Paeds · investigations-procedures-and-technology
Abdominal radiograph and acute imaging decisions
Also known as Abdominal radiograph · Abdominal X-ray · AXR · Plain film of the abdomen · Acute abdominal imaging · Imaging modality selection · ALARA in children · Radiation-aware paediatric imaging
Fellowship guide to the abdominal radiograph and the acute paediatric imaging decision. Covers when an abdominal radiograph answers the question (suspected perforation, obstruction, constipation burden, and the ingested foreign body or button battery) and when it does not, the low diagnostic yield of the radiograph in non-specific abdominal pain, the ALARA principle and the cancer-risk evidence that underpins it, the ultrasound-first pathway for appendicitis and intussusception, the role of the upper gastrointestinal contrast study for malrotation and midgut volvulus, and the careful, lowest-dose use of computed tomography when ultrasound is equivocal and the child is unstable or complex. Reproduces the radiographic signs of free air, obstruction, the intussusception target sign, and neonatal pneumatosis, and the regional guidelines that govern the choices.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
The abdominal radiograph is the oldest plain-film investigation of the acute paediatric abdomen, and the imaging decision it sits inside has changed more in the last two decades than any other part of the paediatric workup. The question is no longer "what does the abdominal X-ray show" but "which modality, if any, answers the clinical question at the lowest radiation dose". The abdominal radiograph, the ultrasound, the computed tomography scan, and the contrast study each answer a different question, and choosing the wrong one wastes time, adds radiation, and can still miss the diagnosis. This page is about that choice. [2][3]
The abdominal radiograph itself is a single supine film of the abdomen that shows the bowel gas pattern, the calcifications, the air-fluid interfaces when an erect or a decubitus view is added, and any radiopaque foreign body. Its genuine strengths are narrow: it confirms the free air of a perforation, the dilated loops of an obstruction, the radiopaque foreign body or button battery, and sometimes the constipation burden. Its weakness is that it has a very low yield in the well child with non-specific abdominal pain, it rarely changes the management in that setting, and it delivers a small radiation dose that is not justified when the question is better answered by ultrasound. The guidelines are consistent on this point. [7][8]
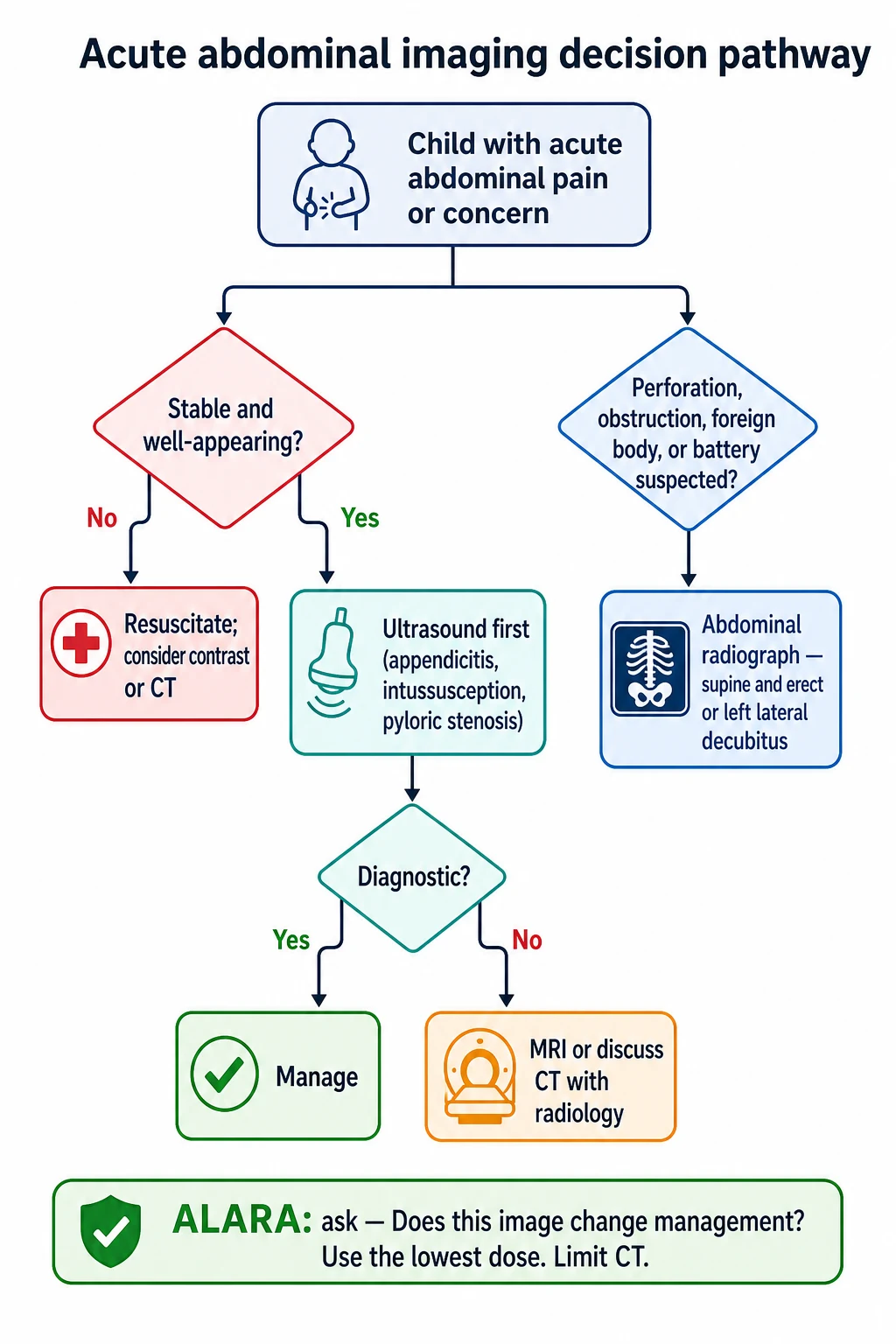
The imaging decision rests on three principles that run through every section of this page. The first is the ALARA principle, that the radiation dose should be As Low As Reasonably Achievable, because the young child carries a small but real lifetime cancer risk from ionising radiation that is higher than the adult's. The second is the modality match, that each clinical question has a best first test, and that ultrasound is usually the first test in the child because it uses no ionising radiation. The third is the imaging pathway, that the result of the first test drives the next step rather than requesting everything at once. The Pearce 2012 cohort study linked computed tomography scans in childhood to a small increase in the later risk of leukaemia and brain tumours, and that evidence underpins the modern radiation-aware practice. [1][2]
Classification
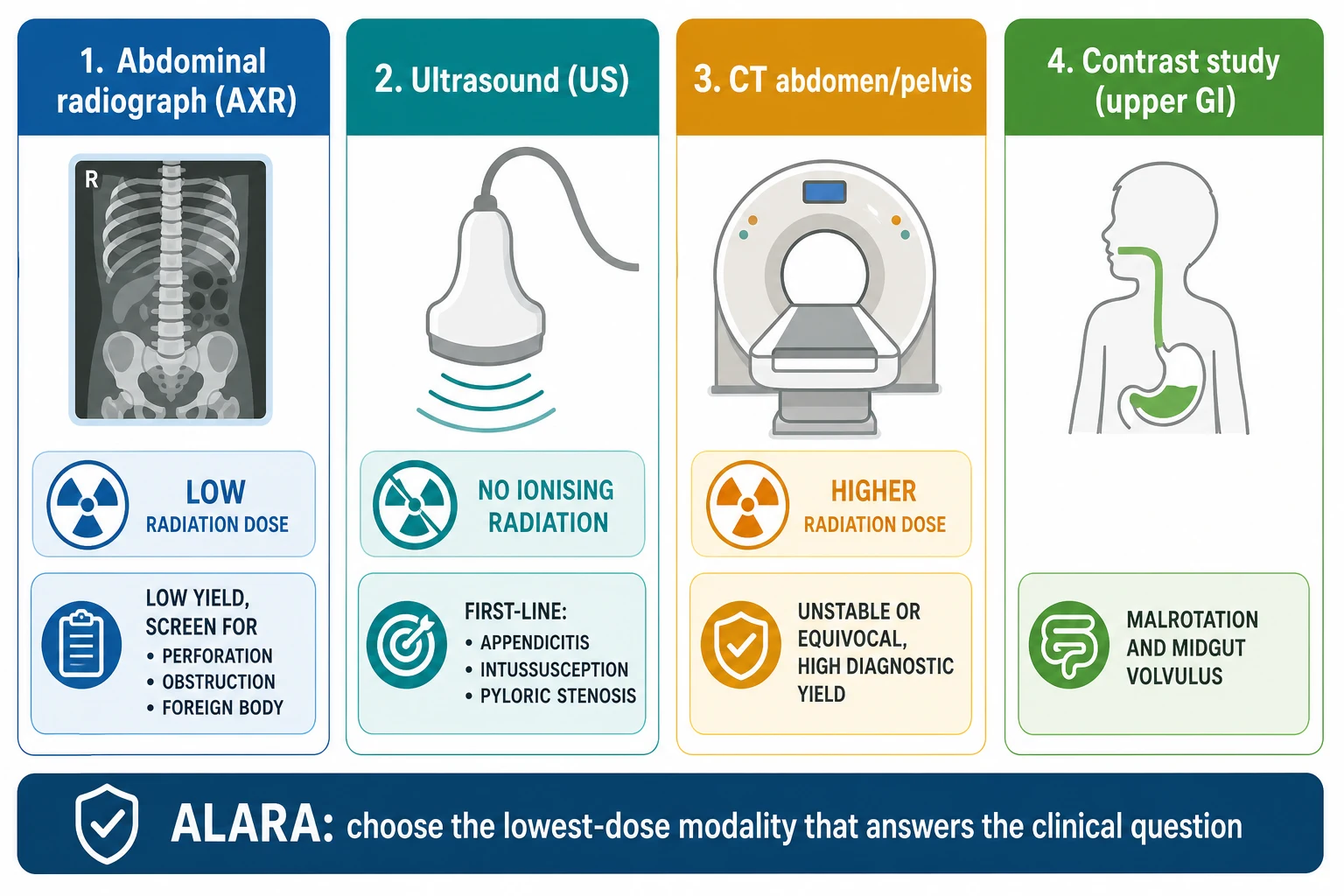
The classification of the imaging modalities rests on the question each one answers and the radiation dose each one delivers. The abdominal radiograph delivers a low dose of ionising radiation, roughly 0.05 to 0.7 millisieverts for a single supine film depending on the technique and the equipment, and it answers the structural questions of free air, obstruction, and the radiopaque foreign body. The ultrasound delivers no ionising radiation and answers the soft-tissue and the dynamic questions of appendicitis, intussusception, and pyloric stenosis, and it is the default first test in the child wherever it is available. [2]
The computed tomography scan delivers the highest dose, roughly 2 to 10 millisieverts for an abdomen and pelvis in a child when it is not dose-modified for size, and it answers the question that ultrasound cannot answer in the unstable, the obese, or the complex child. The upper gastrointestinal contrast study delivers a low-to-moderate dose and answers the specific question of malrotation with midgut volvulus by demonstrating the position of the duodenojejunal flexure. The fluoroscopic guidance for an enema reduction of an intussusception delivers a moderate dose and answers both the diagnostic and the therapeutic question in one sitting. [9]
The clinical consequence of the classification is the modality match. The radiograph is matched to the free-air and the obstruction question, the ultrasound to the appendicitis and the intussusception question, the contrast study to the malrotation question, and the computed tomography scan to the residual question that the others cannot answer. A radiograph requested for appendicitis is the wrong match, because it cannot see the appendix in the well child and it delivers a radiation dose without changing the management. A radiograph requested for constipation is also the wrong match, because functional constipation is a clinical diagnosis. The classification is therefore the foundation of the imaging decision. [7][8]
Epidemiology & Risk Factors
The abdominal radiograph remains one of the most frequently requested imaging studies in the paediatric emergency department, and the concern is that it is requested more often than the clinical question justifies. The epidemiological studies of the yield of the abdominal radiograph in children consistently report a low rate of clinically meaningful findings in the well child with non-specific abdominal pain, and a substantial proportion of the radiographs change nothing about the management. The overuse is the epidemiological signature of the imaging decision gone wrong. [12]
The risk factors for an unnecessary radiograph are the non-specific presentation, the absence of a focal finding, the request made before the clinical assessment is complete, and the habit of ordering the film as a routine. The well child with abdominal pain that resolves, the child with constipation in whom the diagnosis is already clinical, and the child with gastroenteritis in whom the film cannot change the management are the common overuse scenarios. The risk factors for a missed diagnosis are the opposite: the child in whom the radiograph is requested instead of the ultrasound for appendicitis or intussusception, and the film is normal or non-specific, and the diagnosis is delayed. [3]
The epidemiology of the radiation risk is the reason the overuse matters. The Pearce 2012 retrospective cohort study of nearly 180,000 children who had computed tomography scans in the United Kingdom estimated a small but statistically significant increase in the risk of leukaemia and brain tumours with increasing cumulative dose, and the authors concluded that although the absolute risk was small, the practice of radiation-aware imaging in the young child was justified by the evidence. The Image Gently campaign of the Alliance for Radiation Safety in Pediatric Imaging translated that evidence into the practical guidance that every scan in a child must be justified, dose-modified, and limited to the region that answers the question. [1][2]
The epidemiological shift in the imaging practice is the move from the radiograph to the ultrasound for the common acute presentations, and the move from the computed tomography scan to the ultrasound or the magnetic resonance imaging for the equivocal case. The clinical pathway for suspected appendicitis, supported by the pARC risk calculator of Kharbanda and colleagues and the ACR Appropriateness Criteria, uses ultrasound first and reduces the computed tomography rate without compromising the diagnostic accuracy. The study by Barricelli and colleagues confirmed that the implementation of a clinical pathway for suspected appendicitis reduced the computed tomography utilisation, and the wider trend is the deliberate, evidence-based reduction of the radiation dose in the paediatric imaging. [3][4][12]
Pathophysiology
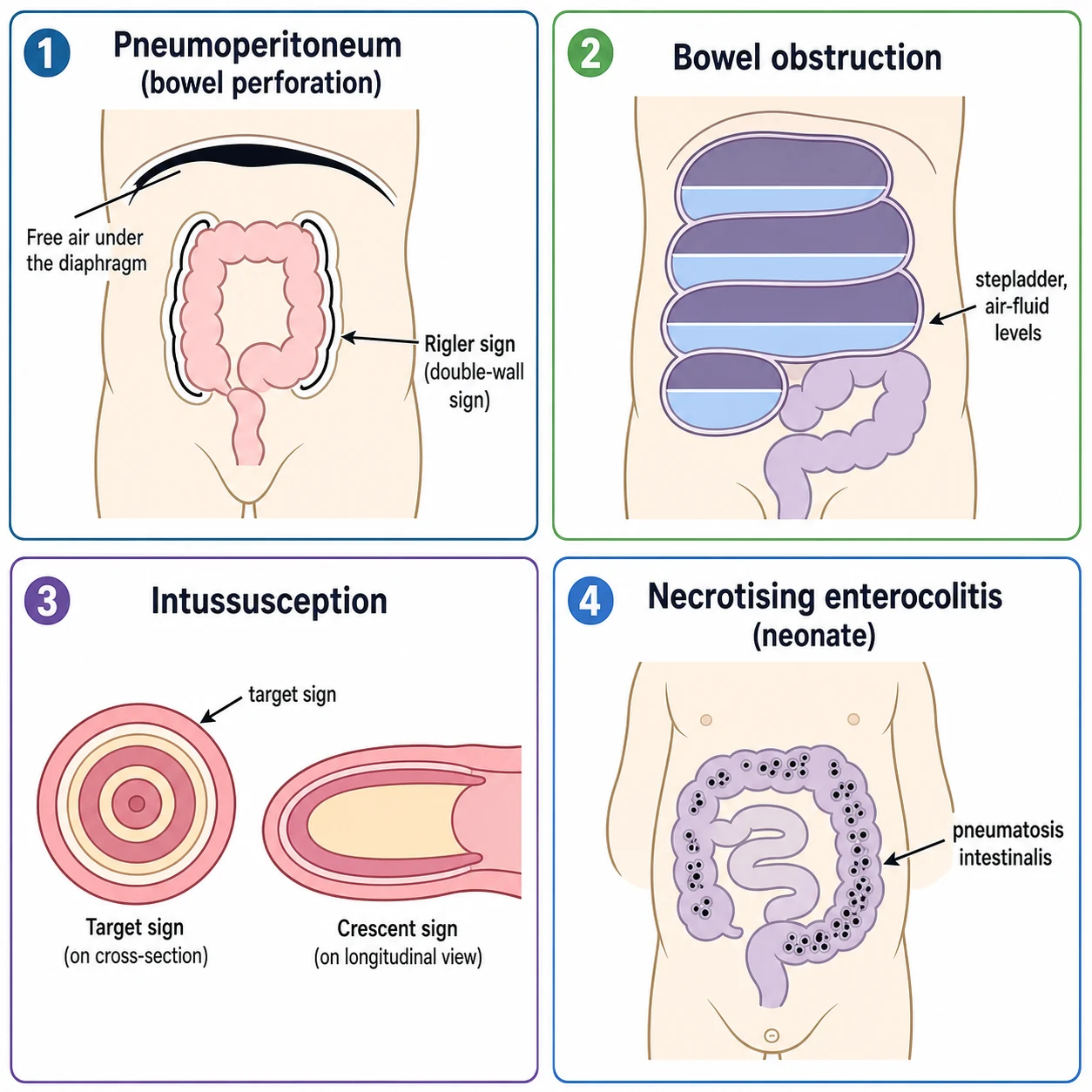
The pathophysiology behind the radiographic signs explains why the abdominal film answers some questions and not others. The free air of a bowel perforation rises to the highest part of the peritoneal cavity, which is why the erect chest radiograph or the left lateral decubitus abdominal film demonstrates it as a curved lucency beneath the diaphragm or beneath the lateral abdominal wall. The supine film alone can miss the free air, because the air disperses across the anterior abdomen and only the Rigler sign, the visualisation of both sides of the bowel wall outlined by air on the luminal side and the free air on the peritoneal side, betrays it. The addition of the erect or the decubitus view is therefore the rule when perforation is genuinely suspected. [10]
The bowel obstruction distends the loops proximal to the blockage with gas and fluid, and the radiograph shows the dilated loops stacked in the stepladder pattern with multiple air-fluid levels on the erect view. The neonatal obstruction from the atresia, the meconium plug, or the Hirschsprung disease shows the disproportion between the dilated proximal loops and the unused distal bowel. The adult and the older-child obstruction from the adhesion or the hernia shows the central ladder pattern. The radiograph confirms the obstruction but rarely names the cause, and the contrast study or the computed tomography scan is the next step when the cause matters. [9]
The intussusception produces the target sign on the abdominal radiograph, the concentric rings of the telescoped bowel seen end-on, and the crescent sign of the soft-tissue mass with the meniscus of the intraluminal gas. The radiograph is neither sensitive nor specific enough to rule the intussusception in or out, and the ultrasound is the diagnostic test of choice because it demonstrates the target lesion and the pathological lead point in the hands of an experienced operator. The pneumatosis intestinalis of the neonatal necrotising enterocolitis is the bubbly or the linear lucency in the bowel wall that marks the gas in the submucosa and the subserosa, and the portal venous gas is the branching lucency in the liver that marks the advanced disease. [5][10]
Clinical Presentation
The clinical presentations that trigger the imaging decision are the acute abdominal pain, the bilious vomiting, the suspected perforation or the obstruction, the suspected foreign body or button battery ingestion, and the neonatal abdominal emergency. Each presentation drives a different first test, and the role of the abdominal radiograph differs in each. The well child with the non-specific abdominal pain is the presentation in which the radiograph has the lowest yield, and the imaging decision favours either no imaging or the ultrasound depending on the focality of the pain. [3]
The child with the suspected perforation presents with the severe abdominal pain, the rigid abdomen, and the signs of peritonitis or sepsis. The imaging decision here favours the abdominal radiograph with the erect chest or the left lateral decubitus view to confirm the free air, and the computed tomography scan if the cause or the extent needs further definition. The child with the suspected obstruction presents with the colicky pain, the distension, the vomiting, and the failure to pass stool or flatus, and the abdominal radiograph confirms the dilated loops and the air-fluid levels. [9]
The presentations that drive the imaging decision
The well child with the non-specific abdominal pain: no imaging or ultrasound, not the radiograph
The child with the focal right-lower-quadrant pain: ultrasound for the appendicitis, using the pARC score to stratify the risk
The infant with the episodic colicky pain and the currant-jelly stool: ultrasound for the intussusception
The infant with the bilious vomiting: upper gastrointestinal contrast study for the malrotation and the midgut volvulus
The child with the rigid abdomen and the peritonitis: abdominal radiograph with the erect or decubitus view for the free air
The child with the suspected button battery ingestion: radiograph to localise the battery
The neonate with the abdominal distension and the bloody stool: abdominal radiograph for the necrotising enterocolitis
The infant with the bilious vomiting is the presentation in which the imaging decision is the most time-critical, because the malrotation with the midgut volvulus can infarct the entire small bowel within hours. The bilious vomit in the infant is a surgical emergency until proven otherwise, and the upper gastrointestinal contrast study demonstrating the abnormal position of the duodenojejunal flexure is the diagnostic test. The child with the suspected button battery ingestion is the presentation in which the radiograph is the single most useful test, because a battery lodged in the oesophagus can perforate into the aorta or the trachea within hours and the radiograph localises it immediately. [9][11]
Differential Diagnosis
The differential at the imaging-decision level is the choice of the modality for the clinical question. For the right-lower-quadrant pain, the differential is the appendicitis, the mesenteric adenitis, the ovarian pathology, and the ureteric stone, and the ultrasound is the first test because it addresses the first three and the radiation-free assessment of the pelvis. For the episodic colicky pain in the infant, the differential is the intussusception, and the ultrasound is the diagnostic test. For the bilious vomiting, the differential is the malrotation with the midgut volvulus, and the upper gastrointestinal contrast study is the test. [5][9]
The second distinction is between the diagnostic and the therapeutic imaging. The ultrasound and the contrast study are the diagnostic tests that name the problem, and the enema under the fluoroscopic or the ultrasound guidance is the therapeutic test that reduces the intussusception at the same sitting. The abdominal radiograph is rarely therapeutic, because it does not treat anything, and its role is the confirmation of the structural problem that the clinical team then acts on. The computed tomography scan is occasionally therapeutic in the sense that it guides the drainage of the abscess, but its primary role is the diagnostic. [6]
Abdominal radiograph
- Low yield in the non-specific abdominal pain
- Confirms the free air, the obstruction, and the radiopaque foreign body
- Not needed for the clinical diagnosis of the functional constipation
- A small radiation dose that must be justified
Ultrasound
- First-line for the appendicitis, the intussusception, and the pyloric stenosis
- No ionising radiation, the default first test in the child
- Operator-dependent, limited by the bowel gas and the body habitus
- Answers the soft-tissue and the dynamic questions
Computed tomography
- Highest radiation dose, reserve for the equivocal or the unstable
- High diagnostic yield, fast, and not operator-dependent
- Dose-modified to the size of the child under the ALARA principle
- The justified second-line when the ultrasound is non-diagnostic
Contrast study
- Upper GI for the malrotation and the midgut volvulus
- Enema for the therapeutic reduction of the intussusception
- Low to moderate radiation dose
- Answers the specific anatomical question
The third distinction is between the child who needs the imaging now and the child who needs the resuscitation first. The unstable child with the acute abdomen is resuscitated before the definitive imaging, and the FAST scan, the focused assessment with sonography for trauma, or the plain film is the bridge to the definitive study. The child with the peritonitis and the sepsis may go to the theatre on the clinical findings and the free air on the film, without the computed tomography scan that the stable child would have. The imaging decision is therefore the clinical judgement of the team, and the modality is the last piece of the pathway rather than the first. [9]
Clinical & Bedside Assessment
The bedside assessment before the imaging request is the foundation of the radiation-aware practice. Confirm the clinical question that the imaging must answer, because the modality is chosen to answer the question and not to screen the abdomen. Examine the abdomen for the focality of the pain, the distension, the rigidity, the mass, and the hernial orifices, and assess the hydration, the perfusion, and the conscious state. The focality of the pain drives the ultrasound for the appendicitis, the distension drives the radiograph for the obstruction, and the rigidity drives the radiograph with the erect or decubitus view for the free air. [3]
The risk stratification for the appendicitis is the practical example of the bedside assessment driving the imaging decision. The pARC calculator of Kharbanda and colleagues uses the age, the sex, the pain duration, the migration of the pain, the tenderness in the right lower quadrant, the guarding, the rebound, the anorexia, and the nausea to estimate the probability of the appendicitis, and the high-probability child proceeds to the surgical review with or without the ultrasound, and the intermediate-probability child has the ultrasound as the deciding test. The calculator is the formal version of the clinical judgement that every clinician applies at the bedside. [4]
The communication with the radiologist is the part of the bedside assessment that is most often omitted. The request that states the clinical question, the relevant findings, and the specific concern allows the radiologist to choose the right protocol, the right modality, and the right sequence. The request that simply asks for the abdominal film without the clinical context is the one most likely to be unhelpful, because the radiologist cannot redirect the study to the question that was not stated. The discussion before the computed tomography scan is especially important, because the radiologist may suggest the ultrasound or the magnetic resonance imaging that the requesting team had not considered. [2][3]
Investigations
The investigation here is the imaging study itself, and the interpretation is the integration of the radiographic or the sonographic findings with the clinical picture. The abdominal radiograph is interpreted for the bowel gas pattern, the free air, the calcifications, and the foreign body. The free air on the erect chest or the decubitus film is the surgical finding, and the Rigler sign on the supine film is the secondary clue. The dilated loops proximal to the obstruction and the absence of the gas distally mark the obstruction, and the stepladder pattern with the air-fluid levels on the erect view confirms it. [9]
The ultrasound is interpreted for the appendix, the intussusception, the pylorus, and the pelvic organs. The non-compressible appendix with the outer diameter greater than 6 millimetres and the wall thickening marks the appendicitis, and the target lesion with the alternating echogenic and hypoechoic rings marks the intussusception. The pyloric channel length and the wall thickness mark the hypertrophic pyloric stenosis. The limitation of the ultrasound is the operator dependence and the interference by the bowel gas, and the non-diagnostic scan in the obese or the uncooperative child is the bridge to the computed tomography or the magnetic resonance imaging. [5]
The upper gastrointestinal contrast study is interpreted for the position of the duodenojejunal flexure, which normally lies to the left of the spine at the level of the pylorus in the well-rotated bowel. The flexure that lies to the right of the spine, or low and central, marks the malrotation, and the corkscrew or the bird-beak appearance of the duodenum marks the midgut volvulus. The contrast enema is interpreted for the intussusception and the reduction, with the coiled-spring or the claw sign of the intussusceptum and the reflux of the contrast into the terminal ileum marking the successful reduction. [5][9]
The computed tomography scan is interpreted for the appendicitis, the obstruction, the perforation, the abscess, and the mass that the ultrasound missed. The scan is dose-modified to the size of the child, the region is limited to the question, and the intravenous contrast is used when the soft-tissue detail is needed. The magnetic resonance imaging is the radiation-free alternative for the child in whom the ultrasound is non-diagnostic and the computed tomography is to be avoided, and it is increasingly used for the appendicitis and the inflammatory bowel disease in the centres that have the access and the expertise. [3][12]
Management — Resuscitation
The resuscitation comes before the imaging in the unstable child with the acute abdomen. The airway, the breathing, and the circulation are addressed first, the intravenous access is obtained, the fluid bolus of 10 millilitres per kilogram of the isotonic saline is given for the shock, and the empirical antibiotics are started for the suspected perforation or the sepsis. The imaging is requested once the child is stable enough to leave the resuscitation bay, and the FAST scan or the portable film is the bridge in the child who is too unstable to move. [9]
The analgesia does not obscure the abdomen and is the standard of care. The morphine at 0.05 to 0.1 milligrams per kilogram intravenously, or the fentanyl at 1 to 2 micrograms per kilogram, relieves the pain and allows the better examination, and the modern evidence confirms that the opioid analgesia does not mask the peritonitis or the surgical abdomen. The withholding of the analgesia to preserve the examination is the outdated practice that the guidelines do not support. [3]
Analgesia for the acute abdominal pain in the child before the imaging
Dose
Morphine 0.05 to 0.1 mg per kg intravenously, or fentanyl 1 to 2 micrograms per kg
The imaging decision in the resuscitation is the modality that answers the question in the shortest time. The child with the rigid abdomen and the free air on the film goes to the theatre on the radiograph, without the computed tomography scan that would add the time and the radiation. The child with the equivocal ultrasound and the suspected appendicitis has the computed tomography scan or the surgical review, and the decision is the joint one of the surgical and the radiological team. The child with the intussusception and the peritonitis may bypass the imaging and go to the theatre for the exploratory laparotomy. [5][6]
Management — Definitive & Stepwise
[3]The definitive stepwise management is the application of the modality match and the ALARA principle to the clinical scenario. For the suspected appendicitis, the pathway is the clinical risk stratification with the pARC score, the ultrasound as the first imaging study, the surgical review for the high-probability case, and the computed tomography or the magnetic resonance imaging for the equivocal case after the radiology discussion. The ACR Appropriateness Criteria recommend the ultrasound as the first study in the child with the suspected appendicitis, and the computed tomography as the reserved second-line. [3][4]
For the suspected intussusception, the pathway is the ultrasound as the diagnostic test, and the enema under the fluoroscopic or the ultrasound guidance as the therapeutic reduction. The Daneman and Navarro review of the diagnostic approaches confirmed the ultrasound as the first test, and the Navarro study of the delayed and the repeated reduction attempts established the practice that the failed first enema reduction can be followed by the delayed repeat attempt in the stable child, with the surgery reserved for the failed reduction, the peritonitis, or the pathological lead point. [5][6]
For the suspected malrotation with the midgut volvulus, the pathway is the upper gastrointestinal contrast study as the urgent diagnostic test, and the surgery as the definitive treatment. The pictorial essay of Choi and colleagues on the gastrointestinal emergencies in the neonates and the infants illustrated the radiographic and the contrast findings of the malrotation, the volvulus, and the obstruction, and the principle that the contrast study is the test when the plain film is non-specific and the bilious vomiting raises the concern. [9]
ASK for the radiation-aware imaging request
For the suspected necrotising enterocolitis in the neonate, the pathway is the abdominal radiograph for the pneumatosis intestinalis, the portal venous gas, and the free air of the perforation, and the surgery for the perforation or the clinical deterioration despite the medical management. The Rich and Dolgin review in the Pediatrics in Review summarised the diagnostic and the management framework, with the Bell staging of the suspected, the confirmed, and the advanced disease, and the radiographic signs that mark each stage. [10]
Specific Subtypes & Scenarios
The suspected button battery ingestion is the scenario in which the abdominal radiograph is the single most useful test. The battery lodged in the oesophagus can perforate into the aorta or the trachea within hours, and the radiograph localises the battery as the double-ring or the halo sign of the coin-cell, distinct from the uniform disc of the coin. The European Society for Paediatric Gastroenterology, Hepatology and Nutrition position paper of Mubarak and colleagues recommended the radiograph for every suspected button battery ingestion, and the urgent endoscopic removal of the oesophageal battery, with the observation or the removal of the gastric battery depending on the size and the symptoms. [11]
The suspected appendicitis is the scenario in which the ultrasound-first pathway is the best supported. The ACR Appropriateness Criteria, the pARC calculator, and the clinical pathway studies all converge on the ultrasound as the first imaging study, with the computed tomography reserved for the equivocal or the unstable child. The study by Barricelli and colleagues confirmed that the clinical pathway reduced the computed tomography utilisation, and the principle is that the radiation-aware pathway maintains the diagnostic accuracy while reducing the dose. [3][4][12]
[2]The suspected malrotation with the midgut volvulus is the scenario in which the imaging decision is the most time-critical. The bilious vomiting in the infant is the surgical emergency, and the upper gastrointestinal contrast study is the diagnostic test. The delay for the less-urgent imaging or the overnight observation is the avoidable cause of the short bowel syndrome, and the principle is that the green vomit in the infant is the malrotation and the volvulus until the contrast study proves otherwise. The child with the recurrent vomiting and the failure to thrive may have the malrotation without the acute volvulus, and the elective contrast study is the appropriate test. [9]
The suspected functional constipation is the scenario in which the abdominal radiograph is the most overused. The NASPGHAN 2006 guideline and the ESPGHAN and NASPGHAN 2014 update by Tabbers and colleagues stated that the functional constipation is a clinical diagnosis based on the Rome criteria, and the abdominal radiograph is not needed to confirm it because the correlation between the radiographic stool burden and the clinical picture is poor. The radiograph is reserved for the atypical case in which the obstruction or the anatomical cause is suspected, and the principle is that the clinical diagnosis is the standard. [7][8]
Complications & Pitfalls
The complications of the imaging decision are the missed diagnosis and the unnecessary radiation. The missed diagnosis arises when the radiograph is requested instead of the ultrasound for the appendicitis or the intussusception, and the non-specific film reassures the team falsely and the diagnosis is delayed. The unnecessary radiation arises when the radiograph is requested for the non-specific abdominal pain or the functional constipation, and the small dose is delivered without the clinical benefit. The complications are the two sides of the imaging decision, and the avoidance of both is the modality match and the ALARA principle. [3][7]
The missed free air is the classic pitfall of the single supine film. The free air disperses across the anterior abdomen on the supine film, and only the Rigler sign betrays it. The addition of the erect chest or the left lateral decubitus view is the rule when the perforation is genuinely suspected, and the failure to add the view is the avoidable cause of the missed perforation. The over-reliance on the radiograph for the appendicitis is the second pitfall, because the film cannot see the appendix in the well child and the ultrasound is the first test. [10]
The third pitfall is the overuse of the computed tomography scan in the child. The Pearce 2012 cohort study linked the childhood computed tomography to the small increase in the leukaemia and the brain tumour risk, and the practice of the radiation-aware imaging follows from the evidence. The computed tomography scan that is not dose-modified to the size of the child, that covers more than the region of the question, or that is requested without the prior ultrasound or the radiology discussion is the avoidable radiation exposure. The Image Gently campaign translated the evidence into the practical guidance that the dose must be justified, modified, and limited. [1][2]
The fourth pitfall is the delay in the contrast study for the suspected malrotation with the midgut volvulus. The bilious vomiting in the infant is the surgical emergency, and the delay for the less-urgent imaging or the overnight observation is the avoidable cause of the short bowel syndrome. The fifth pitfall is the failure to localise the button battery in the suspected ingestion, because the battery in the oesophagus is the emergency and the radiograph is the test. [9][11]
Prognosis & Disposition
The prognosis after the imaging decision is the prognosis of the underlying condition and the timeliness of the diagnosis. The well child with the non-specific abdominal pain and the normal or the ultrasound imaging has the excellent prognosis, and the discharge with the safety net is the disposition. The child with the confirmed appendicitis and the timely ultrasound has the good prognosis, and the appendicectomy is the definitive treatment. The child with the malrotation and the timely contrast study has the good prognosis, and the Ladd procedure is the definitive treatment. [5][9]
The child with the delayed diagnosis has the prognosis of the complication. The delayed appendicitis with the perforation and the abscess has the longer hospital stay and the higher complication rate. The delayed malrotation with the volvulus and the bowel infarction has the short bowel syndrome and the lifetime dependence on the parenteral nutrition. The delayed intussusception with the perforation and the peritonitis has the higher morbidity. The imaging decision is the link between the timely diagnosis and the good prognosis, and the radiation-aware practice is the link between the diagnosis and the lowest-harm pathway. [6][10]
The disposition after the imaging is the integration of the findings with the clinical picture. The child with the diagnostic ultrasound and the appendicitis is referred to the surgery. The child with the diagnostic ultrasound and the intussusception proceeds to the enema reduction. The child with the diagnostic contrast study and the malrotation proceeds to the surgery. The child with the non-diagnostic ultrasound and the persistent concern has the computed tomography or the magnetic resonance imaging after the radiology discussion, or the surgical review on the clinical findings. The child with the normal imaging and the resolving symptoms is discharged with the safety net. [5][9]
Special Populations
The neonate and the young infant are the population in which the radiation sensitivity is the highest and the imaging decision is the most consequential. The neonatal necrotising enterocolitis is the emergency that the abdominal radiograph addresses with the pneumatosis and the free air, and the premature infant is the highest-risk group. The malrotation with the midgut volvulus is the emergency that the upper gastrointestinal contrast study addresses, and the infant with the bilious vomiting is the presentation. The radiation dose is minimised by the size-specific protocols and the justification of every study. [10]
The child with the complex chronic and the technology-dependent condition has the higher exposure to the imaging and the higher cumulative radiation dose over the lifetime. The child with the inflammatory bowel disease, the recurrent pancreatitis, the surgical short bowel, and the oncology follow-up accumulates the computed tomography and the fluoroscopy dose, and the radiation-aware practice is the substitution of the magnetic resonance imaging and the ultrasound wherever possible. The cumulative dose is the relevant metric for the cancer risk, and the tracking of the dose over the years is the modern practice. [1][2]
The child from the remote and the rural setting has the imaging pathway shaped by the access. The ultrasound and the plain film at the point of care are the first tests, and the tele-radiology discussion guides the decision before the transfer. The transfer for the definitive imaging is the decision that balances the risk of the delay against the risk of the missed diagnosis, and the principle is that the unstable child is resuscitated and stabilised before the transfer. Aboriginal and Torres Strait Islander children and the children from the migrant and the refugee backgrounds have the higher threshold for the access and the importance of the culturally appropriate communication about the imaging and the radiation. [9]
The child with the suspected non-accidental injury is the population in which the imaging is the part of the safeguarding assessment. The skeletal survey, the computed tomography of the head, and the abdominal imaging are the components of the protocol, and the radiation dose is justified by the safeguarding question. The principle is that the imaging in the safeguarding context is the specialist, protocolised assessment, and the radiation-aware practice is the application of the same ALARA principle to the justified study. [2]
Evidence, Guidelines & Regional Differences
The evidence base spans the radiation-risk studies, the modality-selection guidelines, and the clinical pathway studies. The Pearce 2012 retrospective cohort study of the childhood computed tomography scans in the United Kingdom estimated the small increase in the leukaemia and the brain tumour risk with the increasing cumulative dose, and the authors concluded that the radiation-aware practice was justified by the evidence. The Image Gently campaign of the Alliance for Radiation Safety in Pediatric Imaging, described by Frush and Goske, translated the evidence into the practical guidance for the dose optimisation and the justification. [1][2]
The ACR Appropriateness Criteria for the suspected appendicitis in the child, authored by Koberlein and the Expert Panel on Pediatric Imaging, recommend the ultrasound as the first imaging study and the computed tomography as the reserved second-line. The pARC calculator of Kharbanda and colleagues, developed and validated in the paediatric emergency departments, stratifies the probability of the appendicitis and guides the imaging decision. The patient-friendly summary by Romero translated the criteria into the family-facing language. [3][4]
Pearce 2012 Lancet
- Retrospective cohort of nearly 180000 children with CT scans
- Small increase in leukaemia and brain tumour risk with the cumulative dose
- Underpins the radiation-aware practice in the young child
ACR Appropriateness Criteria
- Ultrasound first for the suspected appendicitis in the child
- Computed tomography as the reserved second-line
- Koberlein and the Expert Panel on Pediatric Imaging
NASPGHAN and ESPGHAN
- Functional constipation is a clinical diagnosis
- Abdominal radiograph not needed to confirm
- Tabbers 2014 update of the 2006 guideline
Daneman and Navarro
- Ultrasound is the first test for the intussusception
- Delayed repeated enema reduction attempts in the stable child
- Surgery for the failed reduction, peritonitis, or pathological lead point
The NASPGHAN 2006 guideline on the constipation and the ESPGHAN and NASPGHAN 2014 update by Tabbers and colleagues established the functional constipation as the clinical diagnosis that does not require the abdominal radiograph to confirm, and the pictorial essay of Choi and colleagues on the gastrointestinal emergencies in the neonates and the infants illustrated the imaging of the malrotation, the volvulus, and the obstruction. The Rich and Dolgin review in the Pediatrics in Review summarised the necrotising enterocolitis, and the Mubarak position paper summarised the button battery ingestion. [7][8][9][10][11]
The regional differences centre on the access to the ultrasound, the magnetic resonance imaging, and the paediatric radiology expertise. In the well-resourced settings, the ultrasound-first pathway is the standard, the magnetic resonance imaging is the radiation-free alternative for the equivocal case, and the paediatric radiologist is available for the discussion. In the lower-resource settings, the plain film and the limited ultrasound are the available modalities, the computed tomography is used more readily, and the radiation-aware practice is applied with the available resources. The international guidelines, including the ACR Appropriateness Criteria, the NASPGHAN and ESPGHAN guidelines, and the ESPGHAN position papers, are applicable across the settings, with the intensity of the pathway and the access to the alternatives tailored to the local resources. [3][9]
Exam Pearls
AROMA for the acute paediatric abdominal imaging decision
References
- [1]Pearce MS, Salotti JA, Little MP, et al Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study Lancet, 2012.PMID 22681860
- [2]Frush DP, Goske MJ Image Gently: toward optimizing the practice of pediatric CT through resources and dialogue Pediatric Radiology, 2015.PMID 25680878
- [3]Koberlein GC, Trout AT, Rigsby CK, et al ACR Appropriateness Criteria: Suspected Appendicitis-Child Journal of the American College of Radiology, 2019.PMID 31054752
- [4]Kharbanda AB, Vazquez-Benitez G, Ballard DW, et al Development and Validation of a Novel Pediatric Appendicitis Risk Calculator (pARC) Pediatrics, 2018.PMID 29535251
- [5]Daneman A, Navarro O Intussusception. Part 1: a review of diagnostic approaches Pediatric Radiology, 2003.PMID 12557062
- [6]Navarro OM, Daneman A, Chae A Intussusception: the use of delayed, repeated reduction attempts and the management of intussusceptions due to pathologic lead points in pediatric patients AJR American Journal of Roentgenology, 2004.PMID 15100113
- [7]Constipation Guideline Committee of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition Evaluation and treatment of constipation in infants and children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition Journal of Pediatric Gastroenterology and Nutrition, 2006.PMID 16954945
- [8]Tabbers MM, DiLorenzo C, Berger MY, et al Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN Journal of Pediatric Gastroenterology and Nutrition, 2014.PMID 24345831
- [9]Choi G, Je BK, Kim YJ Gastrointestinal Emergency in Neonates and Infants: A Pictorial Essay Korean Journal of Radiology, 2022.PMID 34983099
- [10]Rich BS, Dolgin SE Necrotizing Enterocolitis Pediatrics in Review, 2017.PMID 29196510
- [11]Mubarak A, Benninga MA, Broekaert I, et al Diagnosis, Management, and Prevention of Button Battery Ingestion in Childhood: A European Society for Paediatric Gastroenterology Hepatology and Nutrition Position Paper Journal of Pediatric Gastroenterology and Nutrition, 2021.PMID 33555169
- [12]Barricelli E, Lo Cascio JN, Noiman A, et al CT Scan Utilization Decreases With Implementation of a Clinical Pathway for Children With Suspected Acute Appendicitis Pediatric Emergency Care, 2026.PMID 42011037