Paeds · neurology-neurodisability-and-neuromuscular
Non-epileptic events and functional seizures
Also known as Psychogenic non-epileptic seizures in children · Dissociative seizures · Functional seizures in young people · Non-epileptic attack disorder · Functional neurological disorder with seizures · PNES in children and adolescents
Fellowship guide to the child or adolescent whose episodes look like epilepsy but are not: non-epileptic events, and within them the high-stakes entity of functional (dissociative) seizures. The single most important message is that functional seizures are real and involuntary, that antiseizure drugs do not work, and that the correct path is a positive diagnosis by video-electroencephalogram, an honest explanation, supervised withdrawal of unnecessary medication, and cognitive behavioural therapy. The page covers the semiology that distinguishes a functional seizure from an epileptic one and from the physiological mimics, the coexistence of epilepsy in a substantial minority, the management of an acute flurry in the emergency department without escalating sedation, and the safeguarding lens that any clinician must hold over the adolescent carrying this diagnosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Picture the patient this topic exists for. A fifteen-year-old is referred to the epilepsy service for spells that have occurred several times a week for a year and have not responded to two escalating antiseizure medications. The events last many minutes, her eyes stay closed and resist opening, her limbs thrash in a changing pattern, and she is tearful but fully oriented within a minute of stopping. She is exhausted, stigmatised, and on a drug that gives her no benefit and real side effects. The diagnosis is not refractory epilepsy — it is a functional seizure, and the correct move is to stop the drugs, name the condition, and begin therapy. [2]
This page covers the distinction between non-epileptic events broadly and functional seizures specifically, the semiology and video-electroencephalogram findings that confirm the diagnosis, the coexistence of genuine epilepsy in a substantial minority, the management of the acute emergency-department flurry, the stepwise pathway to recovery, and the safeguarding lens that must always sit over the adolescent carrying this label. It links to the first-seizure leaf for the broader mimics list, to the functional-neurological-symptoms leaf for motor and sensory functional disorders, and to the somatic-symptom leaf for the wider psychosomatic context. [1]
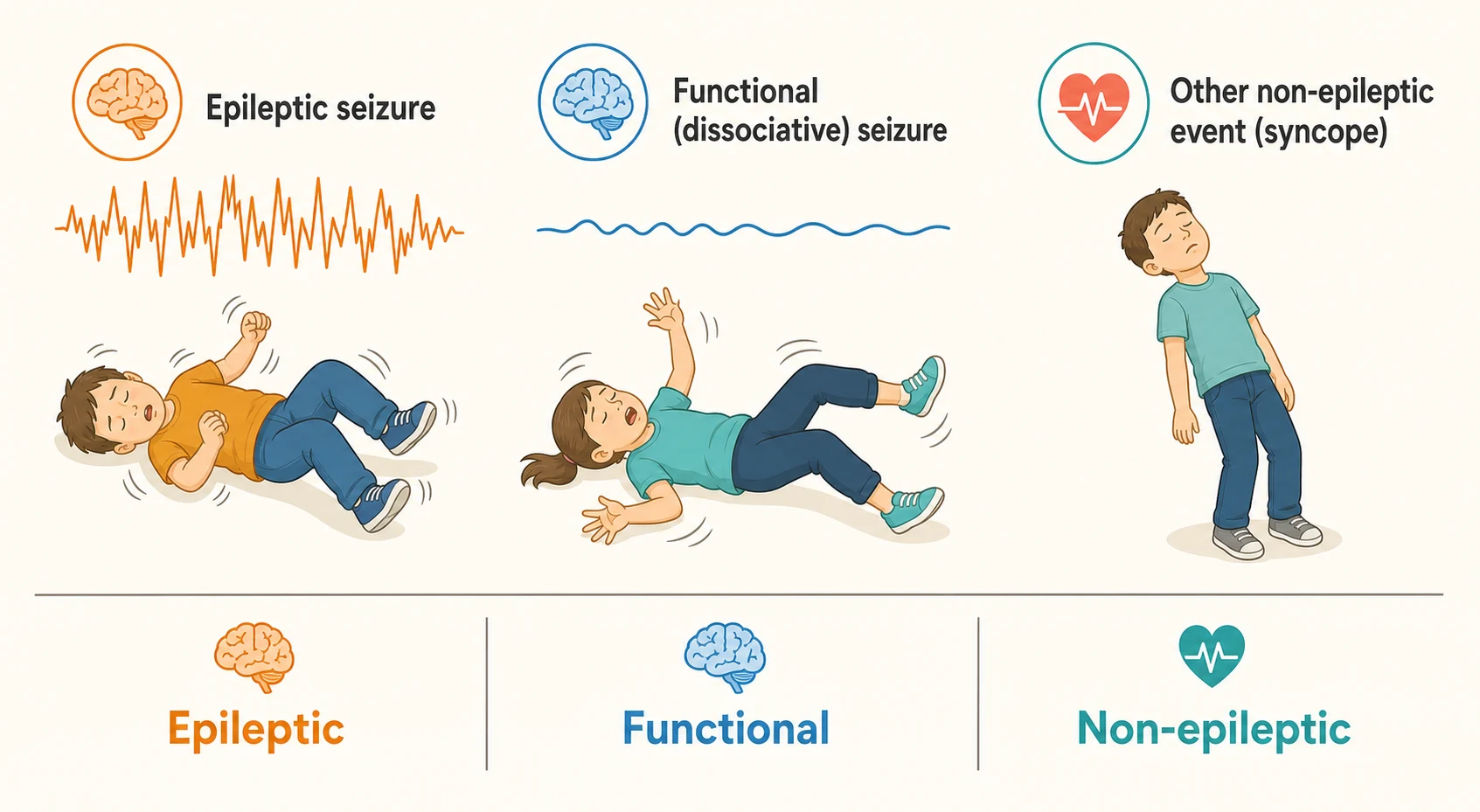
Overview & Definition
The first idea to hold is that a paroxysmal event and an epileptic seizure are not the same thing. An epileptic seizure is the transient appearance of signs or symptoms from abnormal, excessive and synchronous cortical neuronal activity. Many sudden episodes in a child look like that but arise from a completely different mechanism — a faint, a breath-holding spell, a sleep disturbance, a movement disorder, or a psychological process — and these are gathered under the umbrella term non-epileptic events. [1]
The functional, or dissociative, seizure is the most important member of that umbrella for the clinician to master. It is an involuntary episode of altered movement, sensation, consciousness or experience that resembles an epileptic seizure but occurs without the cortical electrical discharge. It sits within functional neurological disorder, the modern name for the group of conditions once called conversion disorder, in which genuine neurological symptoms are produced by a problem of nervous-system function rather than structure. [4]
Two words must be stripped from the clinician's vocabulary at the bedside. The first is "fake" — functional seizures are involuntary, and patients are not pretending or choosing to have them. The second is "all in the mind" — the events are as real to the patient as any seizure, the distress is genuine, and functional neuroimaging shows measurable alterations in the brain networks that generate movement and self-awareness. [6] The harm of the wrong language is immediate: a child told their attacks are "put on" disengages from care, loses trust in clinicians, and is denied the therapy that would help.
The practical consequence is that the clinician facing an unexplained attack holds two parallel questions. The first is whether the event is epileptic. The second, only if it is not, is which non-epileptic mechanism is at work — physiological or functional. Jumping straight to an antiseizure drug on the assumption that any convulsion is epilepsy is the single most common and most damaging error in this area of medicine. [1]
Classification
Non-epileptic events separate first into those driven by a physiological mechanism and those driven by a functional or psychological process. The physiological group includes syncope, breath-holding spells, parasomnias, migraine variants, movement disorders, tics, self-stimulatory behaviour and transient metabolic disturbances such as hypoglycaemia. These are mimics with a body-based cause, and each is worked up and managed on its own terms. [1] The functional group, headed by the dissociative seizure, is the focus of this page because it is the one most often mistaken for refractory epilepsy.
The functional seizure itself is defined by its mechanism and by the context it sits in. Under the framework of functional neurological disorder it shares its underlying model with functional weakness, functional tremor and functional sensory symptoms — a real symptom produced by altered nervous-system function, with normal structure, and shaped by a biopsychosocial interplay of predisposition, precipitant and perpetuation. [4] The diagnostic label in DSM-5 is conversion disorder, a dissociative or functional neurological symptom disorder, and the criteria are deliberately clinical rather than requiring that a psychological cause be identified. [11]
[1]The distinction matters because the two conditions travel through completely different pathways. Epilepsy is investigated with electroencephalography and imaging and treated with antiseizure medication. A functional seizure is confirmed by video-electroencephalogram and treated by psychological therapy and rehabilitation, and an antiseizure drug is actively unhelpful. A child given the wrong label is carried down the wrong pathway, sometimes for years. [5]
Epidemiology & Risk Factors
Functional seizures are commoner than most clinicians expect, and they are heavily over-represented in the tertiary epilepsy population. Around one in five to one in three patients admitted to an epilepsy monitoring unit for drug-resistant spells is found to have functional seizures rather than epilepsy, and in children and adolescents the diagnosis emerges most often in the early teenage years with a female predominance. [7] The delay between onset and the correct diagnosis is frequently measured in years, and that delay is itself a perpetuating factor because each year adds another ineffective drug and another layer of stigma.
The risk factors cluster into predisposing, precipitating and perpetuating groups, following the standard biopsychosocial model. Predisposing factors include anxiety, depression, a family or personal psychiatric history, neurodevelopmental difference, and a prior epilepsy or other neurological condition. [2] Precipitating factors are the adverse experiences and stressors that often precede onset — family breakdown, bullying, academic pressure, bereavement, chronic illness, and abuse or neglect. Perpetuating factors are the things that keep the attacks going, chief among them the misdiagnosis of epilepsy, the ongoing antiseizure medication, unrecognised and untreated comorbid depression or anxiety, and the secondary gain of attention or escape that no one would choose but that nonetheless reinforces the cycle. [3]
Pathophysiology
The mechanism of a functional seizure is best understood as a problem of nervous-system function rather than a problem of mind or of brain structure. During an epileptic seizure a population of cortical neurons fires in a hypersynchronous, excessive discharge that is visible on the electroencephalogram as spikes, sharp waves and rhythm. During a functional seizure the same body convulses, but the cortex does not produce an epileptic discharge, and the electroencephalogram keeps a normal background rhythm throughout the attack. [1] That single observation is why video-electroencephalogram is the diagnostic test.
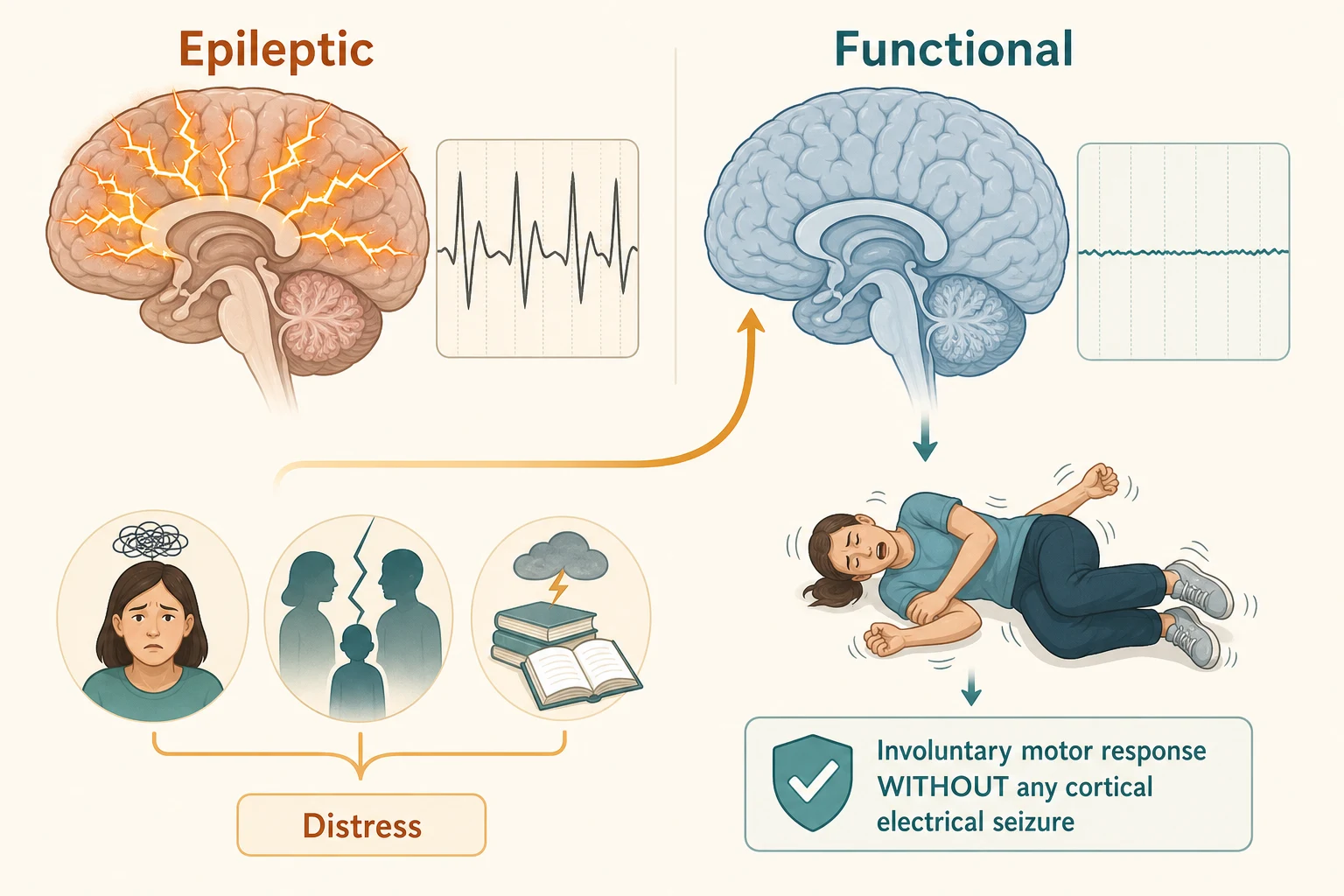
Modern functional neuroimaging has moved the field firmly away from the old idea that the symptom is imagined. Studies of functional neurological disorder show altered connectivity and activation between prefrontal regions, the limbic system and the motor networks, with a consistent theme of impaired sense of agency — the brain moves the body without registering the movement as self-generated. [6] The symptom is therefore produced by a genuine change in how the nervous system operates, even though the structure is intact and the electrical discharge of epilepsy is absent.
The biopsychosocial model ties this neurobiology to the clinical story. A vulnerable nervous system, shaped by predisposition, meets a precipitating stressor, and the result is an involuntary functional event. The perpetuating factors then lock the pattern in — the mislabel of epilepsy, the unnecessary drug, the unrecognised mood disorder, the unresolved adversity. Treatment works because it reverses these perpetuating factors rather than because it removes an imaginary symptom. [3]
Clinical Presentation
The presentation of a functional seizure is built almost entirely from the eyewitness account, because the attack is over by the time the child reaches the clinician. The features that point away from epilepsy and toward a functional origin are positive and observable, and an examiner expects a candidate to name them. The eyes are usually closed and resist the examiner's attempt to open them, in contrast to the open or deviated eyes of an epileptic seizure. The motor pattern is variable rather than stereotyped — thrashing, rolling, an asynchronous and out-of-phase movement of the limbs that waxes and wanes in intensity rather than building and terminating in a predictable rhythm. [1]
Other features reinforce the pattern. The attack is often prolonged, lasting several to many minutes rather than the one or two minutes typical of an epileptic convulsion. Pelvic thrusting, side-to-side head movement, forced eye closure and a changing rather than fixed motor pattern are classic. The recovery is rapid and complete, with the patient tearful and distressed but fully oriented within a minute, in sharp contrast to the postictal confusion and drowsiness of epilepsy. Recall of the event is often preserved, cyanosis and incontinence are uncommon, and the attacks frequently occur in the presence of others or in emotionally charged settings. [7]
The precipitant is as important as the semiology. A careful psychosocial history often uncovers an adverse experience in the months before onset — family breakdown, parental illness, bullying, academic or sporting pressure, bereavement, a new chronic illness, or disclosure of abuse. Comorbid anxiety, depression, post-traumatic stress, self-harm and other functional symptoms such as non-cardiac chest pain, chronic fatigue or functional weakness are the rule rather than the exception, and their presence both supports the diagnosis and defines the treatment. [2]
Differential Diagnosis
The differential of an attack that looks like a seizure but is not epileptic is wide, and the clinician's job is to place each event in the right mechanism. The physiological mimics are syncope with its brief convulsive jerks, breath-holding spells of infancy, parasomnias and night terrors, benign paroxysmal vertigo, migraine variants, Sandifer syndrome, shuddering attacks, tics and stereotypies, hypoglycaemia, and the rigors of fever. The functional mimics are the dissociative seizure itself and, less commonly, panic attacks and dissociation without convulsion. [1]
Functional seizure against its closest imitators
Two pitfalls deserve special emphasis. The first is frontal-lobe epilepsy, whose brief, bizarre, hyperkinetic and often nocturnal attacks can mimic a functional seizure perfectly and yet show a normal scalp electroencephalogram — the very feature that wrongly reassures the clinician. Stereotypy, short duration, clustering through the night and a response to an antiseizure drug point toward epilepsy, and a sleep or invasive electroencephalogram may be needed to resolve it. [1] The second is convulsive syncope, in which the brief myoclonic jerks of cerebral hypoperfusion are mistaken for a generalised tonic-clonic seizure; the upright trigger, prodromal pallor and rapid recovery mark the cardiovascular mechanism, and an electrocardiogram is mandatory before any other test.
The single most important differential question is not which mimic it is, but whether genuine epilepsy coexists. Around one in five to one in three young people with functional seizures also have epilepsy, and the two must be separated attack by attack. [12] A child can have a proven functional seizure recorded on video-electroencephalogram and still have genuine epileptic events at other times, and each is treated on its own merits. Assuming that one excludes the other, in either direction, is a serious error.
Clinical & Bedside Assessment
The assessment begins, as always, with the question of whether the child is safe and back to baseline. A child who is still in an attack, or who has not recovered, is assessed and supported while the episode runs its course — calm reassurance, a low-stimulation environment, and attention to airway, breathing and any injury. Once the child is settled, the structured assessment turns to the semiology, the psychosocial context, and the search for comorbidity and coexisting epilepsy. [7]
The functional-seizure assessment
Take a minute-by-minute account from every witness of the pre-ictal setting, the ictal motor pattern, the eye state, the duration, and the recovery — and ask the family to video any further event.
Distinguish the attack from epileptic and physiological mimics using the positive semiological features, never on a single sign.
Take a sensitive psychosocial history for adverse childhood experiences, family and school stressors, and screen for anxiety, depression, trauma, self-harm and other functional symptoms.
Examine for incongruent or inconsistent neurological signs (for example a positive Hoover sign) that support a functional process, and for any focal deficit that demands imaging.
Arrange video-electroencephalogram monitoring to capture a typical event, and actively look for coexisting epilepsy.
The psychosocial history is the part that clinicians most often underweight, and it is the part that most often explains the illness. Ask gently and without assumption about family functioning, parental illness, separation and conflict, about school attendance, friendship and bullying, about bereavement, chronic illness and hospital contact, and — when trust allows — about abuse, neglect and safety at home. The same history screens for the comorbid mood, anxiety and trauma disorders that drive the attacks and that must be treated for the attacks to remit. [2]
The examination looks for two things. The first is a functional neurological sign — a Hoover sign, where hip extension returns when the contralateral leg is tested against resistance, is the classic bedside marker of functional weakness and supports a functional process without proving the diagnosis. [4] The second is any focal neurological deficit, papilloedema or failure to return to baseline that points to a structural cause and demands urgent imaging. A normal examination is the expected finding in a functional seizure, and its normality is itself part of the picture.
Investigations
The investigation that matters is the video-electroencephalogram, and the goal is to capture a typical event. A diagnosis of functional seizure is a positive one: the child is admitted for monitoring, a typical attack is recorded, and the electroencephalogram during that attack shows a normal background rhythm with no epileptiform correlate while the clinical event unfolds. [1] The combination of the patient's habitual semiology and a normal ictal electroencephalogram is the gold standard, and it is the finding that allows the clinician to withdraw antiseizure medication with confidence.
[1] [8]Two investigative traps cause recurring harm. The first is reading a normal interictal electroencephalogram as proof of a functional seizure — it is not. A normal tracing between attacks is compatible with epilepsy, with a functional seizure, and with half the population, and only the capture of a typical event is diagnostic. The second is the historical use of prolactin, once drawn to separate epileptic from non-epileptic events; it is unreliable, it overlaps between the two, and it has no place in modern practice. [1]
When the diagnosis remains uncertain despite monitoring, the clinician returns to the semiology and the possibility of frontal-lobe epilepsy, whose bizarre brief attacks can escape scalp electroencephalography. A repeat study with sleep deprivation, additional temporal or additional anterior temporal electrodes, or, in a specialist centre, invasive monitoring may be required before the functional label is applied or rejected. [8] The cost of a wrong label is high in either direction, and the standard of proof is a captured event.
Management — Resuscitation
The resuscitation scenario in this topic is the child who arrives in the emergency department in a prolonged, repetitive flurry of functional attacks — sometimes called status non-epilepticus. The episode can run for tens of minutes to hours, looks dramatic, and triggers the reflex to give escalating benzodiazepines and to call for anaesthesia. That reflex is wrong and it is dangerous. [5] The attacks are not driven by cortical electrical discharge, so sedative drugs do not terminate them and add the real risk of respiratory depression in a patient who is breathing and conscious throughout.
The correct management is environmental and supportive. Move the child to a quiet, low-stimulation area, reduce the audience to essential staff, speak calmly and reassuringly, and avoid restraint and confrontation. One-to-one nursing observes for and manages any self-injury, and the precipitant — an argument, a distressing disclosure, an unrecognised stressor — is gently sought and, where possible, removed. [7] Intravenous access is secured only if genuinely needed, and fluids and routine bloods are directed at the clinical question rather than reflexively ordered.
The distinction from convulsive status epilepticus is made on the semiology and, where available, on the electroencephalogram, and it is not always easy in the heat of the moment. A reasonable principle is that an attack still running beyond five minutes in a known epileptic is managed as status epilepticus until proven otherwise, while a prolonged, variable, eyes-closed attack in a known or suspected functional-seizure patient is managed supportively. When the diagnosis is genuinely unclear, a small dose of a benzodiazepine that promptly and completely terminates a stereotyped convulsion points back toward epilepsy, while an attack that continues unabated through adequate sedation points toward a functional origin. [1]
Management — Definitive & Stepwise
Definitive management is a sequence, and the order matters. The diagnosis must first be made positively and then delivered well, the unnecessary antiseizure drugs withdrawn, the psychological therapy begun, the comorbidities treated, and the child supported back into school and normal life. [3]
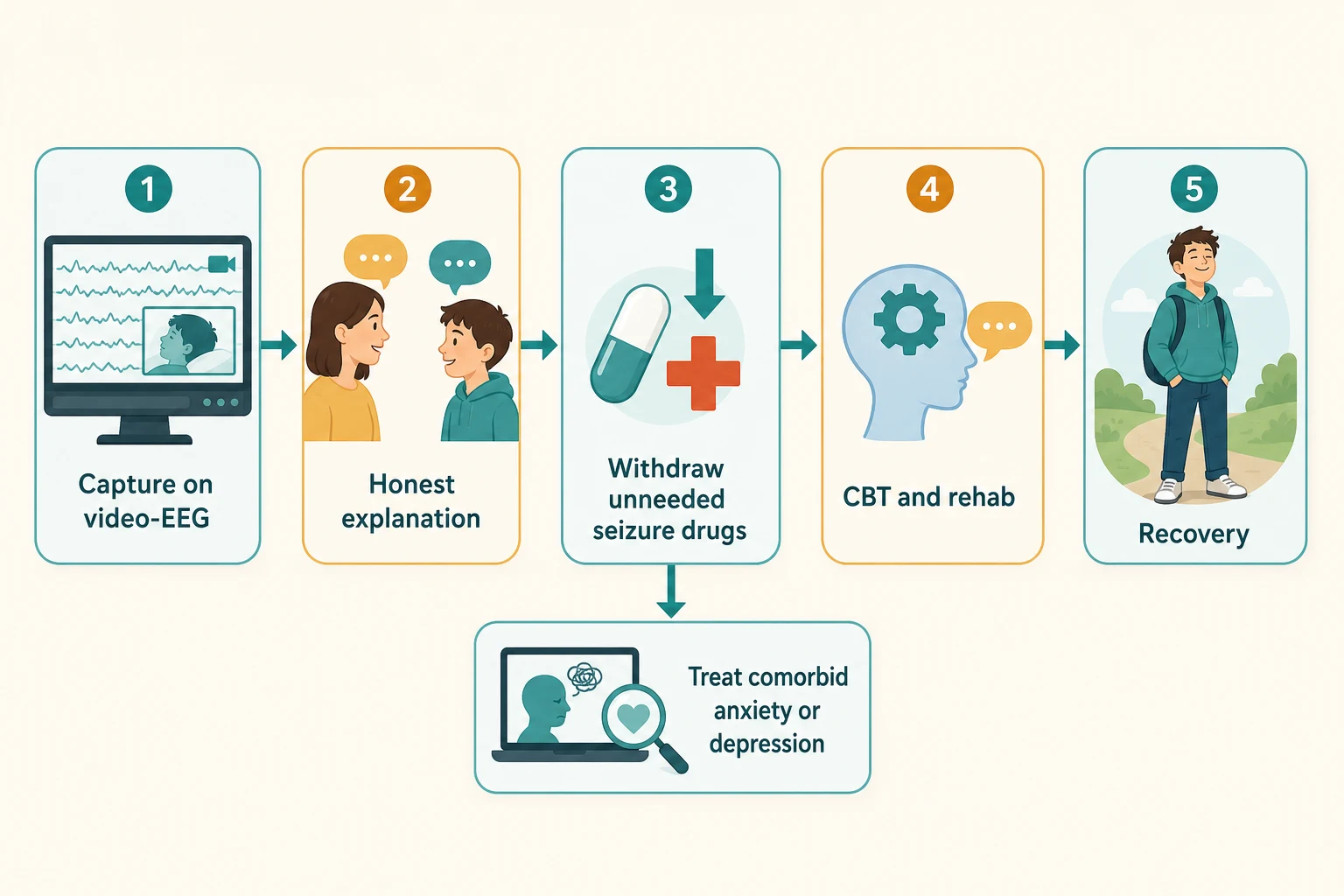
The first step is the explanation, and it is therapeutic in its own right. The clinician tells the child and family, without stigma and without minimising, that the attacks are real, that they are involuntary, that they are not epilepsy, and that the electroencephalogram has proven this. A good explanation names the condition, removes the frightening uncertainty, hands the agency for recovery back to the young person, and is the single intervention most strongly associated with a reduction in events. [8]
The second step is the supervised withdrawal of antiseizure medication that the child never needed. A drug given for a misdiagnosis of epilepsy provides no benefit, carries cognitive and behavioural side effects, and reinforces the wrong illness narrative, so it is tapered carefully under supervision — never abruptly — once the diagnosis is secure. [5] Where genuine epilepsy coexists, the antiseizure drug is continued for the epileptic events and withheld from the functional ones, and the family is taught to tell the two apart.
No antiseizure medication (first-line for a functional seizure)
Dose
None — withdraw any antiseizure drug that was started for a misdiagnosis, under supervised taper; an antiseizure drug does not treat functional seizures and is harmful
The third step is psychological therapy, with cognitive behavioural therapy as the first-line approach. The CODES trial in adults showed that cognitive behavioural therapy plus standardised medical care reduced seizure frequency more than standardised medical care alone, and the approach is extended to young people with adaptation to age and developmental stage. [10] Therapy addresses the perpetuating factors — the unrecognised mood and anxiety disorders, the avoidance and the illness behaviour, the unresolved adversity — and teaches the young person to recognise and interrupt the warning signs of an attack.
The fourth step is the multidisciplinary layer and the treatment of comorbidity. Physiotherapy and occupational therapy help re-establish normal movement and confidence where functional weakness or avoidance has set in, a graded return to school and activity reverses deconditioning and isolation, and a comorbid moderate or severe depression or anxiety disorder is treated in its own right, with an SSRI such as fluoxetine prescribed per the local paediatric formulary alongside psychological therapy when indicated. [9] Family work supports the parents to respond to attacks with calm reassurance rather than emergency escalation.
Specific Subtypes & Scenarios
The child with both epilepsy and functional seizures is the subtype that punishes the unwary. Around one in five to one in three affected young people carry both diagnoses, and the two are managed in parallel: the antiseizure drug for the epileptic events, the therapy and drug withdrawal for the functional ones. [12] The family is taught to distinguish the attacks by their semiology, a rescue plan is written for the epileptic events alone, and the clinician resists the temptation to attribute every attack to a single mechanism.
The adolescent who arrives in emergency with a prolonged flurry of functional attacks is managed as set out above — calm environment, reassurance, observation, and avoidance of escalating sedation. The episode usually settles as the arousal and audience reduce, and the admission is used to make the diagnosis, to begin the explanation, and to arrange the outpatient pathway rather than to escalate medical treatment. [7]
The child with a background of abuse, neglect or family breakdown carries the heaviest burden and the highest stakes. The functional seizure is often the visible signal of an unspoken distress, and a sensitive trauma history and a safeguarding assessment are part of the work-up, not an optional extra. [2] Disclosure may emerge only once trust is established, and the clinician's role is to hold the safeguarding lens steadily and to involve the appropriate child-protection and mental-health services.
The child with a neurodevelopmental condition or established neurodisability presents differently and is more easily mislabelled. The semiology may be harder to elicit, the comorbid epilepsy commoner, the communication of distress harder, and the response to standard cognitive behavioural therapy less straightforward. Adapted psychological and behavioural input, close work with the family and school, and a lower threshold for multidisciplinary involvement are the keys, and the diagnosis is no less valid for being harder to reach. [8]
Complications & Pitfalls
The complications of a functional seizure are largely the complications of its mismanagement. A child labelled with refractory epilepsy accumulates years of ineffective and toxic antiseizure medication, repeated emergency attendances, unnecessary investigations, driving and occupational restriction, stigma, and lost schooling. The iatrogenic harm of an emergency-department anaesthetic given for status non-epilepticus is real and occasionally fatal, and it is entirely avoidable. [5]
The diagnostic pitfalls are the mirror image of the semiology. Frontal-lobe epilepsy is dismissed as a functional attack because of its bizarre brief movements and normal scalp electroencephalogram. Convulsive syncope is labelled a seizure because of its brief jerks. A prolonged, variable, eyes-closed attack is labelled status epilepticus and over-sedated. And coexisting epilepsy is missed because the functional seizure is assumed to explain every event. The investigative pitfalls are reading a normal interictal electroencephalogram as proof, relying on prolactin, imaging every child, and failing to capture a typical event. [1]
Prognosis & Disposition
The prognosis for children and adolescents with functional seizures is better than for adults, and it depends above all on early diagnosis and engagement. Young people who receive a clear explanation, who withdraw unnecessary medication, and who engage with cognitive behavioural therapy and multidisciplinary rehabilitation achieve event-freedom in a clear majority, and the gains hold when comorbid mood and anxiety disorders are treated and schooling is restored. [7]
The prognosis is least favourable where the diagnosis is delayed, where antiseizure medication continues, where comorbid depression or anxiety goes untreated, and where the precipitating adversity remains unresolved. [3] Each year of delay adds another ineffective drug and another layer of illness behaviour, and the longer the attacks run the harder they are to interrupt — which is why prompt diagnosis and a confident explanation are themselves treatment.
Disposition is shared care. The general paediatrician or paediatric neurologist holds the medical narrative, confirms the diagnosis, withdraws the unnecessary drug, and coordinates the return to school. Child and adolescent mental-health services deliver the cognitive behavioural therapy and treat the comorbid mood, anxiety and trauma disorders. Physiotherapy and occupational therapy support rehabilitation where functional weakness or avoidance has set in, and the school is briefed and supported to manage any further event calmly rather than as an emergency. [8]
Special Populations
Children in out-of-home care, in youth-justice settings, and from backgrounds of abuse, neglect, family violence and socioeconomic disadvantage carry a higher burden of the adversity that drives functional seizures, and they are over-represented among those whose diagnosis is delayed. A trauma-informed assessment, a low threshold for a safeguarding review, and equitable access to video-electroencephalogram monitoring and psychological therapy are the priority, because a late or missed diagnosis in this group compounds existing disadvantage with the burden of unnecessary treatment and stigma. [2]
Indigenous Australian, Maori, Pacific, and migrant and refugee children face additional barriers — language and cultural distance in the consultation, limited access to specialist monitoring and child mental-health services in rural and remote areas, and a healthcare encounter that can feel stigmatising rather than supportive. Culturally safe communication, interpreter use, and engagement with the family and community are part of the diagnostic conversation, and the explanation and therapy must be delivered in a way that the young person and family can actually take up. [3]
Children with neurodevelopmental conditions, learning disability or established complex chronic neurological illness present a particular challenge. The semiology is harder to characterise, comorbid epilepsy is commoner, the communication of distress is harder to read, and standard cognitive behavioural therapy may need adaptation. The diagnosis is no less valid, and a multidisciplinary, family-centred approach with adapted behavioural and psychological input gives the best chance of recovery. [8]
Evidence, Guidelines & Regional Differences
The evidence base for functional seizures is anchored by the CODES trial of cognitive behavioural therapy for adults with dissociative seizures, which demonstrated a reduction in seizure frequency with therapy over standardised medical care alone, and by the LaFrance multicentre pilot treatment trial, which informed the pharmacological and psychological approach. [10] [9] The conceptual framework draws on the modern functional neurological disorder literature, which reframes the condition as a disorder of nervous-system function with measurable neurobiological correlates, and on the DSM-5 criteria for conversion disorder. [4] [11]
The paediatric evidence is thinner than the adult evidence and is largely extrapolated, because the major trials recruited adults. The principles of positive diagnosis, compassionate explanation, drug withdrawal and cognitive behavioural therapy are nevertheless stable across guidelines, and the consistent finding that children do better than adults when diagnosed and treated early supports a low threshold for video-electroencephalogram monitoring in the young person with refractory spells. [7] [8]
Controversies persist around the role of suggestion during monitoring, the place of antidepressant medication, and the boundary between functional seizures and the wider somatic symptom and dissociative disorders, but the consensus that an antiseizure drug is the wrong treatment and that cognitive behavioural therapy is the right one is firm across regions. [5]
Exam Pearls
Three rules that mark a fellowship answer
The high-yield minutiae an examiner rewards: a functional seizure is a real, involuntary, non-epileptic attack within functional neurological disorder; the gold-standard test is video-electroencephalogram capture of a typical event with a normal ictal recording; the semiology is eyes closed and resisted, variable thrashing, prolonged duration, pelvic thrusting and rapid full recovery; antiseizure drugs do not work and should be withdrawn under supervision; coexisting epilepsy is found in around one in five to one in three; status non-epilepticus is managed with calm and observation rather than sedation; cognitive behavioural therapy is the first-line treatment on the CODES evidence; and children carry a better prognosis than adults when the diagnosis is made early and the comorbidities are treated. [7] [10]
References
- [1]Leibetseder A; Eisermann M; LaFrance WC Jr; et al How to distinguish seizures from non-epileptic manifestations Epileptic Disord, 2020.PMID 33399092
- [2]Doss JL; Robinson JO; et al Psychogenic non-epileptic seizures in youth: Individual and family psychiatric characteristics Front Psychiatry, 2022.PMID 36590633
- [3]Gasparini S; Beghi E; Ferlazzo E; et al Management of psychogenic non-epileptic seizures: a multidisciplinary approach Eur J Neurol, 2019.PMID 30300463
- [4]Espay AJ; Aybek S; Carson A; et al Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders JAMA Neurol, 2018.PMID 29868890
- [5]Lopez MR; LaFrance WC Jr Treatment of Psychogenic Nonepileptic Seizures Curr Neurol Neurosci Rep, 2022.PMID 35674871
- [6]Hallett M; Aybek S; Dworetzky BA; et al Functional neurological disorder: new subtypes and shared mechanisms Lancet Neurol, 2022.PMID 35430029
- [7]Patel H; Blake H; Dunn D Psychogenic Nonepileptic Seizures in Children and Adolescents Indian Pediatr, 2021.PMID 33713062
- [8]Albert DVF; Voeller K; et al Psychogenic Nonepileptic Seizures in Children and Adolescents Semin Pediatr Neurol, 2022.PMID 35450667
- [9]LaFrance WC Jr; Baird GL; Barry JJ; et al Multicenter pilot treatment trial for psychogenic nonepileptic seizures: a randomized clinical trial JAMA Psychiatry, 2014.PMID 24989152
- [10]Goldstein LH; Robinson EJ; Mellers JDC; et al Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial Lancet Psychiatry, 2020.PMID 32445688
- [11]Spiegel D; Lewis-Fernandez R; Lanius R; et al Dissociative disorders in DSM-5 Annu Rev Clin Psychol, 2013.PMID 23394228
- [12]Hamed SA; Attiah FA; Fawzy M Psychogenic nonepileptic seizures in adults with epilepsy: a tertiary hospital-based study Int J Neurosci, 2020.PMID 31771384