Paeds · nephrology-urology-fluids-and-electrolytes
Urinalysis, renal function and paediatric kidney assessment
Also known as Bedside Schwartz eGFR children · Urine dipstick interpretation paediatrics · Estimated GFR children · Protein-to-creatinine ratio children · Urinalysis interpretation paediatrics · Renal function testing children
A fellowship approach to paediatric kidney assessment at the bedside: how to collect and interpret urine, read the dipstick and microscopy, estimate glomerular filtration rate with the bedside Schwartz equation, stage chronic kidney disease, and combine urine and blood data into a safe plan from neonate to transition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child passes urine, and you send blood to the laboratory. The two streams tell you different things, and the skill is making them speak to each other. Urinalysis tells you what is happening at the kidney surface and along the tubule right now. Renal function testing tells you how much filtration the kidney is performing. Together they separate pre-renal, intrinsic and post-renal problems, and they show whether a kidney is acutely injured, chronically scarred or working well. [2] [4]
Urinalysis means the macroscopic appearance of urine, the chemical dipstick, and the spun-urine microscopy. Each layer adds resolution. The dipstick is a screening tool; microscopy and culture confirm what it suggests. A dipstick is never the end of a diagnostic sentence in a sick child. [2] [3]
Renal function is the clearance work the kidney performs, summarised as the glomerular filtration rate. Direct measurement with iohexol or inulin clearance is the standard, but it is invasive and slow. At the bedside you estimate GFR from serum creatinine and height, because creatinine is freely filtered at the glomerulus and barely secreted or reabsorbed. [1] [11]
The bedside kidney-assessment pathway
Collect urine you can trust
Clean-catch or catheter for diagnosis; avoid bag urine where the result will change treatment.
Read dipstick plus microscopy
Pair the chemistry strip with cells and casts; never read the strip alone in a sick child.
Estimate GFR with Schwartz
eGFR equals 0.413 times height in cm divided by creatinine in mg per dL, indexed to 1.73 m2.
Quantify any abnormality
Protein-to-creatinine ratio and culture confirm a dipstick signal before you act.
Combine and trend
Marriage of urine and blood data, then trend the creatinine over hours to days.
Classification
Separate what you are measuring before you interpret it. Urinalysis classifies by what the dipstick pad and the microscope show. Renal function classifies by the filtration stage. Mixing these axes is the classic exam trap. [2] [4]
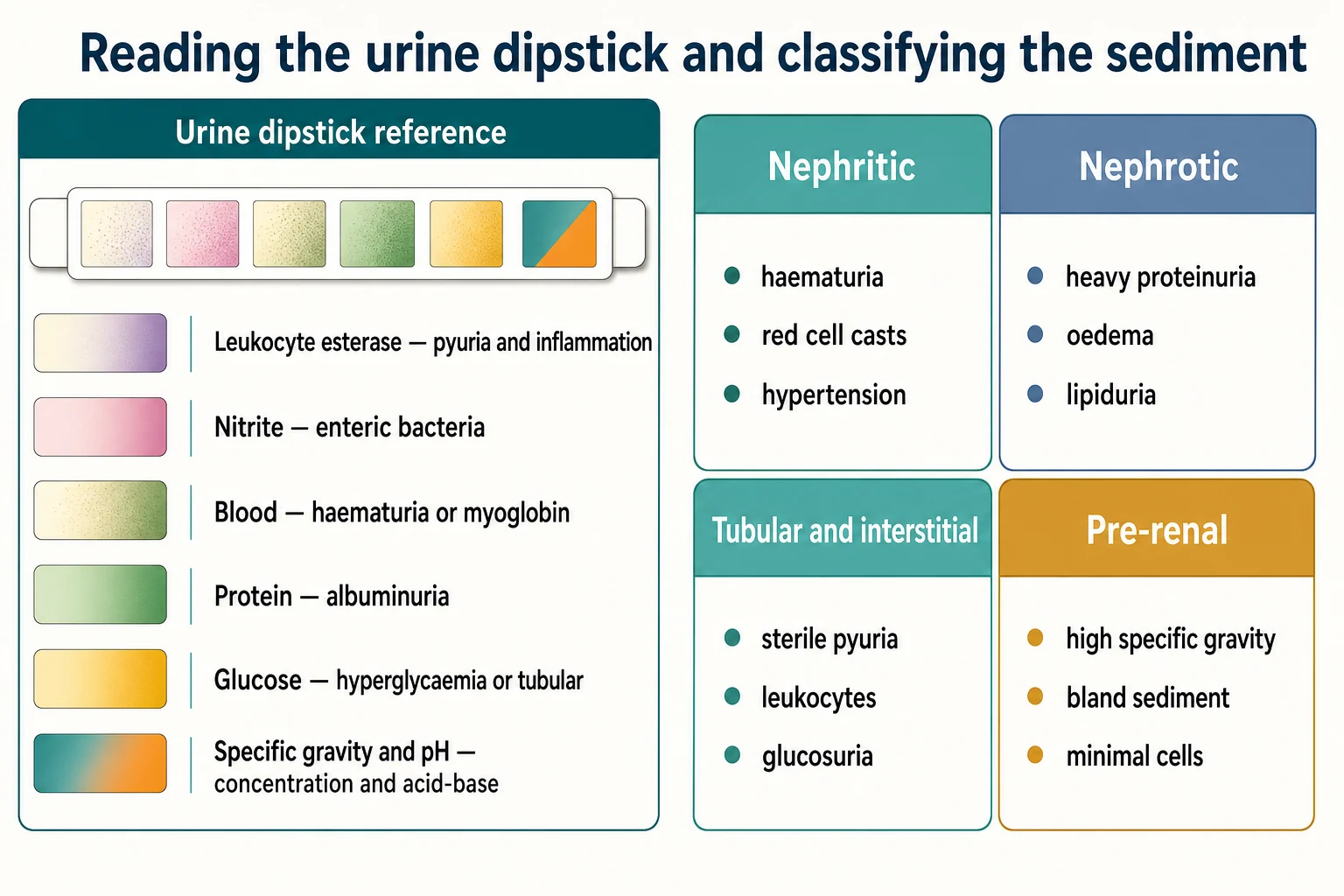
Each dipstick pad answers a different question. Leukocyte esterase detects neutrophil enzymes and points to inflammation or infection. Nitrite suggests enteric bacteria that reduce dietary nitrate, but it needs bladder dwell time, so a quick void gives a false negative. Blood is positive with intact red cells, free haemoglobin or myoglobin, so the strip cannot distinguish them. Protein reacts mainly to albumin, so it under-detects low-molecular-weight tubular proteins. Glucose signals hyperglycaemia or tubular dysfunction, and specific gravity estimates urine concentration. [2] [3]
The sediment sorts the pattern. Red cell casts mean glomerular bleeding. White cell casts mean inflammation or infection. Granular casts and muddy-brown tubular cells point to acute tubular injury. Crystals and bacteria complete the picture. The dipstick raises a hypothesis; the sediment and culture confirm it. [2]
Nephritic pattern
- Haematuria with dysmorphic red cells
- Red cell casts
- Mild to moderate proteinuria
- Often hypertension and reduced eGFR
Nephrotic pattern
- Heavy albuminuria
- Oval fat bodies and lipiduria
- Bland sediment with few cells
- Oedema and low serum albumin
Tubular pattern
- Leukocytes and sterile pyuria
- Glucosuria with normal blood glucose
- Defective concentrating ability
- Possible eosinophiluria in interstitial disease
Pre-renal pattern
- High specific gravity
- Bland sediment
- Minimal protein or blood
- Functional reduction rather than kidney damage
Renal function stages by filtration. KDIGO indexes GFR to 1.73 square metres of body surface area so that children of different sizes and adults compare on one scale. [4]
| KDIGO category | eGFR in mL per min per 1.73 m2 |
|---|---|
| G1 | 90 or higher |
| G2 | 60 to 89 |
| G3a | 45 to 59 |
| G3b | 30 to 44 |
| G4 | 15 to 29 |
| G5 | below 15 |
Epidemiology & Risk Factors
Mild dipstick abnormalities are common in well children and most are benign, which is why isolated findings need quantification and a repeat sample rather than instant alarm. Up to a tenth of school-age children show dipstick blood or protein at least once on a random sample, yet persistent abnormality is far less frequent. Distinguishing the transient from the structural is the whole game of screening. [7] [8]
Asymptomatic bacteriuria is a trap of its own. A meta-analysis confirms that bacteria can grow in bladder urine of children who have no symptoms and no tissue injury, so a positive culture alone is not disease. Treating it does not prevent later infection and can cause harm. [8]
Risk for genuine kidney disease clusters in recognisable groups. The strongest signal is a structural urinary tract abnormality detected antenatally, followed by a family history of inherited nephropathy, episodes of dehydration or hypoxia in a neonate, exposure to nephrotoxic drugs, and septic or multi-organ failure in intensive care. [6]
Collection error is itself a risk factor for a false pathway. Bag urine carries a high contamination rate, and a positive culture from a bag is far more likely to be skin flora than true infection. Clean-catch and catheter samples cut this contamination, and direct comparison in preschool children shows a clear difference in usable results. [3] [9]
Pathophysiology
Filtration is a bulk-flow process. Each glomerulus passes plasma across a size-and-charge barrier into Bowman space, and the resulting filtrate travels down the tubule where water and solutes are reclaimed. Creatinine crosses that barrier freely, and the kidney neither reabsorbs nor meaningfully secretes it, so its clearance tracks glomerular filtration closely. This is why creatinine became the bedside proxy for GFR. [1] [11]
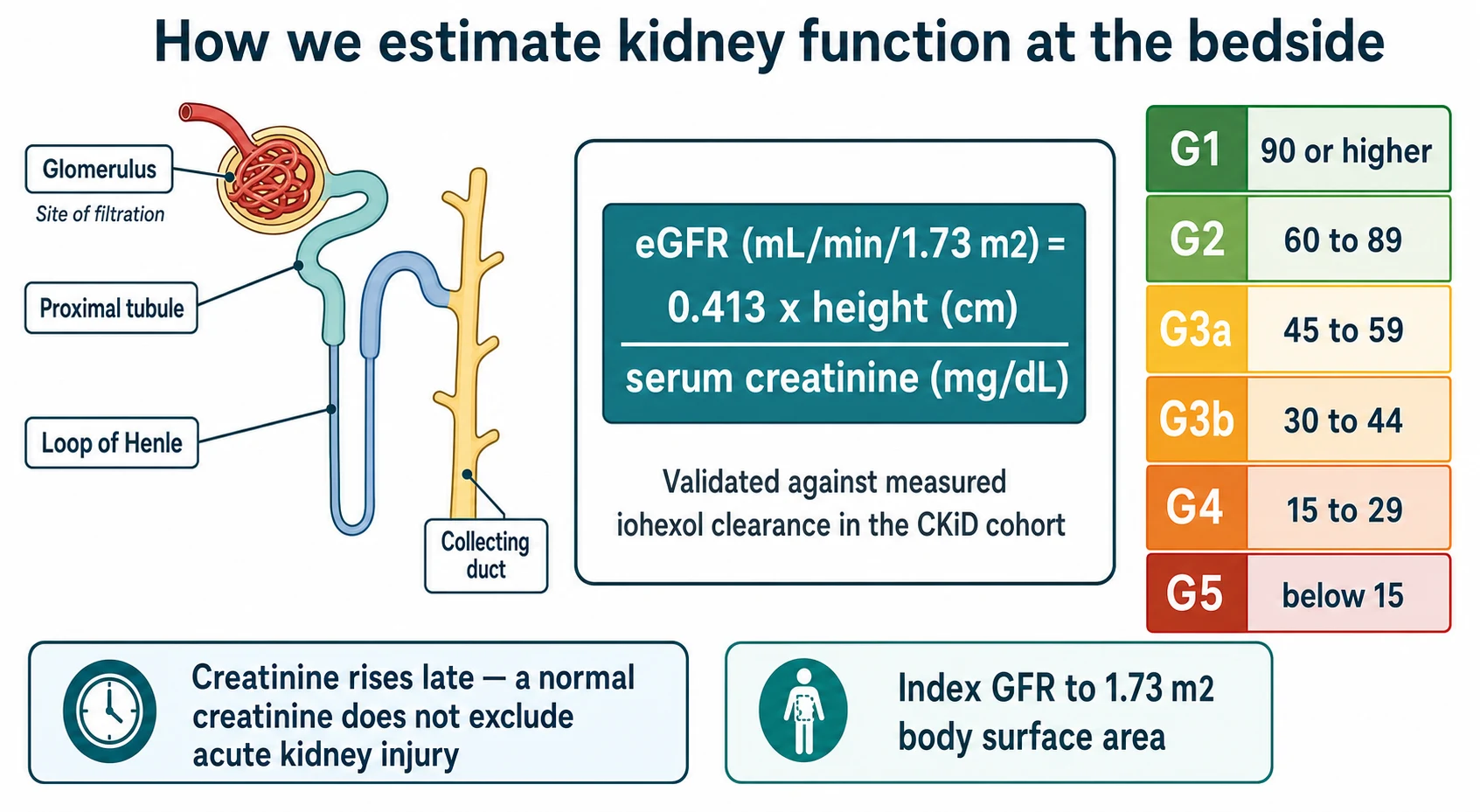
The bedside Schwartz equation turns that physiology into a number. The updated CKiD equation gives eGFR in mL per min per 1.73 m2 equal to 0.413 multiplied by height in centimetres divided by serum creatinine in mg per dL. The height term replaces muscle mass, because taller children generate more creatinine and need more filtration. The equation validates against measured iohexol clearance in children with chronic kidney disease. [1] [12]
The original 1976 Schwartz formula used a constant of 0.55, and 0.45 for infants, but modern enzymatic creatinine assays read lower than the old methods, so the constant was revised upward to the 0.413 used today. Quoting the wrong constant is a real error, because it changes the estimate. Always state which equation you used and in which units. [1] [5]
Three caveats protect you from over-reading the number. First, creatinine is a lagging marker, so early acute kidney injury hides behind a normal value. Second, muscle mass distorts the equation in cachectic, amputee or neuromuscular disease, where creatinine generation is low and the child can have a deceptively reassuring result. Third, every estimate needs a measured height, because a guessed height produces a guessed GFR. [6] [11]
Cystatin C offers a muscle-independent cross-check. It is filtered freely and reabsorbed and catabolised by the tubule, so it is less dependent on muscle mass than creatinine. Equations that combine creatinine and cystatin C perform best across the paediatric range, and cystatin C is particularly helpful when muscle mass is abnormal. [11] [12]
Clinical Presentation
Presentation is the reason the test was sent, and it sets your pre-test expectation. A febrile infant, a puffy child, a teenager with brown urine, and a neonate with failing oxygenation each change the meaning of the same dipstick. Start from the child, not from the laboratory printout. [2] [6]
Age shapes the likely script. A neonate with poor urine output after a hypoxic or septic course raises acute kidney injury, and the serum creatinine still reflects maternal creatinine in the first days of life. A toddler with fever and irritability raises urinary tract infection. A school-age child with cola-coloured urine two weeks after a sore throat raises post-infectious glomerulonephritis. An adolescent with oedema and frothy urine raises nephrotic syndrome. [4] [7]
Red flags in the history raise the cost of a false negative. These include oliguria or anuria, gross haematuria, marked oedema, hypertension, a flank mass, recent nephrotoxin exposure, and a strong family history of renal failure or deafness. Any of these moves the threshold toward confirming rather than watching. [4]
Drug exposure belongs in every kidney history. Non-steroidal anti-inflammatory drugs, aminoglycosides, angiotensin-converting enzyme inhibitors, radiocontrast and certain chemotherapy agents all reduce filtration or injure the tubule. Polypharmacy in a complex child compounds the risk. [6]
Differential Diagnosis
Use the urine and blood together to separate where the problem sits. The same reduced urine output can be pre-renal, intrinsic or post-renal, and the tests tell them apart. [2] [4]
A pre-renal problem keeps a concentrated, bland urine with high specific gravity and normal sediment, because the kidney itself is intact and trying to hold water. Intrinsic disease shows cells, casts, blood or protein in the sediment, because the tissue is injured. A post-renal obstruction shows a variable sediment and needs imaging to confirm. [2]
For isolated microscopic haematuria, a systematic review of over a thousand children shows that the commonest cause is benign, but a smaller fraction have glomerular disease, hypercalciuria or stones. Persistent or symptomatic haematuria, or haematuria with proteinuria, hypertension or reduced eGFR, shifts the work-up toward nephrology. [7]
For proteinuria, decide whether it is transient, orthostatic or persistent. Transient proteinuria follows fever, exercise or illness and resolves. Orthostatic proteinuria appears only upright and is benign in children. Persistent fixed proteinuria on a first-morning sample needs quantification and referral. [4]
Clinical & Bedside Assessment
Before you interpret any result, check three things at the bedside. Confirm the sample came from the right child, confirm the collection method, and confirm the timing relative to fluid status and drugs. A result divorced from these facts misleads. [3] [9]
Examine the child for volume status, because filtration and urine concentration depend on it. Look for dehydration, oedema, hypertension and a palpable bladder or flank mass. Blood pressure belongs on every kidney assessment, and it must use the right cuff and the right centile for age and height. [4]
Read the dipstick against the clinical question. Leukocyte esterase and nitrite together raise urinary infection, but either alone is weaker. A systematic review shows that dipstick sensitivity for childhood infection is imperfect, so a negative strip in a sick febrile infant does not exclude it. [3]
Note the urine appearance. Cola or tea-coloured urine suggests glomerular bleeding. Frothy urine suggests heavy protein. Red urine that is clear of red cells suggests free haemoglobin or myoglobin, which the dipstick blood pad reads as positive. [2]
Investigations
This section is the core skill of the topic. Sequence the tests so each step decides the next. [1] [2]
1. Collect the urine correctly
Choose the method for the clinical question. For diagnosing urinary tract infection in a sick child, use clean-catch, catheterisation or suprapubic aspiration, because bag urine contaminates too often. Comparison of catheter and clean-catch samples in preschool children shows acceptable and similar contamination when the technique is good, whereas bag samples fail. [3] [9]
2. Read dipstick and microscopy as a pair
Run the chemistry strip, then spin the urine and read the sediment. The strip screens; the cells and casts confirm. Red cell casts are pathognomonic of glomerular disease. White cell casts point to infection or interstitial nephritis. Muddy-brown granular casts point to acute tubular injury. [2]
3. Estimate GFR with the bedside Schwartz equation
Calculate eGFR in mL per min per 1.73 m2 as 0.413 times height in cm divided by serum creatinine in mg per dL. Measure the height properly. If the laboratory reports creatinine in micromol per L, divide by 88.4 to convert to mg per dL before you apply the equation. State the equation and the units every time. [1]
4. Stage with KDIGO categories
Place the eGFR on the G1 to G5 ladder and combine it with an albuminuria stage. This single act frames how urgently and how aggressively to investigate and refer. [4]
5. Quantify proteinuria
If the dipstick shows protein, measure a protein-to-creatinine ratio or albumin-to-creatinine ratio on a first-morning sample. A first-morning value under 20 mg protein per mmol creatinine is normal. A normal random ratio excludes significant proteinuria; a raised first-morning ratio needs referral. Albuminuria categories run A1 under 30 mg per g, A2 from 30 to 300 mg per g, and A3 above 300 mg per g. [4]
6. Confirm infection with culture
Send culture from a reliable sample. Interpret growth against the method: a single organism at a significant count from a catheter or suprapubic sample supports infection, while mixed growth from a bag sample usually means contamination. Remember asymptomatic bacteriuria in children and do not treat it as disease. [3] [8]
7. Add biomarkers and imaging when they change the plan
Novel markers such as urinary NGAL are being evaluated to distinguish renal from lower-tract infection in young febrile children, but they are adjuncts rather than replacements for culture. Reserve renal ultrasound and other imaging for obstruction, stones, structural disease or persistent unexplained abnormality. [10] [4]
Management — Resuscitation
When kidney findings come from an unwell child, treat the threat first and investigate alongside it. Hyperkalaemia, severe acidosis, fluid overload with pulmonary oedema, and hypertensive emergency each kill before any confirmatory result returns. [6]
Stabilise airway, breathing and circulation, check the blood glucose, and secure intravenous access. Treat a potassium above 6.5 mmol per L or any level with electrocardiogram changes immediately, because it can arrest the heart. Manage fluid overload with restriction, diuretics and respiratory support, and control a hypertensive emergency with a carefully titrated agent. [6]
Tell the family what you fear and what you are doing. The sentence "we are treating your child's kidneys as injured while we find out why" is clearer than a list of assays. Escalate early to paediatric intensive care and nephrology when urine output stays low or the potassium climbs. [4]
Management — Definitive & Stepwise
After the threat is controlled, work through a repeatable algorithm that turns an abnormal screen into a directed plan. [1] [4]
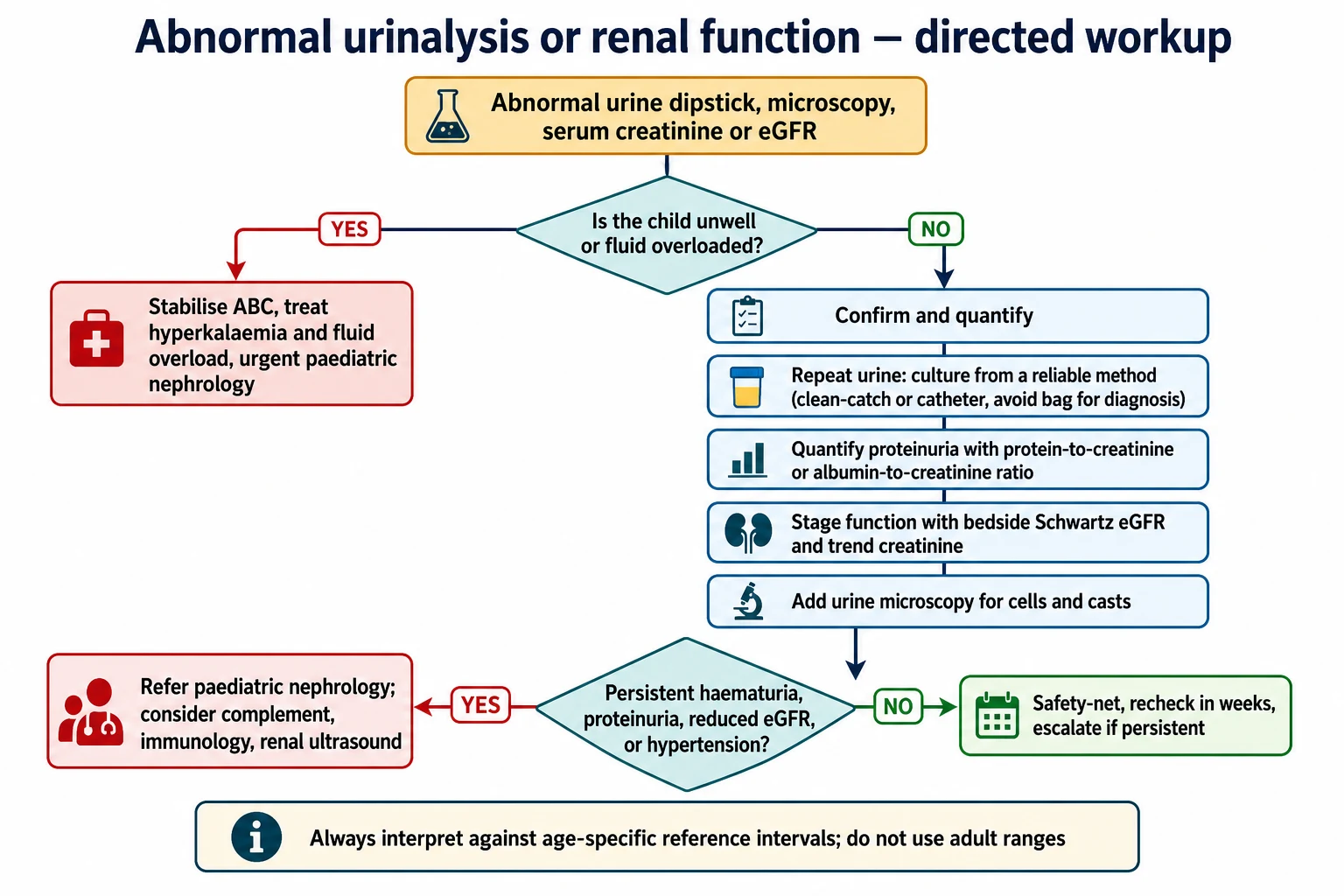
- Re-state the clinical question from the child in front of you. [2]
- Confirm the urine result with a reliable sample and microscopy before acting. [3] [9]
- Quantify proteinuria with a first-morning ratio and stage the eGFR with Schwartz and KDIGO. [1] [4]
- Trend the creatinine over hours to days, because a single value under-represents acute change. [6]
- Refer paediatric nephrology for persistent haematuria, persistent proteinuria, eGFR below 60, hypertension, or a structural finding. [4]
FILTRATION at the bedside
Safety-net the well child with a minor isolated finding. Arrange a first-morning repeat in a few weeks, give clear return triggers, and escalate only if the abnormality persists or new red flags appear. [4] [7]
Specific Subtypes & Scenarios
Neonate and young infant. Serum creatinine reflects the mother in the first days of life and falls over roughly two weeks in a term baby, slower in a preterm infant. Use the change from baseline, not a single value, to judge acute kidney injury. Height-independent methods help estimate baseline creatinine in critically ill children where a reliable height is hard to get. [6]
Suspected urinary tract infection. Collect by clean-catch, catheter or suprapubic aspiration. Treat a positive culture from a reliable sample in a symptomatic child, but do not chase mixed growth from a bag. Dipstick and novel markers are adjuncts, not replacements for culture. [3] [9] [10]
Isolated microscopic haematuria. Most children have a benign cause, but persistent or symptomatic bleeding, or bleeding with proteinuria, hypertension or reduced eGFR, needs nephrology referral and a search for glomerular disease, hypercalciuria or stones. [7]
Suspected nephrotic or nephrotic-range proteinuria. Quantify with a ratio, check serum albumin and complement, and refer. Heavy proteinuria with oedema warrants prompt nephrology input because of thrombotic and infectious risk. [4]
Transition to adult care. Equation choice changes at the boundary between paediatric and adult services. The Full Age Spectrum equation and cystatin C-based equations cross this boundary more smoothly than the paediatric Schwartz equation, which is built for children. Agree the equation with the adult team so the GFR does not jump at handover. [5] [11]
Technology-dependent child. Compare values with the child's personal baseline, not only population ranges. Neuromuscular disease distorts creatinine through low muscle mass, so cystatin C becomes more reliable. [11] [12]
Complications & Pitfalls
Trusting a normal creatinine in a sick child. Creatinine lags injury. A normal value in a dehydrated, septic or oliguric child does not exclude acute kidney injury. Trend it. [6]
Acting on a bag-urine culture. Bag samples contaminate, and a positive culture often reflects skin flora rather than infection. Use a reliable method before committing to treatment. [3] [9]
Using the wrong equation or units. The original 0.55 constant overestimates GFR with modern assays; use 0.413 for the bedside Schwartz equation. Mixing mg per dL with micromol per L corrupts the result. Always state the equation and units. [1] [5]
Adult reference intervals. Neonatal creatinine is naturally higher than adult creatinine, and normal ranges shift with age. Applying adult ranges mislabels a healthy infant. [6]
Quoting an eGFR without a measured height. A guessed height produces a guessed GFR. The equation is only as good as its inputs. [1]
Missing asymptomatic bacteriuria. Treating bacteria in a well child does not prevent infection and adds harm. Distinguish colonisation from disease. [8]
Ignoring muscle mass. In cachexia, amputation or neuromuscular disease, creatinine generation falls and the estimate drifts upward, falsely reassuring. Add cystatin C. [11] [12]
Discharging a persistent abnormality. A single abnormal dipstick may be benign, but persistent unexplained haematuria or proteinuria needs quantification and follow-up. [4] [7]
Prognosis & Disposition
Disposition follows the combination of the urine pattern, the filtration stage, the trend and the child's stability. A well child with a transient isolated finding and a normal first-morning repeat can go home with safety-netting. A child with persistent proteinuria, reduced eGFR, hypertension or a structural lesion needs nephrology referral. [4]
Pending results need an owner, a timeframe and a plan if they return abnormal. Hand the creatinine trend and the first-morning ratio forward, not just single numbers, so the next team can judge trajectory. [6]
Prognosis depends on the underlying cause more than on any single test. A pre-renal insult that is reversed recovers; a structural or glomerular disease follows its own course. The role of assessment is to detect early, stage honestly, refer promptly, and watch the trend. [4] [11]
Special Populations
Neonates. Maternal creatinine confounds early values, and preterm infants have immature tubules. Use baseline change and watch closely after hypoxic or septic insult. [6]
Complex and technology-dependent children. Personal baselines, polypharmacy and device issues change both the pre-test risk and the meaning of a result. Compare with the child, not only the textbook. [11]
Neuromuscular disease and low muscle mass. Creatinine under-represents filtration. Reach for cystatin C or a combined equation. [12]
Immunocompromised children. Atypical organisms and blunted inflammation change the urinalysis. Widen the culture and the differential earlier. [4]
Indigenous and migrant families. Access to repeat sampling, transport and follow-up shapes whether the plan is real. Use interpreters and address cultural safety, particularly for Aboriginal and Torres Strait Islander families and for Māori whānau. [4]
Socioeconomic disadvantage. A plan that needs unpaid leave, private transport or reliable phone access the family lacks is not a safe safety-net. Build follow-up around what the family can actually do. [4]
Adolescents at transition. Agree the equation and the reference intervals with the adult team so the GFR does not jump at handover. Confidential sexual-health testing can change the differential. [5]
Evidence, Guidelines & Regional Differences
The updated CKiD Schwartz equation remains the bedside standard for estimated GFR in children with chronic kidney disease, validated against measured iohexol clearance. The original formula used a constant of 0.55 and 0.45 for infants, but enzymatic assays shifted the constant to 0.413. Cystatin C and combined equations add accuracy when muscle mass is abnormal, and race has been removed from modern paediatric estimating equations. [1] [5] [11] [12]
KDIGO 2012 supplies the G1 to G5 staging and the albuminuria categories that frame assessment and referral. Simerville's review remains a high-yield teaching reference for dipstick and microscopy interpretation, and systematic reviews of urine sampling and dipstick performance anchor the evidence on collection method and screening limits. [2] [3] [4]
Do not export any single study's cut-off as universal local protocol. NICE and local fever pathways operationalise thresholds, but they do not replace clinical judgement about the child in front of you. Novel biomarkers such as NGAL are still under evaluation as adjuncts. [10]
Reference intervals and creatinine assays vary between laboratories, so confirm the local method before quoting a number. Retrieval distance changes how aggressively a rural clinician confirms and stabilises before transfer. Cultural safety for Aboriginal and Torres Strait Islander families, and Te Tiriti-informed care for Māori whānau, belongs inside how uncertain results are explained and followed up. [4]
NICE guidance on chronic kidney disease in under-25s frames paediatric assessment, staging and transition. MRCPCH theory rewards precise definitions of the Schwartz equation, the KDIGO stages and the dipstick pads, while clinical stations reward residual-risk language after an abnormal result. [4]
ABP nephrology content and ACGME clinical-reasoning milestones treat test selection and interpretation as core competence. The CKiD study underpins paediatric GFR estimation in North America, and CALIPER-informed age-specific reference intervals shape laboratory interpretation, especially in Canada. Race-free equations are now the standard. [1] [12]
Exam Pearls
- State the bedside Schwartz equation with the right constant: eGFR equals 0.413 times height in cm divided by serum creatinine in mg per dL. [1]
- Always index GFR to 1.73 square metres of body surface area. [4]
- A normal creatinine does not exclude acute kidney injury; trend it. [6]
- The original constant was 0.55, or 0.45 for infants; modern enzymatic assays use 0.413. [1]
- Read the dipstick and the microscopy together; red cell casts mean glomerular disease. [2]
- Nitrite needs bladder dwell time, so a quick void gives a false negative. [2]
- Use a reliable urine collection method; bag cultures contaminate. [3] [9]
- Quantify proteinuria with a first-morning protein-to-creatinine ratio. [4]
- Do not treat asymptomatic bacteriuria in a well child. [8]
- Cystatin C is the cross-check when muscle mass is abnormal. [11]
References
- [1]Schwartz GJ, et al New equations to estimate GFR in children with CKD J Am Soc Nephrol, 2009.PMID 19158356
- [2]Simerville JA, et al Urinalysis: a comprehensive review Am Fam Physician, 2005.PMID 15791892
- [3]Whiting P, et al Rapid tests and urine sampling techniques for the diagnosis of urinary tract infection (UTI) in children under five years: a systematic review BMC Pediatr, 2005.PMID 15811182
- [4]Stevens PE, et al Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline Ann Intern Med, 2013.PMID 23732715
- [5]Pottel H, et al Estimating glomerular filtration rate at the transition from pediatric to adult care Kidney Int, 2019.PMID 30922665
- [6]Hessey E, et al Evaluation of height-dependent and height-independent methods of estimating baseline serum creatinine in critically ill children Pediatr Nephrol, 2017.PMID 28523356
- [7]Clark M, et al Etiologies of asymptomatic microscopic hematuria in children - systematic review of 1092 subjects Diagnosis (Berl), 2015.PMID 29540037
- [8]Shaikh N, et al Prevalence of Asymptomatic Bacteriuria in Children: A Meta-Analysis J Pediatr, 2020.PMID 31787323
- [9]Bogie AL, et al Is There a Difference in the Contamination Rates of Urine Samples Obtained by Bladder Catheterization and Clean-Catch Collection in Preschool Children? Pediatr Emerg Care, 2021.PMID 34772880
- [10]Forster CS, et al Accuracy of NGAL as a Biomarker for Urinary Tract Infection in Young Febrile Children: An Individual Patient Data Meta-Analysis J Pediatr, 2023.PMID 37001635
- [11]Salvador CL, et al Estimating glomerular filtration rate in children: evaluation of creatinine- and cystatin C-based equations Pediatr Nephrol, 2019.PMID 30171354
- [12]Ng DK, et al Self-reported Race, Serum Creatinine, Cystatin C, and GFR in Children and Young Adults With Pediatric Kidney Diseases: A Report From the Chronic Kidney Disease in Children (CKiD) Study Am J Kidney Dis, 2022.PMID 34974031