Paeds · investigations-procedures-and-technology
Electrocardiogram acquisition and interpretation in children
Also known as Paediatric ECG · Children's ECG · 12-lead ECG in children · Neonatal ECG · Paediatric electrocardiography · ECG interpretation by age
Fellowship guide to electrocardiogram acquisition and interpretation in children. Covers the technical principles of 12-lead acquisition and electrode placement in an uncooperative infant, the age-specific normal intervals for heart rate, PR, QRS duration and axis, the right ventricular dominance of the newborn that resolves through childhood, the Bazett and alternative QTc formulae and the age-specific prolonged-QTc thresholds, the structured systematic interpretation sequence, and the high-yield abnormal patterns of long QT syndrome, pre-excitation, chamber hypertrophy, AV block and the juvenile T-wave pattern.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the six-week-old infant brought in with poor feeding and a fast heart rate, the eight-year-old who has fainted during a swimming lesson, or the teenager referred by the GP for an "abnormal ECG" after a routine check. In each case the question the ECG must answer is whether the electrical activity of the child's heart is normal for their age, and that question cannot be answered with adult ranges. That is the territory this page owns. [1] [2]
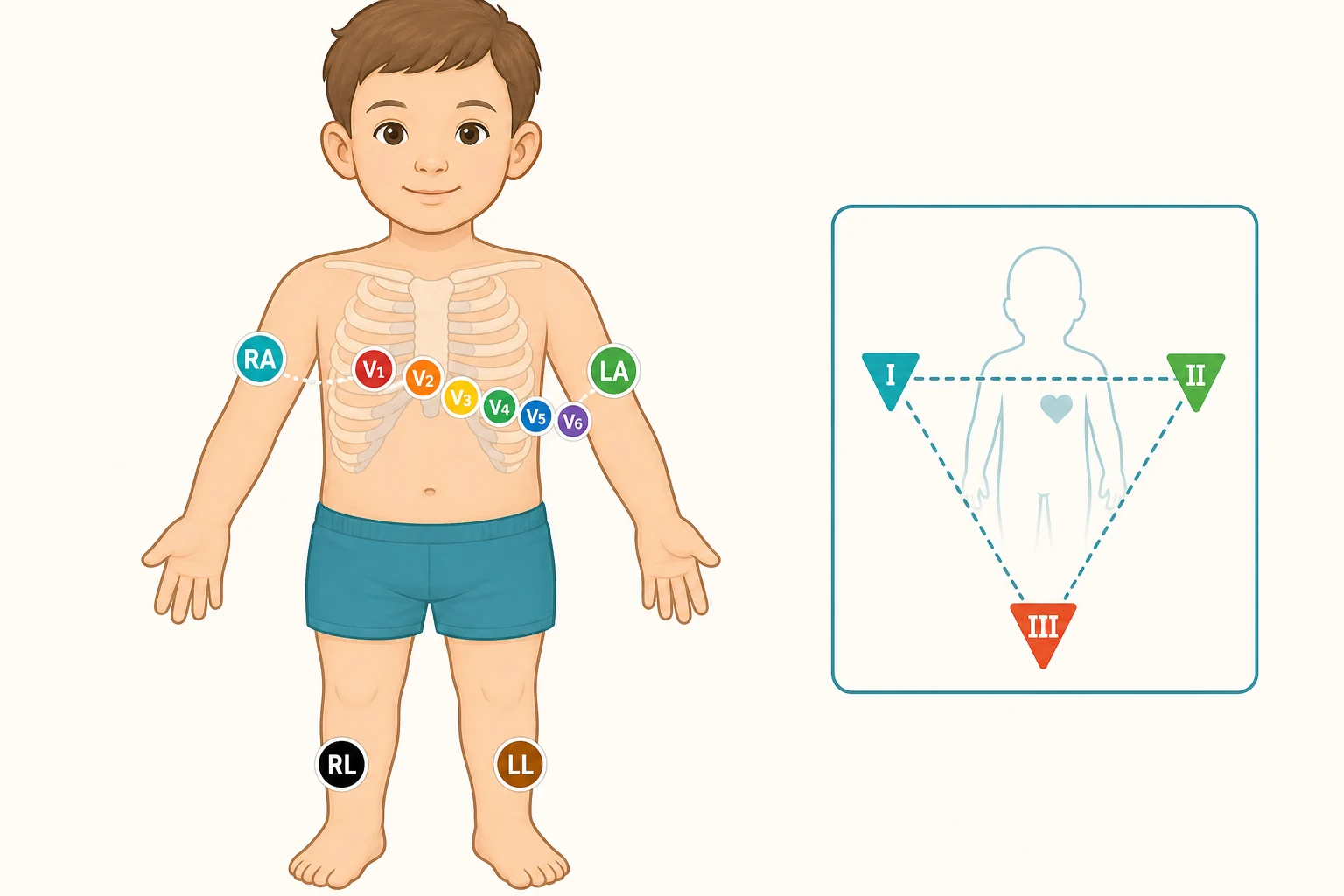
A 12-lead electrocardiogram (ECG) is the non-invasive recording, from ten surface electrodes (four limb and six precordial), of the summed electrical potentials generated by the myocardium over time and displayed as twelve different spatial views or leads. In a child the same physical principles apply as in the adult, but the normal ranges for heart rate, the PR and QRS intervals, the QRS axis, and the T-wave morphology all change with age, and the newborn ECG in particular is dominated by the right ventricle because the right heart has been working against the high pulmonary vascular resistance of fetal life. The discipline of the paediatric ECG is therefore to acquire a clean tracing and to interpret it against age-specific norms. [1] [9]
What distinguishes the paediatric ECG from the adult is a combination of a small, fast, often uncooperative patient and an electrical anatomy that is still maturing. The neonatal right ventricle is dominant, the intervals shorten with faster heart rates and lengthen as the heart grows, the T waves in V1 to V3 are normally inverted through childhood, and a number of channelopathies and congenital arrhythmias declare themselves on the surface ECG long before they declare themselves clinically. The fellowship skill being tested is acquiring a technically adequate tracing, interpreting it systematically against the correct age ranges, and recognising the patterns that demand urgent cardiology referral. [2] [6]
Classification
The paediatric ECG is best sorted by why it is being recorded, by how long the tracing is, and by the age band the child falls into, because each axis changes the leads you request, the gain and speed you use, and the normal ranges you compare against. [2] [4]
By purpose, a resting diagnostic 12-lead ECG is the standard investigation for chest pain, syncope, palpitations, a murmur, suspected electrolyte disturbance, or drug toxicity; a rhythm strip is a single lead (usually lead II) recorded continuously to characterise a paroxysmal arrhythmia; and an ambulatory Holter or event monitor records the rhythm over 24 hours or longer to capture an intermittent symptom. By urgency, a cardiac-arrest ECG is the rhythm strip during a pulseless arrest that decides between shockable and non-shockable rhythms; a stat ECG accompanies chest pain, haemodynamic compromise, or a tachyarrhythmia; an elective ECG screens or stratifies, such as before stimulant medication or in the family of a patient with a channelopathy. [2] [4]
By age band, the newborn (first month), infant (one month to one year), young child (one to eight years) and older child and adolescent (over eight years) each carry their own normal ranges for heart rate, intervals and axis. The neonate and young infant are the most error-prone, because right axis deviation, dominant R waves in V1, upright T waves in V1 in the first week of life, and QTc values that are higher than in older children are all expected in that age band. [9] [1]
The numbers that anchor your viva
Epidemiology & Risk Factors
The resting paediatric ECG is one of the commonest investigations performed in a children's emergency department and ward, and the volume of tracings makes interpretation accuracy a real patient-safety issue. Studies of paediatric ECG interpretation in the emergency setting have documented substantial inter-observer variability, with a meaningful fraction of tracings misinterpreted even by experienced clinicians — the implication for the fellowship candidate is that the discipline of a systematic, age-referenced read is what keeps a child safe, not pattern recognition. [3] [4]
The likelihood that a paediatric ECG is abnormal is concentrated in a small number of clinical contexts. Chest pain that is exertional, or that mimics angina, raises the probability of an anomalous coronary or myocardial ischaemia. Syncope that occurs on exertion, during or immediately after emotion, or in response to a sudden loud noise raises the probability of a channelopathy, particularly long QT syndrome. A resting tachycardia that is too fast for age, or that is paroxysmal and abrupt in onset and offset, raises the probability of supraventricular tachycardia, which in infancy is most often an accessory-pathway mechanism. A neonate with poor feeding, irritability, and a heart rate above 220 is the classic presentation of infant SVT. [4] [2]
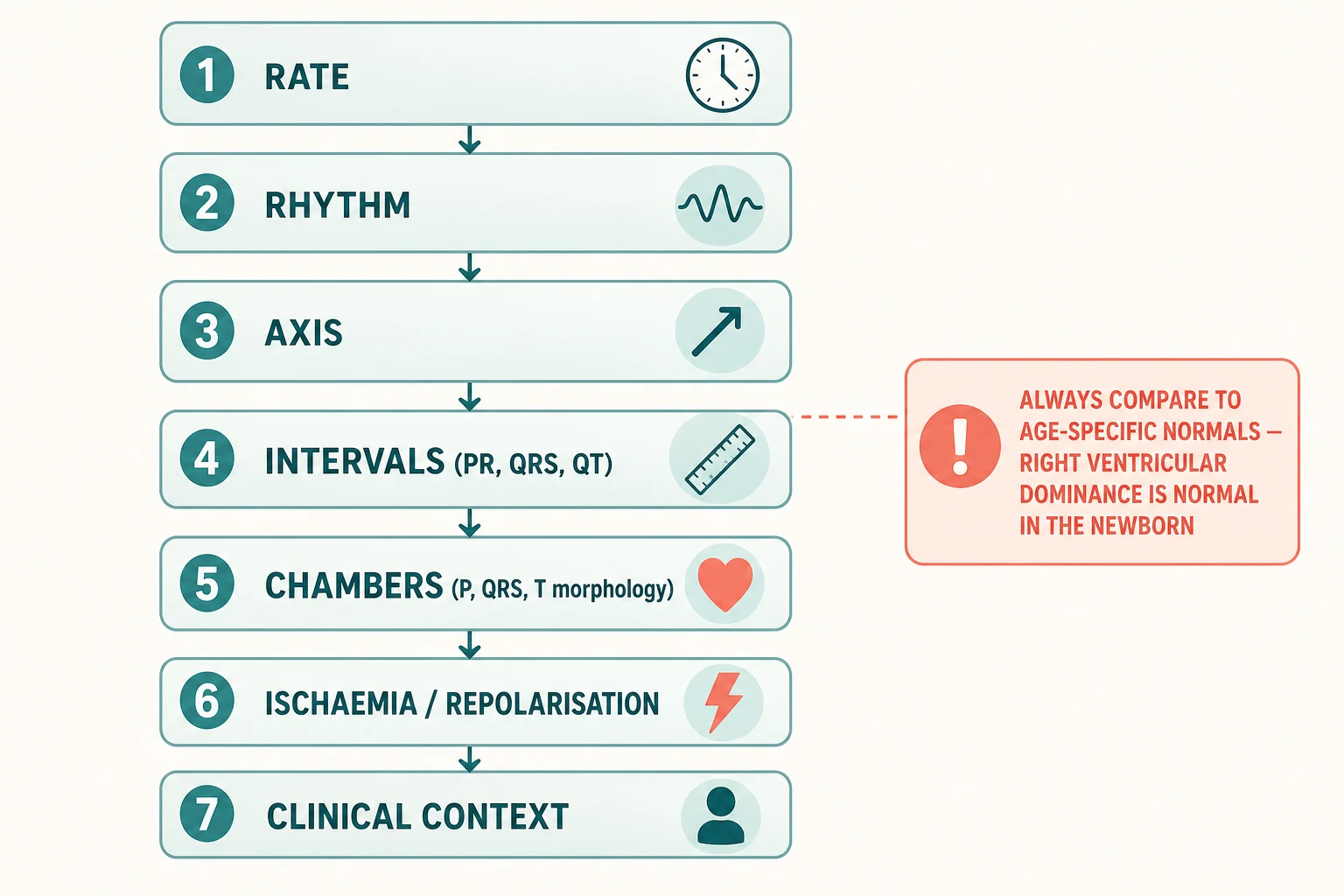
The most important patient-safety risk is reading a child's ECG against adult normals. The newborn right axis, the dominant R wave in V1, the inverted T waves in V1 to V3, and the longer QTc of infancy are all normal in the right age band, and mistaking them for right ventricular hypertrophy, ischaemia, or a channelopathy generates unnecessary cardiology referral, parental anxiety, and occasionally iatrogenic harm from unnecessary restriction or investigation. The reverse error — dismissing a QTc of 500 milliseconds in a teenager with exertional syncope as "normal for the child" — is the more dangerous mistake. [6] [12]
Pathophysiology
The teaching model runs from the cellular origin of the ECG signal to the age-related remodelling that makes a child's tracing distinct from an adult's, and it rests on two facts — the heart is an electrical organ, and its electrical anatomy changes with age. [1] [9]
Every wave on the surface ECG corresponds to a phase of myocardial depolarisation or repolarisation. The P wave is atrial depolarisation; the PR interval is the time from atrial to ventricular depolarisation, dominated by AV nodal conduction; the QRS complex is ventricular depolarisation, the broad fast spike; the ST segment is the brief isoelectric period of plateau-phase ventricular action potentials; and the T wave is ventricular repolarisation. The QT interval is the total duration of ventricular depolarisation plus repolarisation, and because it shortens as heart rate rises, it is conventionally corrected to a heart rate of 60 using Bazett's formula (QTc = QT divided by the square root of the RR interval in seconds). Bazett overcorrects at fast heart rates and undercorrects at slow rates, which matters in a small child whose heart rate is often 130 to 150, and the modern cardiology literature prefers Fridericia (cube root of RR) or a subject-specific formula for drug-safety work, but Bazett remains the bedside and screening standard. [12] [5]
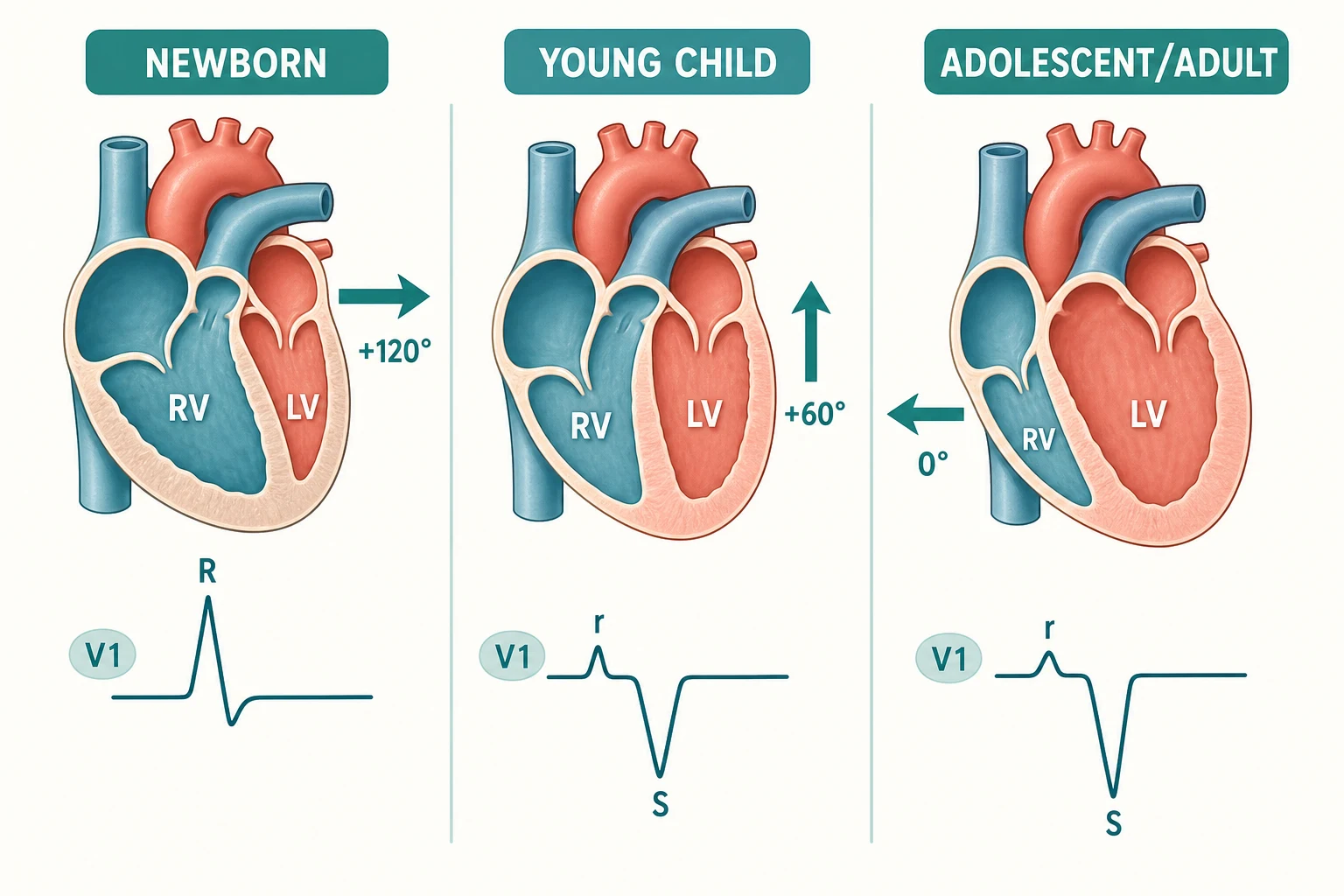
The single most testable physiological fact is that the newborn right ventricle is dominant. Through fetal life the right ventricle ejects the bulk of the cardiac output across the foramen ovale and ductus arteriosus into the systemic circulation, and at birth it is as thick as, or thicker than, the left ventricle. After birth, pulmonary vascular resistance falls, the ductus closes, and the left ventricle progressively takes over the systemic workload and thickens relative to the right. This remodelling is read on the surface ECG as a rightward QRS axis and dominant R waves in V1 in the newborn, which evolve to a leftward axis and a dominant S wave in V1 with a small r (the "rS" complex) in the older child and adult. [9] [1]
The T-wave pattern evolves in parallel. In the newborn, the T wave in V1 is upright in the first 24 to 48 hours of life as the right ventricle is still dominant, then inverts over the first week and remains inverted through childhood in V1 to V3 — the so-called juvenile T-wave pattern. The T waves only become upright in the right precordial leads again at adolescence; a persistent inverted T wave in V1 to V3 in an adult, or an upright T wave in V1 in an older child, is occasionally the first clue to right ventricular pathology such as arrhythmogenic right ventricular cardiomyopathy. [2] [10]
Clinical Presentation
The clinical scenarios that prompt a paediatric ECG are few and well defined, and the first task is to decide which of them the child is in, because the urgency of the tracing and the threshold for cardiology referral differ. [2] [4]
The commonest diagnostic scenario is palpitations or a documented fast heart rate. Picture the irritable neonate with a heart rate of 240, or the school-age child with sudden racing of the heart that stops as abruptly as it began. In these children the ECG captures the arrhythmia. If the child is in sinus rhythm when seen, the ECG looks for a pre-excitation pattern or a prolonged QTc as the substrate. The second is syncope, in whom the ECG is one of the first-line investigations and is most informative when the syncope was exertional, was triggered by emotion or a loud noise, occurred in water, or is accompanied by a family history of sudden death or deafness — the constellation that raises long QT syndrome. The third is chest pain, in whom the ECG is normal in the great majority but is mandatory to exclude an anomalous coronary, myocarditis, or pericarditis when the pain is exertional, severe, or accompanied by fever, dyspnoea, or a friction rub. [2] [6]
The fourth scenario is the routine or screening ECG — the pre-sport or pre-stimulant-medication tracing, the ECG in a child with a murmur being worked up for structural heart disease, or the ECG in a first-degree relative of a patient with a channelopathy. The fifth is the cardiac-arrest rhythm strip, in whom the ECG during resuscitation decides between shockable (ventricular fibrillation or pulseless VT), non-shockable but treatable (slow PEA, Brad-asystole), and the rhythms that need a specific reversible cause. [2] [10]
The presenting features that should prompt urgent rather than elective interpretation are haemodynamic compromise with the arrhythmia, syncope on exertion or with a family history of sudden death, chest pain that is exertional or angina-like, a neonate with a heart rate above 220 or an infant above 200, a wide-complex tachycardia, and any rhythm that the bedside clinician cannot confidently name. The presenting features that should prompt a paediatric cardiology referral rather than a "watch and wait" are a QTc above 480 milliseconds in an infant or above 470 milliseconds in an older child, complete heart block of any cause, a wide-complex tachycardia, a pre-excitation pattern with syncope, and an ECG pattern the bedside clinician cannot interpret confidently. [6] [5]
| Scenario | Urgency | What it dictates |
|---|---|---|
| Palpitations or documented tachycardia, captured | Urgent ECG; stat if haemodynamically compromised | Wide vs narrow QRS; SVT vs sinus; look for pre-excitation and prolonged QTc once in sinus rhythm |
| Syncope, exertional or with family history of sudden death | Urgent ECG and cardiology referral | Measure QTc carefully; screen for long QT, Brugada pattern, pre-excitation, and structural disease with echocardiography |
| Chest pain, exertional or severe | Urgent ECG | Look for ischaemia, pericarditis, myocarditis, ventricular ectopy; consider anomalous coronary if ECG and echo discordant |
| Routine pre-sport or pre-stimulant screening | Elective ECG | Apply age-appropriate normal ranges; refer only the abnormal or the suspicious |
| Cardiac arrest | Stat rhythm strip | Decide shockable vs non-shockable; identify reversible causes (4 Hs and 4 Ts) alongside the rhythm |
The trap is the child whose ECG is technically poor but is reported as "normal" or "abnormal" on that tracing — a squirming infant generates baseline wander and muscle artefact that mimic ST changes and T-wave inversion, and a mistraced QRS can be read as a bundle branch block. The discipline is to repeat the tracing in a calm child before committing to an abnormal reading. [3] [1]
Differential Diagnosis
The differential at the bedside is not "what is causing the palpitations" — it is whether the ECG is normal for the child's age, abnormal but benign, or abnormal and requiring urgent referral. Frame the read around three questions and the right action follows. [2] [6]
Normal for age
default
- Rate, rhythm, axis, intervals and repolarisation all within the age-specific normal range
- Neonatal right axis, dominant R in V1, juvenile T-wave inversion in V1 to V3 accepted
- Reassure the family; no cardiology referral needed
- Document the read against age-appropriate ranges
Abnormal but benign
- Sinus arrhythmia in a child (phasic with respiration)
- Isolated premature atrial or ventricular ectopics that suppress on exercise and are otherwise structurally normal
- First-degree AV block in an asymptomatic older child with an otherwise normal ECG
- Confirm with history and clinical examination; follow up only if symptomatic
Abnormal, urgent referral
- QTc above 480 ms in infant or above 470 ms in older child, especially with syncope or family history
- Second- or third-degree AV block, or a wide-complex tachycardia
- Pre-excitation with syncope, or ventricular ectopy with structural disease
- Refer to paediatric cardiology the same day; treat arrhythmia per APLS if haemodynamically compromised
Technical artefact, not pathology
- Baseline wander from a moving or crying child
- Muscle tremor simulating atrial flutter or ventricular fibrillation
- Wrong lead placement generating axis shift or R-wave regression
- Repeat the tracing in a calm child before any abnormal read is committed
A second layer of differential is the named patterns an examiner will reward for identifying. A short PR interval with a delta wave and a widened QRS is ventricular pre-excitation (Wolff-Parkinson-White pattern). A QTc above 480 milliseconds in the infant or above 470 milliseconds in the older child is long QT until proven otherwise. A Brugada pattern is a coved ST-segment elevation in V1 to V3 with a right bundle branch block morphology. A dominant R wave in V1 in an older child, beyond the age at which right ventricular dominance has resolved, raises right ventricular hypertrophy or an atrial septal defect. An rSR' in V1 with a QRS under 120 milliseconds is a right bundle branch block pattern, common after surgical repair of congenital heart disease. [2] [5]
The sinus arrhythmia deserves a specific question because it is common and often mistaken for pathology. Phasic slowing and speeding of the sinus rate with respiration is the normal autonomic signature of a healthy child's heart and is not an arrhythmia in the disease sense; the heart rate varies with the respiratory cycle, the P-wave morphology is unchanged, and each P wave is conducted. The teaching is that sinus arrhythmia in a child is a sign of a healthy, vagally-toned heart, not a sign of disease. [2]
Clinical & Bedside Assessment
Assessment before an ECG is short and focused: it asks what the question the tracing has to answer is, how to acquire a technically adequate recording in this particular child, and which age-specific normal ranges will be applied. The aim is never to be surprised by a poor tracing or a misread. [1] [3]
Begin with a focused clinical history. Ask about the symptom that prompted the ECG and its triggers, which include exertion, emotion, sudden noise, and water. Clarify the onset and offset: abrupt in SVT, gradual in sinus tachycardia. Ask about any family history of sudden cardiac death before the age of 40, congenital deafness (the Jervell and Lange-Nielsen long QT phenotype), and structural or electrical heart disease. List any medication the child takes that prolongs the QT interval, including macrolides, fluoroquinolones, ondansetron, antipsychotics, and methadone. Examine the cardiovascular system: heart rate and rhythm, blood pressure, the presence of a murmur, a heave, or a friction rub, the femoral pulses (to exclude coarctation), and the oxygen saturation (cyanotic congenital heart disease often shows left axis deviation or a superior axis on ECG). [2] [6]
Assess the child's likely tolerance of the procedure and plan accordingly. A sleeping neonate can be traced in a cot with the limb leads on the limbs and the chest leads placed gently; a wriggling toddler benefits from a parent holding them and from a warm room, because cold and anxiety generate muscle tremor; a school-age child can usually cooperate if the procedure is explained. A single 10-second strip is the target, and the acquisition should not be prolonged in a child who will not settle, because a longer tracing in an upset child accumulates artefact without diagnostic gain. [1]
The pre-ECG checklist
What is the clinical question the ECG has to answer (arrhythmia, syncope, chest pain, screening, drug monitoring)?
Confirm the child's age and the age-appropriate normal ranges you will apply
Position the child calm, warm and supported; a parent at the bedside often suffices
Place the four limb leads and the six precordial leads in the correct anatomical positions
Set the ECG machine to 25 mm per second and 10 mm per millivolt; confirm the calibration square
Acquire a 10-second 12-lead tracing plus a long lead II rhythm strip; label with name, date, time and age
Investigations
The ECG is the investigation; the question is how to acquire it well and how to read it systematically against the age-specific norms. The minimum acquisition is a standard 12-lead ECG at 25 mm per second and 10 mm per millivolt, with a rhythm strip in lead II (or V1) for at least 10 seconds. The technical conventions are the same as in the adult — paper speed 25 mm per second (one large box equals 200 milliseconds, one small box equals 40 milliseconds), gain 10 mm per millivolt (one large box equals 0.5 millivolt), and a calibration square at the start of the tracing — and they must be checked before any measurement is trusted. [1] [2]
| Measurement | Neonate (0–1 mo) | Infant (1–12 mo) | Child (1–8 yr) | Older child / adolescent |
|---|---|---|---|---|
| Heart rate (awake) | 100–180 bpm | 100–160 bpm | 70–140 bpm | 55–90 bpm |
| PR interval | 80–120 ms | 70–130 ms | 90–150 ms | 100–180 ms |
| QRS duration | 30–70 ms | 40–80 ms | 50–90 ms | 60–100 ms |
| QRS axis | +90 to +190° | +30 to +150° | +10 to +120° | +20 to +100° |
| QTc (Bazett), upper normal | <480 ms | <470 ms | <450–460 ms | M <450, F <460 ms |
| R/S in V1 | R dominant (R/S > 1) | R dominant to transitional | rS (S dominant) | rS (S dominant) |
| T wave in V1 | Upright first 24–48 h, then inverted | Inverted (juvenile T) | Inverted (juvenile T) | Inverted through adolescence |
The interpretation runs in the same order every time — rate, rhythm, axis, intervals, chambers, repolarisation, clinical context — and at every step the measurement is compared to the age-specific range. The rate is read from the RR interval: at 25 mm per second, 300 divided by the number of large boxes between two R waves gives the rate in beats per minute (so a three-large-box interval is 100, a four-large-box interval is 75). The rhythm is read from a long lead II strip: is the rhythm sinus (every P wave followed by a QRS, every QRS preceded by a P wave, a constant PR interval), regular or irregular, and is the irregularity phasic with respiration (benign sinus arrhythmia) or chaotic (atrial fibrillation, rare in children)? The axis is read from the limb leads: the net polarity of the QRS in leads I and aVF approximates the axis quadrant (I positive and aVF positive is a normal axis, I positive and aVF negative is left axis, I negative and aVF positive is right axis, both negative is northwest or indeterminate). [2] [9]
The intervals are the part of the paediatric ECG that changes most with age and is most often misread. The PR interval shortens with faster heart rate and lengthens with age; a PR interval under 90 milliseconds in the infant suggests an accessory pathway. The QRS duration is shorter in the young child because the ventricular mass is smaller, and a QRS over 120 milliseconds is a bundle branch block or a ventricular rhythm at any age. The QT interval is measured from the start of the QRS to the end of the T wave in the lead with the clearest T-wave termination (usually lead II or V5), is corrected with Bazett's formula, and is interpreted against the age-specific threshold — a Bazett-corrected QTc above 480 milliseconds in an infant under six months, or above 470 milliseconds in an older child, is prolonged and warrants cardiology review. [5] [12]
Management — Resuscitation
When the ECG accompanies a child who is haemodynamically compromised by the rhythm shown on it, the order of priorities is airway, breathing, circulation, and the treatment of the arrhythmia, not the elegant classification of the tracing. The ordered bundle is oxygen if hypoxic, intravenous access, and the APLS algorithm for the rhythm, and the ECG is interpreted alongside, not instead of, the resuscitation. [2] [4]
The single most important rule in the tachyarrhythmias is to distinguish narrow-complex from broad-complex, because the management diverges. A narrow-complex tachycardia with no discernible P waves and a heart rate above 220 in an infant or above 180 in a child is supraventricular tachycardia until proven otherwise. If the child is shocked, the treatment is synchronised electrical cardioversion at 0.5 to 1 joule per kilogram, escalating if needed, under sedation if time permits. If the child is stable, the first manoeuvre is vagal manoeuvres appropriate to age. A cold pack to the face uses the diving reflex in the infant, while Valsalva suits the cooperative older child. These are followed by intravenous adenosine at 100 micrograms per kilogram as a rapid bolus, escalating to 300 micrograms per kilogram if the first dose fails. A broad-complex tachycardia in a haemodynamically compromised child is treated as ventricular tachycardia — synchronised cardioversion at 0.5 to 1 joule per kilogram if a pulse is present, or defibrillation at 4 joules per kilogram if pulseless — and amiodarone 5 milligrams per kilogram is added if the rhythm is refractory. [2]
Adenosine (supraventricular tachycardia, stable child, ANZ / APLS)
For the bradyarrhythmias, a slow heart rate with haemodynamic compromise is symptomatic bradycardia, and the APLS algorithm treats reversible causes (hypoxia is the commonest in a child) and gives intravenous adrenaline 10 micrograms per kilogram if the bradycardia persists after airway and oxygenation, escalating to an adrenaline infusion or external cardiac pacing for refractory symptomatic bradycardia. Congenital complete heart block in a neonate often needs transcutaneous or transvenous pacing while awaiting cardiology input and definitive pacemaker placement. [2]
For the pulseless arrest, the ECG decides between shockable (ventricular fibrillation or pulseless VT) and non-shockable (asystole or PEA) rhythms and the APLS algorithm runs uninterrupted high-quality chest compressions with two-minute rhythm checks; reversible causes are sought alongside the algorithm. The interpretation of the arrest ECG is binary — shockable or not — and the elegant paediatric subtleties are deferred to the post-arrest 12-lead once a pulse returns. [2]
Management — Definitive & Stepwise
Once the tracing has been acquired and the urgent arrhythmia addressed, the systematic interpretation of the 12-lead ECG is an ordered sequence that should run the same way every time: rate, rhythm, axis, intervals, chambers, repolarisation, clinical context. [1] [2]
Rate. Read from the RR interval at 25 mm per second: 300 divided by the number of large boxes between R waves. A neonate at 140, a toddler at 110, a teenager at 70 are all normal sinus rates. A rate above 180 in an infant that is regular and narrow-complex with no visible P waves is SVT until proven otherwise; a rate below 60 in a child with haemodynamic compromise is symptomatic bradycardia. [2]
Rhythm. On a long lead II strip, ask four questions: is every P wave followed by a QRS, is every QRS preceded by a P wave, is the PR interval constant, and is the rhythm regular? Sinus rhythm answers all four yes; sinus arrhythmia adds phasic variation with respiration and is normal in a child; SVT shows no visible P waves and a narrow regular tachycardia; atrial flutter shows sawtooth flutter waves, most often in a child with structural heart disease; atrial fibrillation is chaotically irregular and rare in a structurally normal child. [2] [4]
ARRANGED
Axis. The limb leads give the frontal plane axis. In the newborn the axis is rightward, +90 to +190 degrees, reflecting right ventricular dominance; the axis shifts leftward through infancy and childhood to the adult range of +20 to +100 degrees. Right axis deviation beyond the age-specific range raises right ventricular hypertrophy, an atrial septal defect, or a posteroseptal accessory pathway; left axis deviation (more negative than −30 degrees, or a superior axis in the neonate) raises AV canal defect, tricuspid atresia, or a left anterior fascicular block, and is a recognised clue to certain forms of congenital heart disease. [9] [1]
Intervals. The PR interval lengthens with age as the AV node matures and the heart rate slows; a PR interval under 90 milliseconds in the infant suggests an accessory pathway and warrants a search for a delta wave. The QRS duration lengthens with age as the ventricular mass grows; a QRS over 120 milliseconds is a bundle branch block or a ventricular rhythm at any age. The QT interval is corrected for heart rate with Bazett's formula and interpreted against the age-specific threshold: a Bazett QTc above 480 milliseconds in an infant under six months or above 470 milliseconds in an older child is prolonged, and a QTc above 500 milliseconds at any age is a high-risk torsades phenotype. When tracking QTc on a known QT-prolonging drug, the Fridericia formula or a linear formula is preferred to minimise the rate-dependent artefact of Bazett. [5] [12]
Chambers. The P wave gives atrial size — a tall peaked P wave in lead II or V1 (P pulmonale) suggests right atrial enlargement, a broad notched P wave (P mitrale) suggests left atrial enlargement. The QRS gives ventricular size — a dominant R wave in V1 beyond the neonatal period (R in V1 plus S in V6 above the age-specific threshold, or a pure R in V1 in an older child) raises right ventricular hypertrophy; a tall R wave in V6 with a deep S in V2 raises left ventricular hypertrophy. The voltage criteria for hypertrophy are age-specific and the borderline voltage in a slim adolescent should be interpreted with the echocardiogram. [2] [10]
Repolarisation. The ST segment and T wave are read against the juvenile pattern. An ST elevation across multiple leads in a child with chest pain is pericarditis, myocarditis, or an anomalous coronary until proven otherwise. A deep T-wave inversion in the lateral leads beyond the normal juvenile pattern raises hypertrophic cardiomyopathy, particularly if the voltage criteria for left ventricular hypertrophy are also met. A coved ST elevation in V1 to V3 with a right bundle branch block pattern is the Brugada pattern and warrants urgent electrophysiology referral. [2] [6]
Specific Subtypes & Scenarios
The approach to the paediatric ECG changes with the child and the clinical question, and the fellowship candidate must adjust the read and the threshold for referral to the subtype in front of them. [1] [6]
In the neonate, the ECG is dominated by right ventricular physiology: right axis deviation (axis +90 to +190 degrees), dominant R waves in V1 (R/S ratio greater than 1), upright T waves in V1 in the first 24 to 48 hours that then invert, and shorter PR and QRS intervals than in the older child. The neonatal QTc is also longer than the older child's, with an upper normal of 480 milliseconds by Bazett, and the modern case for ECG screening in infancy rests on the observation that a substantial fraction of infants who die of sudden infant death syndrome have a prolonged QTc that would be detected by a neonatal ECG. The neonate with a wide-complex tachycardia and haemodynamic compromise is treated as VT until proven otherwise. [7] [8]
In the infant and young child, the right ventricle is still dominant but the axis and intervals are evolving toward adult values; the T waves in V1 to V3 remain inverted (juvenile pattern), and a sinus rate of 110 to 140 is normal. The classic infant arrhythmia is accessory-pathway SVT, presenting with poor feeding, irritability, and a heart rate above 220; the ECG in SVT shows a narrow regular tachycardia with no visible P waves, and the post-cardioversion ECG may show a delta wave and short PR of Wolff-Parkinson-White pattern. [2] [4]
In the school-age child, the axis is in the adult range, the juvenile T-wave pattern persists in V1 to V3, and the arrhythmias of childhood (accessory-pathway SVT, atrial ectopic tachycardia) coexist with the emerging channelopathies that declare themselves with exertional syncope. The screening ECG before stimulant medication for ADHD is a defensible indication, and the read should focus on the QTc, on pre-excitation, and on any structural-heart-disease pattern. [4] [12]
In the adolescent and the young athlete, the ECG overlaps with the adult range and the question is the differentiation of the athlete's heart (early repolarisation, isolated voltage criteria for left ventricular hypertrophy, sinus bradycardia, first-degree AV block) from the inherited cardiomyopathies and channelopathies that cause sudden death in sport. The International Recommendations for ECG Interpretation in Athletes separate the normal physiological training-related findings (which do not require investigation) from the borderline and abnormal findings (which require further investigation with echocardiography, exercise testing, or electrophysiology). The QTc in an athlete should be measured at rest and at peak exercise, because a borderline resting QTc that fails to shorten normally with exercise raises long QT syndrome. [10] [11]
In the child on a QT-prolonging drug (macrolides, fluoroquinolones, ondansetron, antipsychotics, methadone), a baseline ECG and a follow-up ECG after the drug is established are the practical monitoring, and the Fridericia correction is preferred to Bazett for tracking the QTc over time, because the child's heart rate often changes between tracings. [12]
In the child with congenital heart disease, the ECG is part of the longitudinal follow-up and the read must integrate the structural lesion (a superior axis in AV canal defect; left axis deviation and a dominant R in V1 in tricuspid atresia; a Q in V6 in a duct-dependent lesion; the rSR' in V1 after surgical repair) with the rhythm disturbances that complicate the natural history and the surgery. [2]
Complications & Pitfalls
The "complications" of a non-invasive ECG are not procedural; they are the harms of a misread — the false positive that generates unnecessary referral and anxiety, and the false negative that misses a child at risk of sudden death. The discipline is to acquire a technically adequate tracing and to apply the age-specific norms systematically. [3] [4]
The common pitfall is reading the child's ECG against adult ranges. A neonate with right axis deviation, a dominant R in V1, and an inverted T in V1 after the first week is normal; an infant with a QTc of 460 milliseconds by Bazett at a heart rate of 150 is normal; a school-age child with T-wave inversion in V1 to V3 is showing the juvenile pattern. Each of these, read against adult ranges, generates a false positive and an unnecessary cardiology referral. The opposite — dismissing a QTc of 500 milliseconds in a 14-year-old with exertional syncope as "a fast-rate Bazett artefact" — is the more dangerous mistake. [1] [6]
The serious pitfall is missing a child at risk of sudden cardiac death. A QTc above 480 milliseconds in an infant or above 470 milliseconds in an older child, with syncope, a family history of sudden death, or congenital deafness, is long QT syndrome until proven otherwise. A pre-excitation pattern with syncope is high-risk Wolff-Parkinson-White. A wide-complex tachycardia in a haemodynamically compromised child is VT until proven otherwise. Second- or third-degree AV block in a neonate raises congenital complete heart block, often from maternal anti-Ro and anti-La antibodies, and needs urgent pacing evaluation. [5] [6]
A frequently tested misconception is that the QTc is the same measurement regardless of heart rate. It is not: the raw QT shortens as heart rate rises, and the Bazett correction overcompensates at the fast rates of infancy and young childhood, so a Bazett QTc at a heart rate of 150 reads longer than at 80. The practical implication is to repeat an unexpectedly long QTc at a slower rate if the child is calm, and to use Fridericia for drug monitoring. [12] [5]
Prognosis & Disposition
The prognosis after a paediatric ECG is dictated almost entirely by the underlying rhythm or lesion, not by the ECG itself. The disposition is therefore a function of what the tracing shows, not that the tracing was performed. [2] [6]
For a normal ECG in an asymptomatic child, the disposition is reassurance and return to normal activity; no cardiology follow-up is needed. The discipline is to have applied the age-specific ranges, so that a normal neonate is not referred for "right axis deviation" and a normal school-age child is not referred for "juvenile T-wave inversion in V1 to V3". [1]
For an abnormal but benign ECG — sinus arrhythmia, isolated ectopics that suppress on exercise, first-degree AV block in an asymptomatic older child — the disposition is clinical follow-up with the general paediatrician, with a low threshold for cardiology referral if symptoms evolve. An exercise test that suppresses the ectopics is reassuring. [2]
For the child with a channelopathy or a high-risk arrhythmia substrate, the disposition is urgent paediatric cardiology referral the same day. These substrates include a prolonged QTc, a Brugada pattern, a pre-excitation with syncope, and complete heart block. Treatment follows the APLS algorithm if the child is haemodynamically compromised. Give the family a clear written and verbal handover of the rationale for the referral and the next steps. The long-term prognosis of treated long QT syndrome is excellent with beta-blockade and activity modification; the prognosis of untreated long QT syndrome carries a measurable risk of sudden death. [5] [6]
For the child resuscitated from a cardiac arrest, the disposition is paediatric intensive care, a post-arrest 12-lead ECG, and the workup for the underlying cause (channelopathy, anomalous coronary, myocarditis, drug overdose), because the ECG that prompted the resuscitation is now part of a longitudinal risk-stratification pathway. [2]
Special Populations
The approach to the paediatric ECG is adjusted for the child in front of you, and the fellowship candidate must show that they can match the read and the referral threshold to the population. [1] [6]
In the neonate, the right-ventricular-dominant ECG, the longer QTc, and the shorter intervals are normal, and the case for a routine neonatal ECG to screen for a prolonged-QT infant at risk of SIDS is supported by the observation that a meaningful fraction of SIDS infants have a prolonged QTc on the neonatal tracing. The neonate with a wide-complex tachycardia is treated as VT until proven otherwise. [7] [8]
In the child with congenital heart disease, the ECG is part of the structural diagnosis (the superior axis of AV canal, the left axis of tricuspid atresia, the right axis of an ASD) and of the longitudinal follow-up after surgical repair, where the rSR' in V1, the residual voltage criteria for hypertrophy, and the arrhythmia substrate (atrial flutter, ventricular ectopy) dictate the cardiology pathway. [2]
In the child on a QT-prolonging drug, the baseline and follow-up ECGs monitor the QTc, and the Fridericia correction is preferred to Bazett for tracking over time. The child on a macrolide, an antipsychotic, or methadone is the one in whom a "borderline" Bazett QTc at a fast heart rate should be rechecked before a drug is changed. [12]
In the young athlete, the ECG separates the physiological training-related changes (early repolarisation, isolated voltage criteria for hypertrophy, sinus bradycardia, first-degree AV block) from the inherited cardiomyopathies and channelopathies that cause sudden death in sport, using the International Recommendations for ECG Interpretation in Athletes. The QTc is measured at rest and at peak exercise. [10] [11]
In the first-degree relative of a patient with a channelopathy, the screening ECG is part of a broader workup that includes genetic testing, and the read must integrate the QTc, the Brugada pattern, the pre-excitation, and the structural echo with the family history. [6]
In the Indigenous, remote, or under-resourced setting, access to paediatric cardiology and to age-specific normal ranges at the bedside may be limited, and the equity intervention is to acquire a technically adequate tracing, to apply the systematic age-referenced read, to refer on a small defensible list of red flags, and to use telehealth and retrieval to bridge the distance. [3]
In the technology-dependent or neurodivergent child, the procedure is planned with extra time, a communication strategy appropriate to the child, and a sedation or distraction plan that the child and family can support, because a clean tracing in a calm child is more informative than a longer tracing in an upset one. [1]
Evidence, Guidelines & Regional Differences
The evidence base for the paediatric ECG has matured in three areas: the normal age-specific intervals, the role of ECG screening in infancy, and the interpretation of the athlete's ECG. The candidate should know each one and the regional deltas that follow from them. [1] [8]
The age-specific normal ranges are anchored on the classic Davignon and Rautaharju datasets, refined by modern Z-score analyses. The neonatal QRS axis evolution has been mapped in detail in the first four weeks of life, confirming the rightward axis of the newborn and its leftward shift. The QTc thresholds are derived from the Schwartz diagnostic criteria for long QT syndrome, with a Bazett QTc above 480 milliseconds in the infant under six months and above 470 milliseconds in the older child flagged as prolonged, and the modern drug-safety literature prefers the Fridericia correction to Bazett because Bazett overcorrects at fast heart rates. [5] [9]
The role of ECG screening in infancy rests on the observation that a substantial fraction of infants who die of sudden infant death syndrome have a prolonged QTc on a neonatal tracing, and that early identification and treatment of long QT syndrome prevents sudden death. The case for universal neonatal ECG screening has been argued on these grounds, and a consensus statement set out the rationale and objectives for ECG screening in infancy, although universal screening has not been adopted in most countries including Australia and the United Kingdom. [7] [8]
Prolonged QT interval and the sudden infant death syndrome (NEJM 1998)
PMID 9624190
Population: Infants with an ECG recorded on day 3 or 4 of life in a large Italian birth cohort
Comparator: Infants with a normal neonatal QTc
Key finding
Infants who subsequently died of SIDS had a markedly longer mean QTc on the neonatal ECG than survivors, supporting prolonged QTc as an identifiable risk factor in a subset of SIDS and underpinning the case for neonatal ECG screening.
The interpretation of the athlete's ECG has been standardised by the International Recommendations for ECG Interpretation in Athletes, which separate the normal physiological training-related findings (which do not require investigation) from the borderline and abnormal findings (which do). The Z-score-based approach refines the read by expressing each measurement against an age-, sex- and ethnicity-specific reference, and exercise testing is the gold standard for the diagnosis of long QT syndrome where the resting QTc is borderline. [10] [11]
Several points remain weak or contested. The optimal QTc correction formula in infancy is unresolved, with Bazett the bedside standard despite its rate-dependent artefact. The case for universal neonatal ECG screening is supported by the SIDS-association data but is not adopted in most countries. The threshold for cardiology referral in the asymptomatic child with a borderline QTc is debated, with 460 to 480 milliseconds in the older child a grey zone. The role of the ECG in routine pre-sport screening of the young athlete is recommended by some sporting bodies, though its cost-effectiveness is contested. Each is a defensible topic for the viva. [12] [10]
Exam Pearls
The fellowship examiner expects a candidate who can acquire a technically adequate tracing, interpret it systematically against the age-specific norms, and recognise the patterns that demand urgent referral. [1] [2]
The single most testable fact is that the paediatric ECG is dominated by the right ventricle in the newborn and evolves toward the adult pattern through childhood. A neonate with right axis deviation, a dominant R in V1, an upright T in V1 in the first week that then inverts, a QTc up to 480 milliseconds by Bazett, and a heart rate of 140 is normal. The same tracing in a teenager would be abnormal. [9] [1]
The exam rewards naming several abnormal patterns. A short PR with a delta wave and a wide QRS is the Wolff-Parkinson-White pattern. A QTc above 480 milliseconds in an infant or above 470 milliseconds in an older child, with syncope, family history, or deafness, is long QT syndrome. A coved ST elevation in V1 to V3 with a right bundle branch block morphology is the Brugada pattern. A superior axis in a neonate raises an AV canal defect or tricuspid atresia. A dominant R in V1 in an older child raises right ventricular hypertrophy or an atrial septal defect. [5] [6]
The resuscitation doses that must be quoted exactly: adenosine 100 micrograms per kilogram as a first IV bolus in SVT, escalating to 300 micrograms per kilogram; synchronised DC cardioversion 0.5 to 1 joule per kilogram in a shocked narrow-complex tachycardia; adrenaline 10 micrograms per kilogram in symptomatic bradycardia; 4 joules per kilogram defibrillation for pulseless VT or VF. The paediatric nuances — SVT presenting with heart rates above 220 in the infant, VT treated as the default for any wide-complex tachycardia in a sick child — are the marks that distinguish the paediatric from the adult answer. [2]
The exam rewards naming several classic distractors. Reading a neonate's right axis as right ventricular hypertrophy is a false positive. Calling a school-age child's inverted T waves in V1 to V3 "ischaemia" is a false positive. Relying on a single Bazett QTc at a heart rate of 150 to diagnose long QT is a mistake. Treating a wide-complex tachycardia in an infant as SVT with aberrancy is dangerous. Reporting a technically poor tracing as abnormal without repeating it in a calm child is avoidable. [3] [12]
References
- [1]Miliaraki M, Protogeros D, Mazaris A, et al Pediatric Electrocardiogram in Preparticipation Screening: Narrative Review of Normal Values in Key Features Children (Basel), 2026.PMID 41749567
- [2]Sharieff GQ, Rao SO The pediatric ECG Emerg Med Clin North Am, 2006.PMID 16308120
- [3]Wathen JE, Shaikh KA, Merritt CG, et al Accuracy of ECG interpretation in the pediatric emergency department Ann Emerg Med, 2005.PMID 16308065
- [4]Gandhi S, Luetmer PH, O'Meara JG, et al Predictors of abnormal electrocardiograms in the pediatric emergency department Ann Pediatr Cardiol, 2018.PMID 30271014
- [5]Schwartz PJ, Moss AJ, Vincent GM, Crampton RS Diagnostic criteria for the long QT syndrome. An update Circulation, 1993.PMID 8339437
- [6]Zareba W, Moss AJ, Schwartz PJ, et al Long QT syndrome in children J Electrocardiol, 2001.PMID 11781951
- [7]Schwartz PJ, Stramba-Badiale M, Segantini A, et al Prolongation of the QT interval and the sudden infant death syndrome N Engl J Med, 1998.PMID 9624190
- [8]Saul JP, Schwartz PJ, Ackerman MJ, et al Rationale and objectives for ECG screening in infancy Heart Rhythm, 2014.PMID 25239430
- [9]Pærregaard MM, Bjerre JV, Johansen M, et al The Evolution of the Neonatal QRS Axis during the First Four Weeks of Life Neonatology, 2021.PMID 33691309
- [10]Park J, Joo E, Kim JH, et al Fine Tuning ECG Interpretation for Young Athletes: ECG Screening Using Z-score-based Analysis Sports Med Open, 2024.PMID 39441450
- [11]Pinsky AM, Tran N, Bos JM, et al Proceed with caution: Standard protocol exercise stress tests fail to replicate the diagnostic utility of supine-stand tests for long QT syndrome Pacing Clin Electrophysiol, 2024.PMID 38348899
- [12]Gotta V, Egli A, Wieser M, et al QT interval prolongation: clinical assessment, risk factors and quantitative pharmacological considerations J Pharmacokinet Pharmacodyn, 2025.PMID 41204044