Paeds · mental-behavioural-and-psychosomatic
Delirium in children and adolescents
Also known as Paediatric delirium · Pediatric delirium · PICU delirium · Acute brain dysfunction in critically ill children · Hospital-acquired delirium in children
Fellowship guide to delirium in children and adolescents: DSM-5-TR criteria-based clinical diagnosis, motoric subtypes (hyperactive, hypoactive, mixed), CAPD and pCAM-ICU screening, the ABCDEF prevention bundle, cause-first treatment with non-pharmacologic priorities, antipsychotics as last resort, and the 2022 SCCM PADIS guideline evidence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the five-year-old, three days post-cardiac surgery, who was sitting up and chatting yesterday and today cannot recognise her parents, pulls at her lines, and cannot settle to sleep. That acute change in attention and awareness in an ill child is delirium until proven otherwise — and it is far commoner than most clinicians realise. [5]
Delirium is defined by the DSM-5-TR as a disturbance in attention and awareness that develops acutely, fluctuates through the day, and represents a change from baseline, with additional disturbance in cognition, and is the direct physiological consequence of a medical condition, substance intoxication or withdrawal, or toxin exposure. It does not occur exclusively in the context of a coma, and it is not better explained by a pre-existing neurocognitive disorder. [1]
The single most important conceptual shift for paediatric trainees is this: delirium in children is not rare, not benign, and not a psychiatric diagnosis. It is acute brain dysfunction — an organ-failure equivalent of the brain — and it signals that something is physiologically wrong. The child who is acutely confused needs the same urgency as the child who is acutely hypoxic. [5] [6]
Classification
Paediatric delirium sorts into clinical shapes that change what you do, and the first split is by motoric subtype: hyperactive, hypoactive, and mixed. [5]
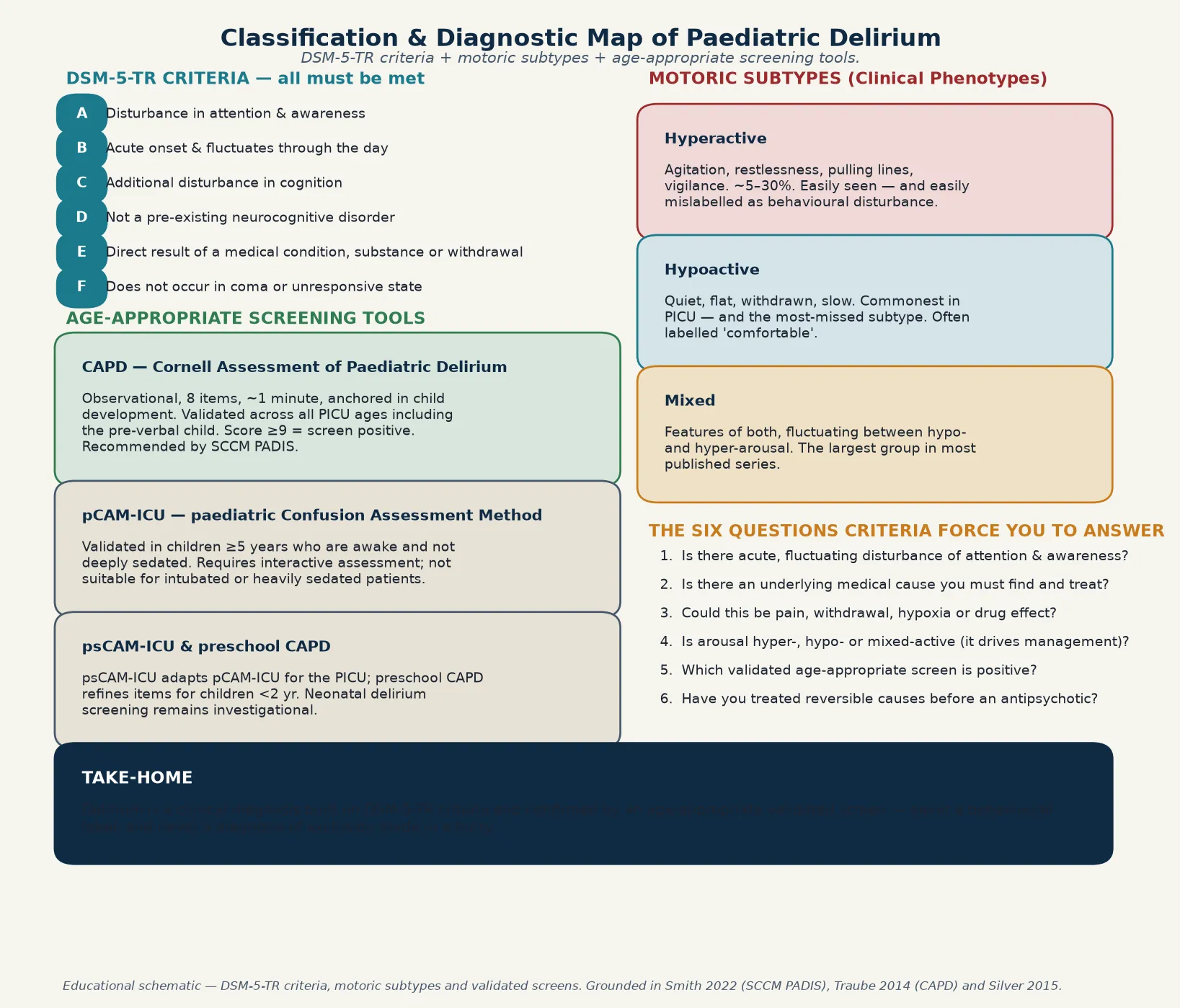
Hyperactive delirium is what most clinicians picture: agitation, restlessness, pulling at lines, hypervigilance, and sometimes hallucinations. It accounts for roughly 5–30% of cases and is easily seen — but also easily mislabelled as behavioural disturbance or anxiety, which delays the search for the underlying cause. [5] [6]
Hypoactive delirium is the quiet child who is withdrawn, flat, slow to respond, and minimally interactive. It is the commonest subtype in the PICU and also the most-missed, because the child looks comfortable and does not demand attention. Missing hypoactive delirium is a serious clinical error — it carries at least the same morbidity as the hyperactive form. [5] [6]
Hyperactive
Agitated, restless
- Pulling lines, hypervigilant, sometimes hallucinating
- ~5–30% of cases — easily seen
- Often mislabelled as behavioural disturbance or anxiety
- Risk: over-sedation to control behaviour instead of cause-finding
Hypoactive
Quiet, withdrawn
- Flat affect, slow, minimally interactive
- Commonest subtype in PICU — and the most-missed
- Often documented as 'comfortable' or 'settled'
- Risk: under-recognition delays treatment of the underlying cause
Mixed
Fluctuating between both
- Features of both hyper- and hypo-arousal
- Fluctuates through the day and between assessments
- The largest group in most published series
- Requires repeated screening to capture the full picture
A second, useful clinical split is by setting and presumed trigger: PICU-acquired delirium (the commonest, driven by critical illness, sedation, and immobility), postoperative delirium (especially after cardiac surgery), and delirium in children on general wards or with oncological or transplant presentations. The setting changes the differential but not the diagnostic principle: identify delirium, then investigate the cause. [8] [10]
Epidemiology & Risk Factors
Delirium was once thought to be rare in children, but systematic screening in the PICU has transformed the epidemiology. Reported prevalence and incidence range from roughly 20–50% of PICU patients, with the highest rates in the most critically ill and the most heavily sedated. [1] [4]
Headline numbers for viva
The 2023 Ista systematic review and meta-analysis is the definitive synthesis of paediatric delirium risk factors. The factors that consistently emerge are younger age (especially developmental vulnerability of the CNS), greater severity of illness (high PRISM or PIM scores), pre-existing cognitive or neurodevelopmental impairment, mechanical ventilation, and the use of benzodiazepines and other sedatives. [4]
The link between benzodiazepines and delirium is causal, not merely associative. The 2018 Mody study used a target-trial emulation framework to estimate the causal effect of benzodiazepine exposure on delirium development in critically ill children, finding a substantial attributable risk. This is why the 2022 SCCM PADIS guideline recommends preferential use of dexmedetomidine over benzodiazepines for sedation where feasible. [7] [1]
Other important risk amplifiers include immobilisation, sleep disruption, the presence of lines and tubes, anticholinergic medication load, electrolyte and metabolic derangement, infection or sepsis, and the cumulative noise and light exposure of the ICU environment. In oncology patients, delirium is driven by the disease, chemotherapy, transplantation conditioning, infection, and the psychological load of isolation. [8] [4]
Pathophysiology
There is no single broken circuit to name in paediatric delirium. The teaching model that best fits the evidence is a final common pathway: multiple insults converge on the developing brain through three interlocking mechanisms — neuroinflammation, altered neurotransmission, and network disconnection. [14]
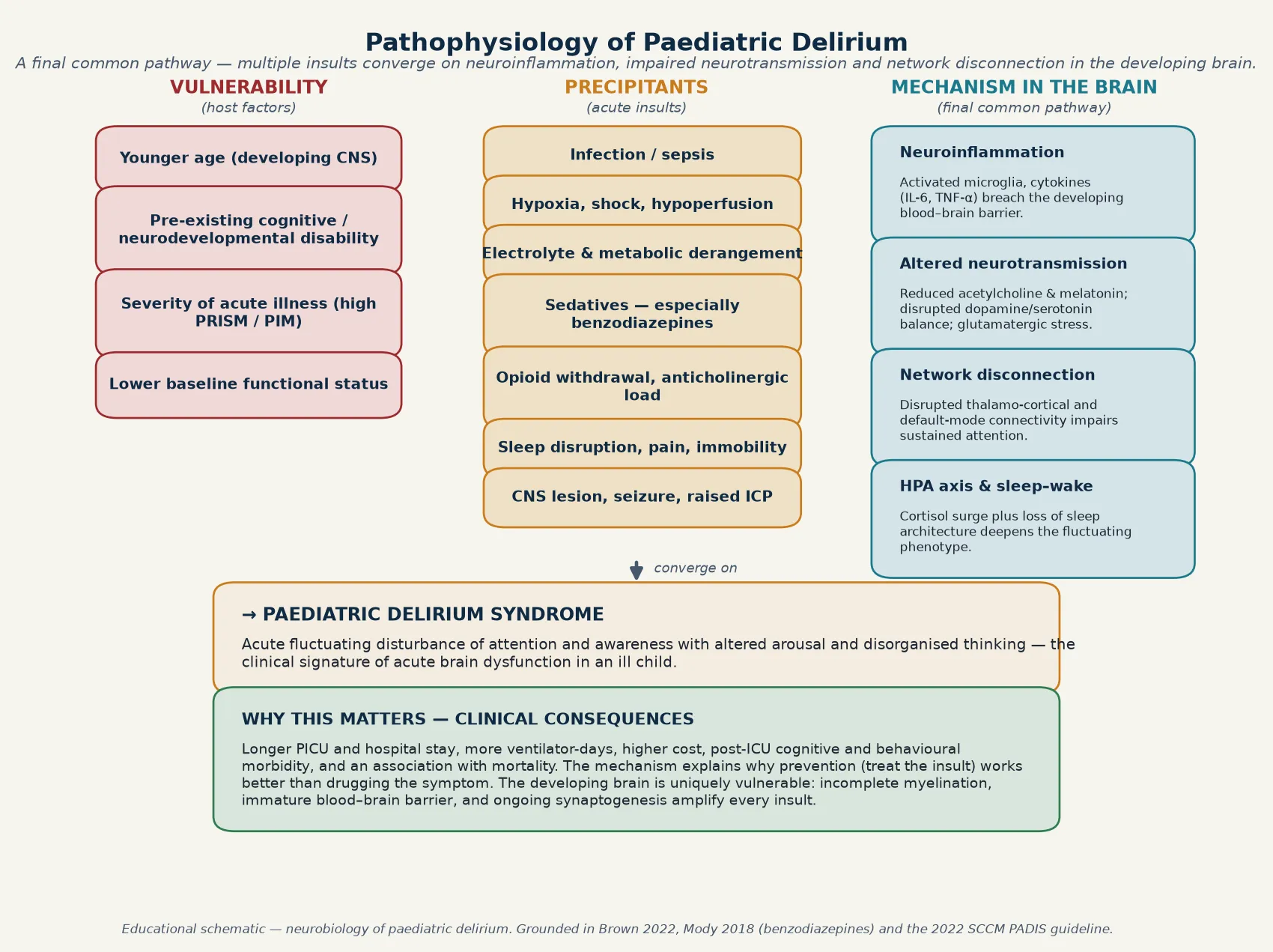
At the mechanism level, neuroinflammation drives activated microglia and a cytokine surge (including IL-6 and TNF-α) that breaches the still-developing blood–brain barrier. Altered neurotransmission includes reduced acetylcholine and melatonin signalling, disrupted dopamine and serotonin balance, and glutamatergic stress. Network disconnection disrupts the thalamo-cortical and default-mode circuits that sustain attention and awareness. [14]
I WATCH DEATH
This pathway model explains two clinically important truths. First, the developing brain is uniquely vulnerable: incomplete myelination, an immature blood–brain barrier, and ongoing synaptogenesis amplify the impact of every insult, which is why younger children are at higher risk. Second, because the mechanism is multi-hit and reversible, prevention and cause-treatment work better than symptomatic drugging — you cannot drug your way out of ongoing sepsis or persistent benzodiazepine exposure. [14] [1]
Clinical Presentation
The child in front of you rarely arrives with a label of delirium. What you see is a change from baseline: the settled child becomes agitated or withdrawn, the interactive child cannot sustain attention, the sleeping child has a disrupted sleep–wake cycle, and the recovering child suddenly looks worse rather than better. [5]
Hyperactive delirium presents with restlessness, agitation, pulling at lines and tubes, hypervigilance, irritability, and sometimes visual or auditory hallucinations. The child may scream, fight care, or appear terrified. This is the presentation that triggers urgent nursing and medical review — but it must trigger delirium screening, not just sedation. [5] [6]
Hypoactive delirium is the quiet, flat, withdrawn child with reduced motor activity, minimal facial expression, slow or absent responses to voice, and reduced interaction with the environment. This child is often documented as comfortable or settled, when in fact they are acutely delirious. Hypoactive delirium is easy to miss at the bedside and is associated with at least equivalent morbidity. [5] [6]
| Bedside observation | Do not stop here | Must still do |
|---|---|---|
| 'Agitated and pulling lines' | This may be hyperactive delirium, not just anxiety | Screen with CAPD; investigate infection, hypoxia, withdrawal, pain |
| 'Quiet and comfortable' | This may be hypoactive delirium — the most-missed subtype | Screen with CAPD; do not reassure without assessing |
| 'Sleeping all day, awake all night' | Sleep–wake disruption is a core DSM-5-TR feature | Screen, correct environment, cluster care, treat the cause |
| 'Not recognising parents' | Acute disorientation in an ill child is delirium until proven otherwise | Urgent neurological assessment, CAPD, neuroimaging if focal signs |
| 'Worse since we started midazolam' | Benzodiazepines are a causal risk factor for delirium | Review the sedation plan; consider dexmedetomidine switch |
The presentation varies with age and developmental stage. Pre-verbal infants and toddlers cannot tell you they are confused, so the clinical signs are behavioural: altered sleep–wake cycle, reduced eye contact, inconsolable crying or abnormal quietness, dystonia or dyskinesia, and regression in developmental skills. School-age children and adolescents can show more recognisable features: disorientation, rambling or incoherent speech, perceptual disturbances, and impaired attention on formal testing. [3] [5]
The clinical course is fluctuating — this is the single most distinctive feature. A child who was delirious in the morning may appear lucid at midday and delirious again by evening. This is why screening must be repeated at least twice daily, and why a single normal assessment never excludes delirium. [1] [2]
Differential Diagnosis
Build the differential in four piles so you do not anchor on the obvious: things that cause agitation and look like hyperactive delirium, things that cause reduced responsiveness and look like hypoactive delirium, dangerous mimics you must not miss, and the extremes of normal behaviour in hospital. [10]
Pain is the most important mimic and co-traveller — an agitated child in pain can look delirious, and a child in pain can become delirious. Untreated pain is both a differential and a cause, which is why the ABCDEF bundle starts with structured pain assessment and management. Other common mimics include anxiety, fear, and sleep deprivation, each of which can produce agitation or withdrawal that overlaps with delirium. [1] [9]
Substance or medication withdrawal — especially opioid or benzodiazepine withdrawal after prolonged ICU sedation — produces a clinical picture that is difficult to distinguish from delirium and often coexists with it. The management principle is the same: identify and treat the withdrawal alongside the delirium. [7] [10]
Agitation mimics
- Pain — always assess and treat first
- Anxiety, fear, sleep deprivation
- Opioid or benzodiazepine withdrawal
- Steroid-induced mood change
Reduced responsiveness mimics
- Sedation effect — over-sedated, not delirious
- Sleep (normal) vs pathological lethargy
- Post-ictal state
- Metabolic encephalopathy without delirium
Dangerous to miss
- CNS lesion — tumour, stroke, bleed
- Encephalitis or meningitis
- Non-convulsive status epilepticus
- Raised intracranial pressure
Psychiatric differentials
- Early-onset psychosis — less acute, less fluctuating
- Acute stress or dissociation
- Autistic meltdown or sensory overload
- Mania — sustained elevated mood, not fluctuating
The single most important principle in the differential is Traube and Silver's framing: identify delirium, then investigate the underlying aetiology. Delirium is the clinical syndrome; the cause is what you must find and treat. A positive screen is the start of the workup, not the end of thinking. [10]
Clinical & Bedside Assessment
The assessment has two parts: screen for delirium using a validated, age-appropriate tool, and investigate the underlying cause. The screening is structured and observational; the investigation is clinical and targeted. [2] [10]
The Cornell Assessment of Pediatric Delirium (CAPD) is the tool the 2022 SCCM PADIS guideline recommends for screening all PICU patients, including pre-verbal infants and intubated children. It is an observational, 8-item tool anchored in child development, takes about one minute to complete, and is scored on a simple scale. A score of 9 or above is a screen positive, triggering formal assessment and investigation. [2] [1]
The paediatric Confusion Assessment Method for the ICU (pCAM-ICU) is validated for children aged 5 years and older who are awake enough to interact. It requires the child to participate in attention testing and is therefore not suitable for intubated, heavily sedated, or very young patients. The psCAM-ICU adapts it for the PICU environment. The original CAPD was designed specifically to fill the gap that pCAM-ICU cannot cover — the pre-verbal and deeply sedated child. [15] [2]
The bedside assessment must also include a structured mental state and neurological examination. Document the level of arousal (alert, drowsy, agitated, unresponsive), attention (can the child sustain and shift attention?), orientation (for school-age children), thought content and perception (any hallucinations, paranoia, or disorganisation), and a focused neurological exam looking for new focal deficits, pupillary asymmetry, or signs of raised intracranial pressure. [14] [10]
Crucially, the assessment is multi-informant: the bedside nurse who has cared for the child across shifts is often the person who notices the acute fluctuation first, because they know the child's baseline. Parent report that a child is not themselves is a powerful signal — families know their child's normal state, and an acute change reported by a parent must be taken seriously. [9] [3]
Investigations
There is no blood test for delirium. Investigations are about finding and treating the underlying cause, not confirming the syndrome. The approach is structured: identify delirium, then investigate for reversible contributors. [10]
The cause-finding workup after a positive screen
Review the chart for new or changed medications — benzodiazepines, anticholinergics, corticosteroids, opioids.
Check infection markers, cultures, and inflammatory markers — is there sepsis, a new infection, or a source?
Correct metabolic derangement — sodium, calcium, glucose, magnesium, renal and hepatic function, blood gas.
Assess oxygenation and perfusion — is there hypoxia, hypercapnia, or shock?
Review pain and withdrawal — is pain adequately treated? Is there iatrogenic withdrawal?
Consider neuroimaging (CT or MRI) for new focal neurology, seizures, deteriorating GCS, or unexplained delirium.
Consider EEG if non-convulsive status epilepticus is possible — especially in the neurologically injured child.
Routine neuroimaging is not required for every delirious child, but it is indicated for new focal neurological signs, a sudden drop in conscious level, seizures, a deteriorating or unexplained picture, or any clinical suspicion of raised intracranial pressure. An EEG is indicated when non-convulsive status epilepticus is in the differential — particularly in children with known epilepsy, traumatic brain injury, or post-anoxic injury. [14] [13]
The PODIUM consensus (2022) provides contemporary consensus definitions for acute neurological dysfunction in critically ill children, and reinforces that delirium is part of a spectrum of acute brain dysfunction that includes seizures, stroke, and encephalopathy — the assessment must consider all of these together, not just delirium in isolation. [13]
Management — Resuscitation
"Resuscitation" for delirium means safety and cause-finding first. Before you reach for a drug to modify behaviour, you must answer: is this child physiologically safe, and have I found and started treating the underlying cause? [1] [10]
The immediate response to a distressed, agitated child is environmental and physical safety first: ensure the child cannot harm themselves (one-to-one nursing, appropriate supervision, minimise lines and tubes that can be pulled), address reversible contributors urgently (treat pain, correct hypoxia, investigate infection), and avoid escalating sedation that will deepen the delirium and obscure the neurological exam. [1] [9]
Do not give a benzodiazepine to control the agitation of delirium unless you are treating a specific indication such as withdrawal or alcohol-related delirium — benzodiazepines are a causal risk factor for delirium in critically ill children, and escalating sedation to settle behaviour often worsens the underlying problem. [7] [1]
Management — Definitive & Stepwise
Once safety is secured and the cause is being investigated, definitive management is stepped and cause-first: the ABCDEF prevention and treatment bundle is first-line, non-pharmacologic priorities dominate, and antipsychotics are reserved for severe distress or safety risk after the bundle has failed. [1] [9]
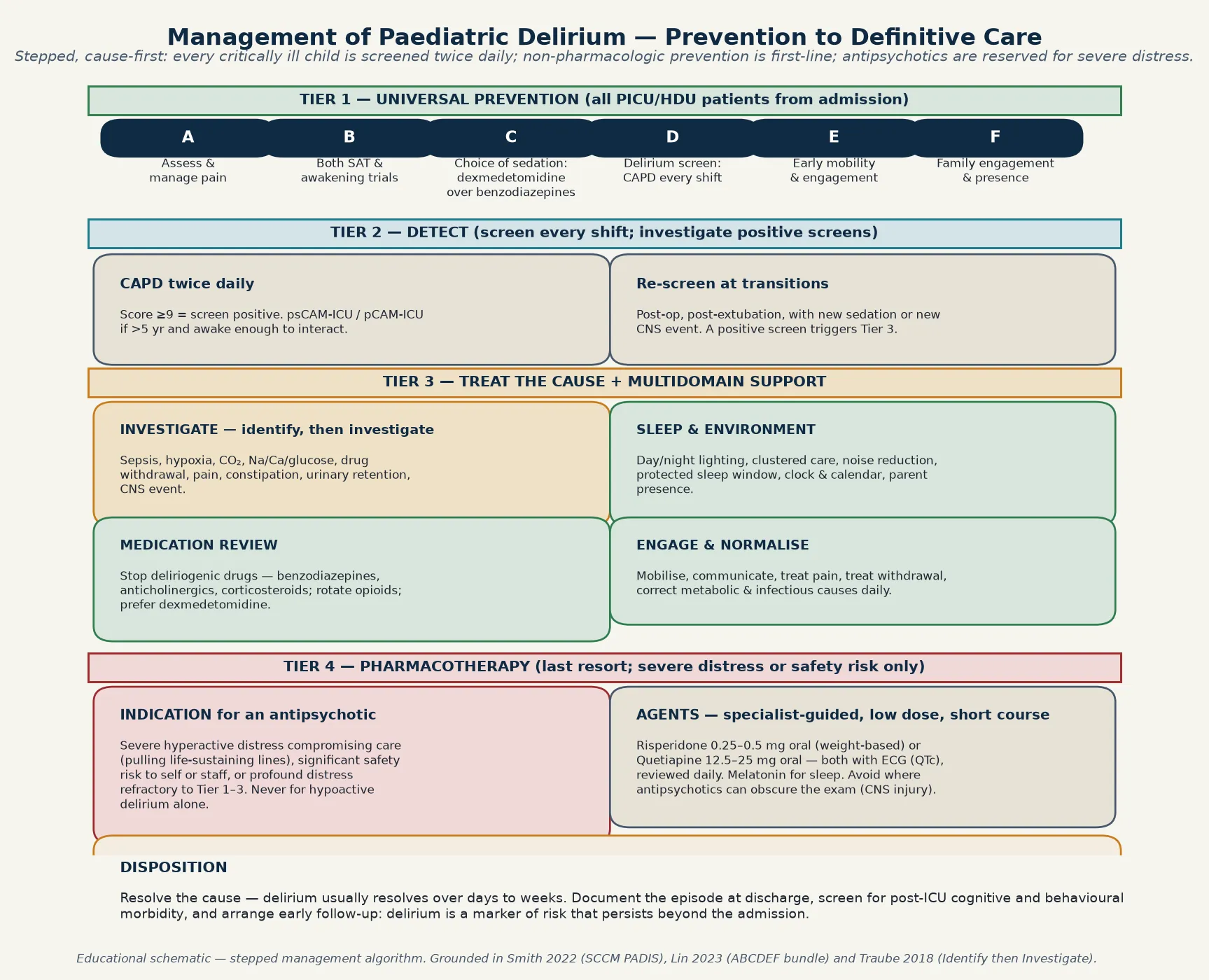
The ABCDEF bundle is the cornerstone of prevention and treatment, adapted from adult critical care for paediatric use. The 2023 Lin study of the paediatric ICU Liberation Bundle collaborative showed that structured application of the bundle is feasible and associated with improved outcomes in critically ill children. [9]
| Element | What it means at the bedside |
|---|---|
| A — Assess and manage pain | Use validated pain scores (FLACC, numeric); treat pain adequately — untreated pain both causes and worsens delirium |
| B — Both SAT and SBT | Spontaneous awakening trials and spontaneous breathing trials where clinically appropriate, to reduce over-sedation |
| C — Choice of sedation | Prefer dexmedetomidine over benzodiazepines; minimise anticholinergic and corticosteroid load |
| D — Delirium screening | CAPD at least twice daily on every PICU patient; investigate every positive screen |
| E — Early mobility | Mobilise, engage, and prevent immobility-associated morbidity as soon as clinically safe |
| F — Family engagement | Parent presence, day/night orientation, familiar objects, and structured communication |
Sedation choice is a modifiable risk factor you control today. The 2022 SCCM PADIS guideline recommends dexmedetomidine over benzodiazepines for sedation in critically ill children where feasible, based on the causal evidence linking benzodiazepines to delirium and the favourable profile of dexmedetomidine. Review the sedation plan daily, stop deliriogenic drugs where possible, and rotate opioids to avoid accumulation. [1] [7]
Sleep and environment are not soft extras — they are treatment. Restore the day–night cycle with lighting and clustered care, reduce noise at night, protect a sleep window, provide orientation cues (clock, calendar, familiar objects), and maximise parent presence. The ICU environment is itself deliriogenic, and modifying it is evidence-based prevention. [1] [9]
Smith 2022 — SCCM PADIS guideline (PMID 35119438)
Society of Critical Care Medicine clinical practice guideline (PADIS) for paediatric patients
Key finding
Recommends routine screening with validated tools (CAPD); the ABCDEF bundle; dexmedetomidine over benzodiazepines; and multidomain non-pharmacologic prevention as first-line. Antipsychotics are not recommended for routine prevention.
Practice change
Delirium prevention is built into the structure of PICU care, not added on when a screen turns positive.
Specific Subtypes & Scenarios
Post-cardiac surgery delirium is one of the highest-risk scenarios, with reported rates exceeding 50% in some cardiac ICU series. The drivers include cardiopulmonary bypass, hypothermia, haemodynamic instability, deep sedation, and the pre-existing developmental vulnerability of many cardiac patients. Screening must begin on the first postoperative day, and the ABCDEF bundle is applied from admission. [6] [4]
Delirium in children with cancer was quantified by Traube et al. in a prospective study of hospitalised oncology patients, which found a substantial incidence driven by the disease, chemotherapy, transplantation conditioning, infection, and the psychological load of isolation. The management principle is the same — identify, then investigate — but the differential is broader and the child is often immunocompromised, which changes the investigation strategy. [8]
Delirium in the neonatal unit is an emerging area. The clinical features in pre-verbal neonates — altered sleep–wake cycle, abnormal tone, reduced interaction — overlap with other neonatal neurological signs, and validated screening tools remain investigational. The principle of cause-finding still applies: sepsis, metabolic derangement, drug withdrawal, and intracranial pathology must all be considered and excluded. [3] [14]
Delirium after traumatic brain injury is part of a spectrum of acute neurological dysfunction that includes post-traumatic amnesia, agitation, and post-concussive symptoms. The assessment must consider seizures, raised ICP, and structural injury, and antipsychotics should be used cautiously because they can obscure the neurological exam and prolong recovery. [13] [14]
Complications & Pitfalls
The complications of paediatric delirium are substantial and measurable. Delirium is associated with longer PICU and hospital stay, more ventilator-days, higher cost, post-ICU cognitive and behavioural morbidity, and an association with mortality. The 2020 Silver study found that delirium during the PICU admission was associated with reduced quality of life after discharge — the harm extends beyond the admission. [6] [11]
The largest pitfall is under-recognition, especially of hypoactive delirium. A child who is quiet and apparently comfortable may be acutely delirious, and the failure to screen and investigate delays treatment of the underlying cause. Routine, structured, twice-daily CAPD screening is the intervention that closes this gap. [1] [5]
The opposite pitfall is over-sedation to control behaviour. When a delirious child is agitated, the instinct to give a sedative is strong — but benzodiazepines worsen delirium, deepen the level of arousal, and obscure the neurological exam. The correct response to agitation is cause-finding and environmental management, with antipsychotics reserved for severe distress that cannot be managed safely otherwise. [7] [1]
Under-recognition
- Missing hypoactive delirium — the 'quiet' child
- No routine CAPD screening on the unit
- Dismissing acute change as 'behavioural'
- Failing to investigate a positive screen
Over-sedation
- Escalating benzodiazepines for agitation
- Deepening arousal and obscuring the exam
- Worsening the causal pathway
- Missing the window to switch to dexmedetomidine
Premature antipsychotic
- Reaching for risperidone before cause-finding
- Not applying the ABCDEF bundle first
- Risking QTc prolongation without monitoring
- Obscuring neurological recovery in TBI
Single-screen reassurance
- One normal CAPD does not exclude delirium
- The course fluctuates — re-screen twice daily
- Missing the fluctuation that defines the syndrome
- Failing to involve the bedside nurse and family
When an antipsychotic is indicated for severe hyperactive distress that compromises care or poses a safety risk, the evidence base is limited but supports cautious use of low-dose risperidone or quetiapine with ECG monitoring for QTc prolongation, reviewed daily, and stopped as soon as the acute insult resolves. The Joyce retrospective review of quetiapine in critically ill children found it was used without major adverse effects in this population, but no drug is licensed for paediatric delirium prevention, and specialist guidance is essential. [12]
Prognosis & Disposition
Paediatric delirium is usually reversible over days to weeks once the underlying cause is identified and treated, but it is a marker of serious illness and the harm extends beyond the acute episode. The factors that predict a longer or more complicated course are greater severity of illness, pre-existing cognitive impairment, ongoing exposure to deliriogenic drugs, delayed recognition, and the cumulative burden of critical illness. [6] [11]
Disposition depends on the underlying cause and the child's recovery trajectory. Most delirium resolves in the PICU or ward as the acute illness is treated. The ABCDEF bundle should continue throughout the admission and into recovery, and the child should be screened at every transition — extubation, step-down from PICU to ward, and discharge. [9] [1]
The 2020 Silver study showing an association between delirium and reduced quality of life after discharge means that follow-up is part of the management plan, not an optional extra. Screen for post-ICU cognitive, behavioural, and emotional morbidity at follow-up, involve the family in recognising lingering effects, and coordinate with primary care and developmental services where needed. [11]
Special Populations
Pre-verbal infants and toddlers cannot tell you they are confused, so the clinical signs are behavioural and developmental: altered sleep–wake cycle, reduced eye contact, abnormal tone, inconsolable crying or abnormal quietness, and regression in developmental skills. The CAPD was designed specifically for this population, anchored in child development, and is the appropriate screening tool. [3] [2]
Children with complex chronic conditions and technology dependence — those with tracheostomies, long-term ventilation, feeding tubes, and neurodevelopmental disability — are among the highest-risk patients. Their baseline is often atypical, which makes acute change harder to detect, and they are frequently exposed to sedatives, anticholinergics, and repeated hospitalisations. Carer report of change from the child's normal state is essential. [4] [3]
Children with cancer and transplant recipients carry a particularly high burden of delirium, driven by the disease, chemotherapy, conditioning regimens, immunosuppression, infection, and the psychological load of isolation. The investigation strategy must account for immunocompromise, and the differential is broad. [8]
Indigenous and culturally diverse families may experience the PICU environment as additionally alienating, and the behavioural signs of delirium may be interpreted differently across cultural contexts. Engaging Indigenous health workers, using interpreters, and understanding the family's cultural framing of acute illness and altered mental state improves assessment and care. Rural and remote children who require retrieval to a tertiary PICU are separated from family and country, which adds to the deliriogenic load of the environment. [9] [3]
Evidence, Guidelines & Regional Differences
The syndrome is global, but the screening tools, care bundles, and service models are regional. Name the guideline you are quoting and carry the differences explicitly in the exam. [1] [5]
| Region | Screening standard | Sedation preference | Bundle and prevention |
|---|---|---|---|
| ANZ | CAPD twice daily in PICU | Dexmedetomidine over benzodiazepines | ABCDEF bundle; structured ICU liberation |
| UK (RCPCH / NHS) | CAPD or psCAM-ICU in PICU | Minimise benzodiazepines; protocolised sedation | Sedation holds, sleep protection, family-centred care |
| US (SCCM PADIS) | CAPD for all PICU ages; pCAM-ICU ≥5 yr | Dexmedetomidine preferred (SCCM 2022) | PADIS guideline ABCDEF bundle with early mobility |
| Canada / RCPSC | CAPD; unit-level screening protocols | Protocolised sedation; minimise benzos | Shared critical care; ABCDEF adaptation |
The evidence backbone is a set of studies you should be able to name. The 2022 SCCM PADIS guideline (Smith et al.) is the definitive practice guideline for paediatric delirium in critical care. The Ista 2023 systematic review and meta-analysis is the definitive synthesis of risk factors. The Traube 2014 CAPD validation established the screening tool. The Mody 2018 study established the causal link between benzodiazepines and delirium. The Lin 2023 study demonstrated the feasibility and value of the paediatric ABCDEF bundle. [1] [4] [7] [9]
The live controversy is not whether to screen — that is settled — but how far to push pharmacotherapy. The evidence for antipsychotics in paediatric delirium is limited to retrospective series and extrapolation from adult practice; no drug is licensed for paediatric delirium prevention, and the SCCM guideline does not recommend routine pharmacological prevention. The consensus is cause-first, bundle-first management, with antipsychotics reserved for the narrow indication of severe distress or safety risk. [1] [12]
Exam Pearls
The child who fluctuates between lucid and confused over hours has delirium until proven otherwise — the fluctuation is the signature, and a single normal assessment never excludes it. Re-screen at least twice daily, involve the bedside nurse and the family, and never let a positive screen sit without investigation. [2] [10]
When the examiner asks what you will do for a PICU patient who screens positive for delirium, the answer is not "start risperidone" — it is "identify delirium, then investigate the underlying cause, apply the ABCDEF bundle, prefer dexmedetomidine over benzodiazepines, and reserve an antipsychotic for severe distress or safety risk after non-pharmacologic measures have failed." That is the fellowship answer. [1] [9]
References
- [1]Smith HAB, Besunder JB, Betters KA, et al. 2022 Society of Critical Care Medicine Clinical Practice Guidelines on Prevention and Management of Pain, Agitation, Neuromuscular Blockade, and Delirium in Critically Ill Pediatric Patients With Consideration of the ICU Environment and Early Mobility. Pediatr Crit Care Med, 2022.PMID 35119438
- [2]Traube C, Silver G, Kearney J, et al. Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the PICU*. Crit Care Med, 2014.PMID 24145848
- [3]Silver G, Kearney J, Traube C, et al. Delirium screening anchored in child development: The Cornell Assessment for Pediatric Delirium. Palliat Support Care, 2015.PMID 25127028
- [4]Ista E, Traube C, de Neef M, et al. Factors Associated With Delirium in Children: A Systematic Review and Meta-Analysis. Pediatr Crit Care Med, 2023.PMID 36790201
- [5]Dechnik A, Traube C, et al. Delirium in hospitalised children. Lancet Child Adolesc Health, 2020.PMID 32087768
- [6]Siegel EJ, Traube C, et al. Pediatric delirium: epidemiology and outcomes. Curr Opin Pediatr, 2020.PMID 33105274
- [7]Mody K, Kaur S, Mauer EA, et al. Benzodiazepines and Development of Delirium in Critically Ill Children: Estimating the Causal Effect. Crit Care Med, 2018.PMID 29727363
- [8]Traube C, Ariagno S, Thau F, et al. Delirium in Hospitalized Children with Cancer: Incidence and Associated Risk Factors. J Pediatr, 2017.PMID 29173309
- [9]Lin JC, Srivastava A, Malone S, et al. Caring for Critically Ill Children With the ICU Liberation Bundle (ABCDEF): Results of the Pediatric Collaborative. Pediatr Crit Care Med, 2023.PMID 37125798
- [10]Traube C, Silver G, et al. Identify Delirium, Then Investigate for Underlying Etiology. Pediatr Crit Care Med, 2018.PMID 29303899
- [11]Silver G, Doyle H, Hegel E, et al. Association Between Pediatric Delirium and Quality of Life After Discharge. Crit Care Med, 2020.PMID 33031144
- [12]Joyce C, Witcher R, Herrup E, et al. Evaluation of the Safety of Quetiapine in Treating Delirium in Critically Ill Children: A Retrospective Review. J Child Adolesc Psychopharmacol, 2015.PMID 26469214
- [13]Wainwright MS, Guilliams K, Kannan S, et al. Acute Neurologic Dysfunction in Critically Ill Children: The PODIUM Consensus Conference. Pediatrics, 2022.PMID 34970681
- [14]Brown KL, Agrawal S, Kirschen MP, et al. The brain in pediatric critical care: unique aspects of assessment, monitoring, investigations, and follow-up. Intensive Care Med, 2022.PMID 35445823
- [15]Smith HA, Boyd J, Fuchs DC, et al. Diagnosing delirium in critically ill children: Validity and reliability of the Pediatric Confusion Assessment Method for the Intensive Care Unit. Crit Care Med, 2011.PMID 20959783