Paeds · mental-behavioural-and-psychosomatic
Depressive disorders in children and adolescents
Also known as Paediatric depression · Adolescent depression · Major depressive disorder in youth · Youth depression · Depressive episode in children
Fellowship guide to depressive disorders in children and adolescents: criteria-based clinical diagnosis, irritability-and-school-failure presentation, suicide-risk assessment, stepped care with CBT or IPT-A and fluoxetine as first-line SSRI, the TADS/TORDIA/ADAPT/IMPACT evidence and Cipriani/Zhou network meta-analyses, the black-box warning used wisely, and ANZ/UK/US guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the fourteen-year-old who used to love football and now will not leave her room, whose marks have slid from A to D in a term, who snaps at everyone and tells no one she has started cutting her thighs. That cluster — mood, function and risk changing together — is what you are looking for, not a single sad mood on a clinic day. [10] [13]
A depressive disorder is a syndromal, impairing disturbance of mood and related cognition, body and function, not ordinary sadness and not a reaction in proportion to a small stressor. In young people the mood may be irritable rather than plainly sad, and the presentation is often carried by school decline, withdrawal, sleep and appetite change, or behaviour change rather than a verbal complaint of low mood. [10] [11]
Diagnosis remains clinical and criteria-based. Rating scales such as the PHQ-9 modified for adolescents (PHQ-A) or the Mood and Feelings Questionnaire support screening, severity grading and tracking — they do not make the diagnosis, and a single high score is never sufficient to start a drug. [15] [10]
Classification
depressive disorders sort into a small number of clinical shapes, and the shape changes what you do. The commonest in clinic is major depressive disorder (MDD), defined by a major depressive episode: at least five of nine symptom groups, including depressed or irritable mood or loss of interest, for most of the day nearly every day for at least two weeks, with impairment. [10] [11]
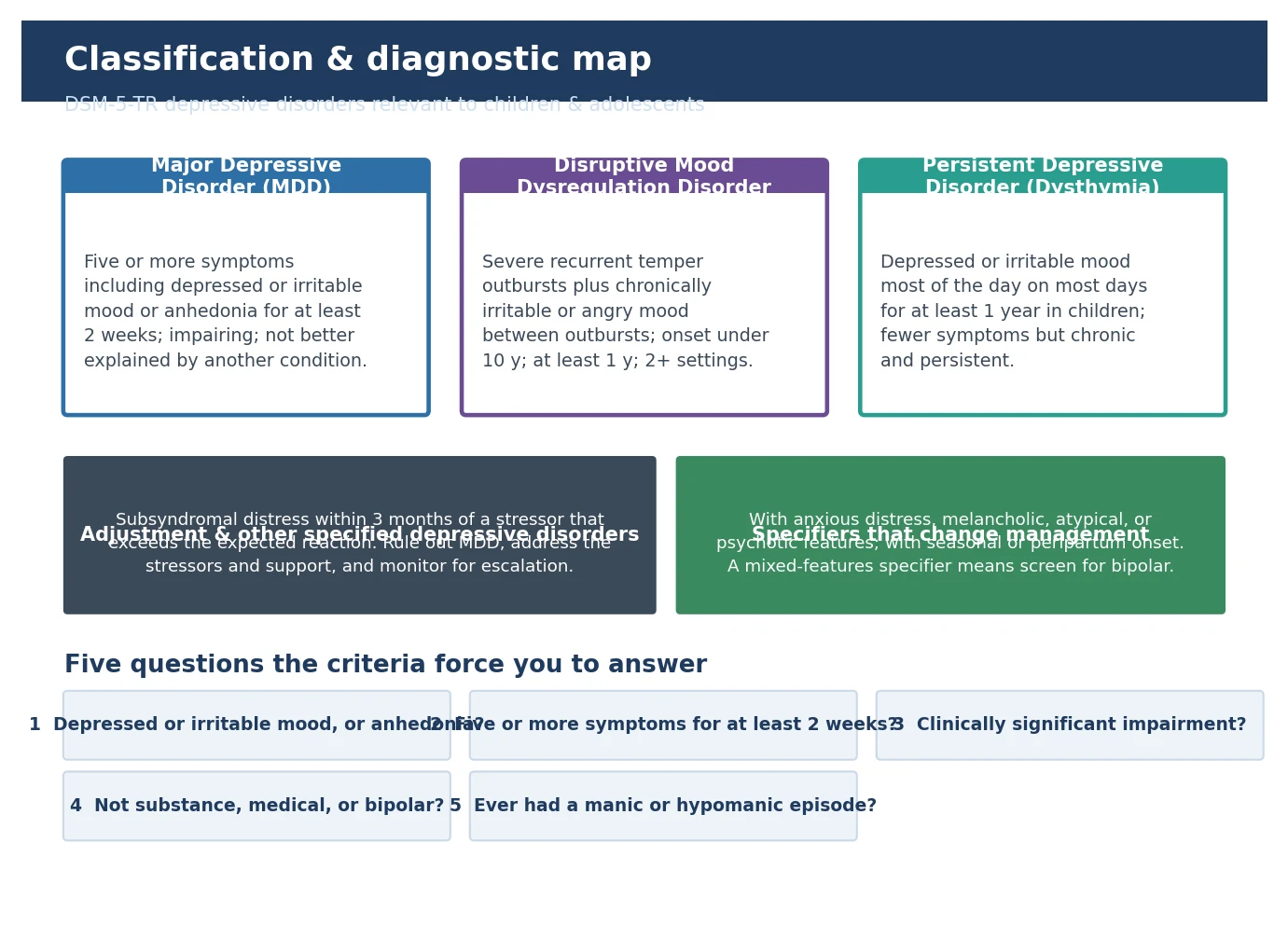
Persistent depressive disorder (dysthymia) runs a longer, lower-grade course — chronic depressed or irritable mood for at least one year in a child, with fewer symptoms than a major episode but persistent functional drag. Many young people eventually superimpose a major episode on this chronic base. [10]
Disruptive mood dysregulation disorder (DMDD) is the subtype built for the child with severe, frequent temper outbursts and a chronically irritable or angry mood between outbursts, starting before age ten and present across two or more settings for at least a year. It was created to stop the over-diagnosis of paediatric bipolar disorder, and its management is built around behaviour therapy, not antidepressants. [11]
Major depressive disorder
Episodic, at least 2 weeks
- Five or more symptoms including mood or anhedonia
- Acute functional impact at school and home
- First-line therapy plus fluoxetine if moderate to severe
- Recurrence is common; plan for relapse prevention
Persistent depressive disorder
Chronic, at least 1 year
- Lower-grade but persistent irritable or low mood
- Fewer symptoms but chronic functional drag
- Often underpins a later major episode (double depression)
- Long-term psychotherapy and support are central
DMDD
Chronic irritability + outbursts
- Onset before age 10; at least 1 year; 2+ settings
- Built to reduce bipolar overdiagnosis
- Behavioural therapy first; antidepressants not first-line
- Rule out trauma, anxiety, ADHD and bipolar
Adjustment / other specified
Stressor-related, subsyndromal
- Distress beyond expected within 3 months of a stressor
- Does not meet full major-episode criteria
- Address the stressor, support and monitor
- Watch for escalation to a major depressive episode
A useful set of specifiers changes management rather than naming a new disease: with anxious distress, melancholic features, atypical features, psychotic features, peripartum onset, or seasonal pattern. The one that must never be missed is the mixed-features specifier, which is your prompt to screen hard for bipolar disorder before reaching for an antidepressant. [11]
Epidemiology & Risk Factors
Depression is uncommon before puberty and then rises steeply, so that by late adolescence it is one of the commonest chronic conditions a young person carries. Community survey data put the lifetime prevalence of a mental disorder in US adolescents around half, with mood and anxiety disorders among the leading contributors. [13]
Headline numbers for viva
The female preponderance emerges at puberty, and the Cyranowski model explains it through the interaction of a rising sex-hormone surge, a still-maturing stress-regulation system, and the social and relational challenges that intensify for adolescent girls — together they tilt the stress response toward a depressive phenotype. [12]
Risk amplifiers cluster: family history of mood disorder (the strongest single risk), early adversity and trauma, chronic illness, comorbid anxiety or ADHD, bullying and peer victimisation, sleep disruption, substance use, and the minority stress carried by LGBTQI+ and gender-diverse young people. Poverty, racism, language barriers and rural isolation change both who becomes depressed and who reaches care. [11] [13]
Pathophysiology
There is no single broken circuit to name. The teaching model that best fits the evidence is biopsychosocial: a polygenic vulnerability meets a brain and body that is primed to over-react to stress, meets the specific stressors of adolescence, and a depressive episode emerges. [1] [12]
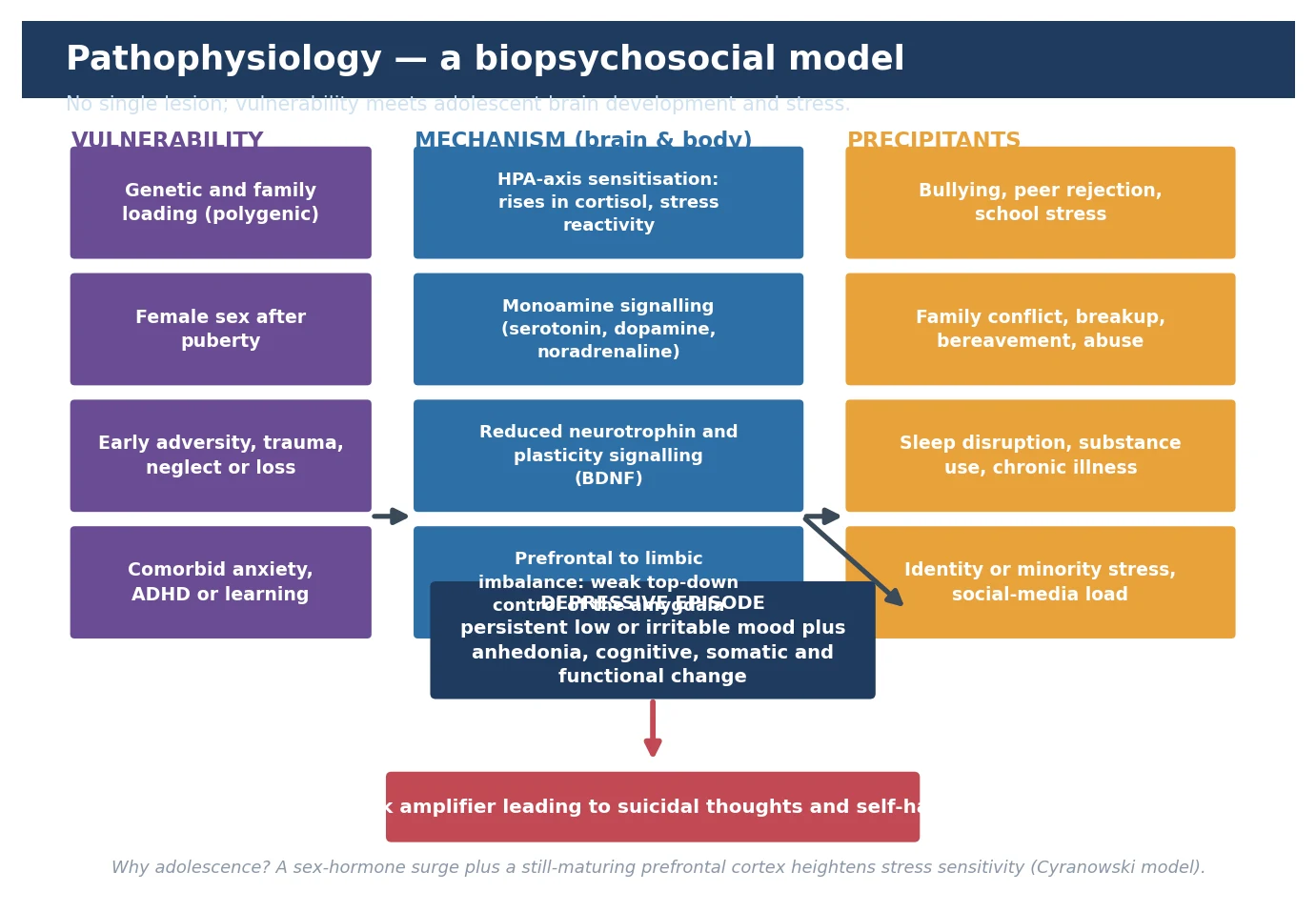
At the mechanism level, the useful threads are sensitisation of the hypothalamic-pituitary-adrenal (HPA) axis with heightened cortisol reactivity, altered monoamine signalling (serotonin, dopamine, noradrenaline — the thread that connects to why an SSRI can work), reduced neurotrophin and neuroplastic signalling such as brain-derived neurotrophic factor, and an imbalance between a still-developing prefrontal cortex and a more mature limbic system so that top-down control of the amygdala is weak. [1] [12]
This is why the question "isn't depression just low serotonin?" is a trap. The serotonin story is one strand of a much larger stress-response and plasticity model, and it explains both why a drug that increases serotonin signalling can help and why a drug alone is rarely the whole answer. [1]
Clinical Presentation
The child in front of you rarely says "I am depressed." You see it in function falling away: the bright student whose grades drop, the sociable child who stops seeing friends, the active child who gives up sport, the settled child who starts picking fights or harming themselves. The mood itself may be sad, flat or — especially in younger children and adolescents — frankly irritable. [10] [11]
| Presentation story | Do not stop here | Must still map |
|---|---|---|
| 'Just a grumpy teenager' | Irritability can be the mood of a major depressive episode in this age group | Duration, pervasiveness, impairment, suicide risk, bipolar screen |
| 'Tired all the time' | Fatigue and somatic complaints are common paediatric carriers | Sleep opportunity, anaemia, thyroid, substances, mood and anhedonia |
| 'School is the problem' | School decline is often the first functional sign | Multi-informant history, bullying, learning load, peer and home stressors |
| 'Cutting for attention' | Self-harm is a risk marker, never dismissed as manipulation | Full suicide and self-harm assessment, means restriction, safety plan |
| 'Sad since the breakup' | A stressor can precipitate, but check whether criteria are met | Five-symptom threshold, duration, impairment, risk |
Preschool depression is recognised but rare and must always prompt a search for organic, developmental, trauma or safeguarding causes. School-age children present with somatic complaints (headaches, abdominal pain), school refusal, behaviour change, irritability and regression. Adolescents look closer to the adult pattern: depressed mood, anhedonia, hopelessness, sleep and appetite disturbance, social withdrawal, declining performance, and risky behaviour or self-harm. [11]
The core symptoms cluster around the familiar SIGECAPS frame — Sleep change, loss of Interest, Guilt or worthlessness, loss of Energy, reduced Concentration, Appetite or weight change, Psychomotor change, and Suicidal thoughts — with the paediatric modifier that irritability can stand in for depressed mood. You still need at least five symptoms for at least two weeks, with at least one being depressed/irritable mood or anhedonia. [10] [11]
Differential Diagnosis
Build the differential in four piles so you do not anchor on the obvious: things that look like depression but are reversible, things that travel with depression, things that are dangerous to miss, and the normal extremes of mood. A thyroid disorder, iron-deficiency anaemia, chronic sleep deprivation, a medication or substance effect, or an underlying infection can each mimic a depressive episode, and several are quickly excluded with focused tests and a careful history. [10] [11]
Reversible mimics
- Hypothyroidism, anaemia, vitamin deficiency
- Severe sleep deprivation or delayed sleep phase
- Substance use, intoxication or withdrawal
- Medication effects (e.g. isotretinoin, corticosteroids)
Common co-travellers
- Anxiety disorders
- ADHD and specific learning disorder
- Autism and sensory differences
- Eating disorders and substance use
Dangerous to miss
- Bipolar depression — a past manic or hypomanic episode
- Psychotic disorder emerging
- Organic brain disease (tumour, encephalitis)
- Safeguarding: abuse, neglect, exploitation
Normal extremes
- Bereavement and acute grief
- Adjustment to a major stressor
- Adolescent moodiness that is brief and non-impairing
- Situational distress without syndromal change
The single most important screen before any antidepressant is for bipolar disorder: ask explicitly about any past period of elevated or irritable mood with decreased need for sleep, racing thoughts, grandiosity, and goal-directed overactivity lasting at least four to seven days. Giving an SSRI to a young person with undiagnosed bipolar depression can precipitate a mixed state, a manic switch, or an increase in suicidality. [11]
Distinguishing grief and bereavement from a depressive episode matters but is not always clean: grief comes in waves with preserved self-esteem and tends to centre on the loss, whereas depression is more pervasive, enduring and self-attacking, and grief that persists and deepens can itself become a treatable depressive episode. Separating DMDD (chronic irritability, not episodic) from MDD, anxiety and ODD relies on the chronic, cross-setting, non-episodic nature of the irritability. [11]
Clinical & Bedside Assessment
The assessment is a structured interview with multiple informants, not a score on a form. You need the young person alone for part of the interview (for confidentiality and to ask about risk directly), and the parents or carers for the developmental and functional history, plus school collateral where possible, because adolescents often under-report and parents often under-detect internalising symptoms. [10] [11]
SIGECAPS
The mental state examination documents appearance and behaviour, speech, mood (subjective and objective), thought form and content (hopelessness, worthlessness, suicidal and homicidal ideation, any psychotic or manic content), perception, cognition, insight and judgement. A flat or sad affect with hopelessness, psychomotor slowing, and expressed worthlessness raises both the probability of depression and the risk of self-harm. [10] [11]
You must ask about suicide directly. Asking does not increase risk. Ask about thoughts, then plans, then intent, then access to means, and weigh protective factors — family and peer connectedness, reasons for living, future orientation, and engagement with help. Frame the question without flinching: "When things feel this heavy, do you ever think about not being here any more, or about hurting yourself?" Document the risk assessment, the means present in the home, and the safety plan you agreed. [7] [11]
Rating scales have a defined supporting role. The PHQ-A (PHQ-9 modified for adolescents) and the Mood and Feelings Questionnaire are reasonable for adolescent screening and for tracking severity over time; they are not diagnostic. A score above the validated adolescent cut-point (for the PHQ-9, around 10 to 11) is a trigger for a full interview, not a prescription trigger on its own. [15]
Investigations
There is no blood test for depression. Investigations are about excluding mimics and establishing a safe baseline, not confirming the diagnosis. In a typical first presentation with no red flags, a focused screen is sufficient; you expand it when the history or examination points elsewhere. [10] [11]
Where relevant, screen for pregnancy and substance use, and consider a sexual-health and infection screen in sexually active adolescents. Record a baseline of height and weight (to detect SSRI-associated growth or weight change) and ask about cardiac symptoms and family history of arrhythmia or sudden death before prescribing, because a corrected QT-prolonging drug or an undiagnosed channelopathy changes your choice. [11]
Management — Resuscitation
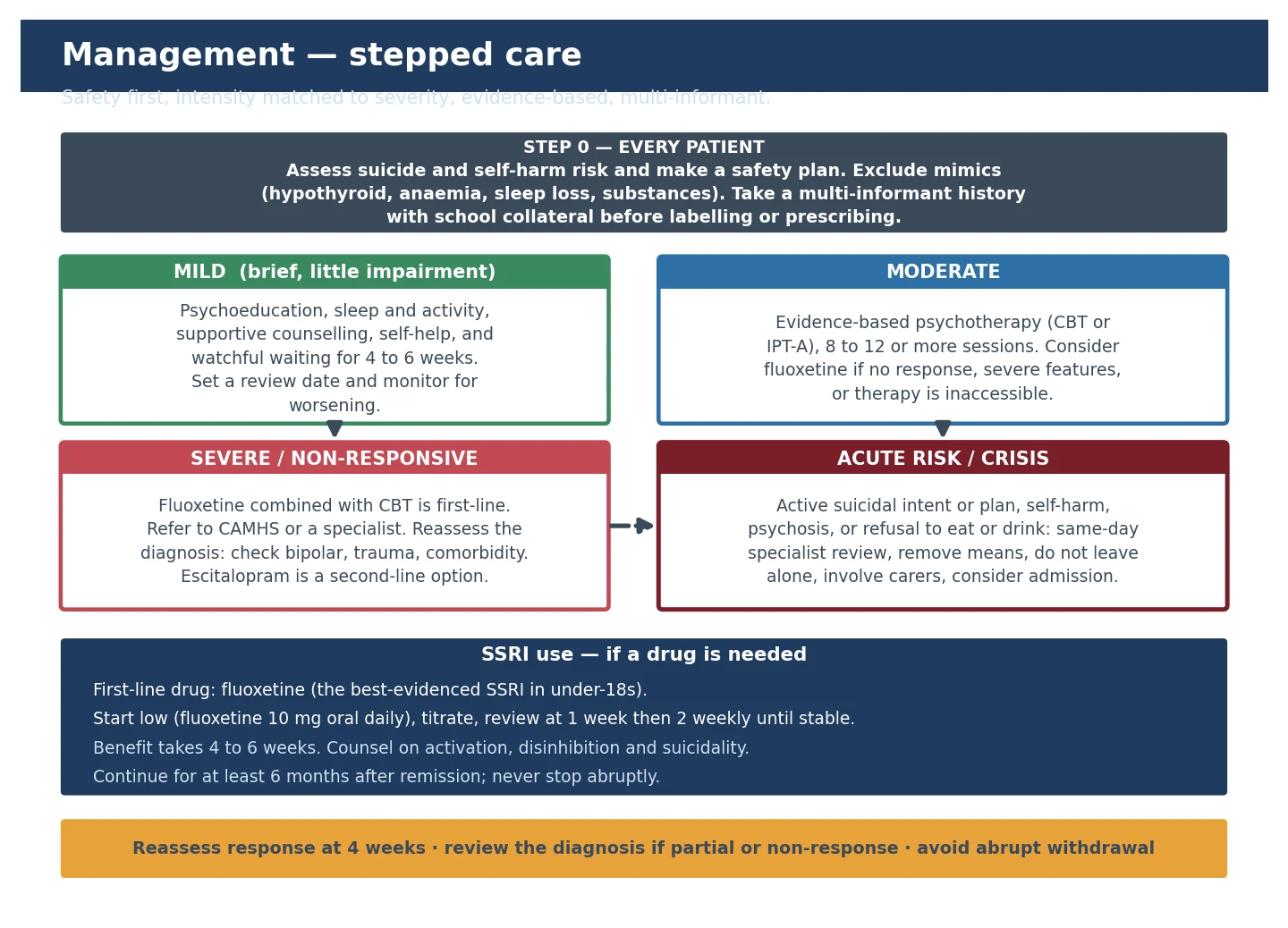
"Resuscitation" for a mood disorder means safety first. Before you discuss weeks of psychotherapy or titrate a drug, you must answer one question: is this young person safe between now and the next contact? Active suicidal ideation with a plan or intent, a recent serious self-harm act, psychotic features, or refusal to eat or drink are psychiatric emergencies. [7] [11]
The immediate bundle is a collaborative safety plan (written warning signs, internal coping, people and places that help, professional contacts, and means restriction), removal or securing of lethal means from the home, a clearly named clinician responsible for follow-up within days, and carer involvement appropriate to the young person's capacity and safety. Asking directly, documenting, and restricting means save lives. [7] [11]
Management — Definitive & Stepwise
Once safety is secured, treatment is stepped — the intensity matches the severity, and every plan is built around the young person and family, not imposed on them. Mild depression may be managed in primary care with psychoeducation, sleep and activity, supportive counselling and watchful waiting; moderate depression adds an evidence-based psychotherapy and considers an SSRI; severe, non-responsive or high-risk depression warrants specialist child and adolescent mental-health care, often combining fluoxetine with psychotherapy. [10] [11]
Psychotherapy is first-line for mild to moderate depression. Cognitive behavioural therapy (CBT), interpersonal psychotherapy for adolescents (IPT-A) and behavioural activation have the strongest randomised-trial evidence. The IMPACT trial found that CBT, short-term psychoanalytic psychotherapy and a brief psychosocial intervention were broadly comparable on average, which means the delivery of a competent, structured therapy matters more than the brand name. [6] [11]
When an SSRI is added — the start, review, decide cycle
Indication: moderate to severe depression, poor response to therapy, or therapy inaccessible — and bipolar and organic causes excluded.
Choose fluoxetine first (best benefit-risk in under-18s). Start low, e.g. fluoxetine 10 mg oral once daily.
Review at one week for tolerability, activation and suicidality, then roughly two weekly until stable.
Allow four to six weeks for full benefit before judging response; titrate within the licensed range if tolerated.
If partial or no response: check adherence and diagnosis, optimise the dose, then switch (e.g. to escitalopram) or combine with psychotherapy; refer for specialist care.
After remission, continue for at least six months, then withdraw gradually to avoid discontinuation symptoms.
When a drug is needed, fluoxetine is the first-line SSRI in under-18s because it is the one with the most favourable balance of efficacy and tolerability across the network meta-analyses, and it is the agent the TADS and Emslie trials turned on. A reasonable start is fluoxetine 10 mg oral once daily, titrating within the licensed range and reviewing at one week then about two weekly. Benefit takes four to six weeks to judge. [1] [3] [9]
The Cipriani network meta-analysis found that of the antidepressants studied in children and adolescents, only fluoxetine had a convincing efficacy advantage over placebo without a disproportionate tolerability burden — which is why paroxetine, venlafaxine and duloxetine are not first-line choices in this age group. The Zhou network meta-analysis extended the comparison to psychotherapies and combinations and supported combined treatment for more severe presentations. [1] [2]
For treatment-resistant depression, the TORDIA trial showed that switching to another SSRI or to venlafaxine, each combined with CBT, produced a higher response than a switch without CBT — so optimising psychotherapy and reassessing the diagnosis (bipolar, trauma, substance use, comorbidity) matter as much as changing the drug. The ADAPT trial similarly supported combining an SSRI with CBT in adolescents with moderate to severe depression who had not responded to brief therapy. [4] [5]
Specific Subtypes & Scenarios
Prepubertal depression is managed psychotherapy-first; the drug evidence is thinner in younger children, so you reach for fluoxetine only when the episode is moderate to severe and psychotherapy has not helped, and you do so with a specialist involved. [9] [11]
Depression with active suicidality or self-harm is treated as a safety emergency first and a mood disorder second: structured risk assessment, a written safety plan, means restriction, rapid follow-up, and specialist involvement. Treat the depression in parallel, but never let the prescription become a substitute for the safety plan. [7] [11]
Depression with comorbid ADHD, anxiety, autism or substance use is the rule, not the exception. Treat the most impairing and dangerous condition first, coordinate with existing teams, and watch for drug interactions — for example, an SSRI added to a stimulant needs attention to appetite, sleep and activation. [11]
Depression with psychotic features requires urgent specialist care and a combination of an antidepressant and an antipsychotic, usually in a specialist setting — it is not managed with psychotherapy and watchful waiting alone. [11]
Complications & Pitfalls
Untreated or undertreated depression carries real and measurable harm: suicide, self-harm, school failure and dropout, substance use, impaired relationships, and recurrence. The complications of treatment are smaller but real and must be discussed openly. [7] [13]
The best-known drug signal is SSRI-related activation and the small absolute increase in suicidal thinking captured in the Bridge meta-analysis and the 2004 regulatory warnings. The effect is small in absolute terms, it is largest early in treatment, and it is best handled by starting low, reviewing at one week, and counselling families to watch for new agitation, restlessness, increased energy with persisting low mood, or new suicidal thoughts. [7] [11]
Bridge 2007 — JAMA (PMID 17440145)
Meta-analysis of randomised controlled trials in under-18s
Key finding
Small absolute increase in suicidal ideation or attempts with antidepressants versus placebo; no completed suicides across the pooled trials.
Practice change
Monitor closely early in treatment; the warning is a reason for careful review, not for withholding effective treatment from a depressed young person.
The pitfall that does the most damage is the opposite of reckless prescribing: undertreatment driven by fear of the warning. The same evidence base that flags a small suicidality signal also shows that fluoxetine and CBT reduce depressive symptoms in adolescents, and that untreated depression is itself a major suicide-risk factor. The task is to use the warning wisely. [1] [3] [7]
Antidepressant discontinuation syndrome — dizziness, flu-like symptoms, sensory disturbances, irritability — occurs when an SSRI with a short half-life (notably paroxetine or venlafaxine) is stopped abruptly; fluoxetine's long half-life makes it uncommon. Taper gradually over weeks and warn the family in advance. [11]
Prognosis & Disposition
Adolescent depression is often an episodic, relapsing condition. A single episode predicts a substantially raised risk of recurrence, and the factors that worsen prognosis are comorbidity (especially anxiety, substance use and a bipolar diathesis), family conflict, chronic stressors, treatment dropout, and a long duration before effective treatment. [13] [14]
Treatment dropout is itself a prognostic signal: adolescents who disengage from psychological treatment during a trial had poorer outcomes, which is why engagement, the therapeutic alliance, and low-barrier follow-up are clinical priorities, not soft extras. [14]
Disposition is layered: mild depression can be managed in primary care with a clear review date; moderate depression in primary care with shared-care specialist input; severe, treatment-resistant or high-risk depression in specialist child and adolescent mental-health services; and acute risk, psychosis or refusal to eat or drink in an inpatient setting. A relapse-prevention plan — early-warning signs, the therapy that worked, the contact who helped, and how to restart care — should be written before discharge, and transition to adult services planned in advance for older adolescents. [11]
Special Populations
Prepubertal children need a psychotherapy-first approach and a careful search for organic, developmental, trauma and safeguarding drivers; drug evidence is weakest here. Young people with neurodevelopmental disability or autism may present with behaviour change rather than verbalised mood, and need assessment tools and therapy adapted to their communication and sensory profile. [11]
Looked-after children and those in out-of-home care, trauma-exposed and refugee or asylum-seeker young people carry elevated rates of depression driven by adversity, loss and instability; trauma-informed assessment and care are essential, and an SSRI must never be a substitute for safety, stability and trauma-focused support. [11]
LGBTQI+ and gender-diverse young people experience depression at substantially higher rates, largely through minority stress rather than identity itself; an affirming, non-judgemental assessment and access to appropriate support are protective. Rural and remote youth often face thin access to child and adolescent mental-health services, so telehealth, school-based supports and a clearly named local clinician matter disproportionately. Indigenous young people may carry the additional weight of intergenerational trauma and culturally unsafe services; engagement is improved by Indigenous-led and culturally responsive models of care. [11] [13]
Evidence, Guidelines & Regional Differences
The disease is global, but the drugs, thresholds and service models are regional. Name the guideline you are quoting and carry the differences explicitly. [1] [11]
| Region | First-line | SSRI of choice | Service model |
|---|---|---|---|
| ANZ | Psychotherapy first; SSRI if moderate to severe | Fluoxetine | GP mental-health treatment plans, headspace, private psychology, CAMHS for severe |
| UK (NICE NG134) | Psychological therapy as first-line for more than mild depression | Fluoxetine (only with psychological therapy) | NHS CAMHS stepped care; antidepressant not for mild depression |
| US (GLAD-PC / AACAP) | Psychoeducation, therapy, and fluoxetine when indicated | Fluoxetine | Primary-care-initiated management with specialist collaboration |
| Canada / RCPSC | Psychotherapy first; pharmacotherapy when indicated | Fluoxetine | Shared mental-health care between primary care and specialists |
The evidence backbone is a set of trials and syntheses you should be able to name. TADS established that fluoxetine, CBT and their combination all help adolescents with depression, with combination treatment giving the best balance of efficacy and safety. TORDIA showed that switching medication plus adding CBT improved response in resistant depression. ADAPT supported SSRI plus CBT in moderate to severe adolescent depression. IMPACT found three structured psychotherapies broadly comparable, emphasising competent delivery. The Cipriani and Zhou network meta-analyses confirmed fluoxetine as the best benefit-risk SSRI and supported combination therapy for more severe presentations. [1] [2] [3] [4] [5] [6]
The live controversy is not whether to treat, but how to use the suicidality warning. The warning rightly drives careful early monitoring; it should not drive a generation of under-treated adolescent depression, because untreated illness is the larger risk. Shared decision-making with the young person and family, documenting the benefits and the monitoring plan, is the standard of care. [7] [11]
Exam Pearls
The adolescent who drops out of therapy does worse — engagement and the therapeutic alliance are clinical priorities, and a clearly named clinician who follows up is part of the treatment. [14]
When you cannot decide whether it is adjustment disorder or a major depressive episode, apply the five-symptom threshold and the duration and impairment tests; if criteria are met, treat the depressive episode, and do not let a stressor narrative delay effective care. [10] [11]
References
- [1]Cipriani A, Zhou X, Del Giovane C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet, 2016.PMID 27289172
- [2]Zhou X, Teng T, Zhang Y, et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: a systematic review and network meta-analysis. Lancet Psychiatry, 2020.PMID 32563306
- [3]March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial. JAMA, 2004.PMID 15315995
- [4]Brent D, Emslie G, Clarke G, et al. Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial. JAMA, 2008.PMID 18314433
- [5]Goodyer I, Dubicka B, Wilkinson P, et al. Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care with and without cognitive behaviour therapy in adolescents with major depression: randomised controlled trial. BMJ, 2007.PMID 17556431
- [6]Goodyer IM, Reynolds S, Barrett B, et al. Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): a multicentre, pragmatic, observer-blind, randomised controlled superiority trial. Lancet Psychiatry, 2017.PMID 27914903
- [7]Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA, 2007.PMID 17440145
- [8]Hetrick SE, McKenzie JE, Bailey AP, et al. New generation antidepressants for depression in children and adolescents: a network meta-analysis. Cochrane Database Syst Rev, 2021.PMID 34029378
- [9]Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized clinical trial. J Am Acad Child Adolesc Psychiatry, 2002.PMID 12364842
- [10]Zuckerbrot RA, Cheung AH, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice Preparation, Identification, Assessment, and Initial Management. Pediatrics, 2018.PMID 29483200
- [11]Cheung AH, Zuckerbrot RA, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part II. Treatment and Ongoing Management. Pediatrics, 2018.PMID 29483201
- [12]Cyranowski JM, Frank E, Young E, Shear MK. Adolescent onset of the gender difference in lifetime rates of major depression: a theoretical model. Arch Gen Psychiatry, 2000.PMID 10632229
- [13]Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry, 2010.PMID 20855043
- [14]O'Keeffe S, Martin P, Goodyer IM, Wilkinson P, Byford S. Prognostic Implications for Adolescents With Depression Who Drop Out of Psychological Treatment During a Randomized Controlled Trial. J Am Acad Child Adolesc Psychiatry, 2019.PMID 30946974
- [15]Richardson LP, McCauley E, Grossman DC, et al. Evaluation of the Patient Health Questionnaire-9 Item for detecting major depression among adolescents. Pediatrics, 2010.PMID 21041282