent for Gram stain, aerobic and anaerobic culture, and, where available, 16S ribosomal RNA polymerase-chain-reaction for organisms that are slow or fastidious. The yield is highest when antibiotics have not yet been given, which is why aspirating before starting antibiotics — when it is safe to do so — is so valuable. Inflammatory markers (CRP, full blood count) support the diagnosis and track response but are not decisive. [8] [2]
The standard workup, run in parallel
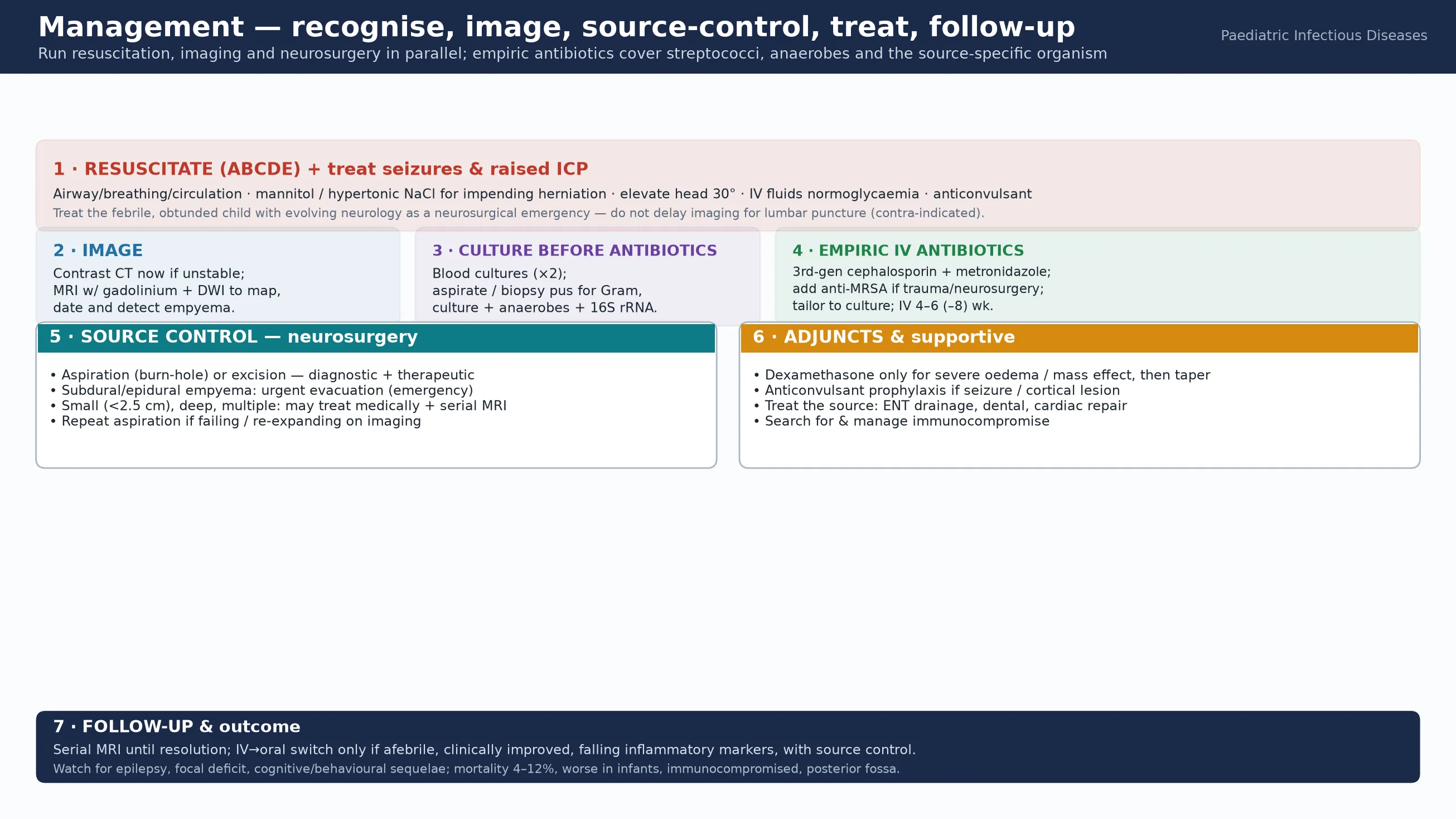
ABCDE; treat seizures and lower raised ICP if there are signs of impending herniation.
Contrast CT now if unstable; contrast MRI with gadolinium and DWI to characterise, date and localise.
Blood cultures ×2 before antibiotics if feasible; do NOT lumbar puncture a suspected mass.
Obtain pus at aspiration or surgery — Gram stain, aerobic and anaerobic culture, 16S rRNA PCR.
Start empiric IV antibiotics: third-generation cephalosporin plus metronidazole (add anti-MRSA if trauma, surgery or shunt).
Find and stage the source: ENT review, echocardiography, dental, and search for immunocompromise.
Serial MRI to monitor response, plan duration, and detect re-expansion or daughter lesions.
Management — Resuscitation
Resuscitation follows the same brain-injury principles as any critically ill child, with the added urgency of a space-occupying lesion. Protect the airway, support breathing and circulation, maintain normoglycaemia and normothermia, and treat seizures promptly with a benzodiazepine, escalating as needed. [1] [6]
If there are signs of impending herniation — a falling conscious state, Cushing's response (bradycardia with hypertension), pupillary asymmetry or posturing — lower the intracranial pressure urgently. Elevate the head of the bed to 30 degrees, and give an osmotic agent such as mannitol 0.25–0.5 g/kg IV or hypertonic (3%) saline 2–5 mL/kg IV while you arrange definitive imaging and neurosurgery. [1] [3]
The key principle is that resuscitation, imaging and neurosurgical referral proceed in parallel, not in sequence. A child with a suspected abscess and falling consciousness is a call to the neurosurgeon and the intensivist now, with imaging as the immediate next step. [9] [5]
Management — Definitive & Stepwise
Once the child is stabilised and imaged, definitive management is a coordinated effort between infectious diseases, neurosurgery, intensive care and the treating-source specialty (ENT, cardiology, dental). The two pillars are source control — aspiration or excision of the abscess and drainage of the subdural or epidural collection — and tailored intravenous antibiotics, guided by the organism recovered from pus. [1] [3]
ABC-PUS
For a parenchymal abscess, aspiration (via burr hole or stereotactic route) is the usual first approach: it is diagnostic, drains the collection, provides material for culture, and can be repeated. Surgical excision is reserved for large, superficial, multiloculated or re-expanding lesions, and for posterior-fossa abscesses where aspiration alone is hazardous. Small abscesses (under about 2.5 cm), deep lesions, and multiple haematogenous abscesses may be managed medically with serial MRI, provided the organism is known or confidently predicted and the child is improving. [1] [15]
Subdural and epidural empyema demand urgent surgical evacuation — this is not a condition to treat with antibiotics and a repeat scan, because the spread and the septic thrombophlebitis will outrun medical therapy. Sinogenic empyema in older children is increasingly managed with combined endoscopic sinus surgery to clear the source and neurosurgical drainage of the collection. [9] [10]
Empiric intravenous antibiotics are started immediately after cultures (or straight away if the child is septic or deteriorating) and tailored once the organism is known. The standard empiric regimen is a third-generation cephalosporin such as cefotaxime or ceftriaxone plus metronidazole, which covers the streptococci and anaerobes typical of contiguous and cryptogenic abscesses. Add anti-staphylococcal cover (vancomycin or an anti-staphylococcal penicillin) when the source is trauma, neurosurgery or a shunt; consider cover for Gram-negatives and Pseudomonas with an agent such as ceftazidime or meropenem for ear infection, and tailor antifungal or mycobacterial therapy to the setting. [3] [8]
Specific Subtypes & Scenarios
The child with cyanotic congenital heart disease is the classic high-risk scenario, because right-to-left shunting seeds the brain with bacteria that bypass the lungs. The abscesses are often multiple, sit at the grey–white junction, and may declare acutely; management is aspiration plus antibiotics, with timely cardiac repair once the infection is controlled to prevent recurrence. [11] [12]
Subdural empyema in the infant may complicate bacterial meningitis, presenting with seizures, bulging fontanelle, sepsis and rapid neurological decline; it is an emergency requiring urgent drainage. Sinogenic subdural or epidural empyema in older children presents with severe headache, fever and focal signs, and is managed with combined endoscopic sinus surgery and neurosurgical drainage. [9] [10]
A typical parenchymal abscess: the temporal arc
The immunocompromised child — neutropenic, post-transplant, or with advanced HIV — may harbour fungal (Aspergillus, Candida) or unusual bacterial pathogens, requires broader empiric cover and tissue diagnosis, and carries a higher mortality. A post-traumatic or post-surgical abscess is more likely staphylococcal and needs anti-staphylococcal therapy plus removal of any retained foreign body or infected hardware. [6] [7]
Complications & Pitfalls
The complications of brain abscess are dominated by its anatomical and neurological consequences. Rupture into the ventricular system is the most feared — it produces sudden, catastrophic collapse with ventriculitis, hydrocephalus and a very high mortality. Herniation from mass effect, seizures (including late epilepsy), focal neurological deficit, and venous sinus thrombosis with venous infarction are the other major threats. [1] [2]
The common pitfalls are diagnostic and therapeutic. Waiting for the classic triad delays imaging; the triad is present in fewer than a quarter of children. Performing a lumbar puncture in the presence of a mass risks herniation and adds no useful information. Starting broad antibiotics before obtaining pus sterilises the culture and forces weeks of blind therapy. Treating a subdural empyema with antibiotics and a repeat scan rather than urgent surgery allows fulminant progression. And using corticosteroids routinely may dampen inflammation and capsule formation, so they should be reserved for severe mass effect and tapered as soon as possible. [9] [13]
[3]Prognosis & Disposition
Mortality from brain abscess in children has fallen with modern imaging and neurosurgery but remains in the range of four to twelve per cent, and it is higher in infants, the immunocompromised, and posterior-fossa or subdural disease. Among survivors, a substantial minority are left with epilepsy, hemiparesis, visual-field or cognitive and behavioural sequelae, the full extent of which often emerges only over years of neurodevelopmental follow-up. [2] [5]
Disposition depends on the stage and the response. The child is admitted for intravenous antibiotics, neurosurgical and intensive-care input as needed, and source control; transfer to a centre with paediatric neurosurgery and infectious diseases is arranged early for any child who cannot be managed locally. The duration of intravenous therapy is typically four to six weeks, extended to six to eight weeks for larger, multiloculated or surgically excised lesions, guided by the clinical course, inflammatory markers and serial imaging. [3] [1]
Transition to oral therapy is considered only when the child is afebrile and clinically improved, inflammatory markers are falling, source control is complete, and a suitable oral agent with good bioavailability and susceptibility is available — and always with a plan for close follow-up and imaging. [3] [5]
Special Populations
Infants and very young children are at higher risk of poor outcome because the diagnosis is delayed — the symptoms are non-specific, the fontanelle is a late sign, and subdural empyema complicating meningitis can evolve rapidly. A low threshold for imaging is essential in any febrile infant with irritability, vomiting, a bulging fontanelle or seizures. [7] [9]
Children with complex chronic conditions and immunocompromise — post-stem-cell transplant, on biologics, neutropenic, or with advanced HIV — may harbour unusual organisms and need broader empiric cover and tissue diagnosis. Indigenous, refugee and remote-living children may present late with untreated cyanotic heart disease or chronic ear disease, so culturally safe assessment and prompt retrieval are part of the standard of care. [12] [6]
Evidence, Guidelines & Regional Differences
| Region | Key guideline | Empiric backbone | Corticosteroids |
|---|
The corticosteroid question deserves a specific viva answer. A systematic review and meta-analysis found that dexamethasone use was associated with higher mortality in brain abscess, although confounding by severity limits causal inference; the consensus is that corticosteroids should be reserved for significant mass effect or impending herniation, used at the lowest effective dose, and tapered as soon as the oedema settles. [13] [3]
Exam Pearls
References
- [1]Brouwer MC, Tunkel AR, McKhann GM II, van de Beek D Brain abscess. N Engl J Med, 2014.PMID 25075836
- [2]Brouwer MC, Coutinho JM, van de Beek D Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology, 2014.PMID 24477107
- [3]Bodilsen J, Brouwer MC, van de Beek D, et al. European society of Clinical Microbiology and Infectious Diseases guidelines on diagnosis and treatment of brain abscess in children and adults. Clin Microbiol Infect, 2024.PMID 37648062
- [4]Mameli C, Dilillo D, Bedogni L, et al. Brain abscess in pediatric age: a review. Childs Nerv Syst, 2019.PMID 31062139
- [5]Gilard V, Hénaux L, Gras-Le Guen C, et al. Brain abscess in children, a two-centre audit: outcomes and controversies. Arch Dis Child, 2020.PMID 31431437
- [6]Bonfield CM, Sharma J, Dobson S Pediatric intracranial abscesses. J Infect, 2015.PMID 25917804
- [7]Sahbudak Bal Z, Güngör S, Üstünbaş G, et al. Brain Abscess in Children: A Rare but Serious Infection. Clin Pediatr (Phila), 2018.PMID 28969451
- [8]Brook I Brain abscess in children: microbiology and management. J Child Neurol, 1995.PMID 7594262
- [9]Muzumdar D Subdural empyema in children. Childs Nerv Syst, 2018.PMID 30014307
- [10]Garin A, Thierry B, Leboulanger N, et al. Pediatric sinogenic epidural and subdural empyema: The role of endoscopic sinus surgery. Int J Pediatr Otorhinolaryngol, 2015.PMID 26304070
- [11]Udayakumaran S, Onyia CU, Lenoble L Forgotten? Not Yet. Cardiogenic Brain Abscess in Children: A Case Series-Based Review. World Neurosurg, 2017.PMID 28780403
- [12]Atiq M, Ahmed US, Allana SS, et al. Brain abscess in children. Indian J Pediatr, 2006.PMID 16741324
- [13]Simjian T, Lehrer M, Jesselson K, et al. Dexamethasone Administration and Mortality in Patients with Brain Abscess: A Systematic Review and Meta-Analysis. World Neurosurg, 2018.PMID 29705232
- [14]Sáez-Llorens X, McCracken GH Jr Brain abscess. Handb Clin Neurol, 2013.PMID 23622320
- [15]Sheehan JP, Jane JA, Ray DK, et al. Brain abscess in children. Neurosurg Focus, 2008.PMID 18518751