Paeds · professional-practice-and-evidence
Open disclosure and duty of candour
Also known as Open disclosure in paediatrics · Duty of candour to children and families · Disclosure of medical error to parents · Patient safety incident disclosure · Being open after harm
Fellowship guide to open disclosure and duty of candour in paediatrics: recognising a notifiable patient safety incident, grading severity, the staged disclosure conversation with apology and expression of regret, adapting disclosure to the child's development and to parents as recipients, the second-victim phenomenon, systemic and cultural barriers, and ANZ/UK/US/Canada frameworks and apology-law differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
O.P.E.N. — the stance you take after harm
Overview & Definition
A 3-year-old on the ward is given ten times the intended dose of an opioid because of a decimal-point error. The nurse realises within minutes, the child is reviewed and is fortunately unaffected, and both parents are at the bedside. What happens in the next hour — what you say, whether you say sorry, whether you are honest about what went wrong — will decide whether this family trusts your team for the rest of their child's care, or leaves feeling deceived. That conversation is open disclosure, and the obligation to have it is the duty of candour. [1] [4]
Open disclosure is the open discussion with a patient, and their family, of a patient safety incident that resulted in harm while they were receiving health care. It is not a confession, a legal admission, or a single scripted speech; it is a staged process of communication that runs in parallel with clinical stabilisation, incident reporting and formal review. The framework was developed and evaluated at national scale in Australia through the Open Disclosure Pilot, which showed that families want the truth, an acknowledgement of harm, an apology, and assurance that the system will learn. [1] [2] [10]
The duty of candour is the obligation behind the process. In paediatrics it carries a particular weight: the patient is a child who may be too young to receive the information directly, so the conversation is usually held with parents or guardians, and the child or young person is brought in developmentally. Harm to a child strikes at the heart of a family's trust in the institution that was meant to protect them, which is exactly why concealment or partial disclosure is so corrosive here. [4] [5]
This page owns the process and obligation of disclosure. Cross-link the dedicated leaves for the recognition and analysis of adverse events, for breaking bad news, for consent and mature-minor frameworks, for communicating risk and uncertainty, for conflict and complaints, and for trauma-informed care — do not rebuild their content here. [6]
Classification
Sort the work by what kind of incident happened and by which duty applies. [1] [11]
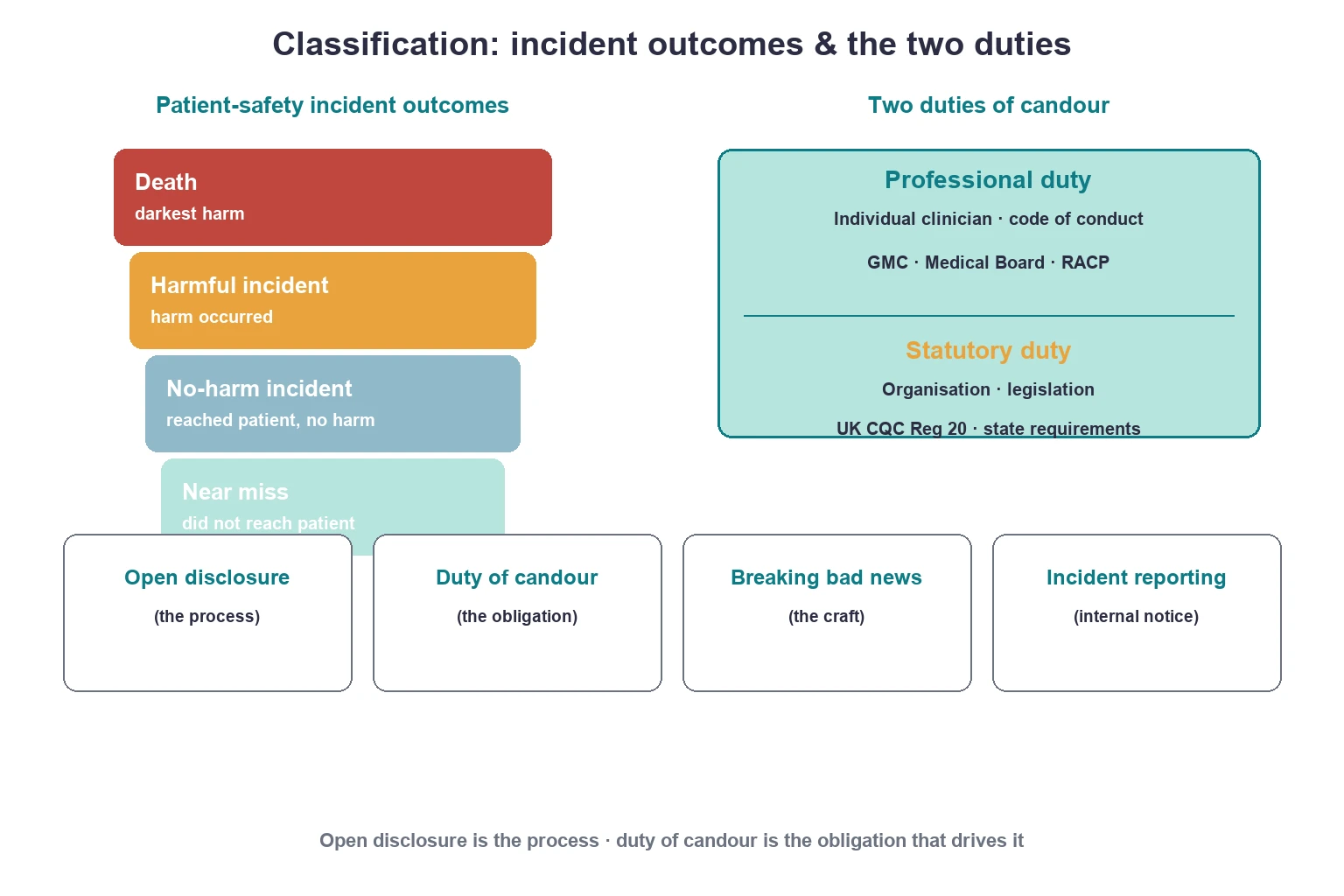
Patient safety incident outcomes. A near miss is an incident that did not reach the patient (a caught error). A no-harm incident reached the patient but caused no detectable harm. A harmful incident caused harm. Death is the most severe outcome. Duty of candour is triggered by harm — and by the threshold of risk of harm set by a statutory regime — but near misses and no-harm incidents still merit internal reporting so the system can learn. [11] [12]
Two duties of candour. The professional (individual) duty sits on each clinician and is set by codes of conduct — the Medical Board of Australia and RACP codes in ANZ, the GMC's professional duty of candour in the UK. The statutory (organisational) duty sits on the regulated body: in England, CQC Regulation 20 imposes a legal duty of candour on providers when a notifiable safety incident occurs. They are distinct but complementary — a clinician cannot hide behind an absent organisational policy, and an organisation cannot discharge its duty without clinicians acting honestly. [4] [5]
What this is NOT. Open disclosure is the process; duty of candour is the obligation; breaking bad news is the craft of delivering serious news (a new diagnosis, a poor prognosis) that may have nothing to do with an error; incident reporting is the internal notification that feeds review and learning. A real incident often needs all four. [1] [6]
Epidemiology & Risk Factors
Patient safety incidents are common in paediatric care, and harmful events occur more often in the systems where children are most vulnerable — neonates and infants, the PICU, the emergency department, and children with medical complexity who depend on multiple medications and devices. Weight-based dosing, decimal-point errors, and look-alike drug concentrations make children especially exposed to medication error, which is one of the most frequent triggers for a disclosure conversation. [6] [12]
The human cost is real, but so is the disclosure gap. Surveys of physicians show that even when clinicians endorse disclosure in principle, many would not fully disclose a harmful error in practice — giving partial information, vague language, or no apology. This gap between belief and behaviour is one of the most reproducible findings in the disclosure literature and is the single biggest reason families end up feeling deceived. [3] [17]
Disclosure is unevenly distributed across families. Language barriers, cultural difference and socioeconomic disadvantage all make it less likely that a family receives a full, timely, interpreter-supported disclosure — a disparity that compounds the harm and erodes trust in the families least able to absorb it. Recognising this is part of practising equitable candour. [5] [12]
Pathophysiology
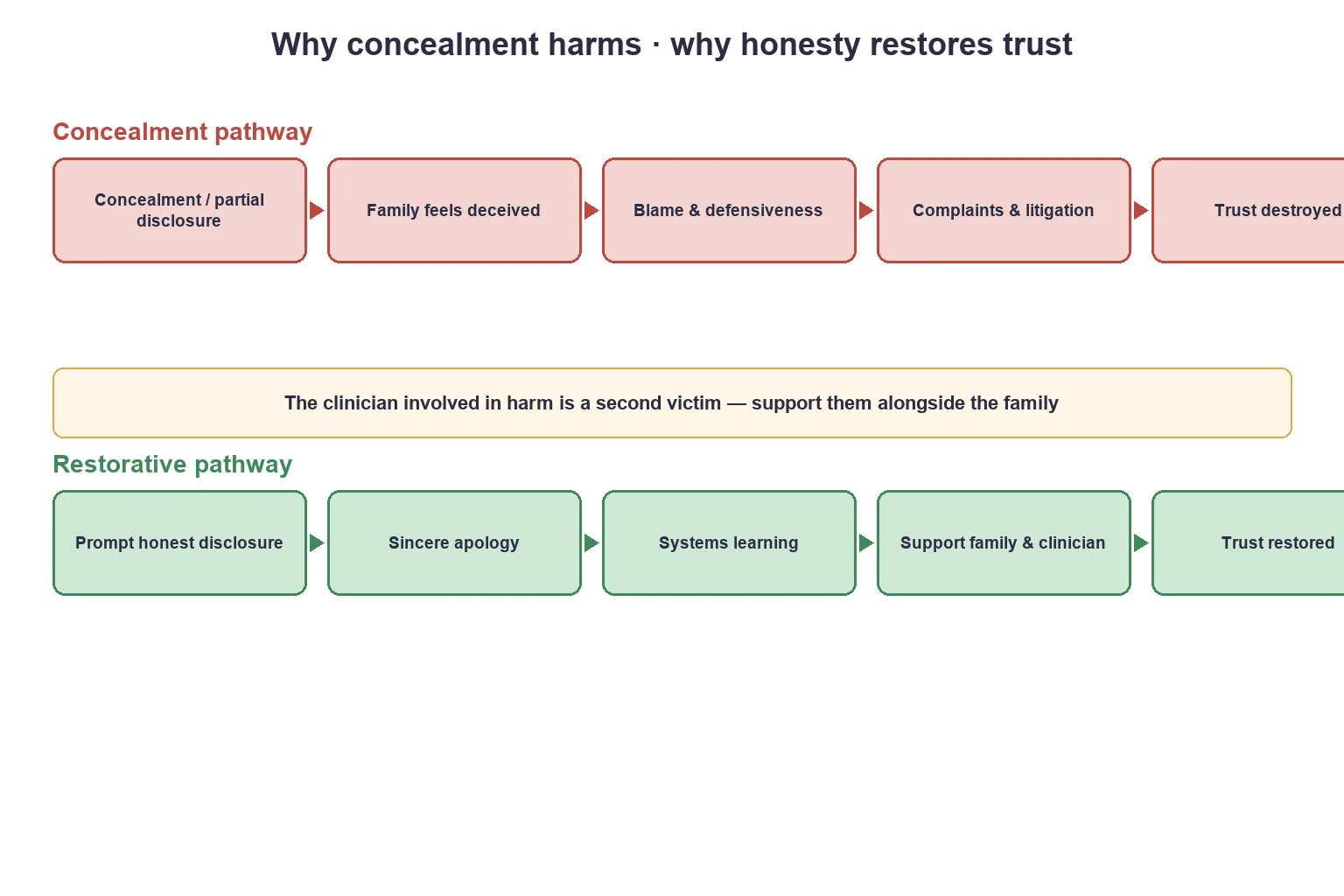
Concealment harms through a predictable cascade. When a family discovers — through their own observation, a side comment, or a delayed complaint — that harm occurred and was not disclosed, the dominant emotion shifts from the harm itself to the sense of having been deceived. Anger, loss of trust, and a drive to complain or litigate follow, and the original clinical harm is overtaken by a relational harm that is far harder to repair. Families harmed in this way consistently describe wanting the truth, an acknowledgement, and an apology more than they want punishment. [2] [11] [16]
Honest disclosure runs the reverse cascade. The Australian evaluation of open disclosure found that when families received a prompt, candid account with an apology and a genuine commitment to learn, trust was often restored rather than destroyed, and complaints and legal action fell rather than rose. The mechanism is that candour meets the family's actual need — for truth, acknowledgement and meaning — rather than their feared need for retribution. [1] [2] [10]
Systems thinking explains why the incident happened in the first place and should shape the conversation. Most harmful events arise from latent system failures — look-alike drugs, workload, interruptions, ambiguous orders — that line up through the defences, not from a single reckless clinician. Framing the incident this way protects the family from a wrong explanation and protects a just-and-learning culture that fixes systems rather than scapegoats people. [6] [12]
Clinical Presentation
A disclosure conversation is triggered by a patient safety incident that caused, or could have caused, harm. The presentations are varied but the response structure is constant. [1] [6]
A child receives a wrong or tenfold medication dose — caught early or discovered only after an effect. A wrong patient or wrong-site procedure occurs in theatre or the emergency department. A diagnosis is missed or delayed — a febrile infant sent home who returns in septic shock — and the gap comes to light after interim harm. A procedural complication or an unplanned return to theatre raises the question of whether it was an expected risk or a preventable error. A healthcare-associated infection outbreak on a neonatal or paediatric ward triggers a duty-of-candour notification to affected families. [5] [6]
Sometimes the family presents the problem to you: a parent finds a discrepancy in the medication chart, or pieces together that a deterioration was not communicated, and confronts the team. This is the highest-risk presentation for trust, because the family already suspects concealment, and the only response that repairs it is immediate, full, apologetic candour. [2] [16]
Differential Diagnosis
Before you frame an incident, be clear what kind of event it is, because the family's question — and your legal exposure — turns on the distinction. [6] [15]
Harmful incident versus an expected, previously-disclosed complication. A postoperative bleed after adenoid surgery is a known, consented risk; a wrong-drug error is not. Only the latter is a candour event in the full sense, though both may need a conversation. [6]
Error versus adverse event. An error is a failure to complete a planned action as intended or a wrong plan — it is about the process. An adverse event is patient harm, whether or not it was preventable. Some adverse events are not errors, and some errors cause no harm. Duty of candour is anchored to harm, but disclosure of an error that reached the patient without harm still builds trust. [11]
Systems failure versus individual lapse. Most events are dominated by system factors; a few reflect individual recklessness. Jumping to the individual explanation misleads the family and undermines a just culture. [6] [12]
Concealment versus genuine uncertainty. Early on you may not know what happened or whether harm occurred. This is not concealment — but you must say so honestly and commit to finding out, rather than staying silent. [1] [4]
Clinical & Bedside Assessment
Assessment happens fast, in parallel with treating the child. Establish immediately what happened, who was involved, whether the child was harmed, and — above all — whether the child is now safe and stable. Grade the severity of the incident using the organisation's severity matrix, because this drives both the urgency of disclosure and the statutory reporting pathway. [1] [11]
Assess the family before you speak to them. What do they already understand about what happened? What is their emotional state? Are they at the bedside or have they gone home? Assess the child's developmental stage and prior involvement to decide how, and how much, to include them — an adolescent with capacity should be a primary participant, while a pre-schooler is shielded from the full weight of the conversation but told the truth in concrete terms. [4] [15]
Check language and cultural needs. If the family has limited English, arrange a trained interpreter before the conversation — never use the child or another family member as the interpreter for a disclosure of harm. Consider whether a social worker, cultural support worker or Aboriginal and Torres Strait Islander / Maori liaison officer should be present. [5]
Investigations
Clinical investigation of the incident runs alongside, but does not delay, the initial disclosure. The child is reviewed and stabilised first. The incident record is opened; the responsible consultant, the unit manager and the risk or patient safety team are notified. For a high-severity (SAC1 or equivalent) incident, a formal review — a root-cause or systems analysis — is triggered, but its findings belong in the follow-up disclosure, not the first one. [1] [10]
Gather the immediate timeline — what is known, who did what, what device or medication was involved — so your first account is accurate and you are not forced to retract it. Document the disclosure itself: who was present, what was said, the apology offered, the family's questions, and the agreed follow-up. This documentation protects the family, the clinician and the institution, and ensures the team speaks with one coherent voice. [1] [10]
Management — Resuscitation
Clinical safety always precedes communication. If the child is deteriorating after the incident, you treat and stabilise first; the disclosure waits until the child is safe and the right people are assembled. A disclosure attempted while a child is being actively resuscitated is a failure of prioritisation. [6]
Acute parental psychological collapse during a disclosure — overwhelming distress, dissociation, or a disclosed intent to self-harm — needs an immediate pause, supportive presence, and escalation to social work or mental health services. A safeguarding concern surfaced by the incident (for example, a non-accidental injury uncovered, or neglect contributing to the error) triggers the local safeguarding pathway in parallel, and does not replace candour to the family about the clinical event. [4] [5]
The clinician involved in the harm may be acutely distressed — a second victim in crisis. If the treating clinician is too shaken to lead the conversation safely, arrange for a senior colleague to lead while they are supported and given cover. Forcing a distressed clinician to disclose unsupported harms them and the family. [14]
Management — Definitive & Stepwise
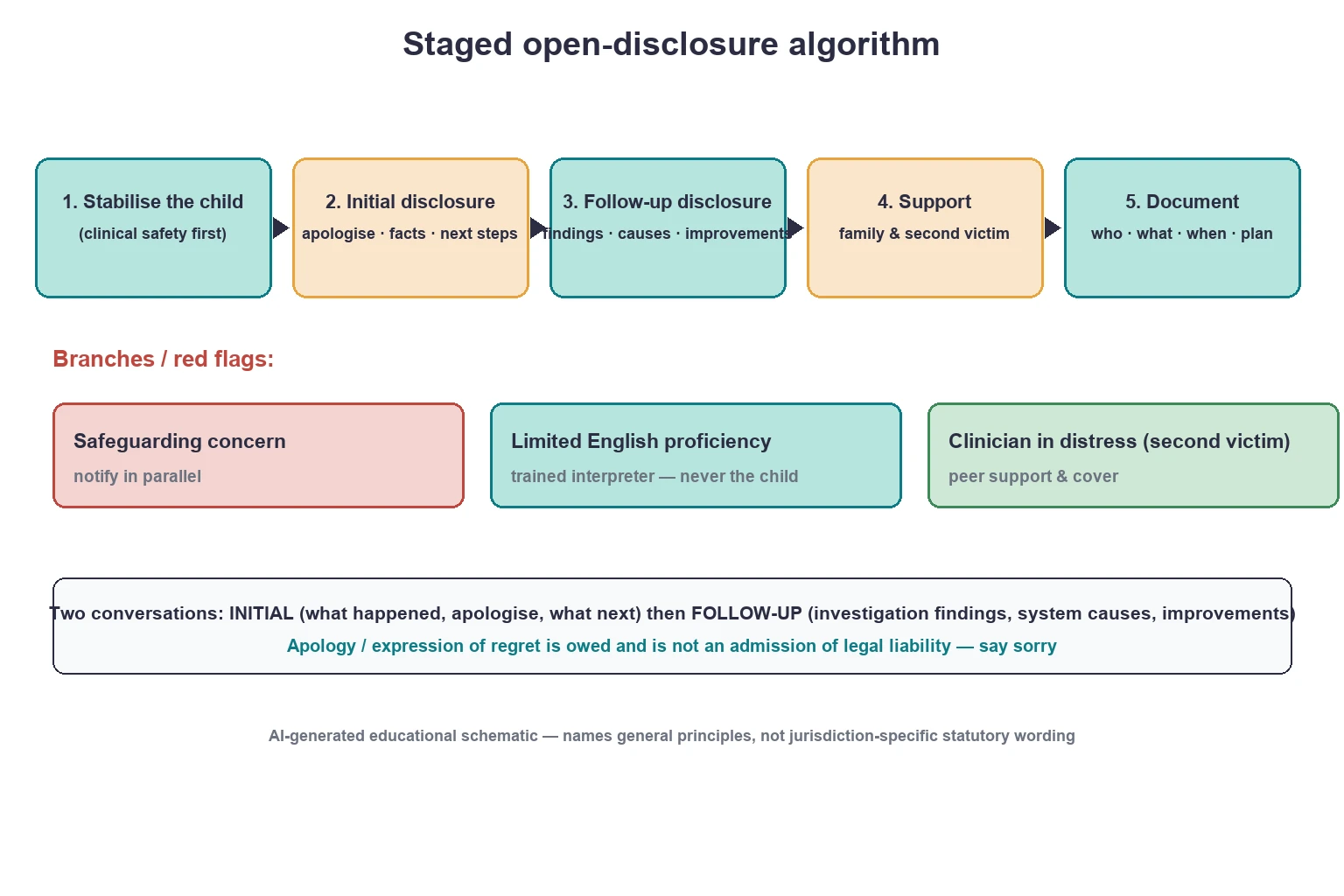
Open disclosure unfolds as two conversations wrapped in a process. The initial disclosure happens promptly, in a private setting, with the right people — the treating clinician or consultant leading, both parents where possible, a nurse or social worker for support, and a trained interpreter if needed. You acknowledge what happened in plain language, give the facts that are known, say honestly what is not yet known, apologise (offer a sincere expression of regret for the harm), and describe what will happen next. You do not speculate about causes, and you do not blame an individual in front of the family. [1] [4]
The staged open-disclosure conversation
Stabilise and treat the child — clinical safety first
Convene the right people in a private space; arrange a trained interpreter if needed
Acknowledge what happened in plain language; give the known facts
Apologise — a sincere expression of regret for the harm
Say what is not yet known and what will happen next; avoid speculation and blame
Check the family's understanding; invite questions; name a single point of contact
Follow up: share the investigation findings, system causes and the improvement plan
Document who was present, what was said, the apology, questions and agreed plan
The apology deserves its own emphasis. An expression of regret — saying sorry for the harm the child suffered — is owed to the family as a matter of honesty and compassion, and across ANZ and many other jurisdictions it is protected by apology legislation that prevents it from being treated as an admission of legal liability. Withholding an apology for fear of legal consequence misreads the evidence: disclosure with apology is associated with reduced, not increased, litigation. [1] [2] [11]
The follow-up disclosure is the second conversation, held once the review or systems analysis is complete. Here you share the findings honestly — what the contributing system factors were, what went wrong, and crucially what will change so that this does not happen to another child. This is where candour becomes system learning, and it is what many families say matters most: not blame, but assurance. [1] [10]
Throughout, provide practical and emotional support: a single named point of contact, a written summary of the conversations, access to counselling, and clear routes to escalate or to complain if they need to. And care for the team: arrange a debrief and peer support for the second victim, because unsupported clinicians may leave practice or repeat errors. [14]
Specific Subtypes & Scenarios
The structure is constant, but each scenario has a particular trap. [6] [9]
Wrong-dose or tenfold medication error in an infant. The classic weight-based decimal-point error. Disclose promptly even if the child appears unharmed; the family needs to know and the system needs the report. Lead with the treating team, apologise, and describe the review of the prescribing–checking–administration chain. [6]
Wrong patient or wrong-site procedure. High-severity, high-trust-impact. These are treated as serious incidents with a formal review, immediate disclosure to both families where relevant, and explicit assurance about the system fix (site-marking, timeout, identity checks). [6]
Missed or delayed diagnosis (for example, delayed sepsis recognition). Often the hardest to disclose because the harm is large and the contribution of the error is contested. Be honest about the gap between what was done and what should have been done; do not minimise. [15]
Healthcare-associated infection outbreak on a neonatal or paediatric ward. Multiple families affected, often requiring coordinated, consistent disclosure led by the service, with public-health and infection-control input — as illustrated by the Scottish paediatric ward incident in which duty of candour and communication were central. [5]
A family who discovers the error themselves. The highest-risk scenario for trust. Respond with immediate, full, apologetic candour; do not become defensive. The relationship can still be repaired if the team is honest from the moment the family raises it. [2] [16]
A clinician who is a second victim and is avoiding disclosure. Recognise the withdrawal, shame and self-doubt as the second-victim phenomenon. Provide peer support and cover, have a senior colleague lead the disclosure if needed, and protect the clinician's capacity to return to safe practice. [14]
Complications & Pitfalls
The failure modes are well described and recurring. [3] [17]
Concealment, cover-up and partial (trickle) disclosure. The most damaging pattern. Giving information in instalments, or only when pressed, signals dishonesty and converts clinical harm into betrayal. [1] [16]
Defensive language. Phrases like "we're sorry this happened to you" distance the team from the harm; the family hears evasion. An honest acknowledgement — "I am sorry that we gave the wrong dose, and that your child was harmed" — is owed. [2]
Delaying disclosure for the investigation. The initial conversation is owed promptly; waiting for the full causal analysis is concealment dressed as caution. [1] [4]
Blaming an individual in front of the family. This undermines a just-and-learning culture, misleads the family about causes, and exposes the clinician unfairly. Causes are usually systemic; the family hears the system analysis at follow-up. [6] [12]
Forgetting the second victim. Clinicians involved in harm experience guilt, anxiety and burnout; left unsupported, some leave practice. Disclosure systems that ignore the clinician fail the team as surely as concealment fails the family. [14]
Confusing candour with the litigation position. Withholding an apology out of misplaced legal fear contradicts the evidence — disclosure with apology is associated with fewer complaints and less litigation, and apology law protects the expression of regret. [1] [11]
Prognosis & Disposition
Honest, timely disclosure with an apology is good medicine and good risk management. The Australian evaluation found that open disclosure restores trust in most families and is associated with reduced complaints and legal action — the opposite of the fear that drives concealment. Families most want four things: the truth, an acknowledgement of harm, an apology, and assurance that it will not happen again. [1] [2]
What families want after harm
Disclosure is a process, not an event, so disposition means planning the follow-up meeting, leaving a written summary, and naming a contact. Unrecognised or unsupported second victims have a poorer prognosis — they may leave the workforce or repeat errors — so arranging clinician support is part of disposition, not an afterthought. [14]
The long-term outcome that honours the harmed patient is systems learning: the review findings and the improvement plan, shared back with the family, close the loop and turn an individual harm into a safer system for the next child. [1] [10]
Special Populations
Neonates and infants. Parents are the sole recipients of disclosure. Emphasise stabilisation and one consistent clinician voice, and protect the infant from parental distress at the bedside. Neonatal units carry a heavy burden of high-severity incidents, so a rehearsed, unit-wide disclosure process matters. [6]
Children with medical complexity and technology dependence. These families are expert partners who carry recurrent risk across long admissions; a disclosure after one incident sits inside a long relationship, and candour protects the trust that ongoing care depends on. [12]
Adolescents. Involve the young person developmentally and, where they have capacity, as a primary participant in the disclosure. Respect confidentiality and assent; offer them time alone with the clinician separate from the parents if they want it. [4] [15]
Families with limited English. Always use a trained interpreter; never the child or a family member. A disclosure delivered through the wrong language channel is not really a disclosure. [5]
Aboriginal and Torres Strait Islander, Maori and Indigenous families. Practise culturally safe, family-centred disclosure, with cultural support and liaison present, recognising the historical and ongoing context that shapes trust in institutions. [5]
Safeguarding interface. Disclosure of a clinical incident does not replace mandatory notification when the incident indicates child harm or neglect; the two duties run in parallel. [4]
Evidence, Guidelines & Regional Differences
The frameworks differ by jurisdiction, but the ethical core — honesty, acknowledgement, apology, learning — is universal. [1] [4]
The ACSQHC Australian Open Disclosure Framework is the ANZ standard: a voluntary, standards-based, four-stage process (recognise, prepare, engage, follow-up), evaluated nationally through the Open Disclosure Pilot. It is reinforced by the Medical Board of Australia and RACP codes of conduct, which impose a professional duty of candour on clinicians. Apology legislation in Australian states and territories protects a sincere expression of regret from being treated as an admission of liability. [1] [10]
The UK carries both duties. The GMC professional duty of candour sits on every doctor. The CQC Regulation 20 statutory duty of candour sits on registered providers and is triggered by a notifiable patient safety incident, with organisational obligations to inform, apologise, and report. NHS England guidance and the "just culture guide" support clinicians in doing the right thing. [4] [5]
Disclosure in the US is largely voluntary and standards-based, supported by the AHRQ and risk-management bodies, and shaped by "sorry works"/apology statutes that vary by state — some protecting only expressions of sympathy (partial), others protecting full apologies (complete). The variability means local policy must be known, but the ethical duty to disclose harm does not depend on the statute. [3] [11]
Canada's Canadian Disclosure Guidelines (originally from the Canadian Patient Safety Institute, now Healthcare Excellence Canada) set a national voluntary standard for open disclosure, aligned with CanMEDS roles of Communicator and Professional. [11]
Regional comparison of the candour and disclosure duty
Exam Pearls
References
- [1]Iedema RA The National Open Disclosure Pilot: evaluation of a policy implementation initiative. The Medical journal of Australia, 2008.PMID 18393742
- [2]Iedema R Patients' and family members' experiences of open disclosure following adverse events. International journal for quality in health care, 2008.PMID 18801752
- [3]Gallagher TH US and Canadian physicians' attitudes and experiences regarding disclosing errors to patients. Archives of internal medicine, 2006.PMID 16908793
- [4]Jacob H Openness and honesty when things go wrong: the professional duty of candour (GMC guideline). Archives of disease in childhood. Education and practice edition, 2016.PMID 27002114
- [5]Inkster T Duty of candour and communication during an infection control incident in a paediatric ward of a Scottish hospital. Journal of medical ethics, 2022.PMID 33593873
- [6]Brandom BW What happens when things go wrong? Paediatric anaesthesia, 2011.PMID 21251144
- [7]Aubin J Benefit of Simulation-Based Training in Medical Adverse Events Disclosure in Pediatrics. Pediatric emergency care, 2022.PMID 34398860
- [8]White AA Crowdsourced Feedback to Improve Resident Physician Error Disclosure Skills: A Randomized Clinical Trial. JAMA network open, 2024.PMID 39110461
- [9]Stroud L Teaching medical error disclosure to physicians-in-training: a scoping review. Academic medicine, 2013.PMID 23619064
- [10]Iedema R Practising Open Disclosure: clinical incident communication and systems improvement. Sociology of health & illness, 2009.PMID 18983420
- [11]O'Connor E Disclosure of patient safety incidents: a comprehensive review. International journal for quality in health care, 2010.PMID 20709703
- [12]Perez B Understanding the barriers to physician error reporting and disclosure: a systemic approach to a systemic problem. Journal of patient safety, 2014.PMID 24553443
- [13]Varjavand N Changes in intern attitudes toward medical error and disclosure. Medical education, 2012.PMID 22691146
- [14]New L Second-Victim Phenomenon. Nursing clinics of North America, 2024.PMID 38272580
- [15]Smith ML Thinking ethically about medical mistakes. Journal of child neurology, 2013.PMID 23435283
- [16]Case J What Drives Patients' Complaints About Adverse Events in Their Hospital Care? A Data Linkage Study of Australian Adults 45 Years and Older. Journal of patient safety, 2021.PMID 33512865
- [17]Mansour R Disclosure of medical errors: physicians' knowledge, attitudes and practices (KAP) in an oncology center. BMC medical ethics, 2020.PMID 32819353
- [18]Wong BM Learning Through Experience: Influence of Formal and Informal Training on Medical Error Disclosure Skills in Residents. Journal of graduate medical education, 2017.PMID 28261397