Paeds · investigations-procedures-and-technology
Echocardiography fundamentals for general paediatricians
Also known as Paediatric echocardiogram · Children's echo · Transthoracic echocardiography in children · Paediatric cardiac ultrasound · Echo report interpretation · Focused cardiac ultrasound in children
Fellowship guide to echocardiography fundamentals for the general paediatrician. Covers what each echo modality shows (two-dimensional anatomy, M-mode dimensions, colour and spectral Doppler flow and gradients), the standard paediatric imaging windows and the comprehensive transthoracic study, Z-score normalisation against body size, the high-yield indications (pathological murmur, cyanosis, heart failure, syncope with red flags), the modified Bernoulli equation and what a valve gradient means, how to read a paediatric echo report systematically, when a focused point-of-care cardiac ultrasound answers a binary question, the echo features of duct-dependent critical congenital heart disease and its prostaglandin resuscitation, and the boundary between the general paediatrician's competence and the paediatric cardiologist's.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the six-week-old infant referred for a heart murmur who feeds well and grows normally, the toddler with Kawasaki disease whose paediatrician needs to know whether the coronaries are involved, and the neonate who turns grey and breathless on day three of life as the ductus arteriosus closes. In each case the echocardiogram is the investigation that answers the structural and functional question, and the general paediatrician must understand what it can and cannot show. That is the territory this page owns. [1] [9]
An echocardiogram is the non-invasive, real-time ultrasound examination of the heart. A piezoelectric transducer placed on the chest wall emits and receives high-frequency sound waves — typically in the 2 to 12 megahertz range, with higher frequencies chosen for smaller children to trade depth penetration for the finer spatial resolution their thin chest walls allow — and the returning echoes are reconstructed into moving images of cardiac structure and blood flow. A comprehensive paediatric transthoracic echocardiogram sequences several imaging modalities through a standard set of acoustic windows to build a complete picture of anatomy, chamber size, ventricular function, valve competence, blood flow, and haemodynamics. [1] [12]
What distinguishes the paediatric echocardiogram from the adult study is the central role of congenital heart disease and the dependence of every measurement on body size. A child's heart is small and growing, so a left ventricular dimension of 30 millimetres is normal in a ten-year-old but grossly dilated in a six-month-old; the discipline of paediatric echo is to normalise every dimension against the child's body surface area and express it as a Z-score. The fellowship skill being tested is knowing when to order an echo, what each modality and measurement tells you, how to read the report systematically, and which findings the general paediatrician must escalate immediately rather than wait for routine clinic review. [1] [7]
Classification
The paediatric echocardiogram is best understood by the modality the ultrasound machine is running, by the depth of the question being asked, and by the setting in which the study is performed, because each axis changes what you can conclude from the report. [1] [2]
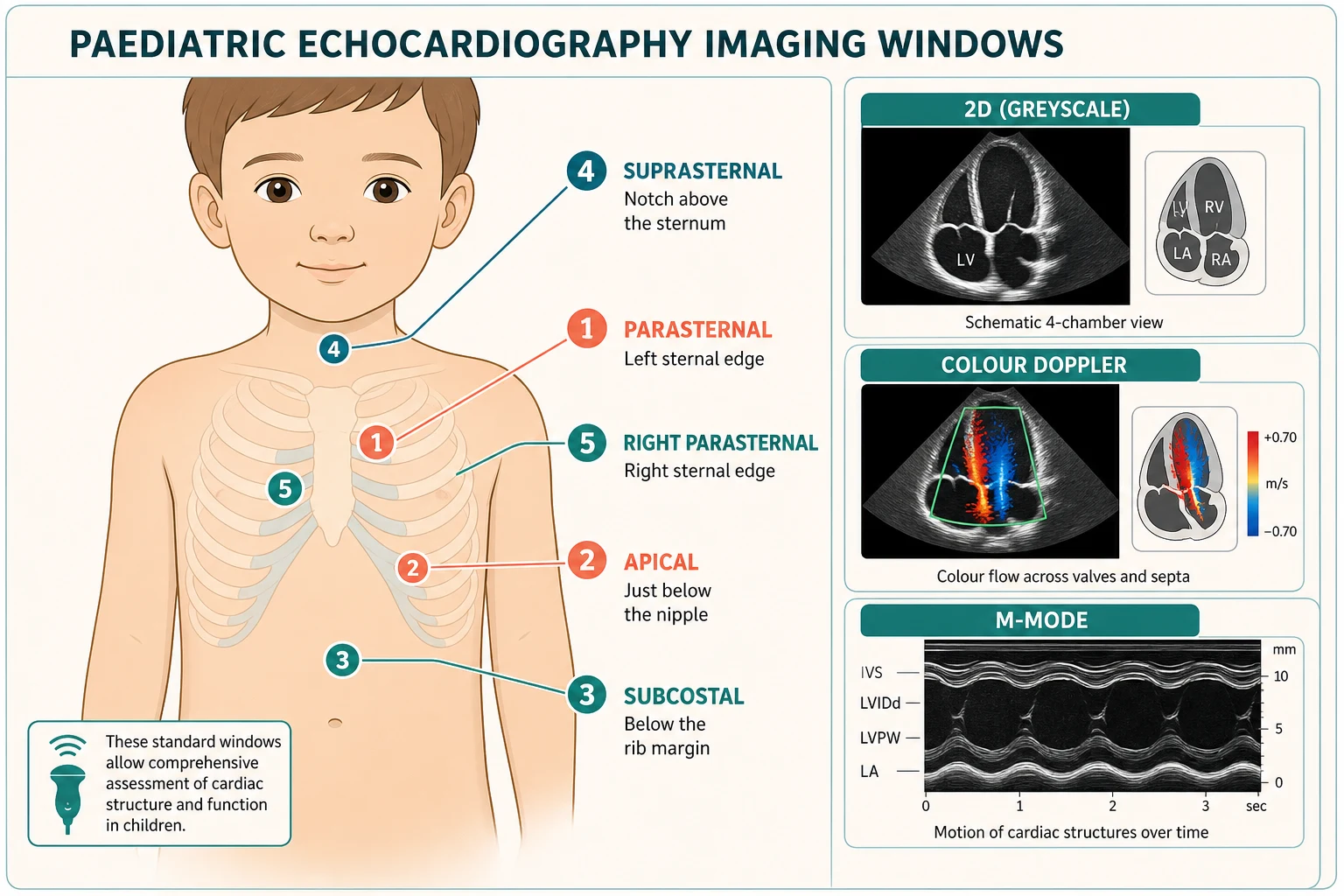
By modality, two-dimensional (2D) imaging is the real-time greyscale cross-section that defines cardiac anatomy — the four chambers, the valves, the septa, and the great vessel connections. M-mode derives a single line of ultrasound data displayed against time, and it gives the precise chamber dimensions and wall thicknesses from which fractional shortening is calculated. Colour Doppler overlays a colour map of blood-flow direction and turbulence on the 2D image — conventionally red toward the probe and blue away — and is the fastest screen for a shunt, a regurgitant jet, or a stenotic flow acceleration. Spectral Doppler displays flow velocity against time: pulsed-wave Doppler measures velocity at a precise location but aliases at high speeds, while continuous-wave Doppler measures the highest velocity along the beam and is the tool for the peak gradient across a stenotic valve. [1] [12]
By depth of question, a comprehensive laboratory transthoracic echocardiogram is the full, protocol-driven study performed and reported by a cardiographer and a cardiologist, and it is the investigation that answers a structural or functional question definitively. A focused cardiac ultrasound or point-of-care cardiac study is a limited, goal-directed examination performed at the bedside by the treating clinician to answer a specific binary question — is there a pericardial effusion, is the left ventricle grossly hyperkinetic or globally impaired, is the inferior vena cava collapsed or plethoric — and it does not replace the comprehensive study. The disciplined general paediatrician knows which depth of question they are asking and orders accordingly. [2] [10]
By setting and route, a transthoracic echocardiogram is performed through the chest wall and is the standard paediatric study; a transoesophageal echocardiogram uses a probe passed into the oesophagus under sedation or anaesthesia for superior posterior-structure imaging during surgery or when the chest wall window is poor; a fetal echocardiogram images the fetal heart through the maternal abdomen; and a stress echocardiogram images the heart before and after exercise or pharmacological stress to unmask gradients or ischaemia. [1]
The numbers that anchor your viva
Epidemiology & Risk Factors
The paediatric echocardiogram is one of the commonest cardiac investigations a general paediatrician requests, and the volume makes the question of appropriate use a real patient-safety and resource issue. Congenital heart disease occurs in roughly 8 per 1000 live births, and a meaningful fraction of these lesions are duct-dependent or critical and declare themselves in the neonatal period, which is why the echo is pivotal in the collapsed neonate. The rest are detected through a murmur, cyanosis, heart failure, or an abnormal antenatal scan. [1] [5]
The likelihood that an echo is abnormal is concentrated in a small number of clinical contexts. A murmur is more likely to reflect structural disease when it is holosystolic or diastolic, grade 3 or louder, harsh, associated with a thrill, or accompanied by a click, and an echo in these children is high-yield. A murmur that is soft, short, vibratory, musical, systolic, and sitting at the left sternal edge in an asymptomatic, well-growing child is most likely innocent, and the discipline is to avoid reflexively echoing every innocent murmur, because the yield is low and the downstream anxiety and cost are real. [9]
The most important patient-safety risks at the request end are the under-requested echo in the duct-dependent neonate whose collapse is misattributed to sepsis, and the over-requested echo for an innocent murmur that a focused clinical assessment would have settled. At the interpretation end, the parallel risks are reading a normal Z-score-adjusted dimension as dilated because the absolute number looks large, and dismissing a real finding because the report is dense and the critical line is buried. The fellowship candidate must show they can do both ends well. [5] [6]
Pathophysiology
The teaching model runs from the physics of the ultrasound pulse to the haemodynamics that Doppler turns into numbers, and it rests on two facts — the echo signal is generated by the reflection of sound at tissue boundaries, and blood-flow velocity encodes pressure. [1] [12]
The transducer's piezoelectric crystal converts electrical energy into a brief pulse of high-frequency sound that travels into the chest and reflects wherever it meets a change in acoustic impedance — the boundary between blood and muscle, muscle and valve, or tissue and air. The time taken for each echo to return gives its depth, and the amplitude gives its brightness, which is the basis of the 2D greyscale image. The practical trade-off is that higher-frequency probes resolve finer detail but penetrate less deeply, which is why the paediatric echocardiographer chooses a higher-frequency probe for the infant's thin chest and a lower-frequency probe for the adolescent. [12]
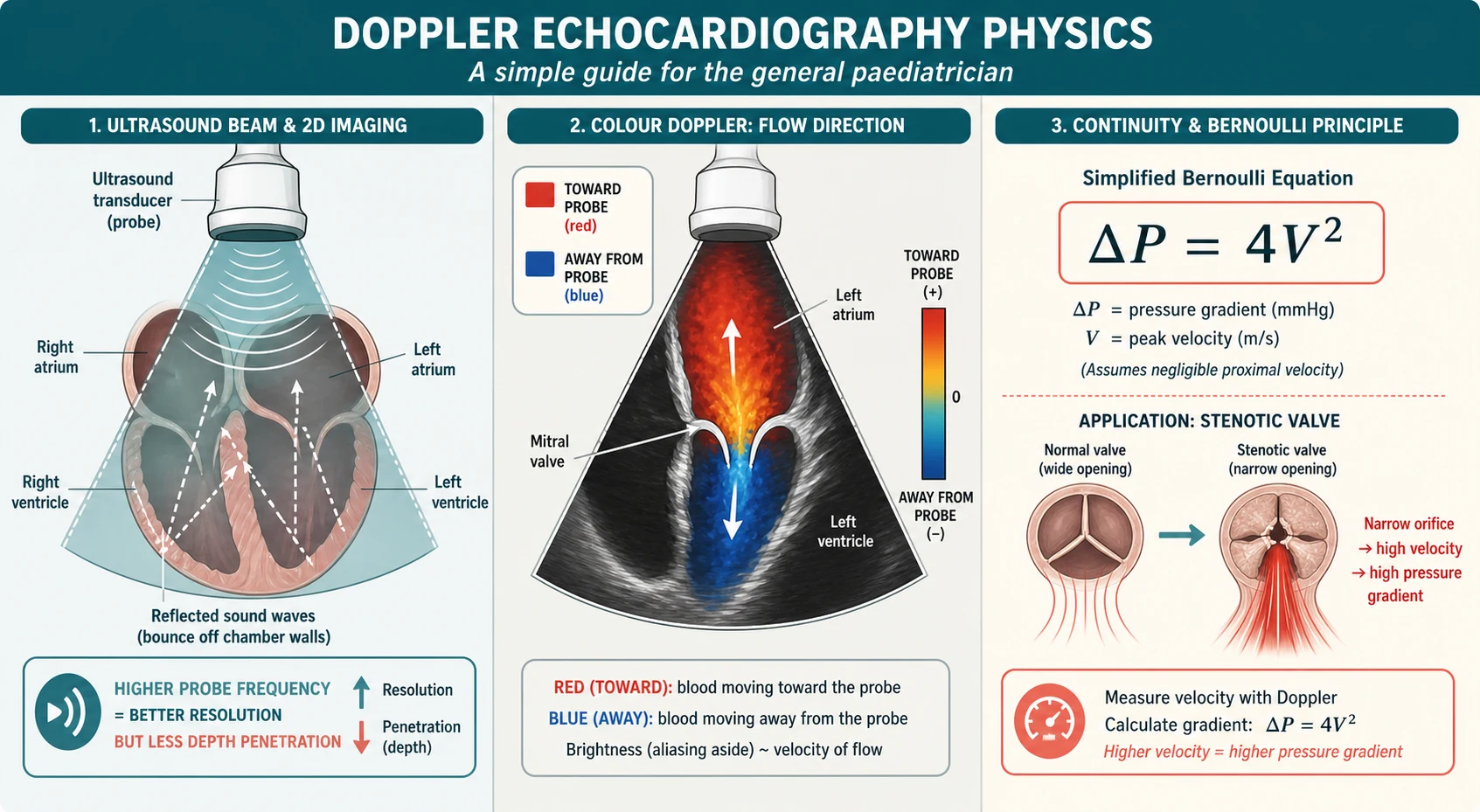
The Doppler principle is that sound reflected from a moving target returns at a shifted frequency, and the shift encodes the target's velocity along the beam. Blood moving toward the probe shifts the frequency up and is coloured red by convention; blood moving away shifts it down and is coloured blue. Colour Doppler gives the qualitative map, and spectral Doppler gives the quantitative velocity trace. Pulsed-wave Doppler samples velocity at one chosen depth but cannot measure velocities above its Nyquist limit without aliasing, so it suits low-velocity flow such as ventricular inflow or outflow tract velocities. Continuous-wave Doppler transmits and receives continuously and measures the highest velocity anywhere along the beam without aliasing, which makes it the tool for the high-velocity jet of a stenotic valve or a ventricular septal defect. [1]
The single most testable haemodynamic fact is the modified Bernoulli equation: the pressure gradient across a narrowing, in millimetres of mercury, is approximately four times the square of the peak velocity in metres per second (gradient equals four times velocity squared). A continuous-wave jet at 4 metres per second across a stenotic aortic valve implies a peak gradient of about 64 millimetres of mercury; a tricuspid regurgitation jet at 3 metres per second implies a right-ventricle-to-right-atrium gradient of about 36 millimetres of mercury, which estimates the pulmonary artery pressure when added to the estimated right atrial pressure. This is how Doppler turns a velocity into a pressure, and it is the basis of every valve-gradient and pulmonary-pressure estimate on the report. [12] [11]
Clinical Presentation
The clinical scenarios that prompt a paediatric echocardiogram are few and well defined, and the first task is to decide which one the child is in, because the urgency of the study and the threshold for cardiology referral differ. [9] [6]
The commonest scenario is the cardiac murmur. A pathological murmur — holosystolic or diastolic, grade 3 or louder, harsh, associated with a thrill or a click, or heard in an infant under one year — warrants an echo. An innocent murmur in an asymptomatic, well-growing child does not, provided the cardiovascular examination is otherwise normal. The second is the cyanotic or collapsed neonate, in whom the echo excludes or confirms a duct-dependent congenital heart lesion and is urgent rather than elective. The third is heart failure — the tachypnoeic, sweating, poorly feeding infant with hepatomegaly, or the older child with exercise intolerance — in whom the echo distinguishes a structural shunt lesion from a cardiomyopathy or myocarditis. [1] [9]
The fourth scenario is syncope with red flags — exertional, with a family history of sudden death, or accompanied by chest pain or palpitations — in whom the echo screens for the structural substrate of arrhythmia such as hypertrophic cardiomyopathy. The fifth is the follow-up of known congenital heart disease, where the serial echo tracks residual shunts, gradients, ventricular size and function, and the complications of surgical repair. The sixth is the specific-disease echo: the coronary assessment in Kawasaki disease, the ventricular function in a child on a cardiotoxic drug, the pericardium in a child with a systemic inflammatory disease, or the thrombus screen in a central line. [6] [12]
| Scenario | Urgency | What the echo answers |
|---|---|---|
| Pathological murmur | Elective to urgent | Structural lesion, shunt, valve disease; or confirms innocent |
| Cyanotic or collapsed neonate | Stat; before transfer | Duct-dependent lesion; great-vessel connections; pulmonary and systemic flow |
| Heart failure in infancy | Urgent | Shunt lesion versus cardiomyopathy versus myocarditis; ventricular function |
| Syncope with red flags | Urgent | Hypertrophic cardiomyopathy, coronary anomaly, structural substrate of arrhythmia |
| Known congenital heart disease | Serial, scheduled | Residual shunt, gradient, ventricular size and function, post-surgical complications |
| Kawasaki disease | Scheduled at diagnosis and serial | Coronary artery Z-scores; aneurysm; ventricular function |
The trap is the child whose clinical picture and the echo report are read in isolation from each other — a report that lists a trivial finding as abnormal generates anxiety and a referral, while a child in cardiogenic shock whose borderline fractional shortening is dismissed as acceptable misses a deteriorating cardiomyopathy. The discipline is to integrate the report with the bedside picture before acting. [4] [5]
Differential Diagnosis
The differential at the bedside is not "what is causing the murmur" — it is whether the echo confirms a lesion that needs referral, settles the question as innocent, or leaves a residual question the cardiologist must close. Frame the read around three outcomes and the right action follows. [9] [6]
Normal for the child
default
- Chamber dimensions, wall thickness, and Z-scores all within the normal range for body size
- No shunt on colour Doppler; trivial physiological regurgitation accepted
- Normal ventricular systolic function; fractional shortening within range
- Reassure the family; no cardiology referral needed
Abnormal but stable
- A small restrictive ventricular septal defect with normal chamber sizes and no pulmonary hypertension
- A bicuspid aortic valve with a low gradient and normal aortic root dimensions
- Mild-moderate valve regurgitation with preserved ventricular function
- Routine cardiology referral for surveillance; not an emergency
Abnormal, urgent referral
- Duct-dependent lesion in a neonate; start prostaglandin and transfer
- Severe ventricular dysfunction or a dilated cardiomyopathy phenotype
- Pericardial effusion with tamponade physiology; elevated pulmonary pressures
- Refer to paediatric cardiology the same day; resuscitate per APLS if compromised
Poor window or equivocal
- Suboptimal acoustic windows in a large adolescent or a child with lung disease
- A finding the general paediatrician cannot confidently interpret
- A technically limited study that needs repeating in the laboratory
- Do not over-call; request a repeat or a cardiology-reported study
A second layer of differential is the named findings an examiner will reward for recognising on a report. A dominant right ventricle with a large subaortic ventricular septal defect and an overriding aorta is the echo signature of tetralogy of Fallot. A dilated, globally hypokinetic left ventricle with a low fractional shortening is dilated cardiomyopathy or myocarditis until distinguished by history and biomarkers. A thick-walled, hyperkinetic left ventricle with systolic anterior motion of the mitral valve is hypertrophic cardiomyopathy. A swirling echo-free space around the heart with chamber collapse is a pericardial effusion with tamponade physiology. [6] [12]
The tricuspid regurgitation jet velocity deserves a specific question because it is the bedside estimate of pulmonary artery pressure. A TR jet velocity above 2.8 to 3.0 metres per second raises pulmonary hypertension, and the finding is strengthened by flattening of the interventricular septum in systole and a short pulmonary acceleration time. The general paediatrician does not manage pulmonary hypertension, but they must recognise the echo signature and refer. [11]
Clinical & Bedside Assessment
Assessment before requesting an echocardiogram is short and focused: it asks what clinical question the study has to answer, what the child's body size is so the Z-scores will be interpretable, and whether the question is one a focused bedside study can answer or one that needs the comprehensive laboratory protocol. [9] [2]
Begin with a focused clinical history. Ask about the symptom that prompted the request, its onset and progression, feeding and growth in the infant, exercise tolerance in the older child, and any colour change or syncope. Ask specifically about a family history of congenital heart disease, sudden death before the age of 40, or cardiomyopathy, and about maternal conditions that raise congenital heart disease risk such as diabetes. List any cardiotoxic or QT-prolonging medication the child takes. Examine the cardiovascular system in full: heart rate and rhythm, blood pressure in the right arm (and a four-limb comparison if coarctation is suspected), the character and radiation of any murmur, the presence of a thrill or a click, the femoral pulses, the oxygen saturation, and the liver edge for hepatomegaly. [9] [1]
Assess the child's body surface area and weight before requesting the study, because the Z-scores on the report are calculated against body size and a weight and height must accompany the request. Decide whether the question is comprehensive or focused: a structural question, a first diagnosis, or a serial follow-up needs the full laboratory study, while a binary bedside question in an unstable child — is there a pericardial effusion, is the left ventricle grossly impaired — is the territory of the focused point-of-care cardiac ultrasound, performed by a trained clinician and never a substitute for the definitive study. [2] [10]
The pre-echo request checklist
What is the clinical question the echo has to answer (structural diagnosis, function, shunt, valve gradient, effusion, follow-up)?
Record the child's weight and height so the Z-scores on the report will be interpretable
Examine the cardiovascular system and document the murmur characteristics, femoral pulses, and saturations
Decide comprehensive laboratory study versus focused point-of-care study, based on the depth of the question
Communicate the clinical context and the specific question on the request so the cardiographer and cardiologist target the study
Plan the timing: stat for the duct-dependent neonate, urgent for heart failure, scheduled for follow-up
Investigations
The echocardiogram is the investigation; the question is what each modality and measurement tells you and how to read the report systematically. The comprehensive paediatric transthoracic study is acquired through five standard acoustic windows — parasternal, apical, subcostal, suprasternal, and right parasternal — and it sequences the 2D, M-mode, colour, and spectral Doppler modalities through each window to build a complete anatomical and haemodynamic picture. [1]
| Modality | What it measures | High-yield question it answers |
|---|---|---|
| 2D imaging | Real-time greyscale cross-sections of anatomy | Are the chambers, septa, valves, and great-vessel connections normal? |
| M-mode | A single ultrasound line against time | Chamber dimensions, wall thickness, fractional shortening (LV function) |
| Colour Doppler | Direction and turbulence of flow overlaid on 2D | Is there a shunt, a regurgitant jet, or a stenotic flow acceleration? |
| Pulsed-wave Doppler | Velocity at a precise location | Low-velocity flow: ventricular inflow, outflow tract velocities |
| Continuous-wave Doppler | Highest velocity along the beam | Peak gradient across a stenotic valve, TR jet velocity for PA pressure |
| Speckle-tracking strain | Myocardial deformation | Subtle systolic dysfunction before EF falls; reference by Z-score |
The standard imaging windows each show a different part of the heart. The parasternal long-axis view shows the left ventricle, the left atrium, the mitral and aortic valves, and the ascending aorta. The parasternal short-axis view, swept from base to apex, shows the aortic valve en face, the pulmonary valve and right ventricular outflow tract, and the left ventricle in cross-section. The apical four-chamber view shows all four chambers, the atrioventricular valves, and the pulmonary venous drainage. The subcostal view is crucial in the neonate and infant for the atrial septum, the inferior vena cava, and the abdominal situs. The suprasternal view shows the aortic arch and its branches, and is the window that excludes a coarctation. [1] [12]
The ventricular function measurements anchor every report. Fractional shortening is the M-mode percentage change in left ventricular dimension between diastole and systole, with a normal range of approximately 28 to 44 percent; a value below this range signals impaired systolic function. Ejection fraction, by the Simpson biplane method, sits normally at about 55 to 70 percent. Modern reports increasingly add speckle-tracking longitudinal strain, a more sensitive marker of systolic function that falls before the ejection fraction does, and these strain values are normalised to body size as Z-scores derived from large healthy-child cohorts. [1] [8]
The valve and flow measurements turn Doppler velocities into gradients. A peak velocity across a valve, measured by continuous-wave Doppler, converts to a gradient by the modified Bernoulli equation (gradient equals four times velocity squared). A peak aortic valve velocity of 4 metres per second implies a peak gradient of about 64 millimetres of mercury, which defines severe aortic stenosis in a child. The tricuspid regurgitation jet velocity estimates the pulmonary artery pressure. A shunt is identified by colour Doppler and its direction and velocity quantified by spectral Doppler, which distinguishes a small restrictive ventricular septal defect (high-velocity, left-to-right) from a large unrestrictive one (low-velocity, bidirectional, with pulmonary hypertension). [11] [12]
Management — Resuscitation
When the echocardiogram accompanies a child who is haemodynamically compromised by the lesion shown on it, the order of priorities is airway, breathing, circulation, and the treatment of the lesion, not the elegant classification of the report. The ordered bundle is oxygen if hypoxic, intravenous access, and the protocol for the lesion, and the echo is interpreted alongside, not instead of, the resuscitation. [9] [1]
The single most important resuscitation scenario is the duct-dependent neonate. Any lesion whose systemic or pulmonary circulation depends on a patent ductus arteriosus — hypoplastic left heart syndrome, critical aortic stenosis, coarctation of the aorta, interrupted aortic arch, pulmonary atresia, severe tetralogy of Fallot, or tricuspid atresia — collapses as the duct closes in the first days of life, presenting with shock, acidosis, and a differential cyanosis or profound desaturation. The echo confirms the lesion, but the treatment does not wait for the cardiologist: the general paediatrician starts intravenous prostaglandin E1 (alprostadil) to reopen and keep the duct patent while arranging transfer to a cardiac centre. [9] [1]
Prostaglandin E1 (alprostadil) for duct-dependent congenital heart disease, ANZ / RCH
For the pericardial effusion with tamponade, the echo shows the echo-free fluid around the heart with diastolic collapse of the right atrium or right ventricle, a plethoric, non-collapsing inferior vena cava, and respiratory variation of the ventricular inflow. The general paediatrician who identifies tamponade physiology on a focused study must escalate to urgent pericardiocentesis or cardiology-led drainage and fluid resuscitation, because the decompensation can be sudden and the echo findings precede the arrest. [2] [1]
For the child in cardiogenic shock from severe ventricular dysfunction, the echo shows a dilated, globally hypokinetic left ventricle with a low fractional shortening, and the resuscitation is oxygen, judicious fluids, and the early involvement of paediatric intensive care for inotropic support, because the child with myocarditis or decompensated cardiomyopathy can deteriorate rapidly. The echo distinguishes cardiogenic shock from distributive or hypovolaemic shock and sets the inotropic and fluid strategy. [1] [6]
Management — Definitive & Stepwise
Once the urgent lesion has been addressed, the systematic reading of the paediatric echo report is an ordered sequence that should run the same way every time: structure, function, valves, flow, pericardium, and special findings. [1] [6]
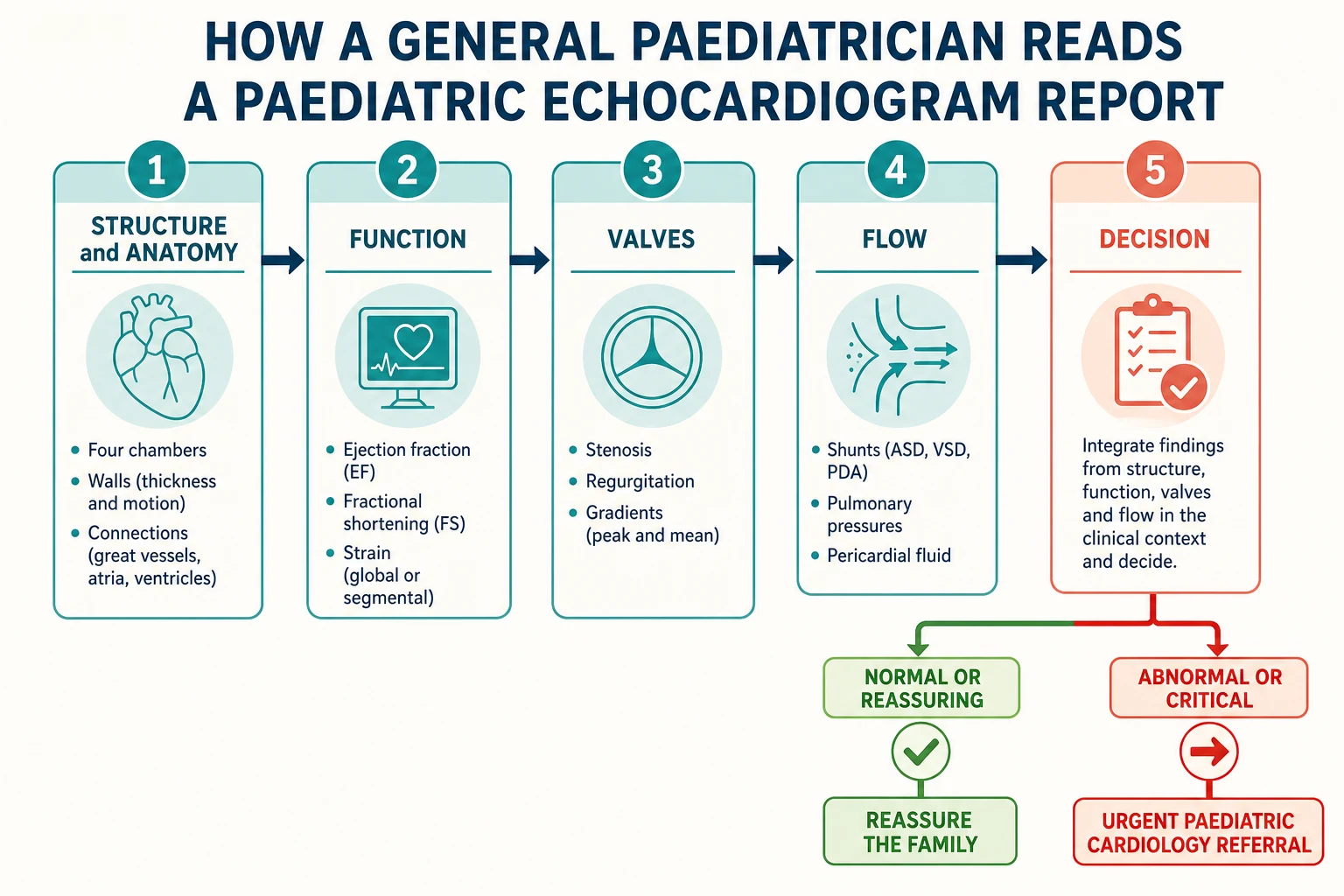
Structure. Begin with the anatomy. Are the four chambers normally related and sized? Is the atrioventricular and ventriculoarterial concordance normal — the right atrium connected to the right ventricle to the pulmonary artery, the left atrium to the left ventricle to the aorta? Are the septa intact, the valves normally formed, the great vessels in their normal relationship? Any abnormality of connections — transposition, atrioventricular septal defect, double-outlet right ventricle — is cardiology territory. [1]
Function. Read the fractional shortening or ejection fraction against the normal range, and check whether the dysfunction is global or regional. A globally dilated, hypokinetic ventricle is dilated cardiomyopathy or myocarditis; a thick-walled, hyperkinetic ventricle with systolic anterior motion is hypertrophic cardiomyopathy; regional wall-motion abnormality raises ischaemia or myocarditis in a segmental pattern. The strain values flag subtle dysfunction before the ejection fraction falls. [1] [8]
Valves. For each valve, ask whether it is structurally normal, whether there is stenosis or regurgitation, and what the gradient is. A bicuspid aortic valve with a low gradient needs surveillance for the aortic root; a stenotic valve with a high gradient needs cardiology referral; significant regurgitation with ventricular dilation needs assessment for the timing of repair. The gradient comes from the peak velocity by the modified Bernoulli equation, and the general paediatrician must know that a peak velocity of 4 metres per second implies a gradient of about 64 millimetres of mercury. [12]
SV-FLOW
Flow. Look for the shunt and the pulmonary pressure estimate. A ventricular septal defect is identified on colour Doppler and its haemodynamic significance judged by the left-heart dilation and the pulmonary artery pressure, not by the size of the colour jet alone. A tricuspid regurgitation jet velocity above 2.8 to 3.0 metres per second, a flattened interventricular septum, and a short pulmonary acceleration time raise pulmonary hypertension and change the child's anaesthetic risk and referral pathway. [11] [6]
Pericardium and special. Check for a pericardial effusion and its haemodynamic significance — chamber collapse means tamponade. In Kawasaki disease, look for the coronary artery Z-scores, where a Z-score of 2.5 or above defines an aneurysm and a giant aneurysm changes the anticoagulation and surveillance pathway. In a child on a cardiotoxic drug, look for the fall in fractional shortening or strain that triggers a dose change. [7] [12]
Specific Subtypes & Scenarios
The approach to the paediatric echo changes with the child and the clinical question, and the fellowship candidate must adjust the read and the referral threshold to the scenario in front of them. [1] [6]
In the neonate, the echo is pivotal in the collapsed or cyanotic infant, and the first question is whether the lesion is duct-dependent. The subcostal and suprasternal windows are essential for the atrial septum, the abdominal situs, and the aortic arch, and the echo confirms or excludes the coarctation, the transposition, and the obstructed lesions that need prostaglandin. A targeted neonatal echocardiogram or cardiac point-of-care study in the neonatal intensive care unit answers focused questions about ductal patency, pulmonary and systemic blood flow, and ventricular function, but it does not replace the comprehensive cardiology study. [3] [9]
In the infant with a murmur and possible heart failure, the echo distinguishes the structural shunt lesion (a ventricular septal defect, an atrioventricular septal defect, a patent ductus arteriosus) from the cardiomyopathy or myocarditis. The size of the shunt is judged by the left-heart dilation and the pulmonary pressure, and a large unrestrictive defect with pulmonary hypertension needs timely cardiology referral and often surgical or catheter closure. [1] [9]
In the school-age child with a pathological murmur or chest pain, the echo looks for the structural lesions that declare in this age band — a bicuspid aortic valve, a subaortic membrane, a small restrictive ventricular septal defect — and, in the child with exertional chest pain or syncope, for the structural substrate of arrhythmia such as hypertrophic cardiomyopathy or an anomalous coronary origin. [6] [12]
In the child with Kawasaki disease, the echo measures the coronary artery dimensions as Z-scores at diagnosis and at serial intervals, because the coronary aneurysm is the feared complication and its detection changes the management from aspirin alone to anti-inflammatory escalation and anticoagulation. A coronary Z-score of 2.5 or above defines dilation or an aneurysm, and a giant aneurysm (Z-score of 10 or above, or an absolute dimension of 8 millimetres or more) carries a high risk of thrombosis and needs long-term anticoagulation and cardiology surveillance. [7] [9]
In the child with known congenital heart disease, the serial echo tracks the residual shunt, the gradient across a repaired valve or outflow tract, the ventricular size and function, and the complications of surgery such as a residual ventricular septal defect, right ventricular outflow obstruction, or branch pulmonary artery stenosis. The appropriate-use criteria guide the frequency of surveillance imaging and the choice between echo, cardiac MRI, and CT. [6]
In the technology-dependent or critically ill child, the focused point-of-care cardiac ultrasound answers the bedside question — is the ventricle hyperkinetic and underfilled (hypovolaemia), globally impaired (cardiomyopathy, sepsis), or is there a new effusion — and guides the fluid and inotropic strategy in real time. [2] [10]
Complications & Pitfalls
The "complications" of an echocardiogram are not procedural in the usual sense, because the transthoracic study is non-invasive and carries no radiation. The harms are the consequences of a misrequested or misread study — the false positive that generates unnecessary referral and family anxiety, and the false negative that misses a child at risk. [4] [5]
The common pitfall is reading a chamber dimension in absolute millimetres without the Z-score. A left ventricular end-diastolic dimension of 35 millimetres is normal in a ten-year-old but markedly dilated in an infant, and reading the raw number as reassuring misses a large shunt. The discipline is to read the Z-score column, where a value beyond positive or negative 2 is abnormal for that child's body size. [7] [8]
The serious pitfall is missing a duct-dependent lesion in the collapsed neonate. A neonate who presents with shock, acidosis, and desaturation in the first days of life has a duct-dependent congenital heart lesion until proven otherwise, and the echo confirms it — but the first dose of prostaglandin must not wait for the cardiologist if the clinical picture fits. The corollary is treating a collapsed neonate as septic without an echo, because duct-dependent lesions and neonatal sepsis share the presentation and the echo is the discriminator. [9] [1]
[1] [9]A frequently tested misconception is that the colour Doppler jet size equals the shunt size or the regurgitation severity. It does not. A small, high-velocity, turbulent colour jet across a tiny restrictive ventricular septal defect can look dramatic on colour but is haemodynamically trivial, while a large unrestrictive defect produces a low-velocity, less turbulent jet that is the dangerous one. The severity is judged by the downstream chamber dilation and the pulmonary pressure, not by the colour map alone. [11] [12]
Prognosis & Disposition
The prognosis after a paediatric echocardiogram is dictated almost entirely by the underlying lesion, not by the study itself. The disposition is therefore a function of what the report shows, integrated with the bedside picture. [9] [6]
For a normal echo in an asymptomatic child with a murmur that prompted the request, the disposition is reassurance and return to normal activity; no cardiology follow-up is needed. The discipline is to have interpreted the report against the Z-score-adjusted norms, so that a normal variant is not referred and the family is given a clear explanation. [9]
For a stable abnormal echo — a small restrictive ventricular septal defect with normal chamber sizes, a bicuspid aortic valve with a low gradient, or mild valve regurgitation with preserved function — the disposition is routine paediatric cardiology referral and serial surveillance at intervals guided by the appropriate-use criteria. These children are followed for the evolution of the gradient, the chamber size, and the ventricular function. [6]
For the child with a critical or high-risk echo finding, the disposition is urgent paediatric cardiology referral the same day, with resuscitation per the lesion. These findings include a duct-dependent lesion in a neonate (start prostaglandin and transfer), severe ventricular dysfunction or a dilated cardiomyopathy phenotype, a pericardial effusion with tamponade, and pulmonary hypertension. The long-term prognosis depends on the lesion and its treatment, and ranges from excellent for a small restrictive ventricular septal defect that closes spontaneously to guarded for a decompensated cardiomyopathy. [1] [6]
For the child with a technically limited or equivocal study, the disposition is a repeat comprehensive study in the laboratory or a cardiology-reported study, because a poor acoustic window in a large adolescent or a child with lung disease can mask a real finding, and the general paediatrician must not over-call or under-call on a study of poor quality. [4] [5]
Special Populations
The approach to the paediatric echo is adjusted for the child in front of you, and the fellowship candidate must show they can match the request and the interpretation to the population. [1] [6]
In the neonate, the echo is pivotal in the collapsed or cyanotic infant, and the targeted neonatal echocardiogram answers focused questions about ductal patency, shunt direction, and ventricular function at the bedside, while the comprehensive cardiology study defines the anatomy definitively. The neonate with a duct-dependent lesion is the one in whom the general paediatrician must start prostaglandin before the transfer. [3] [9]
In the child with known congenital heart disease, the serial echo is the backbone of follow-up, and the appropriate-use criteria guide the frequency and the modality, balancing the value of surveillance against the burden of repeated imaging and the occasional need for cardiac MRI or CT for the structures echo sees less well. [6]
In the child on a cardiotoxic drug — anthracycline chemotherapy, or a drug that raises the pulmonary pressure — the baseline and serial echo monitors the ventricular function and the strain, and a fall in the fractional shortening or strain triggers a dose review with the oncology or respiratory team. [8]
In the technology-dependent and critically ill child, the focused point-of-care cardiac ultrasound answers the bedside haemodynamic question in real time and guides the fluid, inotropic, and ventilation strategy, integrated with the comprehensive laboratory study for the definitive anatomy. [2] [10]
In the Indigenous, remote, or under-resourced setting, access to a paediatric echocardiography laboratory and to a reporting cardiologist may be limited, and the equity intervention is a focused point-of-care study to answer the urgent question, a defensible list of red flags to trigger retrieval, and telehealth links to a cardiac centre for report review and management planning. [10]
In the neurodivergent or anxious child, the study is planned with extra time, a communication strategy appropriate to the child, and a distraction or sedation plan that the child and family can support, because a calm child gives a technically adequate study and a distressed child gives an artefact-ridden one. [4]
Evidence, Guidelines & Regional Differences
The evidence base for the paediatric echocardiogram has matured in four areas: the technical standard for the comprehensive study, the normalisation of dimensions by Z-score, the appropriate-use criteria, and the role of the focused point-of-care study. The candidate should know each one and the regional deltas that follow from them. [1] [6]
The technical standard for the comprehensive paediatric transthoracic echocardiogram is set by the American Society of Echocardiography guidelines, which define the imaging windows, the modalities, the measurements, and the quality benchmarks that every laboratory study should meet. Paediatric echocardiography quality improvement programs track the adherence to these standards and the variation in practice across laboratories, and the findings drive the accreditation of laboratories and the training of cardiographers. [1] [4]
The Z-score normalisation of paediatric dimensions is anchored on large cohorts of healthy children, with reference equations for the left and right ventricular strain, the chamber dimensions, and the coronary arteries. The modern reporting convention is to give the Z-score alongside the raw measurement, so that the general paediatrician can judge whether a dimension is abnormal for the child's body size, and the Kawasaki-disease and congenital-heart-disease literature now reports coronary dimensions primarily as Z-scores. [7] [8]
Pediatric Normal Values and Z Score Equations for Ventricular Strain (JASE 2023)
PMID 36414123
Population: A large cohort of healthy children across the paediatric age range
Comparator: Body-surface-area-normalised Z-score equations for left and right ventricular strain
Key finding
The study provided normative Z-score equations for left and right ventricular longitudinal strain in healthy children, enabling the detection of subtle systolic dysfunction before the ejection fraction falls and the standardisation of strain reporting across paediatric laboratories.
The appropriate-use criteria for multimodality imaging in the follow-up of congenital heart disease guide the frequency of surveillance echo and the choice between echo, cardiac MRI, and CT, and they are the reference the general paediatrician cites when justifying a serial study or declining one. The criteria balance the value of surveillance against the burden of repeated imaging and the rare but real harms of sedation and radiation when alternative modalities are chosen. [6]
The focused cardiac ultrasound is defined by the international evidence-based recommendations and the neonatal point-of-care guidelines, which set the scope of the bedside study — the binary questions it may answer — and the boundary beyond which the comprehensive laboratory study is required. The training and the scope of the general paediatrician's point-of-care practice is an active area of curricular development. [2] [3]
Several points remain weak or contested. The optimal strain-measurement vendor and the Z-score equation for the coronary arteries vary across centres, and the standardisation of paediatric strain reporting is ongoing. The threshold for the anticoagulation of a moderate Kawasaki aneurysm is debated. The role of the general paediatrician's point-of-care cardiac ultrasound is expanding but its scope and training are not yet uniform. Each is a defensible topic for the viva. [7] [12]
Exam Pearls
The fellowship examiner expects a candidate who can request the right echo, read the report systematically against the Z-score-adjusted norms, and recognise the findings that demand urgent referral. [1] [9]
The single most testable fact is that every paediatric chamber dimension must be read as a Z-score, because a normal-looking absolute number can be markedly abnormal for the child's body size. A coronary of 3 millimetres is normal in a teenager but an aneurysm in an infant; a left ventricular dimension that looks acceptable in millimetres may sit at a Z-score of 4 and be grossly dilated. [7] [8]
The exam rewards naming the modified Bernoulli equation and applying it. The peak pressure gradient across a narrowing, in millimetres of mercury, is approximately four times the square of the peak velocity in metres per second. A peak aortic velocity of 4 metres per second implies a peak gradient of about 64 millimetres of mercury, which defines severe aortic stenosis. A tricuspid regurgitation jet velocity of 3 metres per second implies a right-ventricle-to-atrium gradient of about 36 millimetres of mercury and raises pulmonary hypertension. [12] [11]
The resuscitation facts that must be quoted exactly: a duct-dependent lesion in a neonate is treated with intravenous prostaglandin E1 at 0.005 to 0.01 micrograms per kilogram per minute initially, titrated up to 0.05 to 0.1 micrograms per kilogram per minute, while arranging transfer to a cardiac centre; a pericardial effusion with chamber collapse on echo is tamponade and demands urgent drainage. The paediatric nuance — that the collapsed neonate has a duct-dependent lesion until the echo proves otherwise — is the mark that distinguishes the paediatric from the adult answer. [9] [1]
The exam rewards naming several classic distractors. Reading a chamber dimension in millimetres without the Z-score is a false negative. Equating the colour Doppler jet size with the shunt or regurgitation severity is a mistake. Treating a collapsed neonate as septic without an echo misses a duct-dependent lesion. Dismissing a pericardial effusion with chamber collapse as small is dangerous. Reflexively echoing an innocent murmur generates anxiety and cost without yield. [4] [11]
References
- [1]Lopez L, Colan SD, Stylianou MP, et al Guidelines for Performing a Comprehensive Pediatric Transthoracic Echocardiogram: Recommendations From the American Society of Echocardiography J Am Soc Echocardiogr, 2024.PMID 38309834
- [2]Via G, Hussain A, Wells M, et al International evidence-based recommendations for focused cardiac ultrasound J Am Soc Echocardiogr, 2014.PMID 24951446
- [3]McNamara PJ, Jain A, El-Khuffash A, et al Guidelines and Recommendations for Targeted Neonatal Echocardiography and Cardiac Point-of-Care Ultrasound in the Neonatal Intensive Care Unit: An Update from the American Society of Echocardiography J Am Soc Echocardiogr, 2024.PMID 38309835
- [4]Lopez L Pediatric echocardiography quality improvement J Am Soc Echocardiogr, 2012.PMID 23200424
- [5]Camarda JA, Altman CA, Race CR, Thompson WR Practice Variations in Pediatric Echocardiography Laboratories Pediatr Cardiol, 2019.PMID 30353314
- [6]Writing Group, Ryan JJ, Aroney N, Anderson AL, et al ACC/AHA/ASE/HRS/ISACHD/SCAI/SCCT/SCMR/SOPE 2020 Appropriate Use Criteria for Multimodality Imaging During the Follow-Up Care of Patients With Congenital Heart Disease J Am Soc Echocardiogr, 2020.PMID 33010859
- [7]Romanowicz J, Madueme PC, Khan J, Anderson AH, et al Pediatric Normal Values and Z Score Equations for Left and Right Ventricular Strain by Two-Dimensional Speckle-Tracking Echocardiography Derived from a Large Cohort of Healthy Children J Am Soc Echocardiogr, 2023.PMID 36414123
- [8]Dallaire F, Slorach C, Bradley T, et al Pediatric Reference Values and Z Score Equations for Left Ventricular Systolic Strain Measured by Two-Dimensional Speckle-Tracking Echocardiography J Am Soc Echocardiogr, 2016.PMID 27185223
- [9]Ford B, Schulz T, Sahn DJ Heart Murmurs in Children: Evaluation and Management Am Fam Physician, 2022.PMID 35289571
- [10]Miller AF, Pitock M, Adachi A, Leslie LK, et al Use of Cardiac Point-of-Care Ultrasound in the Pediatric Emergency Department Pediatr Emerg Care, 2022.PMID 33122503
- [11]Kamra K, Raghavendra R Role of echocardiography in the assessment of right ventricular function in the pediatric population Paediatr Anaesth, 2019.PMID 30934152
- [12]Grotenhuis HB, Li L, Vasanawala SS Recent evolutions in pediatric and congenital echocardiography Curr Opin Cardiol, 2015.PMID 25398044