Paeds · professional-practice-and-evidence
Family-centred and child-rights-based care
Also known as Patient- and family-centred care · Family-centred care · Child-rights-based care · Partnership with children and families · UN Convention on the Rights of the Child in practice · Children's participation in healthcare · Cultural safety and the family as unit of care
Fellowship-level approach to family-centred and child-rights-based care: the four IPFCC core concepts, the four UNCRC guiding principles, the evolution from paternalistic to child-rights-based care, Hart's ladder of participation, bedside delivery across NICU, complex chronic illness, adolescent, migrant-refugee, Indigenous, disability and end-of-life settings, and ANZ/UK/US/Canada frameworks and cultural-safety obligations.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eight-year-old with a complex chronic illness whose care sprawls across six specialists, a school, and a tired single parent. The question is never just "what is the medical plan?" It is "who is on this team with the child, and does the child and family actually have a say in it?" Family-centred and child-rights-based care is the working answer to that question. [1] [3]
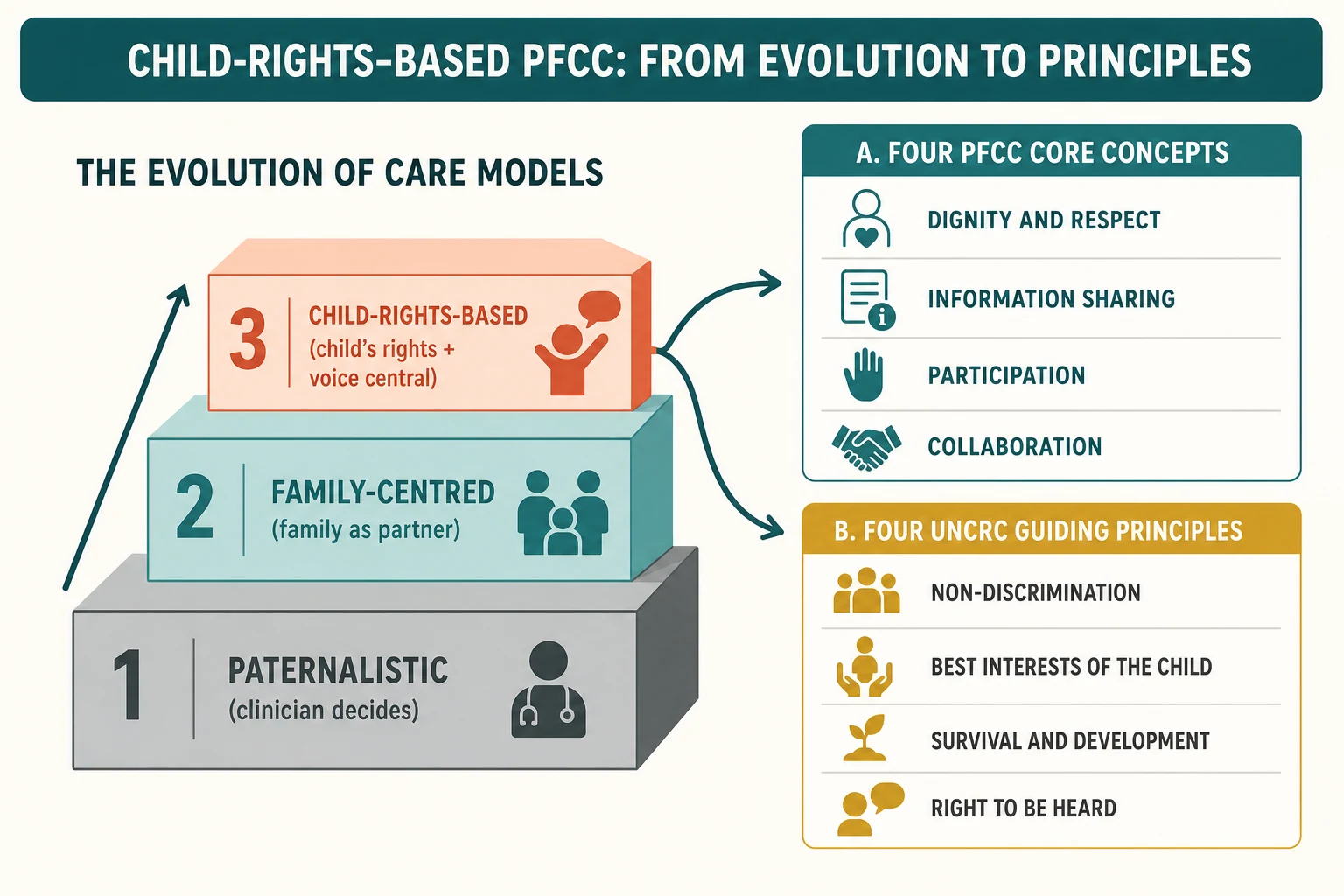
Patient- and family-centred care is an approach in which the clinician and family plan, deliver and evaluate care together as equal partners. The Institute for Patient- and Family-Centered Care frames it through four core concepts that examiners expect you to name: dignity and respect, information sharing, participation, and collaboration. The family is treated as a constant in the child's life, never as a visitor or an obstacle. [1]
Child-rights-based care takes the same partnership and grounds it in a legal frame. The UN Convention on the Rights of the Child is the most widely ratified human rights treaty in history, and it makes the child a rights-holder rather than a passive recipient. Its four guiding principles shape every paediatric encounter: non-discrimination, the best interests of the child, the right to life, survival and development, and the right of the child to be heard and to have their views given due weight. [5]
The two ideas overlap but are not identical. Family-centred care can, if practised carelessly, let "the family will decide" drown out the child's own voice. Child-rights-based care insists that the child holds rights independently of the parent, including the right to accessible information and a say in what happens to their body. The skilled clinician holds both: partners with the family while protecting the child's separate voice. [5] [12]
[1] [3]Classification
Classify by where power sits. The care model a clinician practises falls somewhere on a line from "I decide for you" to "we decide together, and you hold rights I must uphold". [3]
Paternalistic care places the clinician as the sole decision-maker; information flows one way and the family and child are recipients. Family-centred care moves the family to equal-partner status: information is shared, the family participates, and the plan is built collaboratively. Child-rights-based care adds the legal claim that the child is a rights-holder with an independent voice, and that the best interests of the child — not the convenience of the system — lead. [5]
Participation itself can be graded. Hart's ladder distinguishes rungs that are not participation at all from rungs that are. Manipulation, decoration and tokenism — a child asked to colour a poster about a decision already made — carry no weight and are not participation. Genuine participation runs from "assigned but informed" through consultation up to child-initiated, shared decisions with adults. Grading where a given encounter sits tells you whether you are honouring Article 12 or performing it. [12]
Two adjacent models are worth separating. The medical home is the operational expression of family-centred care for children with special health care needs — coordinated, accessible, continuous and compassionate. Family-directed care hands control of services and funding to the family, which still sits inside a clinically safe, coordinated plan. [3] [4]
Care models compared
Epidemiology & Risk Factors
Roughly one in five children lives with a special health care need, which makes family-centred coordination a daily requirement rather than an occasional courtesy. For these families the model is not aspirational; it is how safe care is even possible. [3] [4]
Experience and outcomes vary sharply by race, ethnicity, language, disability and socioeconomic position. Families who speak a language other than the clinician's, or who carry prior trauma with institutions, meet the same system from a different starting line. Rights-based care is therefore an equity instrument, not a soft skill. [5]
Children and adolescents are routinely left out of their own care conversations. Observational work in hospitals shows low rates of genuine child participation at the bedside — often the child is present but not consulted, or consulted in a way designed to secure compliance rather than elicit a view. [6]
The implementation gap is the everyday failure mode. PFCC is endorsed in policy across ANZ, the UK, the US and Canada, but the gap between endorsement and bedside delivery is widest exactly where acuity, crowding and under-resourcing press hardest. Knowing the policy is not the same as practising it. [10] [11]
The strongest risk factor for a rights-violating encounter is time pressure combined with a clinician assumption that children cannot, or should not, be told. Both are reversible at the bedside. [6] [7]
Pathophysiology
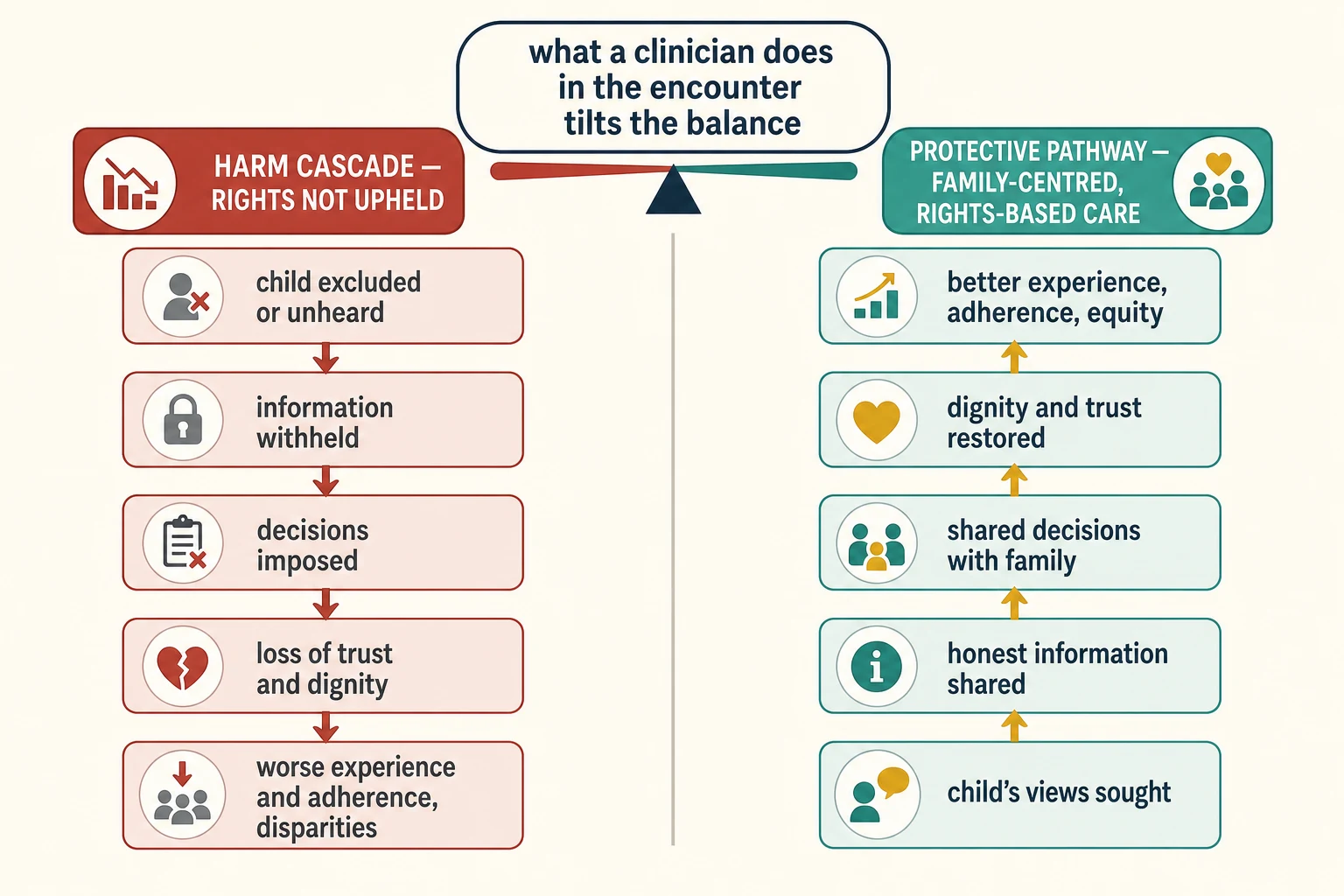
There is no enzyme for dignity, but there is a mechanism. Care that withholds information or excludes the child sets off a recognisable harm cascade, and care that does the opposite buffers it. [10]
When a child is excluded, information is withheld, or decisions are imposed, trust and dignity erode first. The child's anticipatory anxiety rises, adherence falls, and the family carries the memory forward into every future encounter. Over a population, the same dynamic widens disparities, because the families best able to insist on being heard are those with the most resource. [5] [7]
The protective pathway runs in reverse. Honest information, a heard voice and genuine partnership restore trust and build self-efficacy. The child learns that their body is not something done to them without warning, and the family learns that the team treats them as capable. Adherence and experience improve, and equity improves with them. [3]
The family is the unit of care, not a backdrop. Parental coping, sibling needs and the child's developmental processing of illness interact, so a family-centred approach treats the system. A parent who is supported sleeps, asks better questions, and holds the plan better than one left outside the door. [10] [8]
Hospitalisation triggers fight-flight-freeze stress in children. Information, parental presence and a sense of control buffer that stress; without the buffer, acute distress becomes healthcare-related trauma that the child carries for years. Participation is therefore protective physiology, not niceness. [11]
Clinical Presentation
Family-centred and rights-based issues surface wherever the system meets a child and family. The presentations differ, but the underlying question is constant: is this child being treated as a partner with rights, or as a case to be processed? [1]
A child with special health care needs presents a coordination problem first. Multiple providers, equipment, school and home all meet in one family, and the medical home is the structure that keeps the plan coherent. If the family is repeating the child's history to every new clinician, family-centred care has already failed. [3] [4]
An adolescent presents a participation and confidentiality problem. They expect to be spoken to directly, to have a say, and to be offered time without a parent. A clinician who talks over them to their parent has silently downgraded their rights. [5]
A neonate in intensive care presents a presence and information problem. Skin-to-skin care, open communication and shared rounds are the lived expression of family-centred care for a family at their most frightened. [8]
A migrant, refugee or Indigenous family presents a language, culture and kinship problem. The decision-making structure may not be the Western nuclear model, and a professional interpreter is essential, not optional. [9]
A telehealth encounter presents an access and presence problem. Identity, what can and cannot be assessed remotely, and whether the child can actually be seen and heard all become live rights questions. [1]
Differential Diagnosis
When an encounter is going badly, your first job is to name what is actually wrong. The label changes everything downstream. [10]
| Surface presentation | What it might actually be | Must-not-miss alternative |
|---|---|---|
| "Difficult family" | Unmet information need, language barrier, prior trauma | Genuine safeguarding risk requiring statutory action |
| "Child is uncooperative" | Pain, fear, or never told what would happen | Behavioural dissent signalling a rights issue |
| "Family refuses to engage" | Mistrust, cost, access barrier, cultural mismatch | Family violence or coercion driving the refusal |
| "Family wants to decide everything" | Reasonable partnership in a different cultural frame | Family-centred care being used to silence the child |
Discriminate genuine participation from tokenism. A child asked to hold a prop during a consent conversation they cannot influence is decoration, not participation; if their view carries no weight, Article 12 is not met. [12]
Separate cultural difference from a safeguarding concern. Respecting a family's autonomy and decision-making structure never overrides your duty to act on serious, foreseeable harm to the child. The two duties coexist; one does not cancel the other. [1]
Watch for family-centred care used as cover. "The family will decide" can be a phrase that silences the child's own voice — and a clinician's reason not to ask the child directly. The fix is to ask the child yourself, at the right developmental level, and record what they say. [5] [12]
Clinical & Bedside Assessment
Assessment for family-centred, rights-based care is assessment of the people, not of a disease. You are working out who is here, what they need, and how the child can take part. [1]
Start with who is in the family and decision-making unit. Name the parents, carers and kin who matter to this child, and do not assume a Western nuclear structure. For Indigenous families, identify the kinship decision-makers and meet the cultural obligations that apply where you practise. [9]
Assess how the child can participate. Their developmental stage sets what you tell them, how you ask their view, and how much weight that view carries. A preschool child participates through behaviour and simple choices; an adolescent participates through direct conversation and shared decisions. [12]
Assess information needs with two questions the IPFCC borrowed from serious-illness communication: what does the family already know, and how much do they want to know? Then match the format — plain language, pictures, accessible versions, and teach-back to confirm understanding rather than trusting a nod. [1] [7]
Assess language, culture, spiritual and accessibility needs before the encounter, and book a professional interpreter where there is any language barrier. Using a family member as interpreter for high-stakes information is a recognised rights and safety failure. [9]
Assess trust, voluntariness and coercion. Screen for family violence and safeguarding concerns, because these change who actually holds the child's best interests. A plan built on coercion is not a partnership. [1]
Investigations
There is no blood test for family-centred care, but there are structured ways to check whether the four core concepts are actually reaching the bedside. [10]
Patient-reported experience measures and family-centred-care self-assessment tools audit delivery. They expose whether the family felt respected, informed and included — the outcomes that matter for this model, which clinical metrics miss. [11]
The record is itself an investigation of participation. Read the notes: do they record the child's own views, or only the parent's? A chart that never quotes the child is evidence of a participation gap, and a prompt to do better. [6]
Document the family's communication and cultural preferences, the kinship decision-makers, and any advance care plan or custodial arrangement. For Indigenous and migrant families, a cultural and spiritual assessment tailors information sharing and participation safely. [9]
When rights or goals conflict, the "investigation" is a structured ethics or social-work consultation — not another scan. Bring the family advisory structure, interpreter and advocate in early, before the conflict hardens. [1]
Management — Resuscitation
In acute crisis, hold safety and dignity together. Preserve life first, but never let urgency become an excuse to discard the child's voice when you could keep it. [1]
When a child is frightened or refusing, do not override behaviourally. Check the reversible drivers — pain, fear, misunderstanding, hunger — before you conclude the child is simply obstructing. A terrified child who was never told what would happen is not refusing; they are unprotected. [11]
Honest information under pressure is non-negotiable. Lying to a frightened child to secure cooperation ("this won't hurt") buys minutes and costs years of trust. Name what is happening in child-accessible language, and let the family support the child through it. [7]
Allocate roles when crisis and family-centred care compete. One clinician leads the clinical resuscitation while another supports the family, and the child's voice and the consent basis are carried forward explicitly in handover. [1]
A safeguarding concern surfaced during family-centred care engages statutory duties that override ordinary family autonomy. Act on it, and document why — respect for the family does not extend to leaving a child in serious, foreseeable harm. [1] [5]
Management — Definitive & Stepwise
Use a sequence you can defend out loud in a viva, built around the four core concepts and the child's right to be heard. [1] [12]
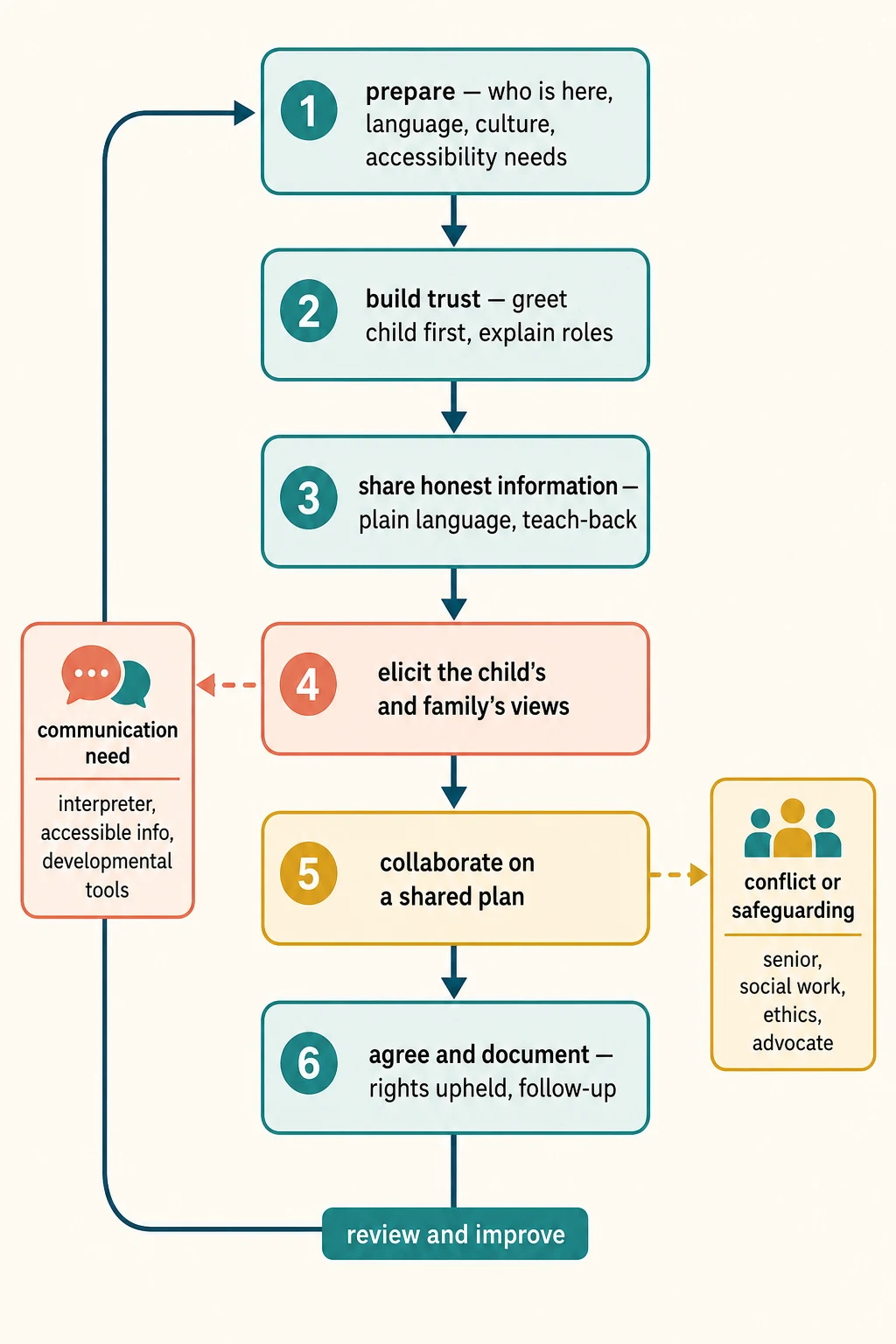
Bedside family-centred, rights-based algorithm
Prepare — who is present, language, culture, accessibility needs, private respectful setting
Build trust — greet the child by name first, explain roles, signal the family is a partner not a visitor
Share honest information — plain language, invite questions, disclose knowns and unknowns, teach-back
Elicit the child's and family's views — ask the child directly at a developmentally right level, weight the views
Collaborate on a shared plan — build the plan with the family around their goals, values and circumstances
Agree and document — who decided, information shared, the child's views recorded, rights upheld, follow-up
Review and improve — close the loop, seek feedback, feed experience into service improvement
For a child with special health care needs, the definitive structure is the medical home: a named coordinating clinician, a shared care plan, and a family who knows whom to call. Coordinated, accessible, continuous care is family-centred care made operational. [3] [4]
For an adolescent, the definitive move is confidential time and direct participation. Speak to them alone, share accessible information, and apply local frameworks for the decisions they can make for themselves. Their voice is theirs, not the family's to relay. [5]
For a migrant or Indigenous family, the definitive move is the professional interpreter and the cultural broker. Pace the conversation for trauma, explain the norms of your health system, and meet your local cultural-safety obligations. [9]
When conflict or safeguarding intrudes, branch early to senior clinician, social work, ethics or a child advocate, and keep the child's best interests leading. Shared decision-making tools structure the conversation; they do not replace the duty to uphold rights. [1]
Specific Subtypes & Scenarios
Neonate in intensive care. Family-centred care is lived as skin-to-skin and kangaroo care, open communication, parental presence on rounds, and structured family support. These reduce length of stay and improve outcomes because a supported family participates better in a fragile baby's care. [8]
Child with special health care needs. The medical home is the model: coordinated, accessible, continuous care with a shared plan and a named coordinator. Family-centred care here is associated with fewer unmet needs and better anticipatory guidance. [3] [4]
Adolescent in clinic. Offer confidential time, speak directly to the young person, share accessible information, and apply local mature-minor frameworks. Treat their voice as theirs, not as something the family relays on their behalf. [5]
End-of-life and palliative care. Let the child's and family's values lead goals of care. Include the child developmentally — many children, given the chance, can say what matters to them, and Article 12 requires that those views be given weight. [12]
Migrant or refugee family. Use a professional interpreter, pace for trauma, and explain the health-system norms the family may not share. Never use a child as interpreter for a parent's medical information. [9]
Indigenous family. Practise cultural safety: recognise kinship decision-makers, meet your obligations under Te Tiriti o Waitangi in Aotearoa New Zealand or truth-and-reconciliation commitments in Canada, and avoid assuming a Western model of family. [9]
Child with disability or neurodiversity. Provide accessible information and supported communication, and grade participation to function rather than age. Never equate disability with inability to take part. [5]
Telehealth encounter. Verify identity, disclose the limits of remote assessment, and make sure the child can actually be seen and heard — a silent child on a screen is a participation risk, not a convenience. [1]
Hospitalised child and shared decisions. Observational evidence shows children are often present but rarely genuinely consulted. Build explicit moments to ask the child's view and record it, so participation is real rather than performed. [6] [7]
Complications & Pitfalls
- Tokenism: inviting the child to be present without giving their views any weight. [12]
- Information dumping or withholding — both breach the information-sharing core concept. [7]
- Treating the family as the unit of care at the expense of the child's own Article 12 voice. [5]
- Cultural imposition: applying your own decision-making norms to another family's structure. [9]
- Using a family member as interpreter for high-stakes information. [9]
- Wrapping a safeguarding failure in "respect for the family" to avoid acting on harm. [1]
- Ignoring the implementation gap — endorsed policy that never reaches the bedside. [10]
- Assuming a nod means understanding; always teach back. [1]
- Clinician moral distress and burnout when systems block genuine partnership. [11]
Prognosis & Disposition
In the short term, a family-centred, rights-based encounter pays off as trust. The family reports understanding, the child's views are on the record, and a shared plan with follow-up is documented. These are the markers of a good encounter for this model. [1]
A child can be discharged safely when the family understands the plan, knows the red flags that should bring them back, and was heard. Safety-netting is itself an act of information sharing and partnership. [1]
Defer when the setting undermines the conversation. If the family is not ready, the room is not private, or the interpreter is absent, schedule a better-prepared follow-up rather than forcing a rights-violating encounter in a corner. [10]
Escalate conflict over goals or rights to ethics, mediation, social work or a second opinion, and bring a child advocate in. Do not leave a contested plan to drift in handover — carry the family's views and the child's views explicitly. [1]
Disposition includes team debrief and service improvement. Feed family experience back into system change, because the implementation gap closes only when bedside practice and the system around it move together. Over the long term, trust, adherence and equity are the returns on practising this way. [11]
Special Populations
Children with special health care needs and technology dependence. Family-centred coordination is essential; the family often carries expertise the team lacks, and the medical home holds the plan together. [3] [4]
Disability and neurodiversity. Use accessible information and supported communication; grade participation to function, not age, and never equate disability with inability. [5]
Indigenous families. Practise cultural safety, recognise kinship decision-makers, and meet Te Tiriti-based or truth-and-reconciliation obligations where you practise. [9]
Migrant, refugee and asylum-seeking families. Professional interpreters and trauma-informed, rights-respecting care; explain the norms of your health system. [9]
Out-of-home care and youth justice. Identify the statutory decision-maker and uphold the child's right to be heard, which does not disappear because a child is in care. [1]
Gender and sexual diversity. Provide respectful, confidential, rights-based care without discrimination; Article 2 forbids it. [5]
Maltreatment and family-violence contexts. Safeguarding duties override ordinary family autonomy; the child's best interests lead, and the child's voice is protected. [1]
Socioeconomic disadvantage. Address access and literacy barriers directly; a plan a family cannot reach, afford or understand is not rights-based care. [5]
Adolescents. Confidential time, direct participation, and developmentally appropriate, accessible information. [12]
Evidence, Guidelines & Regional Differences
The American Academy of Pediatrics anchored the language examiners expect. The 2003 policy statement defined family-centred care and the pediatrician's role, and the 2012 joint statement with the Institute for Patient- and Family-Centered Care reframed it as patient- and family-centred care around the four core concepts. [1] [2]
Kuo and colleagues set out the current applications and future directions of family-centred care, and linked it to reduced unmet needs in children with special health care needs; the same group showed the association with better anticipatory guidance delivery. [3] [4] O'Connor and colleagues provided the concept analysis of family-centred care in the acute hospital setting, naming its attributes and tensions. [10]
Goldhagen and colleagues framed a global rights, justice and equity agenda for child health, grounding the bedside practice in the UN Convention on the Rights of the Child. [5] The International Network for Child and Family Centered Care, through Al-Motlaq and colleagues, set the position statement shaping current practice. [11]
The participation evidence is humbling. Coyne and colleagues showed that information sharing between professionals, parents and children with cancer is more than information exchange — it is a relational act that often under-delivers. [7] Quaye and colleagues observed low rates of genuine child participation in bedside decisions during hospitalisation. [6] Alderson framed children as partners with adults in their own medical care, linking Article 12 directly to practice. [12]
In the NICU, Gooding and colleagues traced the origins, advances and impact of family support and family-centred care, and Shields and Nixon compared hospital care of children across four countries, exposing cultural variation in how partnership is actually practised. [8] [9]
The honest caveat is that randomised evidence for hard clinical outcomes is limited, and the implementation gap is real. Power imbalances mean that policy endorsement does not guarantee bedside delivery — which is exactly why this is examined as a practice skill, not a recited doctrine. [10]
Australia and Aotearoa New Zealand practise family-centred care through the medical home for children with special health care needs and carry specific obligations to Māori whānau under Te Tiriti o Waitangi and to Aboriginal and Torres Strait Islander families through culturally safe practice and community-controlled services. State the principle — partnership, participation, protection — and meet the cultural-safety standards your jurisdiction sets, without inventing statutory wording. [9] [5]
Exam Pearls
PARTNER
References
- [1]COMMITTEE ON HOSPITAL CARE, INSTITUTE FOR PATIENT- AND FAMILY-CENTERED CARE Patient- and family-centered care and the pediatrician's role. Pediatrics, 2012.PMID 22291118
- [2]American Academy of Pediatrics Committee on Hospital Care Family-centered care and the pediatrician's role. Pediatrics, 2003.PMID 12949306
- [3]Kuo DZ, Houtrow AJ, Arango P, Kuhlthau KA, Simmons JM, Neff JM Family-centered care: current applications and future directions in pediatric health care. Matern Child Health J, 2012.PMID 21318293
- [4]Kuo DZ, Frick KD, Minkovitz CS Association of family-centered care with improved anticipatory guidance delivery and reduced unmet needs in child health care. Matern Child Health J, 2011.PMID 21057865
- [5]Goldhagen JL, Shenoda S, Oberg C, Mercer R, Kadir A, Raman S Rights, justice, and equity: a global agenda for child health and wellbeing. Lancet Child Adolesc Health, 2020.PMID 31757760
- [6]Quaye AA, Coyne I, Söderbäck M, Hallström IK Children's active participation in decision-making processes during hospitalisation: An observational study. J Clin Nurs, 2019.PMID 31430412
- [7]Coyne I, Amory A, Gibson F, Kiernan G Information-sharing between healthcare professionals, parents and children with cancer: more than a matter of information exchange. Eur J Cancer Care (Engl), 2016.PMID 26537295
- [8]Gooding JS, Cooper LG, Blaine AI, Franck LS, Howse JL, Berns SD Family support and family-centered care in the neonatal intensive care unit: origins, advances, impact. Semin Perinatol, 2011.PMID 21255703
- [9]Shields L, Nixon J Hospital care of children in four countries. J Adv Nurs, 2004.PMID 15009350
- [10]O'Connor S, Brenner M, Coyne I Family-centred care of children and young people in the acute hospital setting: A concept analysis. J Clin Nurs, 2019.PMID 31099444
- [11]Al-Motlaq M, Neill S, Foster MJ, Coyne I, Houghton D, Angelhoff C Position Statement of the International Network for Child and Family Centered Care: Child and Family Centred Care during the COVID19 Pandemic. J Pediatr Nurs, 2021.PMID 34052501
- [12]Alderson P, Sutcliffe K, Curtis K Children as partners with adults in their medical care. Arch Dis Child, 2006.PMID 16399782