Paeds · mental-behavioural-and-psychosomatic
Substance intoxication, withdrawal and use disorders in youth
Also known as Adolescent substance use disorder · Youth alcohol and other drug use · Cannabis use disorder in adolescents · Adolescent intoxication and withdrawal · Vaping and nicotine dependence in youth · Polysubstance use in adolescents
Fellowship guide to substance intoxication, withdrawal and use disorders in youth: separating the acute (intoxication, withdrawal) from the clinical diagnosis (DSM-5 use disorder), CRAFFT and S2BI screening, SBIRT stepped care with motivational interviewing, CBT and family-based therapy, the Dennis Cannabis Youth Treatment evidence and the Marsch buprenorphine trial, the cannabis-psychosis link, and the Australian context of cannabis, vaping and inhalant (chroming) use.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the fifteen-year-old brought to the emergency department agitated and smelling of cannabis, or the fourteen-year-old whose school has noticed a slide in grades, withdrawal from friends and a new vagueness about where evenings go. These are the two faces of youth substance use that the fellowship exam wants you to hold together: the acute medical state and the slowly-building clinical disorder. [4] [13]
The first move is to separate three related but distinct problems. Intoxication is the acute, time-limited effect of a drug on the body and mind. Withdrawal is the physiological syndrome that appears when a dependent brain is deprived of the drug. A substance use disorder is the persistent, maladaptive pattern of use that causes clinically significant impairment or distress. A young person can be intoxicated without having a disorder, can have a severe disorder without being intoxicated right now, and can be in withdrawal while meeting no other criteria — and the management of each is different. [1] [4]
The three things you must separate
A substance use disorder is not defined by how much a young person uses, nor by a positive drug screen. It is defined by loss of control, social harm, risky use and pharmacological change — the same DSM-5 framework used in adults, but read through the lens of a still-developing brain, an age of heightened reward-seeking, and a clinical picture that is usually hidden, denied and wrapped around comorbidity. [1]
Classification
The DSM-5 swept away the old abuse-versus-dependence split and replaced it with a single dimension of severity. A substance use disorder is present when two or more of eleven criteria are met within a twelve-month period, drawn from four clusters: impaired control (using more or longer than intended, failed efforts to cut down, craving, time spent), social impairment (role failure, continued use despite problems, giving up activities), risky use (use in hazardous situations, continued use despite physical or psychological harm), and pharmacological change (tolerance and withdrawal). [1]
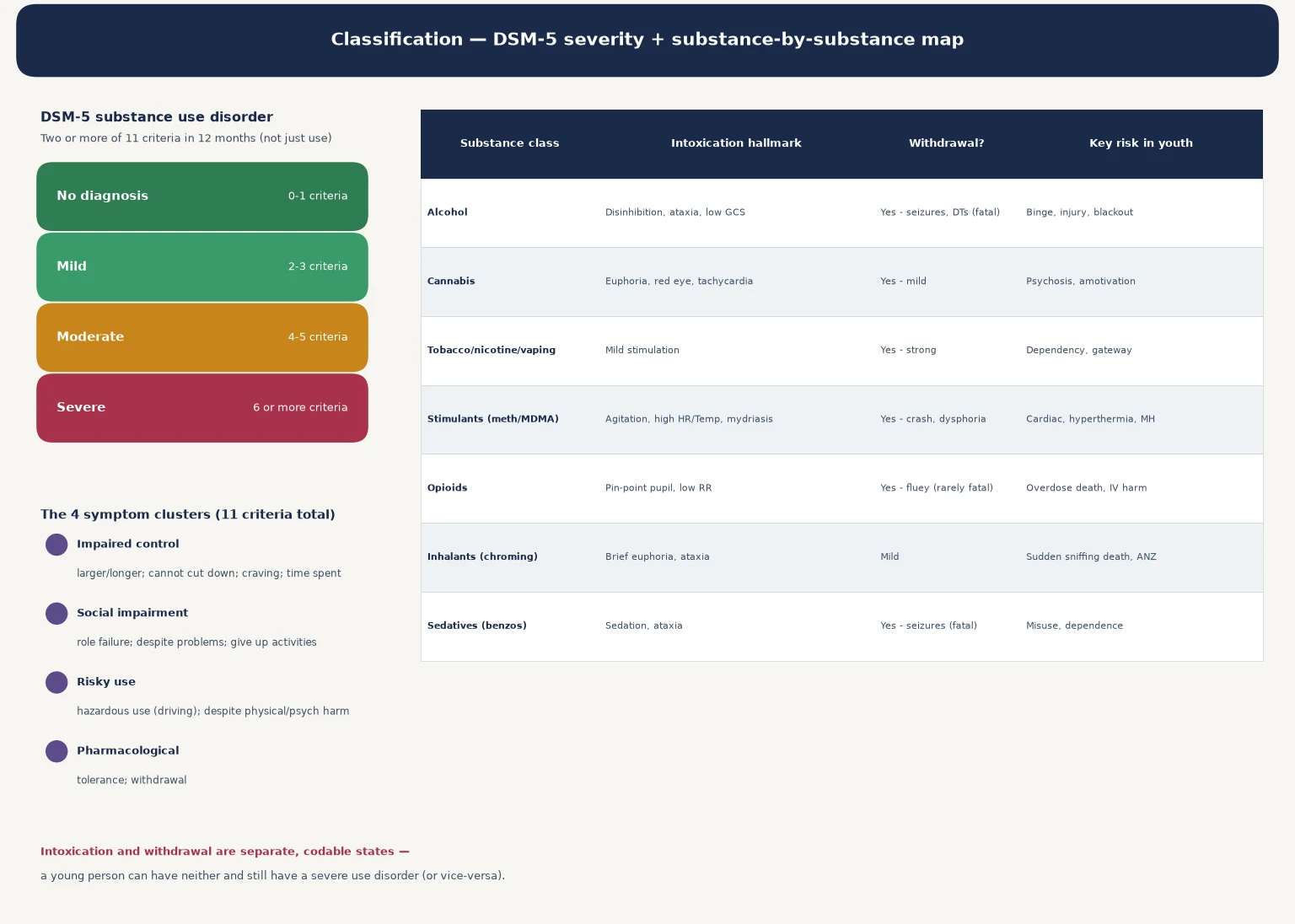
The severity follows the count: mild is two or three criteria, moderate is four or five, and severe is six or more. This matters because it drives the intensity of treatment. Tolerance and withdrawal are included but with a caveat — they do not count if the young person is taking the substance under medical supervision, which is why caffeine is dropped and why prescribed stimulant use for ADHD is not, of itself, a use disorder. [1]
Mild (2-3)
Brief intervention usually enough
- Impaired control or mild social impact
- SBIRT brief intervention and MI
- Re-screen and monitor
- Address risk context and comorbidity
Moderate (4-5)
Specialist youth AOD input
- Multiple criteria across clusters
- Structured psychosocial therapy
- Family involvement and harm reduction
- Treat comorbidity actively
Severe (6+)
Multidisciplinary specialist care
- Marked loss of control and harm
- Intensive therapy; MAT for opioid
- Consider supported withdrawal
- Relapse-prevention and recovery planning
Intoxication / withdrawal
Separate codable states
- Acute drug effect or cessation syndrome
- Treat medically first
- Neither equals a use disorder alone
- But often coexist with one
Intoxication and withdrawal are separately codable states in DSM-5, each specific to the substance. This is the point examiners press: a young person in the emergency department with alcohol intoxication does not thereby have an alcohol use disorder, and a young person with cannabis withdrawal may or may not meet the full disorder criteria. Diagnose each on its own grounds. [1]
Epidemiology & Risk Factors
Substance use is one of the commonest risk behaviours of adolescence, and cannabis use disorder is the leading substance use disorder presenting to youth services in Australia and New Zealand. In the Australasian cohorts, weekly or earlier-onset cannabis use tracks with the worst young-adult outcomes, and the integrative analysis by Silins and colleagues linked heavier adolescent use to lower educational completion, greater welfare dependence, suicide attempts and cannabis and other-drug dependence in young adulthood. [5] [13]
The age of first use matters disproportionately. A brain still undergoing prefrontal myelination is more vulnerable to the neuroadaptive and motivational effects of drugs, so the earlier the onset, the greater the later risk of dependence, mental-ill-health and educational harm. Cannabis dominates the clinical picture in ANZ, alcohol remains a major contributor to acute harm and injury, and vaping and nicotine use have risen sharply in school-aged young people. [5] [8]
Risk is not evenly distributed. Looked-after children, justice-involved young people, those who have experienced abuse or family violence, and Aboriginal, Torres Strait Islander, Māori and Pacific young people carry elevated rates driven by adversity, dispossession, intergenerational trauma and inequitable access to safe services rather than by identity itself. [4]
Pathophysiology
The reason adolescence is the peak window of onset is written into the timetable of brain development. The reward circuit — the mesolimbic dopamine pathway running from the ventral tegmental area to the nucleus accumbens — matures before the prefrontal cortex that is supposed to brake it. The result is a brain primed for novelty, sensation and reward, but with a weak top-down brake on impulse. [4]
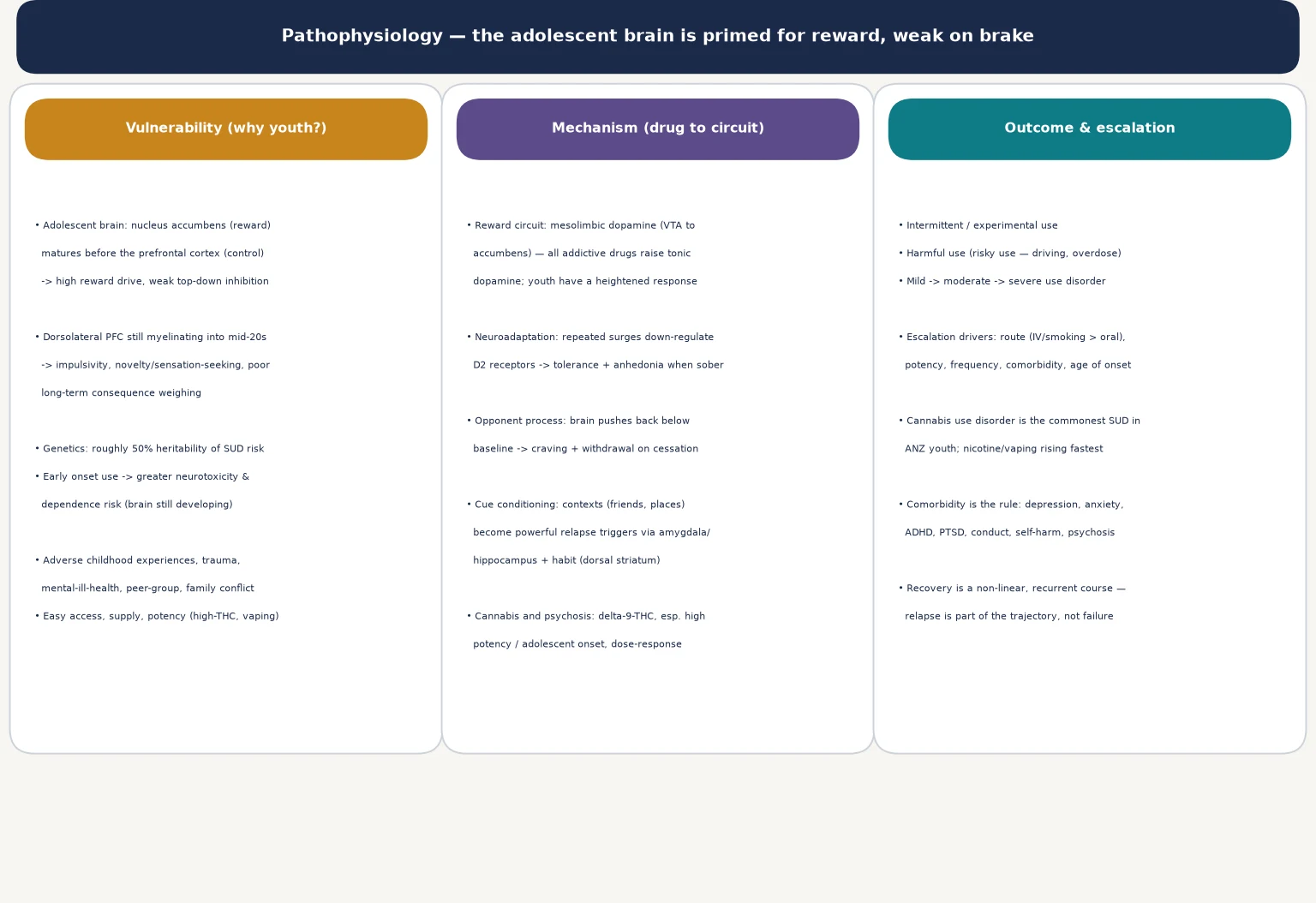
Every drug of misuse ultimately raises tonic dopamine in the nucleus accumbens, and the adolescent reward system responds more intensely than the adult one. Repeated surges down-regulate dopamine D2 receptors, which is the cellular story behind tolerance and the flat, anhedonic state many heavy users describe when sober. The brain then pushes back below baseline — the opponent process — so that the drug is no longer taken for pleasure but to relieve the dysphoria and craving of its absence. [4]
Cue conditioning is what makes relapse so context-dependent. The people, places and paraphernalia around use become powerful triggers through the amygdala, hippocampus and the dorsal striatal habit system, which is why a young person can be abstinent for months and relapse on returning to the same peer group or neighbourhood. Understanding this is what lets clinicians frame relapse as part of a chronic, relapsing course rather than as a personal failure. [4]
The cannabis-and-psychosis question is the one examiners return to. The systematic review by Moore and colleagues found a dose-response relationship between earlier and heavier cannabis use and later psychotic outcomes, and the Hall and Degenhardt review set out the clinical and epidemiological case in the Australian context. The relationship is not deterministic, but high-potency, early-onset use in a vulnerable young person raises the risk of a psychotic disorder in a way that is biologically plausible and clinically actionable. [2] [8]
Clinical Presentation
The acute presentations are the ones that bring young people to the emergency department, and each substance has a signature. Alcohol intoxication shows disinhibition, slurred speech, ataxia and a falling conscious level. Cannabis intoxication brings euphoria, conjunctival injection, tachycardia, increased appetite and sometimes anxiety or a paranoid edge. Stimulant intoxication (methamphetamine, cocaine, MDMA) produces agitation, mydriasis, tachycardia, hypertension and hyperthermia. Opioid intoxication is the triad of pin-point pupils, reduced respiratory rate and falling consciousness. Inhalant intoxication gives a brief euphoria and ataxia that can terminate suddenly in a fatal arrhythmia — sudden sniffing death. [4]
| Drug class | Intoxication — look for | Withdrawal — expect | Key youth risk |
|---|---|---|---|
| Alcohol | Disinhibition, ataxia, low GCS | Tremor, seizures, delirium tremens (can be fatal) | Binge drinking, injury, blackout, overdose |
| Cannabis | Euphoria, red eye, tachycardia, anxiety | Irritability, insomnia, appetite loss | Psychosis, amotivation, educational decline |
| Nicotine / vaping | Mild stimulation | Strong craving, irritability, poor concentration | Rapid dependence, gateway, lung injury |
| Stimulants (meth, MDMA) | Agitation, mydriasis, heat, hypertension | Hypersomnia, dysphoria, anhedonia | Cardiac, hyperthermia, serotonin toxicity |
| Opioids | Pin-point pupils, low respiratory rate, low GCS | Fluey, myalgia, piloerection, distress | Overdose death, injection-related harm |
| Inhalants (chroming) | Brief euphoria, ataxia, slurred speech | Mild irritability and craving | Sudden sniffing death, ANZ relevance |
| Sedatives (benzodiazepines) | Sedation, ataxia, disinhibition | Rebound anxiety, seizures (can be fatal) | Misuse, dependence, polysubstance overdose |
The use disorder itself is usually hidden. What surfaces in clinic is functional decline: dropping grades, school refusal or exclusion, withdrawal from family, new and risky peer associations, money problems, theft, changes in sleep, mood and appetite, and deteriorating mental health. The family often notices the trajectory before the young person acknowledges any use, and the young person may minimise or deny it out of shame, fear of consequences, or genuine lack of insight. [13]
Cannabis withdrawal is real and clinically important. Vandrey and colleagues documented a withdrawal syndrome in adolescent treatment seekers characterised by irritability, anxiety, sleep difficulty and appetite disturbance, which clinicians used to dismiss because it is milder than opioid or alcohol withdrawal. Recognising it matters because it drives relapse and because it responds to psychosocial and symptomatic management. [6]
Differential Diagnosis
Build the differential so you do not anchor on the obvious drug. The first pile is comorbid primary mental illness: depression, anxiety, bipolar disorder, post-traumatic stress, attention-deficit hyperactivity disorder and emerging psychosis can both drive and be driven by substance use, and untangling which came first is often impossible and sometimes beside the point — both need treating. [4] [8]
The second pile is organic mimics of intoxication or withdrawal. Encephalitis, head injury, hypoglycaemia, sepsis, hyponatraemia, a postictal state and prescribed or over-the-counter medication effects can all look like intoxication or withdrawal. A toxidrome pattern narrows the field, but never assume a positive drug screen excludes another diagnosis — a drunk young person can still have a subdural haematoma. [4]
Comorbid mental illness
- Depression, anxiety, bipolar, PTSD, ADHD
- Psychosis — primary or substance-induced
- Conduct disorder and family conflict
- Treat both — neither explains the other away
Organic mimics
- Head injury, encephalitis, hypoglycaemia
- Sepsis, hyponatraemia, postictal state
- Medication or overdose effects
- A tox screen does not exclude these
Trauma and safeguarding
- Abuse, neglect, family violence
- Exploitation, trafficking, coercion
- Out-of-home-care instability
- Use can be a coping or survival response
Behavioural variants
- Experimental use without a disorder
- Risk-taking without dependence
- Adolescent rebellion
- Distinguish on DSM-5 criteria, not morals
The question examiners love is whether a young person's psychotic symptoms are substance-induced or primary. The practical answer is to treat the acute state, observe as the drug clears, and reassess: substance-induced psychosis settles as intoxication resolves, whereas a primary psychotic disorder persists and declares itself. Cannabis and stimulants can both precipitate psychosis, and persistent symptoms after a documented washout period point to an independent disorder needing ongoing mental-health care. [2] [8]
Clinical & Bedside Assessment
The assessment is a structured, confidential interview using a psychosocial framework such as HEEADSSS, layered with a validated substance-use screen. You interview the young person alone for the substance, risk and mental-health history, then bring in parents or carers for the developmental and functional story and the collateral they can see that the young person cannot. Confidentiality is framed around safety: what is shared, and the limits, are explained up front. [4]
CRAFFT
The CRAFFT screen is validated for adolescents and asks about alcohol and other drugs across six items that capture the consequences of use rather than the amount; two or more positive answers signal a likely problem and the need for a fuller assessment. The S2BI (Screening to Brief Intervention) uses single-question past-year frequency questions and efficiently stratifies no-use, lower-risk and likely-disorder groups. The AUDIT-C focusses on alcohol. Screens are decision aids, not diagnoses — a high score triggers a structured interview, not a label. [3] [4]
The substance-use history maps every drug used, the age of first use, the route (smoking, vaping, oral, intranasal, injection), frequency, quantity, setting, consequences and any prior attempts to stop. You ask directly about mental state, self-harm and suicide, abuse and exploitation, pregnancy and sexual health, driving, and the means of overdose or harm present at home. A structured mental state examination documents appearance, behaviour, speech, mood, thought content (including paranoia, hopelessness and suicidal ideation), perception, cognition and insight. [4]
Investigations
There is no blood test for a substance use disorder. Investigations serve two purposes: to characterise and exclude organic mimics in the acutely unwell young person, and to establish a safe baseline before withdrawal or pharmacotherapy. In a straightforward outpatient presentation with no red flags, focused testing is sufficient; you widen the net when the history or examination points elsewhere. [4]
A urine drug screen has a narrow and specific role. It detects recent exposure to classes of drug, not dependence, impairment or a use disorder, and it has false positives and negatives driven by timing, metabolism, adulteration and cross-reactivity. Used without consent or as a surveillance tool it destroys the therapeutic alliance; used with explanation as part of a shared assessment or a safety plan, it has a place. A tox screen never makes the diagnosis of a use disorder and never overrides the clinical history. [4]
Management — Resuscitation
Resuscitation means safety and the airway first, and in substance use that has a sharper edge than in most of adolescent medicine. The opioid-intoxicated young person with a reduced respiratory rate and pin-point pupils needs naloxone titrated to respiratory effort now — you do not wait for a confirmatory screen. Stimulant intoxication with hyperthermia and autonomic instability needs cooling, benzodiazepines for agitation and active management of blood pressure and arrhythmia. Alcohol or sedative withdrawal can be fatal and is treated as a medical emergency. [4]
Alcohol and benzodiazepine withdrawal are the dangerous ones. They can produce seizures and delirium tremens and can kill, so they are managed with a symptom-triggered benzodiazepine taper (such as diazepam), thiamine to prevent Wernicke encephalopathy, fluid and electrolyte correction, and close monitoring. Opioid withdrawal is intensely distressing but rarely fatal on its own; it is managed with symptom relief, clonidine and, where appropriate and supervised, buprenorphine. Cannabis and nicotine withdrawal are brief and supportive. Stimulant withdrawal is largely a crash of hypersomnia and dysphoria managed with sleep, nutrition and mood support. [4]
Safety is wider than the medical: a young person who is intoxicated, dependent or being exploited is at risk of self-harm, overdose, injury, exploitation and blood-borne-virus exposure. Restrict access to means of overdose, involve carers within the bounds of confidentiality and safety, arrange a clearly named clinician for follow-up, and escalate to a safeguarding and child-protection response whenever exploitation, trafficking or coercion is suspected. [4]
Management — Definitive & Stepwise
Once safety is secured, treatment is stepped — the intensity matches the severity, and the young person and family are partners in the plan. The unifying framework is SBIRT: screening, brief intervention, and referral to treatment, applicable in primary care and able to escalate to specialist youth alcohol-and-other-drug services. [4]
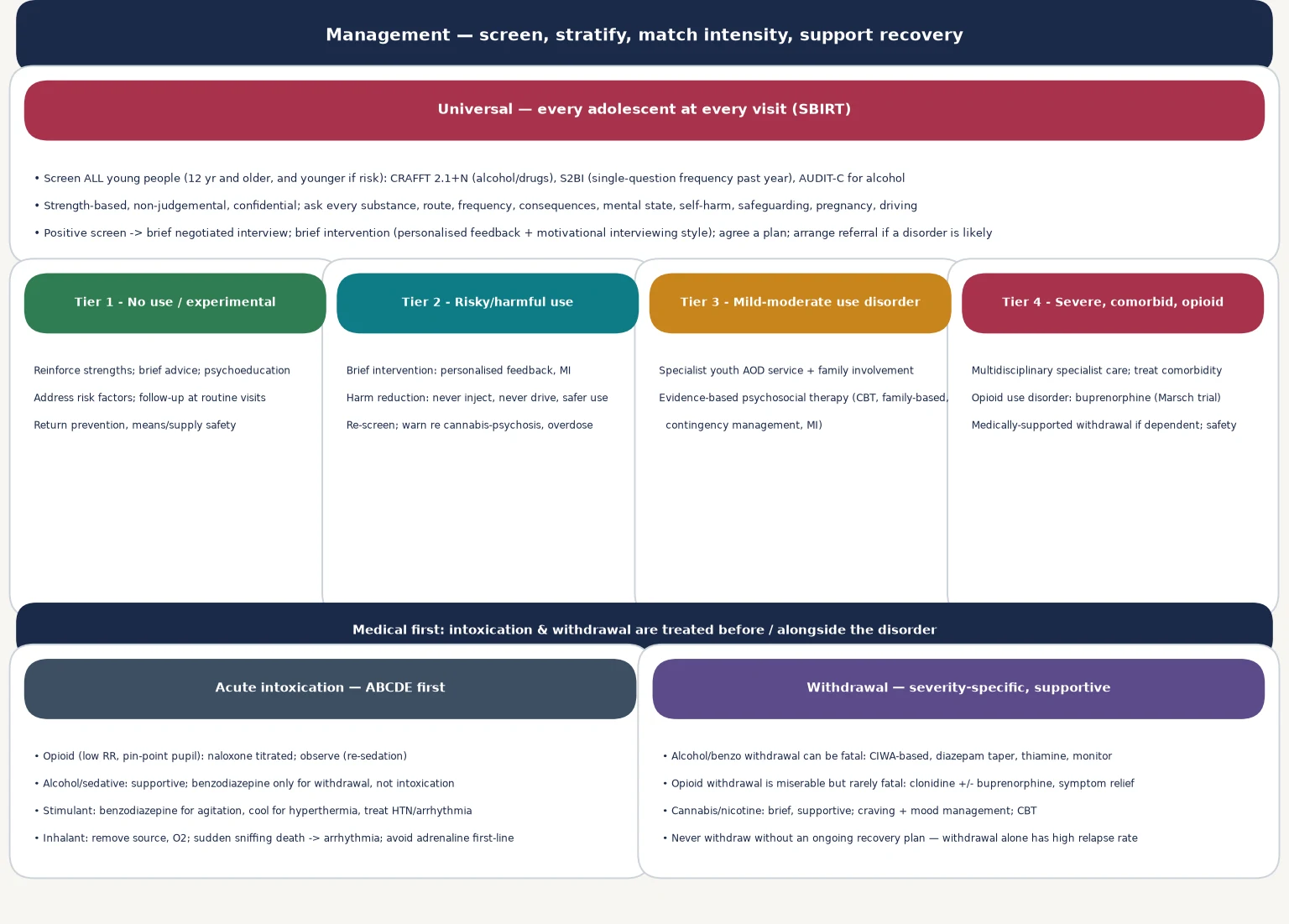
For risky or harmful use without a disorder, a brief intervention using motivational-interviewing principles — personalised feedback, exploring ambivalence, agreeing goals — is effective and is the core of what primary care delivers. It is strength-based, non-judgemental and brief, and it works because it meets the young person where they are rather than where the clinician thinks they should be. [4]
For a diagnosed use disorder, the evidence base is psychosocial. Waldron and Turner's review of evidence-based psychosocial treatments identified cognitive behavioural therapy, family-based therapy, motivational interviewing and contingency management as the approaches with the strongest support in adolescents. The Cannabis Youth Treatment (CYT) study by Dennis and colleagues showed that several brief, manualised interventions produced meaningful and lasting reductions in cannabis use among adolescents, and demonstrated that adolescent group treatment did not produce iatrogenic contagion — a fear that had kept clinicians from treating young people together. [7] [12] [9]
When the disorder is opioid use disorder — the buprenorphine pathway
Confirm opioid use disorder on DSM-5 criteria and exclude acute intoxication requiring medical stabilisation; assess comorbidity and safeguarding.
Engage the young person and family with motivational interviewing; explain medication-assisted treatment as evidence-based, not a substitute addiction.
Initiate buprenorphine during early withdrawal to avoid precipitated withdrawal; supervise the first dose.
Stabilise on a maintenance dose alongside psychosocial therapy and address comorbidity, housing, education and family.
Agree a maintenance duration tailored to the individual; if a taper is pursued, do it slowly and with sustained support.
Provide naloxone take-home and overdose-prevention education to the young person and carers regardless of the plan.
For opioid use disorder, medication-assisted treatment with buprenorphine is evidence-based and underused in adolescents. The Marsch randomised trial showed that a longer buprenorphine taper reduced illicit opioid use more than a short detoxification among opioid-dependent adolescents and young adults, and the Borodovsky review set out the rationale and safety of buprenorphine in this age group. Alongside medication, the young person needs psychosocial therapy, comorbidity care, take-home naloxone and overdose-prevention education. [10] [11]
Medically supported withdrawal has a defined but narrow place. Withdrawal on its own, without an ongoing recovery plan, has a high relapse rate, so it is offered as a gateway to treatment rather than as a standalone cure, and always with a clear follow-on plan for therapy, comorbidity and relapse-prevention. [4]
Specific Subtypes & Scenarios
Cannabis use disorder is the commonest presentation in ANZ youth. It is managed with motivational interviewing, CBT, family involvement and, for heavier use, contingency management; cannabis withdrawal is real and is addressed with sleep, mood and craving management. Counsel openly about the cannabis-psychosis risk, especially with early-onset, high-potency use. [5] [6]
Alcohol use and binge drinking drive acute harm through injury, overdose and blackout. Brief intervention in primary care works for risky use; a disorder needs structured therapy and family involvement. Alcohol withdrawal must be recognised and treated medically because it can be fatal. [4]
Opioid use disorder in a young person is a serious, potentially fatal but treatable condition. Engage with motivational interviewing, confirm the diagnosis, exclude acute intoxication, and offer buprenorphine within a specialist framework alongside psychosocial therapy, take-home naloxone and blood-borne-virus care. [10] [11]
Inhalant use (chroming, petrol and solvent sniffing) carries particular Australian relevance, including in remote Aboriginal communities where petrol sniffing caused lasting harm before low-aromatic Opal fuel was introduced. The acute risk is sudden sniffing death from a sensitised myocardium, so remove the source, give oxygen, and avoid adrenaline as a first-line agent where an alternative exists. [4]
Polysubstance use is the rule rather than the exception, and it complicates both intoxication and withdrawal. Map every substance, treat the most dangerous acute state first, and build the recovery plan around the whole pattern rather than a single drug. [4]
Complications & Pitfalls
The harms of untreated substance use are real and measurable: accidental overdose death (especially with opioids), injury, self-harm and suicide, blood-borne-virus exposure, educational failure and dropout, family breakdown, justice involvement, and the chronic relapsing course of the disorder itself. The cannabis-psychosis link is a complication that is both biologically plausible and clinically actionable. [2] [5]
Silins 2014 — Lancet Psychiatry (PMID 26360862)
Integrative analysis of three Australasian birth cohorts (n > 3700)
Key finding
Heavier and earlier adolescent cannabis use tracked with lower educational completion, greater welfare dependence, suicide attempts, and cannabis and other-drug dependence in young adulthood.
Practice change
Counsel young people and families on the dose-response harm of early, heavy cannabis use; the risk is population-level and clinically meaningful, not deterministic.
The pitfalls are mostly about framing. A punitive, moralising stance destroys the alliance and drives young people away from care. Over-reliance on a urine drug screen — either to make the diagnosis or to police behaviour — misrepresents the disorder and breaches trust. Missing the comorbidity (depression, anxiety, trauma, psychosis, ADHD) leaves the driving force untreated. And assuming that because the young person minimises their use it is not serious is a recurring and dangerous error. [4] [8]
A specific trap is failing to recognise alcohol or benzodiazepine withdrawal in a young person who presents to hospital for another reason. A young person admitted for an injury or an overdose can deteriorate into withdrawal, so take a withdrawal history from every young person who uses alcohol or sedatives and plan for it. [4]
Prognosis & Disposition
Substance use disorder is best understood as a chronic, relapsing condition with a non-linear recovery trajectory, much like depression or diabetes. Relapse is part of the course for many, and framing it as a learning point in a longer recovery — rather than as a failure — keeps young people engaged in care. Early, assertive, evidence-based treatment improves outcomes. [4] [12]
The factors that worsen prognosis are familiar: early age of onset, severity and chronicity, comorbid mental illness, family conflict and instability, ongoing trauma or exploitation, treatment dropout, and limited access to services. Engagement, the therapeutic alliance, and low-barrier, youth-friendly follow-up are therefore clinical priorities, not soft extras. [4]
Disposition is layered. Risky use without a disorder can be managed in primary care with brief intervention and re-screening. A mild to moderate use disorder needs specialist youth alcohol-and-other-drug input with structured psychosocial therapy. Severe, comorbid or opioid use disorder needs multidisciplinary specialist care, sometimes residential, with medication-assisted treatment and integrated mental-health support. A relapse-prevention and recovery plan — early-warning signs, the therapy that worked, the trusted clinician, and how to restart care — is written before discharge, and transition to adult services is planned in advance for older adolescents. [4]
Special Populations
Aboriginal, Torres Strait Islander, Māori and Pacific young people carry elevated rates of substance-related harm driven by colonisation, dispossession, intergenerational trauma, socioeconomic disadvantage and inequitable access to culturally safe care rather than by identity itself. Petrol sniffing and inhalant use in some remote communities prompted the introduction of low-aromatic Opal fuel as a structural intervention. Engagement is improved by Indigenous-led, culturally responsive, community-controlled models of care. [4]
Looked-after children and those in out-of-home care, trauma-exposed, refugee and asylum-seeker young people, and justice-involved youth have rates of substance use disorder far above the general adolescent population, often as a survival or coping response to adversity. Trauma-informed assessment and care are essential, and a substance-use intervention that ignores the trauma underneath will fail. [4]
Young people with neurodevelopmental disability, autism or ADHD may use substances to manage sensory overload, impulsivity or social anxiety, and need assessment and therapy adapted to their communication and cognitive profile. LGBTQI+ and gender-diverse young people face elevated rates of substance use driven by minority stress, and benefit from an affirming, non-judgemental service. Rural and remote youth often have thin access to youth alcohol-and-other-drug services, so telehealth, school-based programs and a clearly named local clinician matter disproportionately. [4]
Evidence, Guidelines & Regional Differences
The drugs, the services and the thresholds differ across regions, and the cannabis-and-psychosis debate is live everywhere. Name the guideline you are quoting and carry the regional differences explicitly. [2] [4]
| Region | Screening | First-line treatment | Service model |
|---|---|---|---|
| ANZ | CRAFFT, S2BI; headspace entry | SBIRT, MI, CBT, family therapy; buprenorphine for opioid | GP mental-health plans, headspace, youth AOD services, CAMHS |
| UK (NICE) | Targeted screening of vulnerable groups | Psychosocial interventions first | NHS CAMHS / young people's substance misuse services |
| US (AAP SBIRT) | Universal SBIRT in primary care | Brief intervention; CBT, family-based, CM; buprenorphine | Primary-care-initiated with specialist collaboration |
| Canada / RCPSC | Routine adolescent screening | Psychosocial therapy; MAT for opioid | Shared youth mental-health and AOD care |
The evidence backbone is a set of trials and reviews you should be able to name. The Cannabis Youth Treatment (CYT) study by Dennis and colleagues established that brief, manualised, evidence-based interventions reduce cannabis use in adolescents, and its companion paper by Burleson, Kaminer and Dennis showed that adolescent group treatment did not cause iatrogenic contagion. The Waldron and Turner review identified the psychosocial treatments with the strongest evidence in adolescents. The Marsch trial demonstrated that a longer buprenorphine taper outperformed short detoxification in opioid-dependent adolescents and young adults, and the Borodovsky review made the case for buprenorphine in this age group. The Moore and Silins papers anchored the cannabis-and-psychosis and young-adult-outcomes evidence. [2] [5] [7] [9] [10] [11] [12]
The live controversy is not whether to treat, but how to balance harm reduction and recovery. Abstinence-only models that exclude young people who are not ready to stop fail the majority; the modern standard is meeting the young person where they are, reducing harm now, and building toward recovery over time. Cannabis legalisation in several jurisdictions has not removed the adolescent harm signal, and the clinical task — screen, assess, treat, and follow up — is unchanged. [2] [5]
Exam Pearls
The young person who minimises their use is the one whose comorbidity and safeguarding context you must dig hardest for; a strength-based, non-judgemental, confidential interview is both the ethical and the clinically effective stance. [4] [13]
When you cannot decide whether psychotic symptoms are substance-induced or primary, treat the acute state, observe as the drug clears, and reassess — persistent symptoms after a documented washout declare a primary disorder. [2] [8]
References
- [1]Hasin DS, O'Brien CP, Auriacombe M, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry, 2013.PMID 23903334
- [2]Moore THM, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet, 2007.PMID 17662880
- [3]Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G. Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Arch Pediatr Adolesc Med, 2002.PMID 12038895
- [4]Levy SJL, Williams JF, Committee on Substance Use and Prevention. Substance use screening, brief intervention, and referral to treatment. Pediatrics, 2016.PMID 27325634
- [5]Silins E, Horwood LJ, Patton GC, et al. Young adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychiatry, 2014.PMID 26360862
- [6]Vandrey R, Budney AJ, Kamon JL, Stanger C. Cannabis withdrawal in adolescent treatment seekers. Drug Alcohol Depend, 2005.PMID 15845324
- [7]Waldron HB, Turner CW. Evidence-based psychosocial treatments for adolescent substance abuse. J Clin Child Adolesc Psychol, 2008.PMID 18444060
- [8]Hall W, Degenhardt L. Cannabis use and psychosis: a review of clinical and epidemiological evidence. Aust N Z J Psychiatry, 2000.PMID 11185941
- [9]Burleson JA, Kaminer Y, Dennis ML. Absence of iatrogenic or contagion effects in adolescent group therapy: findings from the Cannabis Youth Treatment (CYT) study. Am J Addict, 2006.PMID 17182415
- [10]Marsch LA, Moore SK, Borodovsky JT, et al. A randomized controlled trial of buprenorphine taper duration among opioid-dependent adolescents and young adults. Addiction, 2016.PMID 26918564
- [11]Borodovsky JT, Levy S, Fishman M, Marsch LA. Buprenorphine treatment for adolescents and young adults with opioid use disorders: a narrative review. J Addict Med, 2018.PMID 29432333
- [12]Dennis M, Godley SH, Diamond G, et al. The Cannabis Youth Treatment (CYT) study: main findings from two randomized trials. J Subst Abuse Treat, 2004.PMID 15501373
- [13]Tims FM, Dennis ML, Hamilton N, et al. Characteristics and problems of 600 adolescent cannabis abusers in outpatient treatment. Addiction, 2002.PMID 12460128