Paeds · preventive-and-community-paediatrics
School health and school-based care
Also known as School-based health · School nursing and paediatric care · School health plans · School-based health centres · School medical interface
Fellowship guide to school health and school-based care: school nursing and SBHC models, executable chronic-disease and emergency plans, return-to-learn after concussion, infection and sports outbreak principles, confidential adolescent care, and clinic–school coordination.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
S.C.H.O.O.L. plan
Overview & Definition
Picture a parent sliding a blank “school medical form” across the desk. They want a signature before Monday. Your real job is wider. School health and school-based care is the set of services, plans and partnerships that keep children safe and learning during the school day. It includes school nursing, school-based health centres (SBHCs), written emergency and chronic-disease plans, medication systems, return-to-learn after concussion, infection and sports-outbreak responses, and confidential adolescent pathways when local law allows. [1] [2]
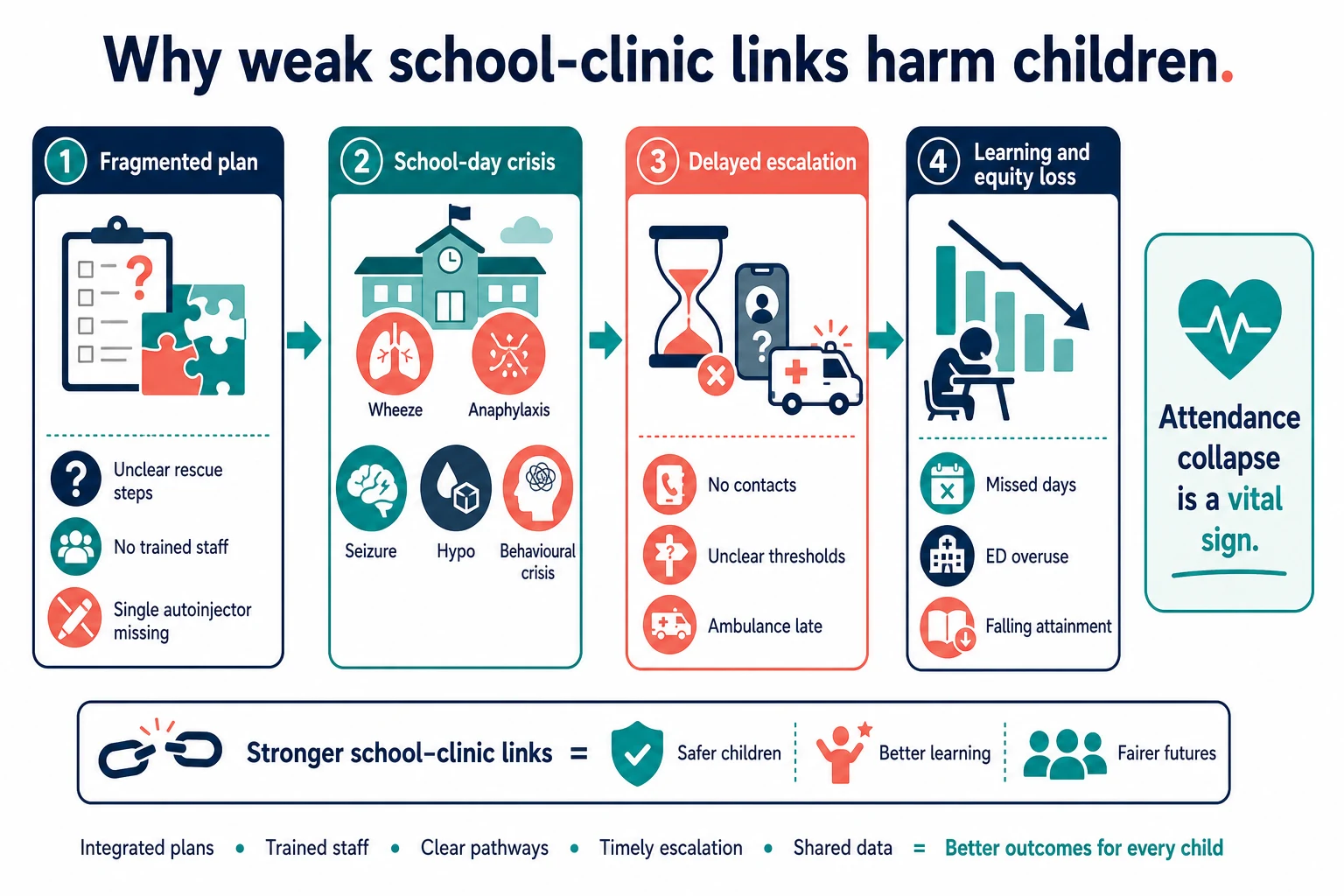
School is not a soft setting. Many children spend more supervised hours at school than in clinic. Asthma flares, anaphylaxis, seizures, hypoglycaemia, behavioural crises and post-concussion cognitive load all present there first. If the plan only lives in the hospital letter, staff cannot act when the child is blue or pale on the playground. [1] [4] [5]
This page owns the school interface. Dedicated leaves cover deep asthma, allergy immunology, diabetes technology, ADHD longitudinal care, and preschool or adolescent well-child packages. Cross-link those rather than hiding whole second chapters here. [8] [9]
Classification
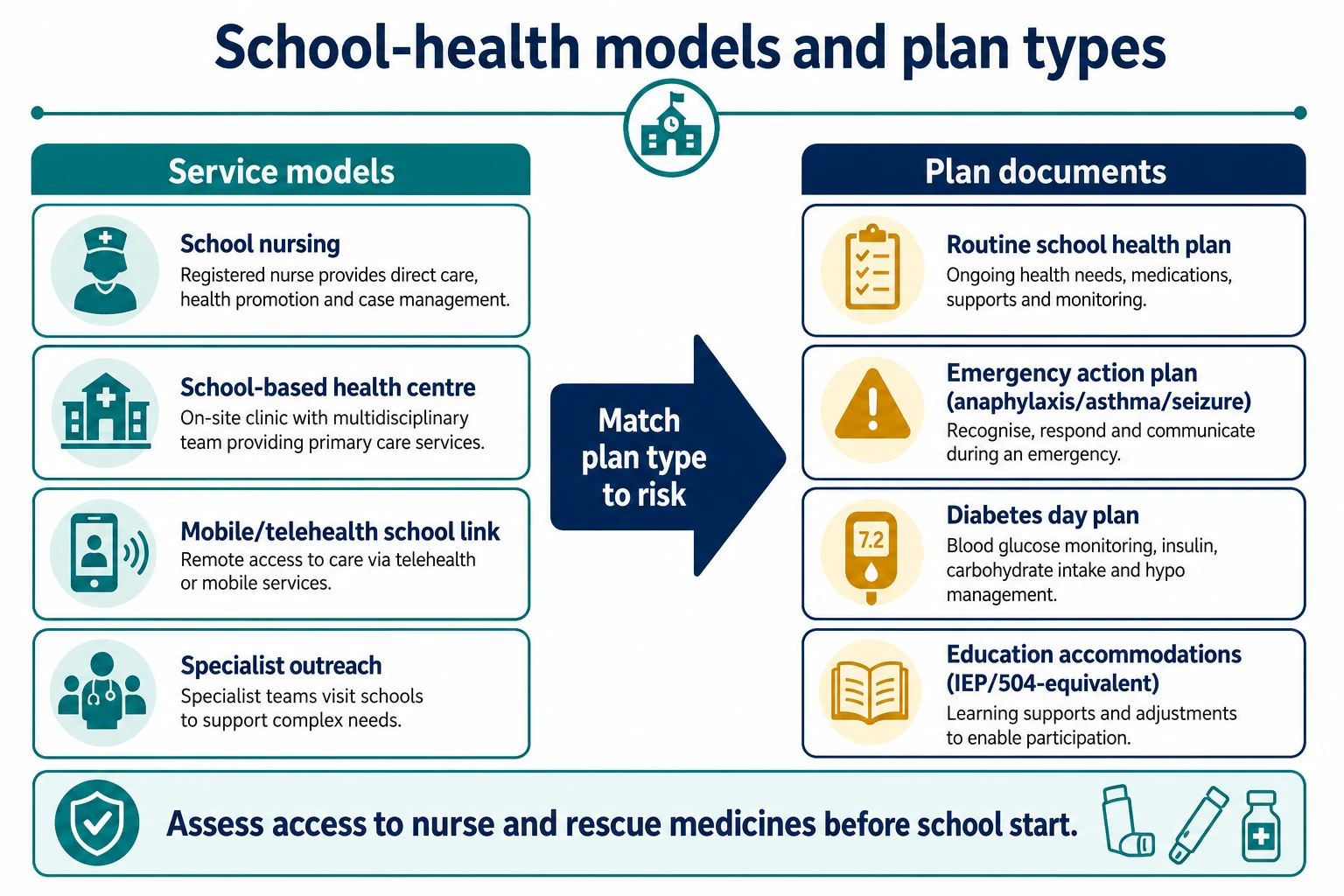
Sort school health by who delivers care, then by what document staff need. [1] [2]
Service models. School nursing (often the backbone). SBHCs that provide on-site primary care, mental health or dental services. Mobile or telehealth school links. Specialist outreach (for example diabetes educators or complex-care nurses). Coverage is uneven: never assume a registered nurse is on site every hour. [1] [2]
Plan types. Routine individual healthcare plan for day-to-day needs. Emergency action plan for anaphylaxis, asthma, seizure or adrenal crisis. Diabetes day plan covering glucose checks, insulin, hypo/hyperglycaemia and sport. Education accommodation documents (US IEP/504-equivalents or local learning-support plans) that translate medical needs into classroom adjustments. [4] [5] [6]
Integration pattern. Medical-home-led care with school implementation. SBHC as expanded medical-home access for underserved students when records and consent link back to primary care. Fragmented dual care without shared plans is a failure mode, not a model. [2] [3]
Epidemiology & Risk Factors
School-day disease burden is not abstract. Asthma, allergy, diabetes, epilepsy, ADHD and rising mental-health presentations drive nurse visits, ambulance calls and missed learning. Children in poverty, unstable housing, migrant families and out-of-home care use school-based access points more and fall through form-only systems more often. [2] [12] [19]
Workforce gaps matter. Schools without a nurse, or with one nurse across several campuses, cannot deliver the same plan fidelity as a fully staffed service. Rural and remote schools may rely on first-aid-trained staff only. Your plan must match that reality. [1]
Attendance collapse is an equity and health signal. Maternal depression and early developmental vulnerability already track with school-entry risk; later school disengagement compounds medical and social harm. Treat repeated unexplained absences as data, not “parenting style.” [20] [12]
Pathophysiology
Think in mechanisms that change Tuesday morning, not only in diagnoses. [1] [4]
Untreated school-day physiology. Bronchospasm, anaphylaxis cascade, hypoglycaemia, prolonged seizure activity and heat illness progress on a minutes-to-hours clock. Rescue medicines only help if they are present, in date, and usable by the person standing next to the child. [4] [5]
Cognitive load after concussion. After mild traumatic brain injury, attention, processing speed and visual tolerance often lag behind “looks fine on the sideline.” Full academic load too early worsens symptoms and prolongs recovery. Return-to-learn is therefore a physiologic pacing problem, not a paperwork delay. [6] [7]
Information fragmentation. When clinic, family and school hold different versions of the plan, dosing errors, delayed adrenaline and missed hypos follow. Handover quality is a safety intervention. [1] [2]
Social pathway. Food insecurity, housing instability and sleep debt present as inattention, headaches and nurse visits. Treating only the symptom without the school and social context fails the child twice. [12] [17] [19]
Clinical Presentation
You will meet school health in three common ways. [1] [2]
Form visit. “Please sign this for school.” Dig for the real problem: what medicines are needed on site, who will give them, what the last school incident was, and whether attendance or PE is already restricted. [1] [9]
School nurse call. Wheeze after sport, possible allergic reaction, seizure, low glucose, head knock, or a child who will not stop crying in the health room. Ask for vital signs, what has already been given, and whether the written plan was followed. [1] [4]
Silent presentation. Rising absences, frequent somatic complaints, falling grades after concussion, or an adolescent using the SBHC for confidential concerns. These are still clinical presentations. [2] [6]
Differential Diagnosis
School avoidance. Anxiety, bullying, learning disability, sensory overload, uncontrolled medical disease, sleep debt, depression, or unsafe home that makes school the only disclosure site. Do not label “school refusal” until medical and safeguarding screens are conscious. [8] [13] [17]
Inattention and nurse visits. ADHD is one pathway, not the only one. Sleep insufficiency, vision or hearing barriers, classroom mismatch, trauma, food insecurity and poorly controlled asthma all look like “won’t focus.” Use multi-setting history before medication changes. [8] [12] [17]
Acute collapse at school. Anaphylaxis, severe asthma, seizure, cardiac syncope, hypoglycaemia, heat illness, head injury and intoxication. ABCDE comes before form logic. [4] [5] [7]
Clinical & Bedside Assessment
Start with the child and caregiver, then the school day timeline. Ask: “What happens between 9 and 3?” Cover nurse visits, PE tolerance, playground incidents, toilet access, lunch supervision, and who holds rescue medicines. [1]
Plan audit. Read the current school plan out loud with the family. Can a teacher’s aide follow it without a medical degree? Are triggers, exact steps, contact numbers and ambulance thresholds written? Is the date current? [4] [5]
Access reality check. Is there a school nurse daily? Where are autoinjectors and inhalers stored? Can the adolescent self-carry? What happens on excursions and after-school sport? [1] [4]
Medical exam when indicated. Focused systems exam for the presenting school concern, growth and BMI when weight or PE restriction is in play, blood pressure with correct cuff size when indicated, and mental-state screening when attendance or mood has collapsed. [9] [15] [16]
Consent and voice. Speak with the child alone when age-appropriate. For gender-diverse or LGBTQ+ adolescents, privacy and respectful naming matter for engagement. Use professional interpreters — never another pupil. [14]
Investigations
Most school-plan visits need no blood test. Investigate when the school story or examination demands it. [9]
Useful when targeted. Peak-flow or spirometry trends for asthma patterns; glucose meter or continuous-glucose data downloads for diabetes day plans; formal concussion assessment tools and specialist review when recovery stalls; teacher rating scales as one input in ADHD evaluation, never the whole diagnosis. [5] [7] [8]
Not useful as form filler. Random panels because a school admin wants “bloods.” Imaging “to clear for school” without clinical indication. Labelling hypertension from one noisy school reading without confirmatory technique. [15]
Safeguarding work-up. When school discloses injuries, fearfulness or sexualised behaviour concerns, follow mandatory reporting and local child-protection pathways rather than a casual “monitor.” [13]
Management — Resuscitation
School emergencies still follow ABCDE. The difference is that the first responder may be a nurse or a trained teacher. [1] [4]
Anaphylaxis. Intramuscular adrenaline into the mid-outer thigh without delay; call emergency services; place the child supine (or sitting if breathing is the dominant problem); prepare for a second dose if still compromised; never leave the child alone after adrenaline. Written school allergy plans exist so non-specialists can do this under stress. [4]
Severe asthma. Reliever as per the child’s plan; oxygen if available; urgent transfer if not improving, speaking in single words, or tiring. [1]
Seizure. Protect from injury, time the event, do not force objects into the mouth, and give prescribed rescue medicine for prolonged seizures per the individual plan. [1]
Hypoglycaemia in diabetes. Fast carbohydrate if conscious and able to swallow; glucagon or emergency pathway if severe or unconscious, following the school diabetes plan. [5]
Behavioural or self-harm crisis. Safety first: remove immediate means, supervise, and escalate to emergency or crisis mental-health services. Do not finish paperwork while the child is unsafe. [2]
Management — Definitive & Stepwise
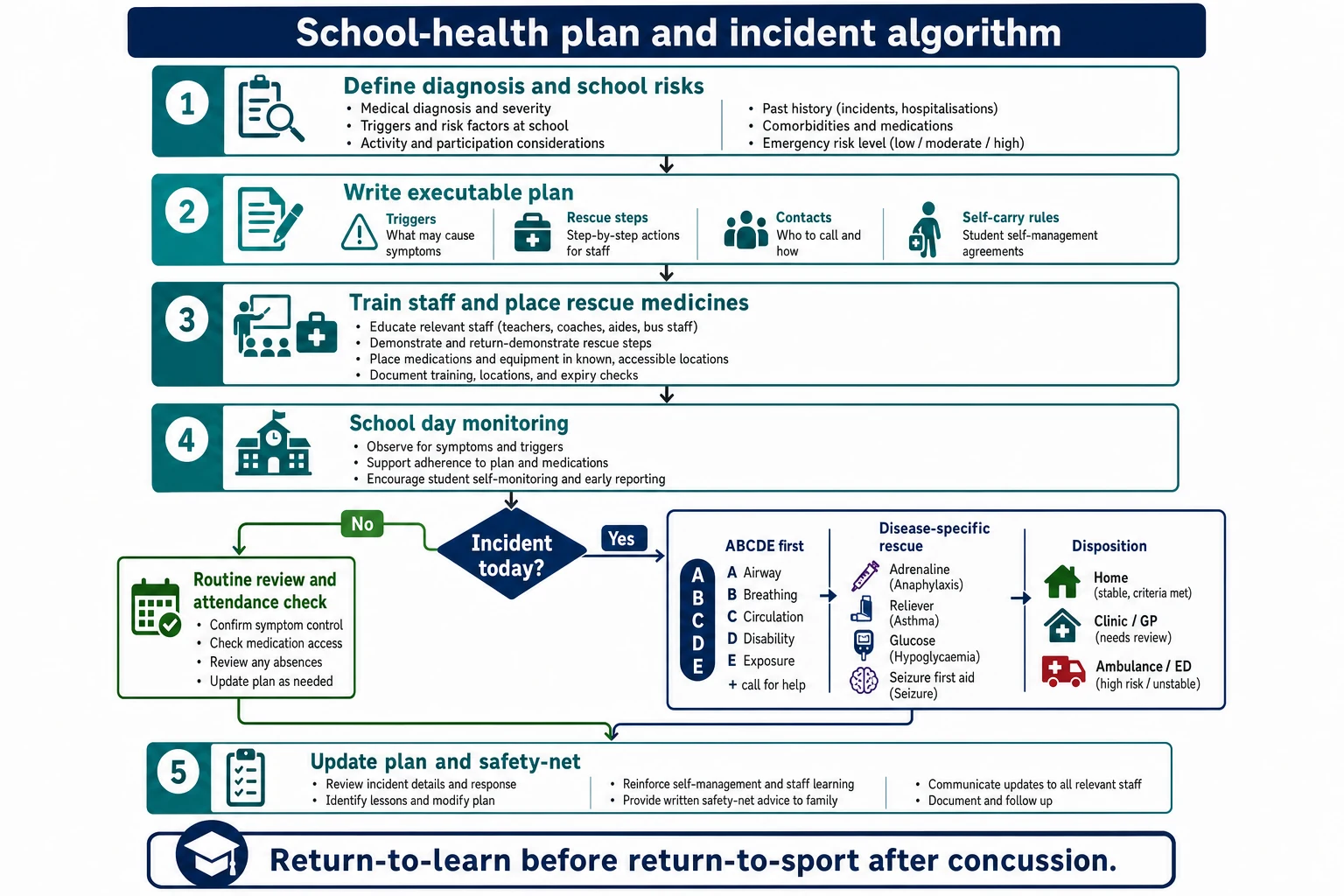
Use a repeatable sequence every time. [1] [2]
- Define the school-day risk. Diagnosis, triggers, early signs, sport and excursion needs.
- Write an executable plan. Short steps, named medicines, doses the school is authorised to give, storage, self-carry rules, contacts, and ambulance thresholds. Allergy plans should follow structured emergency-plan guidance rather than vague “give antihistamine and call mum.” [4]
- Place capacity, not only paper. Rescue medicines on site, expiry checks, and training for the people who will act. Assume staff turnover. [1] [4]
- Integrate with the medical home. SBHCs improve access when they share information and do not become a silent parallel system. [2] [3]
- Return-to-learn after concussion. Reduce cognitive load, allow breaks, delay high-stakes testing if needed, and advance stepwise as symptoms allow. Return-to-learn comes before full return-to-sport. [6] [7]
- Infection and sports outbreak principles. Follow local public-health exclusion tables rather than inventing day counts. Organised sports need hygiene, wound care and outbreak control thinking. [11]
- Immunisation and school entry. Support complete vaccination for school attendance; understand medical versus nonmedical exemption frameworks in the jurisdiction you are working in. Open the official schedule — do not invent catch-up doses from memory. [10] [9]
- Safety-net after incidents. Same-day clinic or ED criteria, plan update within days, and attendance review. [1]
Specific Subtypes & Scenarios
Asthma. School action plan, reliever access, PE warm-up and pollution/cold triggers, and when to stop sport and call for help. [1]
Food allergy and anaphylaxis. Written emergency plan, staff training, on-site adrenaline, avoidance practicalities without false promises of zero risk, and excursion planning. Two-device thinking is common clinical practice when risk is significant — confirm local prescribing norms. [4]
Type 1 diabetes. Glucose monitoring, insulin timing, hypo treatment, hyperglycaemia/ketone rules, sport adjustments and who may supervise. ADA school-setting guidance emphasises safe participation, not exclusion. [5]
ADHD and learning. Multi-setting assessment; teacher scales as adjuncts; medication timing that covers the school day when pharmacotherapy is used; classroom strategies coordinated with education staff. Diagnosis is clinical, not a school label alone. [8]
Epilepsy. First-aid steps, rescue medicine authorisation, water and climbing precautions, and post-ictal supervision. [1]
Concussion / return-to-learn. Symptom-limited academic load, rest breaks, reduced screen glare if needed, delayed exams, and staged sport clearance only after learning tolerance recovers. [6] [7]
Medical complexity and technology. Ventilation, feeds, emergency seizures or adrenal plans need named trained responders and equipment checklists before term starts. [1]
Adolescent confidential care via SBHC. Sexual health, mental health and gender-affirming support may be accessed through school-linked services; know local consent and confidentiality law, and how billing or portal messages can break privacy. [2] [14]
Complications & Pitfalls
- Vague plans staff cannot execute under stress. [4]
- No on-site adrenaline, expired devices, or unlocked cupboard nobody can open. [4]
- Assuming a nurse is always present. [1]
- Return-to-sport before return-to-learn is stable. [6] [7]
- Treating teacher concerns as a complete ADHD diagnosis. [8]
- Using a child as interpreter or breaching adolescent confidentiality without legal basis. [14]
- Ignoring attendance collapse and food insecurity while adjusting stimulants or inhalers. [12] [20]
- Missing safeguarding signals framed as “behaviour.” [13]
- SBHC care that never reaches the medical home record. [2] [3]
Prognosis & Disposition
Well-designed school health systems reduce preventable ED visits, missed learning and family work disruption. Poor systems convert manageable chronic disease into crisis. [2] [3]
After a school incident, choose disposition deliberately. Home with same-day or next-day medical-home review when the plan worked and the child is stable. Same-day clinic when the plan failed, medicines were missing, or control is drifting. Ambulance/ED for anaphylaxis after adrenaline, severe asthma, prolonged seizure, severe hypo, red-flag head injury or unsafe mental-health crisis. [4] [5] [7]
Update the written plan after every significant incident. A plan that failed once will fail again if nothing changes. [1]
Special Populations
Complex chronic and technology-dependent children. Individualised emergency folders, equipment lists, transport plans and trained 1:1 support may be essential. Inclusion is the goal; improvisation is not a plan. [1]
Disability and neurodiversity. Translate medical needs into classroom accommodations without pathologising identity. Sensory breaks and toileting plans are clinical tools. [8]
Indigenous families. Culturally safe communication, community liaison and respect for local schooling contexts improve plan uptake. [12]
Migrant and refugee students. Language access, catch-up immunisation documentation and trauma-informed approaches matter before exclusion debates. [10] [19]
Out-of-home care. Information fragments across carers and schools; name a medical-home owner for plan updates. [19]
Housing insecurity and poverty. School may be the most stable service site; SBHCs and school meals can buffer risk while you treat disease. [12] [19]
Gender and sexual diversity. Affirming names/pronouns, private disclosure pathways and careful record sharing protect engagement and safety. [14]
Evidence, Guidelines & Regional Differences
Core evidence clusters around AAP school nursing and SBHC statements, structured anaphylaxis emergency plans, ADA diabetes school-care guidance, concussion return-to-learn frameworks, ADHD multi-setting assessment, immunisation exemption policy, and sports infectious-disease control. Preventive periodicity still intersects school entry through immunisation, growth, BP and mental-health surveillance. [1] [2] [4] [5] [6] [8] [9] [10] [11]
School nursing and public-health models vary by state/territory and DHB/region. Use local exclusion tables and personal health records; do not invent day counts. Support culturally safe care for Aboriginal and Torres Strait Islander and Māori students. Align immunisation documentation with the national schedule. [9] [10]
School nursing sits within the Healthy Child Programme and local authority public-health nursing structures. Education health care plans and school policies interact with medical letters. Follow UK public-health exclusion guidance and NICE-aligned pathways for asthma, allergy and mental health rather than US form names. [1] [9]
SBHCs are more developed in many districts and can expand medical-home access when integrated. Educational law tools (IEP/504) often operationalise accommodations. AAP school health statements and state nurse practice acts shape medication administration. [2] [3]
Provincial school-health nursing, public health and education accommodations vary. Name the province’s process; principles of executable plans and medical-home linkage still apply. [1] [2]
Controversies to respect: scope of universal school mental-health screening; vaccine mandate and exemption politics; adolescent confidentiality limits when parents pay or portals auto-disclose; and how hard to push full inclusion without adequate trained staff. Exam answers should show judgment and local humility. [2] [10] [14]
Exam Pearls
- A school health plan is a clinical safety device, not stationery. [1]
- Write for the stressed non-clinician: numbered steps, named medicines, clear ambulance lines. [4]
- Anaphylaxis: adrenaline first, stay with the child, plan for second dose and transfer. [4]
- Return-to-learn before return-to-sport after concussion. [6] [7]
- School nurse is a clinical partner; ask what the plan looked like in real life. [1]
- Attendance collapse is a vital sign. [12] [20]
- SBHC care must link to the medical home, not replace it in silence. [2] [3]
- Name the jurisdiction for exclusion tables, educational accommodations and confidentiality law. [10] [11]
- Teacher scales inform ADHD assessment; they do not diagnose alone. [8]
- After every school emergency, update the plan before the next bell. [1]
References
- [1]COUNCIL ON SCHOOL HEALTH Role of the School Nurse in Providing School Health Services. Pediatrics, 2016.PMID 27217476
- [2]Kjolhede C School-Based Health Centers and Pediatric Practice. Pediatrics, 2021.PMID 34544844
- [3]Beem AA School-Based Health Centers as the Pediatric Expanded Medical Home. The Journal of school health, 2019.PMID 31529500
- [4]Wang J Guidance on Completing a Written Allergy and Anaphylaxis Emergency Plan. Pediatrics, 2017.PMID 28193793
- [5]Cogen F Diabetes Care in the School Setting: A Statement of the American Diabetes Association. Diabetes care, 2024.PMID 39602587
- [6]Halstead ME Returning to learning following a concussion. Pediatrics, 2013.PMID 24163302
- [7]Halstead ME Sport-Related Concussion in Children and Adolescents. Pediatrics, 2018.PMID 30420472
- [8]Wolraich ML Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics, 2019.PMID 31570648
- [9]COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [10]COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE Medical Versus Nonmedical Immunization Exemptions for Child Care and School Attendance. Pediatrics, 2016.PMID 27573087
- [11]Davies HD Infectious Diseases Associated With Organized Sports and Outbreak Control. Pediatrics, 2017.PMID 28947608
- [12]COUNCIL ON COMMUNITY PEDIATRICS Promoting Food Security for All Children. Pediatrics, 2015.PMID 26498462
- [13]Flaherty EG Clinical report—the pediatrician’s role in child maltreatment prevention. Pediatrics, 2010.PMID 20945525
- [14]Rafferty J Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and Adolescents. Pediatrics, 2018.PMID 30224363
- [15]Flynn JT Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [16]US Preventive Services Task Force Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2017.PMID 28632874
- [17]Paruthi S Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine, 2016.PMID 27250809
- [18]Piercy KL The Physical Activity Guidelines for Americans. JAMA, 2018.PMID 30418471
- [19]Council on Community Pediatrics Providing care for children and adolescents facing homelessness and housing insecurity. Pediatrics, 2013.PMID 23713108
- [20]Wall-Wieler E Maternal Depression in Early Childhood and Developmental Vulnerability at School Entry. Pediatrics, 2020.PMID 32817440