Paeds · preventive-and-community-paediatrics
School-age health supervision
Also known as School-age well child visit · Primary school health supervision · Middle childhood preventive care · Bright Futures school age
Fellowship guide to school-age health supervision: well-visit structure, growth and BMI, vision hearing BP and oral screens, sleep media activity guidance, school function, safeguarding gates and regional preventive frameworks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
S.C.H.O.O.L. A.G.E.
Overview & Definition
Picture an eight-year-old who “only needs a school form.” That request is your doorway, not your job description. School-age health supervision means planned preventive care across roughly the primary-school years (about 5–12 years). You protect growth, senses, teeth, sleep, movement, mental health and learning. You also catch problems early enough that school does not become the first diagnostician. [1] [2]
A well visit differs from a sick visit. The well visit asks what is going well, what is changing, and what risk is still silent. The sick visit answers an acute complaint. Both can share a room on the same day, but you must name which mode you are in. If the child looks unwell, you stop “form mode” and enter assessment for threat. [23] [24]
Bright Futures–style periodicity schedules list visit components: history, measurements, sensory screening, physical examination, procedures, oral health and anticipatory guidance. Your service may use a different booklet or school-nursing model. The principle stays the same: universal tasks for every child, selective tasks for risk, and immediate conversion when danger appears. [1] [2]
This leaf stops at the preventive framework. Full ADHD pharmacology, obesity drug pathways, adolescent confidential sexual health and complete immunisation tables live in linked topics. You still need enough of each to know when to screen, refer and safety-net. [5] [3]
Classification
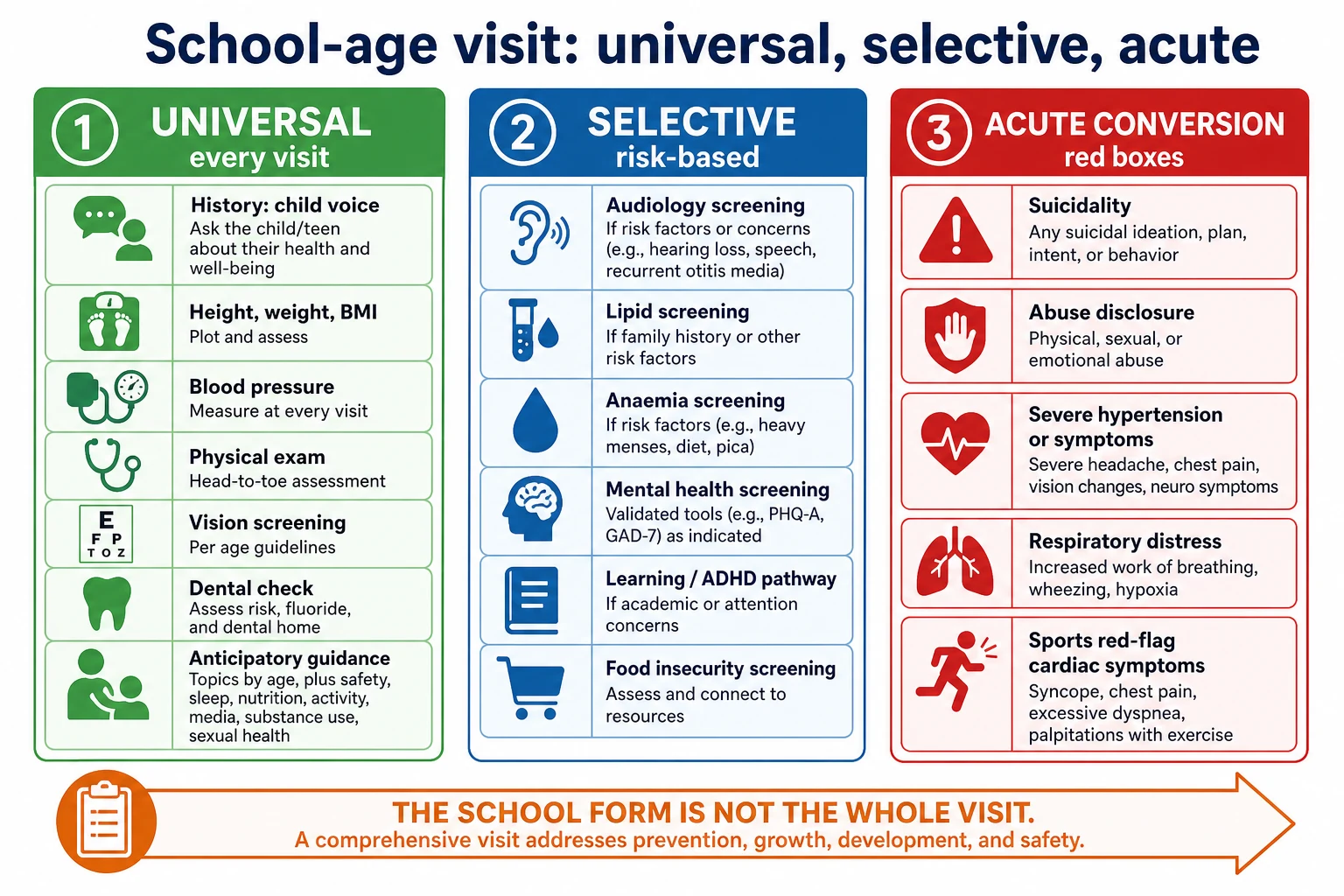
Sort every school-age encounter into three buckets before you open the laptop. [1]
Universal care happens at routine visits for almost every child: child-centred history, height and weight with BMI-for-age, blood pressure with a correct cuff, physical examination, vision screening pathway, dental inspection and fluoride advice, immunisation status check, and anticipatory guidance on sleep, media, activity, safety and school. [1] [9]
Selective or risk-based care follows clues: formal audiology, deeper mental-health tools, learning/ADHD pathway steps, food-insecurity support, lipids or glucose testing only when indicated by age and risk policy, and targeted social work or safeguarding assessment. Do not order a “well-child panel” for comfort. [3] [11] [5]
Acute conversion is the third bucket. Suicidal talk, abuse disclosure, respiratory distress, symptomatic severe hypertension, or cardiac red flags before sport mean you leave the periodicity checklist and treat threat first. [12] [15] [13]
Classify the visit purpose as well: school entry, annual well care, sports preparticipation, foster-care catch-up, or teacher-driven concern. Purpose changes time allocation, not your duty to see the whole child. [15] [14]
Epidemiology & Risk Factors
Middle childhood looks “healthy” until you measure. Overweight and obesity are common enough that BMI screening is a core task, not a special interest. Untreated refractive error, dental caries, sleep restriction, low activity and bullying quietly erode grades and mood. Asthma, eczema and allergic disease often still need plan updates at school age. [3] [17] [12]
Poverty and food insecurity change everything you hear about diet and “picky eating.” Ask about running out of food without shame. Link families to resources rather than lecturing plate diagrams. [11] Racism, housing stress and parental mental illness raise the chance that school notices behaviour before clinic notices trauma. [13] [14]
Disability, autism and medical complexity increase missed dental and vision care, school exclusion risk and caregiver load. Plan longer visits and adapted examination. [18] Migrant and refugee children often carry incomplete immunisation records, caries and interrupted schooling. Use interpreters; do not use children as translators for sensitive content. [20]
Out-of-home care multiplies placement moves and lost paperwork. Assume gaps until proven otherwise. Rural families may pass school van screens that never reach the medical home unless you close the loop. [14] [1]
Pathophysiology
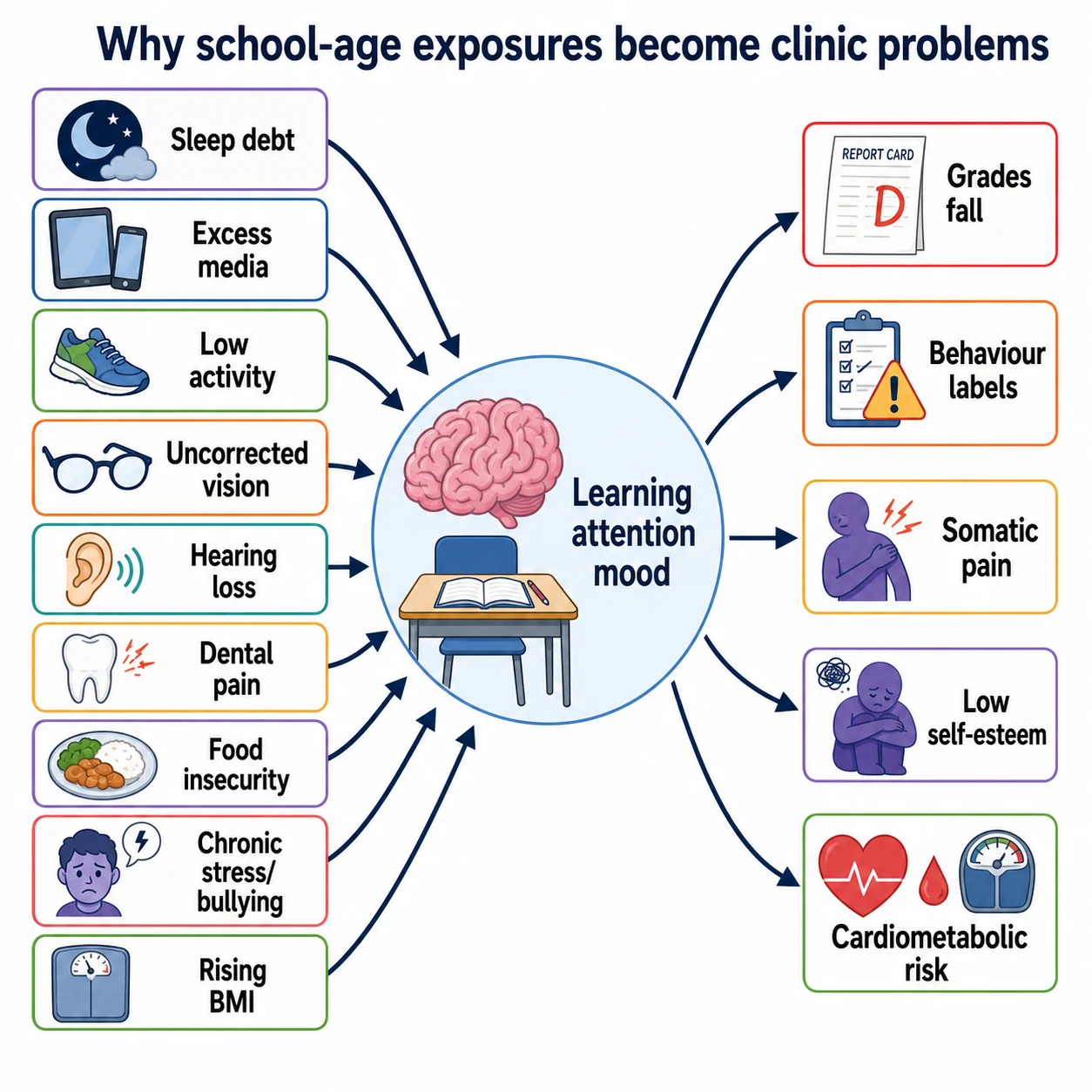
School function is a physiology problem as much as a classroom problem. Sleep debt shortens attention and inflames mood. The American Academy of Sleep Medicine consensus sets age-banded sleep needs; many school-age children miss them on school nights. [8]
Uncorrected refractive error forces the brain to work harder for print. The child looks “lazy” at homework while the true lesion sits in optics. Hearing loss fragments instruction and social cues. Dental pain steals sleep and concentration. None of these children look septic. All of them fail quietly. [4] [9]
Energy imbalance and obesogenic environments drive rising BMI. Stigma then adds a second injury: shame that blocks help. [17] [16] Chronic stress and bullying load the threat system. Somatic pain, school refusal and depression can follow. [12] [13]
Low moderate-to-vigorous activity and high sedentary time couple with cardiometabolic risk across childhood. WHO and US activity guidelines both centre a daily movement target for ages 5–17 years. [6] [7]
Mid-childhood growth still needs serial plotting. Adiposity rebound and channel crossing tell a story one weight cannot tell. Use validated charts and correct technique; details live in the growth topic, but the preventive visit owns the decision to plot and act. [26]
Clinical Presentation
The classic presentation is no presentation: “She’s fine. We need the form.” Your skill is to open the child’s world in five minutes. Ask what they like at school, who they sit with, how sleep feels, and what worries them. Then ask the caregiver what teachers say. [1]
Vision problems may show as rubbing eyes, holding screens close, headaches after reading, or avoiding close work. Hearing problems may show as loud TV, “ignoring” instructions, or lingering speech issues. Learning difficulty may arrive as homework wars, lost books or a teacher email you have not yet read. [4] [5]
Anxiety often wears a stomach-ache costume on school mornings. Depression may look like irritability, boredom or dropping clubs. Bullying may present as missing belongings, unexplained bruises or sudden phone fear. Obesity may be invisible to the family if “everyone looks like this.” [12] [16]
Medical complexity presents as therapy backlog, school absence and emergency-plan drift. Caregiver exhaustion is part of the clinical picture. [18] Caregiver concern that something is wrong deserves weight even when the chart looks tidy. [23]
Differential Diagnosis
When a teacher says “ADHD,” do not jump to stimulant talk. First separate sleep debt, vision or hearing problems, learning disorder, trauma response, absence seizures, anxiety and true ADHD patterns across settings. The AAP ADHD guideline expects a systematic school-age evaluation, not a single noisy clinic hour. [5] [8]
For rising weight, separate common energy-balance obesity from red-flag patterns such as poor linear growth with rapid gain, severe headaches, or other endocrine clues. Most children need family-based support, not a rare-disease chase. Still, do not miss the uncommon. [3] [17]
School refusal is not one disease. Rank medical illness, anxiety, learning shame, bullying, family chaos and, less often, fabricated or induced illness concerns. Chronic abdominal pain needs red-flag gates for organic disease, then a functional pathway when appropriate. [12] [13]
Injury narratives must fit developmental stage and injury pattern. Keep safeguarding open without turning every bruise into an accusation. Trauma-informed care means curiosity, privacy and safety first. [13] [14]
Clinical & Bedside Assessment
Start with seating and voice. Greet the child by name. Sit at their eye level. Let them speak before the adult fills silence. As age rises toward secondary school, create brief private time for sensitive questions with consent principles you can defend. [21] [1]
Measure standing height and weight with shoes off when possible. Calculate BMI and plot BMI-for-age on the chart your service uses. Look at trend, not a single label shouted across the room. Measure blood pressure with a cuff that fits. Wrong cuff size invents disease. [26] [3]
Examine skin, teeth, palate, lymph nodes, chest, heart, abdomen, spine and gait. Note pubertal signs without embarrassment theatre. Check for untreated caries, tonsillar bulk with sleep snoring history, and musculoskeletal pain that limits sport. Age-banded vital-sign context still matters when the “well” child looks off. [9] [24]
Screen vision with the best validated method your clinic can perform and refer on local thresholds. USPSTF evidence is strongest in younger ages for routine vision screening statements; school-age practice still treats vision as essential for learning and continues screening pathways used by your health system and schools. Do not invent acuity cut-offs in a viva if you cannot name the source. [4]
Ask hearing risk questions and act on failed school screens. Inspect teeth and counsel fluoride and dental home access. [9] Screen sleep hours and quality, media patterns, activity minutes, nutrition and food security, helmet and water safety, online safety, bullying and mood. [8] [10] [11] [12]
Use professional interpreters for language discordance. Trauma-informed examination means explain touch before you touch, offer choices, and stop when fear rises. [20] [14]
Investigations
Most thriving school-age children need few laboratory tests at a well visit. The investigation is often the measurement itself: growth chart, BMI trend, BP, vision screen and school information. [1] [3]
Order selective tests when history and examination change pre-test probability. Examples include audiology after failed screens, dental referral for caries, psychology or developmental-behavioural pathways for learning collapse, and metabolic tests only under guideline-aligned risk rules you can cite. Avoid shotgun panels that create incidental cascades. [5] [3]
Immunisation records are data. If the history is uncertain, plan catch-up with the dedicated immunisation topics and national schedules rather than guessing doses from memory. [1] [2]
School van results are not a diagnosis until you confirm and act. Document abnormal screens, referrals and who owns follow-up. Structured handoff reduces dropped balls when many adults share the child. [25]
Management — Resuscitation
“Resuscitation” in preventive clinic means recognising that the well-visit shell can hide an emergency. [12]
If the child discloses active suicidal ideation or ongoing abuse, you do not finish the BMI speech first. Ensure immediate safety, follow local mental-health and safeguarding pathways, and do not send the child back into danger with a smile and a pamphlet. [12] [13]
If the child arrived for a form but shows respiratory distress, altered consciousness, severe pain or symptomatic hypertension, stabilise and escalate as for any acute presentation. Caregiver concern that “this is not my child” can be the earliest warning. [23] [24]
Sports clearance with exertional syncope, chest pain with exercise, or a first-degree relative with premature sudden cardiac death is not a rubber stamp. Pause clearance and investigate or refer along cardiac pathways. [15]
Management — Definitive & Stepwise
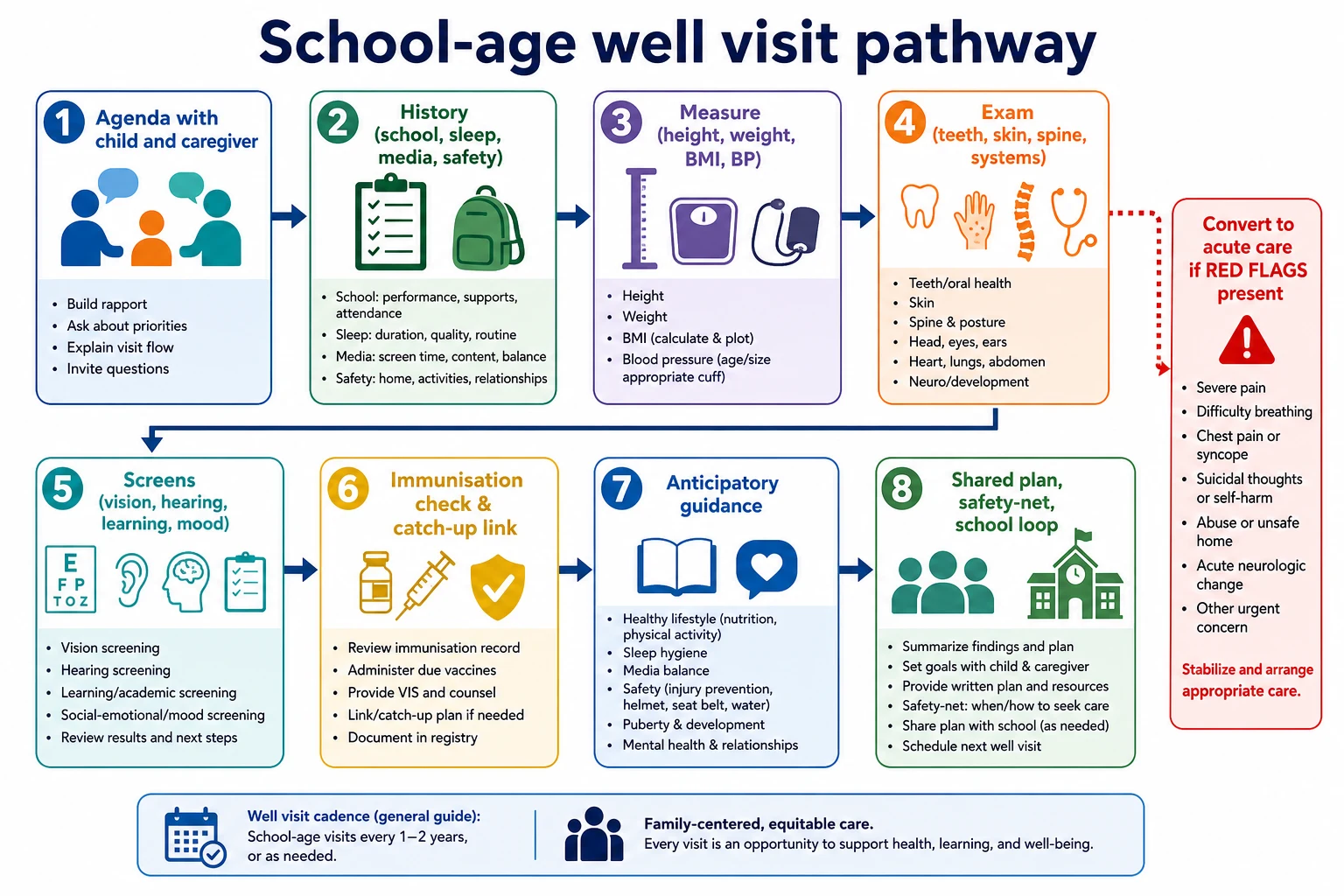
Run the visit as a pathway you can teach a registrar in one minute. [1]
- Agenda. Child goals, caregiver goals, school forms, hidden worries.
- History. School, friends, sleep, media, food, activity, mood, bullying, safety, medicals, medicines, allergies, family.
- Measures. Height, weight, BMI trend, BP, plot.
- Examination. Age-adapted head-to-toe with teeth and spine.
- Screens. Vision pathway, hearing risk, learning/mood tools as indicated, dental, food security.
- Prevention procedures. Immunisation status; catch-up plan if needed (linked topic).
- Guidance. Sleep targets, media rules, daily activity, helmets, dental fluoride, reading for pleasure, online safety.
- Plan. What you will do, what family will do, what school needs, when to return, red flags. [1] [2] [22]
Sleep. Use AASM consensus bands: many children aged 6–12 years need 9–12 hours per 24 hours; teenagers differ. Ask about bedtime screens and snoring. [8] [10]
Activity. Counsel toward at least 60 minutes per day of moderate-to-vigorous physical activity for ages 5–17 years, plus less recreational sedentary time, aligning with US Physical Activity Guidelines and WHO summaries. Make it playable, not a gym sentence. [6] [7]
BMI and weight talk. Screen for obesity and offer behavioural support pathways consistent with USPSTF direction to screen and intervene. Speak about health habits and strength. Never mock body size. Stigma is iatrogenic harm. [3] [16]
Learning and ADHD pathway. Gather caregiver and teacher perspectives across settings. Use structured evaluation principles from the AAP ADHD CPG. Treat sleep and senses first when they are broken. Refer when complexity exceeds primary-care skill. [5]
Oral health. Promote dental home, brushing, and fluoride according to primary-care caries-prevention guidance. Fluoride varnish and dosing details follow local protocol and Clark AAP guidance rather than memory theatre. [9]
Media. Agree family media plans: device-free sleep space, content quality, and offline play. Policy summaries support limits and adult engagement, not only a single magic number shouted without context. [10]
School loop. With consent, share actionable health information with school nurses or learning support. Write clear plans for asthma, anaphylaxis risk, ADHD supports or toileting needs. Handoff quality matters. [25] [18]
Specific Subtypes & Scenarios
School entry (about 5–6 years). Focus readiness, vision and hearing, immunisation gaps, toileting confidence, separation anxiety and dental eruption of permanents. Align forms with national school-entry rules without letting paperwork erase the exam. [1] [4]
Thriving 8-year-old with rising BMI. Plot trend, take diet and activity history without blame, screen food security, set family goals, book earlier review, and avoid shame. [3] [11] [16]
Teacher ADHD concern with poor sleep. Fix sleep opportunity and screens, check vision and hearing, collect school rating information, then decide on ADHD evaluation timing. [5] [8]
Autism or intellectual disability. Adapt sensory load, use plain language, allow caregiver facilitation, update school supports, and watch for diagnostic overshadowing of pain or seizures. [18] [19]
Refugee child with incomplete records. Interpreter, catch-up prevention, dental and vision priority, trauma-informed pacing, and school enrolment support. [20] [13]
Foster care catch-up. Assume missing dental, vision and mental-health care. Clarify consent. Document thoroughly for the next placement. [14] [13]
Preparticipation evaluation. Use PPE structure: history first (symptoms, family cardiac history, concussion, asthma, bleeding, menstrual concerns in older girls), then focused exam. Clear only when risk is addressed. [15]
Rural telehealth hybrid. History and guidance online; insist on in-person measures and vaccines when the question needs hands and calibrated devices. [1]
Complications & Pitfalls
The classic pitfall is treating the form as the patient. Another is diagnosing ADHD with a 12-minute history and no school data. [5]
Shame-based obesity talk drives avoidance and worsens outcomes. Stigma is documented harm, not a motivational tool. [16] Missing sleep and media as reversible drivers creates false disease labels. [8] [10]
Clearing sport without cardiac symptom review is a safety failure. Ignoring interpreter need is a safety failure. Dropping abnormal school screens with no owner is a system failure. [15] [20] [25]
Documenting sensitive disclosures in shared portals without thought can breach trust. Follow local privacy rules and consent guidance. [21]
Prognosis & Disposition
Good school-age supervision changes trajectories: earlier glasses, restored sleep, fewer caries, safer sport, faster learning support, and less entrenched bullying harm. Disposition is usually home with a dated review. Intensify follow-up for BMI, BP, mood, safeguarding or learning pathways. [3] [12] [22]
Same-day emergency or urgent specialist care is for threat, not for paperwork convenience. Safety-net in plain language: what school changes, what pain or mood signs, when to return before the next annual visit. Written advice helps. [22]
As children approach secondary school, begin the shift toward more private interviewing and adolescent preventive care without abandoning caregiver partnership. [1] [21]
Special Populations
Medical complexity. Define baseline, update emergency plans, coordinate therapies, and fight unnecessary school exclusion. Complexity frameworks help teams recognise high need. [18]
Neurodiversity. Sensory-adapted rooms, visual schedules, and respect for communication differences. Do not attribute every behaviour to the diagnosis. [19] [18]
Indigenous children. Practise cultural safety, prioritise hearing and dental equity where burden is high, and partner with community-controlled services rather than parachuting advice. [1] [13]
Migrant and refugee families. Interpreters, catch-up care, nutrition transition, and trauma-aware pacing. [20] [14]
Out-of-home care. Comprehensive catch-up visits, mental-health vigilance, and meticulous records for unstable placements. [14]
Food-insecure households. Screen and link; do not prescribe expensive diets. [11]
Gender-diverse school-age children. Use affirmed names and pronouns in clinic speech. Provide ordinary excellent preventive care. Detailed gender-affirming pathways belong in dedicated topics. [21] [13]
Evidence, Guidelines & Regional Differences
AAP preventive periodicity recommendations (Hackell updates) operationalise Bright Futures components for US-influenced practice and exam answers that expect named schedules. [1] [2] USPSTF supports obesity screening in children and adolescents and behavioural interventions. [3] Vision screening evidence statements are age-specific; know the bound of the USPSTF child vision recommendation rather than inventing school-age meta-analyses. [4]
AAP ADHD 2019 guidance anchors school-age evaluation quality. [5] Activity guidance converges on daily movement for 5–17-year-olds in US and WHO sources. [6] [7] AASM sleep duration consensus remains a high-yield viva source. [8] Fluoride and media policy statements keep teeth and screens inside the paediatric lane. [9] [10]
Food insecurity, bullying–mood links, trauma-informed care and PPE reviews complete the community frame. [11] [12] [13] [14] [15] Obesity sits inside wider commercial and environmental drivers, not only “willpower.” [17]
Controversies to respect: how hard to push universal lipids or BP intensity; quality of school-based ADHD labels; balancing early obesity intervention against stigma; and the evidence strength behind exact recreational screen-time cut-offs. Exam answers should show judgment, not dogma. [3] [16] [10]
Exam Pearls
- The form is a doorway; the child is the visit. [1]
- Child voice before caregiver monologue. [1]
- BMI trend, not a single shaming number. [3] [16]
- Sleep, vision and hearing before stimulant talk. [5] [8]
- About 60 minutes daily MVPA for 5–17 years (US/WHO direction). [6] [7]
- AASM: many 6–12-year-olds need 9–12 hours’ sleep. [8]
- Fluoride and dental home are paediatric work. [9]
- PPE is history-heavy risk triage, not a stamp. [15]
- Teacher concern is data; caregiver concern is data. [5] [23]
- Safety-net school change: grades, friends, sleep, mood, injuries. [22]
References
- [1]Hackell JM 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [2]Hackell JM 2021 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2021.PMID 33593848
- [3]Grossman DC Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2017.PMID 28632874
- [4]Grossman DC Vision Screening in Children Aged 6 Months to 5 Years: US Preventive Services Task Force Recommendation Statement. JAMA, 2017.PMID 28873168
- [5]Wolraich ML Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics, 2019.PMID 31570648
- [6]Piercy KL The Physical Activity Guidelines for Americans. JAMA, 2018.PMID 30418471
- [7]Chaput JP 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. The international journal of behavioral nutrition and physical activity, 2020.PMID 33239009
- [8]Paruthi S Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine, 2016.PMID 27250809
- [9]Clark MB Fluoride Use in Caries Prevention in the Primary Care Setting. Pediatrics, 2020.PMID 33257404
- [10]Hauk L Use of Media by School-Aged Children and Adolescents: A Policy Statement from the AAP. American family physician, 2017.PMID 28671367
- [11]Gitterman BA Promoting Food Security for All Children. Pediatrics, 2015.PMID 26498462
- [12]Kodish T Bullying, Depression, and Suicide Risk in a Pediatric Primary Care Sample. Crisis, 2016.PMID 27040126
- [13]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [14]Marsac ML Implementing a Trauma-Informed Approach in Pediatric Health Care Networks. JAMA pediatrics, 2016.PMID 26571032
- [15]MacDonald J The Preparticipation Physical Evaluation. American family physician, 2021.PMID 33929170
- [16]Pont SJ Stigma Experienced by Children and Adolescents With Obesity. Pediatrics, 2017.PMID 29158228
- [17]Lobstein T Child and adolescent obesity: part of a bigger picture. Lancet (London, England), 2015.PMID 25703114
- [18]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [19]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [20]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [21]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [22]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [23]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [24]Fleming S Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [25]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [26]Kuczmarski RJ 2000 CDC Growth Charts for the United States: methods and development. Vital and health statistics. Series 11, Data from the National Health Survey, 2002.PMID 12043359