Paeds · respiratory-sleep-and-airway
Bronchiectasis in children
Also known as Paediatric bronchiectasis · Non-cystic fibrosis bronchiectasis · Chronic suppurative lung disease · CSLD · Childhood bronchiectasis
Fellowship guide to bronchiectasis in children — the chronic wet cough that defines it, the chronic suppurative lung disease continuum that precedes it, the vicious cycle that drives it, the HRCT that confirms it, the aetiological work-up that must follow, and the airway-clearance-and-antibiotic management that can reverse early disease and prevent lifelong lung damage.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old is brought back for the fifth time in a year with a "chest infection," and each time a course of antibiotics half-settles a cough that never fully goes away. The parents think he simply catches everything at daycare. The task of the paediatrician is to hear that history differently: a wet cough that persists for weeks and returns the moment antibiotics stop is the sound of an airway that cannot clear itself, and it is the earliest signal on the road to bronchiectasis. [1] [4]
Bronchiectasis is the permanent, abnormal widening of one or more bronchi, driven by chronic infection and inflammation that destroy the airway wall. In children it is confirmed on a chest high-resolution CT, where the dilated bronchus becomes wider than its neighbouring artery. The defining clinical feature, present long before any scan, is a chronic wet or productive cough — a cough that brings up sputum or sounds rattly and moist, lasting more than four weeks. [1] [5]
The single most useful idea for the exam is the continuum. Chronic suppurative lung disease describes the child with a persistent wet cough and lower-airway neutrophilic infection whose HRCT does not yet meet radiological criteria for bronchiectasis. Give that same child time and untreated infection, and the airway dilates into established bronchiectasis. The two conditions are the same disease at different stages, which is why the wet cough — not the scan — is the moment to act. [2] [1]
Framing bronchiectasis this way changes the clinical reflex. Rather than treating each "chest infection" as an isolated event, the paediatrician treats the persistent wet cough as a disease that demands both adequate treatment and a search for why the airway keeps failing. In young children this matters enormously, because early bronchiectasis can regress with intensive care in a way that established, long-standing disease cannot. [1] [4]
Classification
Two questions organise the whole topic: what does the damaged airway look like, and why did it happen. The first is answered by the scan and describes the shape of the disease; the second is answered by the work-up and decides the treatment. Holding both in mind stops you from settling for a radiological label when the child still needs a cause. [1] [5]
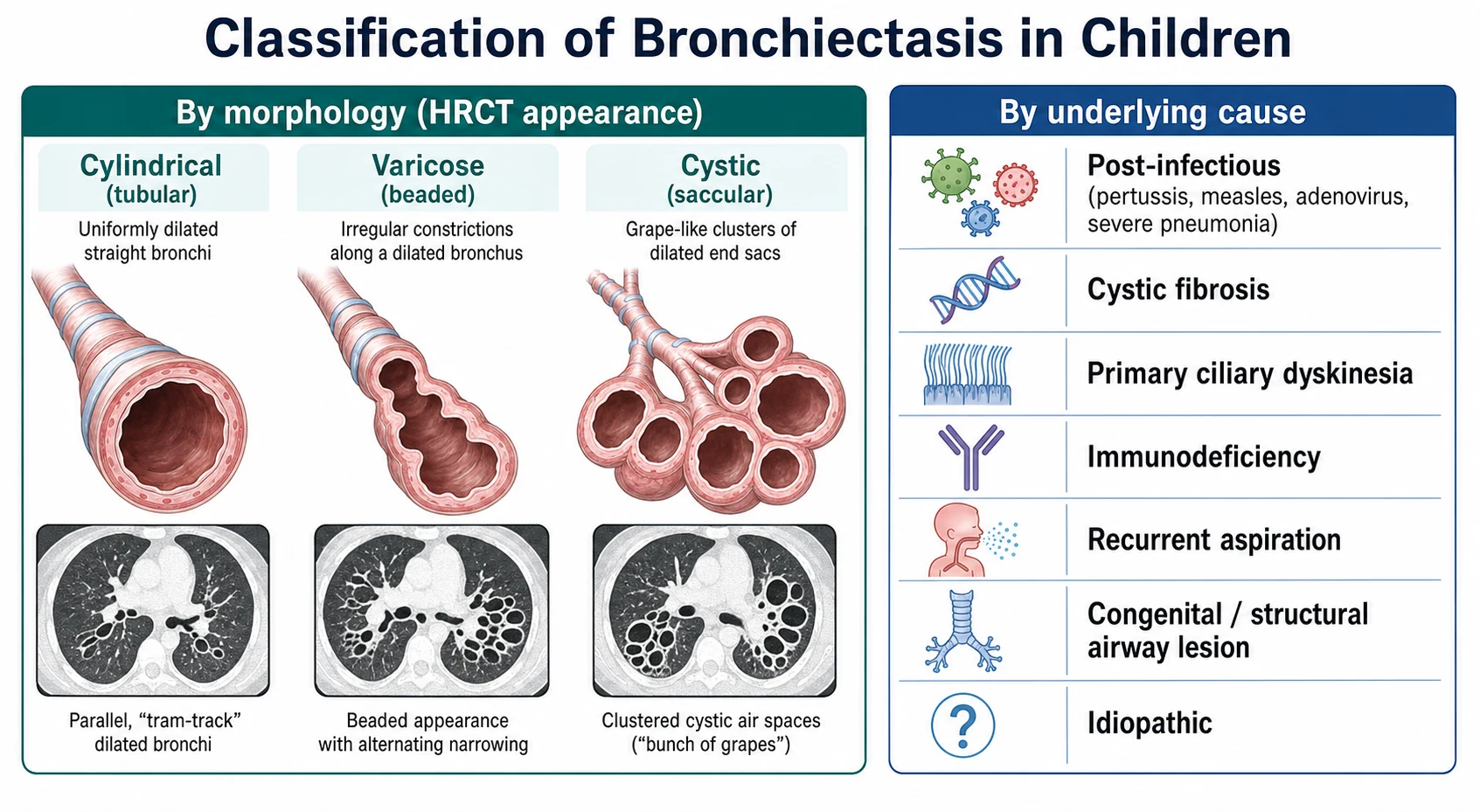
On the scan the disease takes one of three shapes. Cylindrical, or tubular, bronchiectasis is the mildest and commonest, with uniformly dilated airways. Varicose bronchiectasis shows a beaded airway with alternating dilatation and constriction. Cystic, or saccular, bronchiectasis is the most severe, with clusters of ballooned end-sacs. The morphology gives a sense of severity, but it does not tell you the cause and rarely changes the immediate plan. [5] [1]
The classification that actually drives management is by underlying cause. A first, treatable group follows a severe or repeated infection — pertussis, measles, adenovirus, tuberculosis, or a severe pneumonia — that scars the airway. A second group reflects a systemic defect of airway defence: cystic fibrosis, primary ciliary dyskinesia, or an immunodeficiency. A third follows recurrent aspiration or a structural lesion such as a retained foreign body or congenital malformation. When no cause is found despite thorough testing, the disease is labelled idiopathic. [4] [10]
Epidemiology & Risk Factors
For decades paediatric bronchiectasis was dismissed as a rarity confined to the pre-antibiotic past, and this neglect is exactly why it is now described as no longer an orphan disease. It is more common than once believed, it is under-recognised in primary care, and its true burden falls hardest on children in disadvantaged and Indigenous communities where rates rank among the highest in the world. [4] [2]
The risk factors are the conditions and exposures that let infection and inflammation gain a lasting foothold in the airway. Severe or recurrent lower respiratory infection in early childhood, an inadequately treated protracted bacterial bronchitis, and incomplete immunisation all raise the risk, as do any of the systemic host defects that cripple airway defence. Environmental tobacco smoke, indoor air pollution, crowding, and socioeconomic disadvantage amplify every one of these. [10] [4]
Geography and equity shape the epidemiology as much as biology does. In affluent settings a systemic cause such as immunodeficiency or ciliary dyskinesia is proportionally more often found, whereas in disadvantaged and developing settings post-infectious disease dominates and children present later with more severe damage. In Aboriginal, Torres Strait Islander, Māori, and Pacific children the burden is strikingly high, and much of it is preventable with earlier recognition and treatment. [10] [2]
Pathophysiology
Bronchiectasis is the visible scar left by a cycle that feeds on itself. Once an initial insult impairs the airway's ability to clear mucus, secretions stagnate, bacteria colonise the pooled mucus, and a chronic neutrophilic inflammation sets in. That inflammation releases enzymes that digest the airway wall, so the bronchus dilates and drains even worse than before, which invites more infection. This self-perpetuating loop is the vicious cycle, and it is the mechanism to be able to draw and explain. [1] [11]
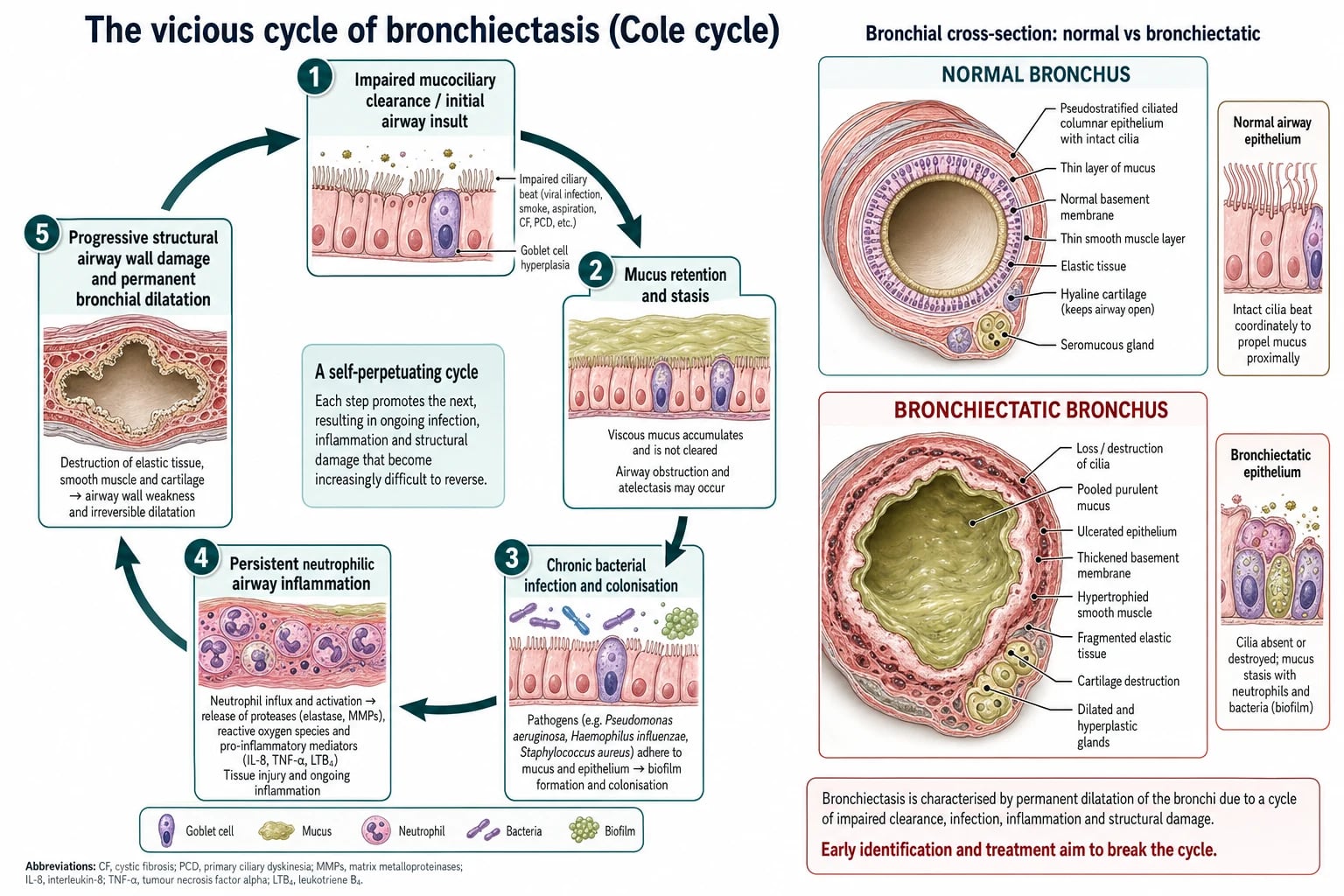
The starting insult differs with the cause, but the cycle is common to all of them. A severe infection can directly injure the airway and mucociliary escalator; cystic fibrosis makes the mucus thick and unclearable; primary ciliary dyskinesia leaves the cilia immotile so mucus is never swept upward; and an immunodeficiency lets ordinary organisms establish chronic infection. Whichever door the disease comes through, it converges on retained infected secretions in an inflamed airway. [1] [6]
The bacteriology of that chronic infection matters clinically. Non-typeable Haemophilus influenzae is the organism most often recovered from children with chronic suppurative lung disease and early bronchiectasis, with Streptococcus pneumoniae and Moraxella catarrhalis also common. The growth of Pseudomonas aeruginosa is a marker of more advanced disease and predicts a worse trajectory, which is why it prompts eradication rather than watchful waiting. [11] [1]
This mechanism explains why the disease can be reversible early and irreversible late. In its earliest stage the airway wall is inflamed but structurally intact, and interrupting the cycle with airway clearance and antibiotics allows recovery; scans in young children can even normalise. Once repeated inflammation has destroyed the elastic and muscular wall, the dilatation is fixed, and treatment can only slow further loss rather than restore the airway. The pathophysiology is therefore also the argument for acting early. [1] [9]
Clinical Presentation
The presentation that must trigger the whole approach is the chronic wet cough. A child with bronchiectasis coughs productively for weeks on end, the cough sounds rattly or moist rather than dry, and although a course of antibiotics may briefly quieten it, the cough returns within days of stopping. Parents often describe a child who is "never really well" or who "always has a chest," and it is this failure to clear between illnesses that separates suppurative lung disease from ordinary recurrent viral coughs. [1] [5]
Between the flares the older child may look deceptively well, but the history and examination hold clues that the disease is established. Exertional breathlessness, reduced stamina, recurrent documented chest infections, and, in advanced disease, haemoptysis all point to significant airway damage. A careful history also asks about the features that suggest a specific cause, from neonatal respiratory distress and chronic ear and sinus disease to feeding difficulty, faltering growth, and infections beyond the chest. [6] [1]
Certain accompanying findings raise the stakes and mark disease that is already advanced. Digital clubbing, chest-wall deformity, faltering growth, and fixed focal crackles that persist between infections all signal established suppurative disease rather than a passing illness. These are the signs that should convert a repeat prescription into a referral for imaging and a search for the cause. [1] [4]
Differential Diagnosis
The first differential to settle is why the cough is chronic and wet at all, because several conditions mimic each other at the wet-cough stage. Protracted bacterial bronchitis is the closest and commonest — a persistent wet cough that resolves fully with an adequate antibiotic course and, crucially, has a normal HRCT. Recurrent or unresolved protracted bacterial bronchitis is a recognised precursor to bronchiectasis, so it sits on the same continuum rather than beside it. [1] [11]
Once the HRCT confirms bronchiectasis, the differential becomes the list of underlying causes, and the exam reward is showing that you would work through it systematically rather than stop at the scan. Cystic fibrosis, primary ciliary dyskinesia, immunodeficiency, recurrent aspiration, a retained foreign body, congenital airway malformation, and post-infectious scarring must each be considered and, where indicated, actively excluded. Asthma is a frequent misdiagnosis in these children and rarely explains a genuinely wet cough. [4] [6]
The trap to avoid is anchoring on asthma or on "recurrent viral infections" and never crossing the line into imaging and a host work-up. A genuinely wet cough that persists despite treatment is the sign that pulls you off those comfortable labels and onto the bronchiectasis pathway, where the job is to prove or exclude a specific, often treatable cause. [1] [4]
Clinical & Bedside Assessment
The history carries most of the diagnostic weight and has three jobs: characterise the cough, gauge the severity, and hunt for the cause. Establish that the cough is genuinely wet and daily, how long it has lasted, and whether it clears between antibiotic courses. Ask about exercise tolerance, documented chest infections, and haemoptysis to judge severity, then take a focused systems history covering the neonatal period, ear and sinus disease, feeding and swallowing, growth, stooling, and family history of cystic fibrosis, immune disease, or consanguinity. [1] [6]
The examination is a deliberate search for the fingerprints of established damage and of the underlying disorder. Plot the growth carefully, inspect for digital clubbing and chest-wall deformity, and listen for fixed focal crackles or reduced breath sounds that persist between infections. Look beyond the chest for the cardiac, neurodevelopmental, and nutritional signs of a systemic predisposition, and examine the upper airway for the chronic rhinosinusitis and glue ear that accompany ciliary disease. [6] [1]
Bedside spirometry adds objective information in the school-aged child and typically shows an obstructive or mixed pattern that helps track disease over time, although a normal result does not exclude significant structural disease. The most valuable bedside habit, however, remains the simplest: taking the wet cough seriously and documenting whether it truly clears, because that single observation decides whether the child needs the full pathway. [9] [1]
Investigations
Investigation runs on two tracks that proceed together: confirm the airway change, and find the cause. The chest high-resolution CT is the diagnostic test, showing bronchial dilatation with a bronchus wider than its adjacent artery, airways visible in the peripheral lung, and failure of the airways to taper. A plain chest radiograph is insensitive and a normal film never excludes the diagnosis, so a convincing clinical picture warrants HRCT rather than reassurance. [1] [5]
The aetiological work-up is done in every child, because a specific cause is found in the majority and because several of the causes are directly treatable. The core panel screens immune function with immunoglobulins and specific vaccine-response titres, excludes cystic fibrosis with a sweat test and genetics, and pursues primary ciliary dyskinesia with nasal nitric oxide and specialist ciliary testing where the clinical cluster fits. A lower-airway culture, from sputum or from bronchoalveolar lavage, defines the organisms and guides treatment. [4] [6]
Bronchoscopy earns its place when a structural lesion or a retained foreign body is possible, when the disease is localised to one region, or when good-quality lower-airway samples are needed in a young child who cannot expectorate. Direct inspection of the airway, together with quantitative lavage culture, both diagnoses anatomical problems and secures the microbiology that empirical treatment would otherwise miss. Testing is matched to the pattern and the pointers rather than fired off as a reflex panel. [11] [1]
Management — Resuscitation
Bronchiectasis is fundamentally a chronic, clinic-managed disease, but individual exacerbations and complications can present acutely and must be stabilised first. A child with an acute exacerbation, respiratory distress, or hypoxaemia needs oxygen, assessment of work of breathing, and prompt antibiotics, with escalation to intravenous therapy and admission for those who are systemically unwell or failing oral treatment. Stabilise the physiology in front of you before returning to the longer question of control. [3] [1]
A small number of presentations are genuine emergencies. Significant haemoptysis, though uncommon in children, can be life-threatening and demands airway protection, resuscitation, and urgent specialist and interventional input. Severe respiratory failure during an exacerbation, or overwhelming infection in an immunodeficient child, similarly override the elective pathway and need immediate senior involvement. The principle is unchanged: secure airway, breathing, and circulation, then treat the exacerbation and reassess the underlying disease. [1] [3]
Where a retained inhaled foreign body is the suspected trigger of localised disease, the urgency is diagnostic as well as therapeutic. A convincing choking history with same-site disease warrants prompt bronchoscopy even when the child is stable, because continued obstruction drives ongoing airway damage in the affected segment. Escalate early rather than watch and wait. [11] [1]
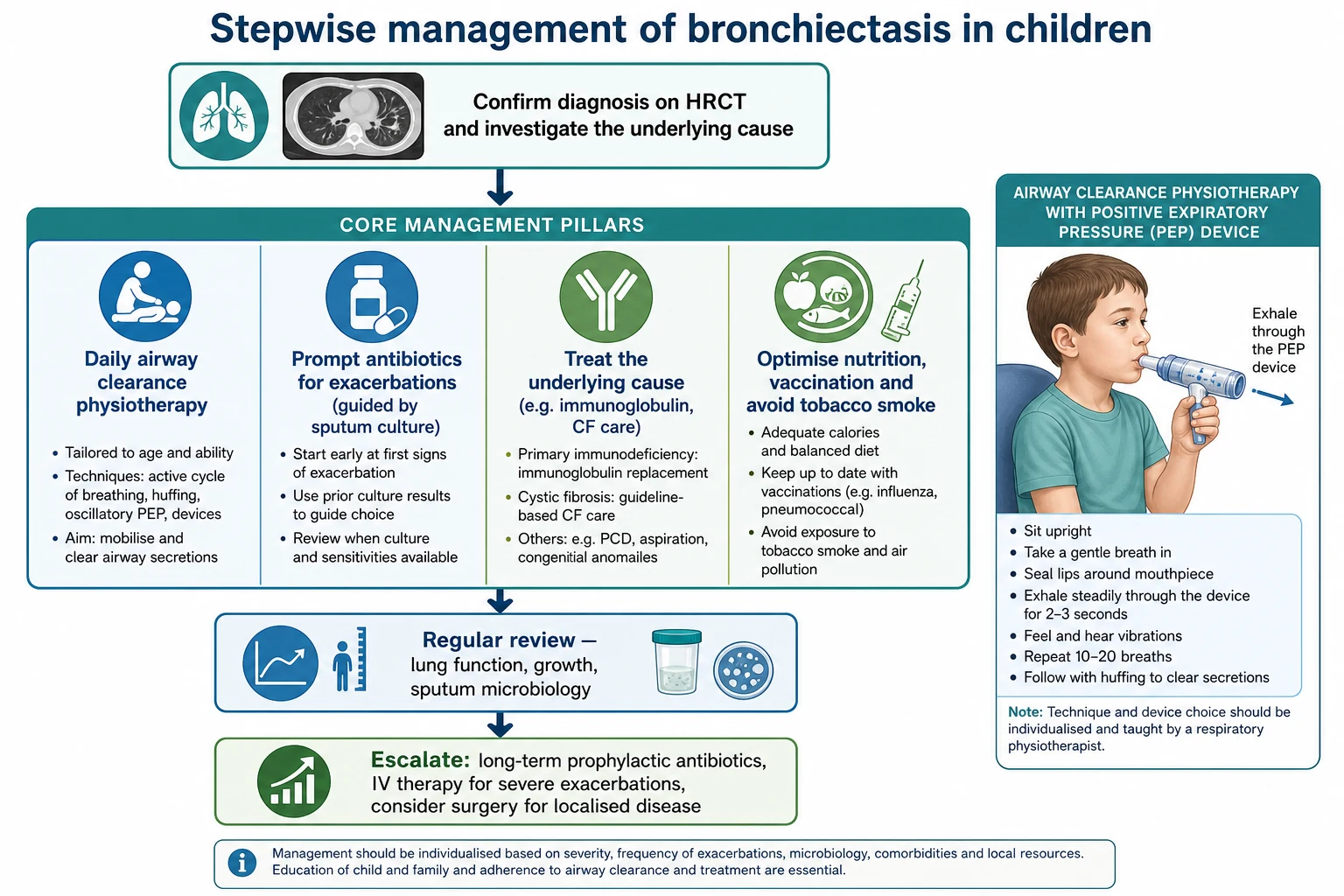
Management — Definitive & Stepwise
Definitive management rests on two pillars that run for years: keep the airways clear, and treat infection promptly and adequately, all while correcting the underlying cause wherever possible. Daily airway clearance physiotherapy, taught by a physiotherapist and adapted to the child's age, is the foundation, using techniques and devices that mobilise and expel the retained secretions that feed the vicious cycle. Regular exercise, good nutrition, complete immunisation including influenza and pneumococcal vaccines, and avoidance of tobacco smoke support the airway between flares. [3] [1]
Exacerbations — signalled by increased cough, a change in sputum, or systemic upset — are treated with a prolonged antibiotic course rather than the short one used for an ordinary chest infection. Treatment is guided by the child's own airway cultures, with amoxicillin-clavulanate a common oral first-line choice because it covers non-typeable Haemophilus influenzae. The BEST-2 trial showed oral azithromycin to be non-inferior to amoxicillin-clavulanate for treating exacerbations, giving a useful alternative, particularly where adherence or allergy is an issue. [7] [3]
Amoxicillin-clavulanate (exacerbation, oral first-line)
Dose
About 45 mg/kg/day of the amoxicillin component in two divided doses; treat for a prolonged course of about 14 days rather than the short course used for simple infection
For selected children with frequent exacerbations, long-term macrolide prophylaxis reduces the exacerbation rate. The Bronchiectasis Intervention Study showed that long-term azithromycin roughly halved exacerbations in Indigenous children with bronchiectasis or chronic suppurative lung disease, at the cost of increased carriage of macrolide-resistant organisms — a trade-off that must be weighed and monitored. Macrolide prophylaxis is therefore reserved for children with a genuinely high exacerbation burden, after cystic fibrosis and non-tuberculous mycobacterial infection have been considered. [8] [3]
Azithromycin (long-term prophylaxis, selected children)
Dose
About 30 mg/kg once weekly, or a comparable thrice-weekly regimen, continued for months in children with frequent exacerbations
Cause-specific and escalated treatment complete the plan. An immunodeficiency is treated with immunoglobulin replacement, cystic fibrosis and ciliary dyskinesia are managed within specialist multidisciplinary teams, aspiration is reduced with feeding modification, and a foreign body is removed. Pseudomonas aeruginosa is eradicated when first isolated. Surgery, in the form of resection, is reserved for the uncommon child with localised disease that continues to cause major symptoms despite optimal medical therapy. [1] [3]
Stepwise approach to bronchiectasis in children
Take the chronic wet cough seriously: more than four weeks, recurring after antibiotics, is suppurative lung disease
Confirm the diagnosis on chest HRCT — a bronchus wider than its adjacent artery, with airways failing to taper
Work up the cause in every child: immune screen, sweat test and CF genetics, ciliary studies, airway culture, and bronchoscopy where indicated
Treat exacerbations with prolonged, culture-guided antibiotics, escalating to intravenous therapy for severe disease
Maintain daily airway clearance physiotherapy, nutrition, exercise, immunisation, and smoke avoidance
Escalate to long-term macrolide prophylaxis, Pseudomonas eradication, or surgery for localised disease as needed, all under specialist review
Causes of childhood bronchiectasis — CHILD-BRONCH
Specific Subtypes & Scenarios
Cystic fibrosis is the systemic subtype that must never be missed, because it is the classic cause of diffuse bronchiectasis and has a specific, life-changing treatment pathway. Faltering growth, steatorrhoea, salt-loss, and early Pseudomonas or Staphylococcus infection point to it, and a sweat test with genetics confirms it. Even in regions with newborn screening, a sweat test is warranted whenever the clinical picture fits, and its exclusion is a mandatory step before a child is labelled with non-cystic fibrosis bronchiectasis. [1] [4]
Primary ciliary dyskinesia is the subtype that hides in plain sight, presenting with the same chronic wet cough plus a telltale cluster: unexplained neonatal respiratory distress in a term infant, chronic rhinosinusitis and glue ear from infancy, and, in about half of cases, situs inversus. Diagnosis rests on nasal nitric oxide screening followed by specialist ciliary function and structural studies, and recognising the cluster is what prompts the right test. [6] [1]
Post-infectious bronchiectasis is the subtype that dominates in disadvantaged and Indigenous communities and is the most preventable of all. A severe or repeated early infection — pertussis, measles, adenovirus, tuberculosis, or a severe pneumonia — scars the developing airway, and inadequate access to timely treatment and immunisation lets the vicious cycle become established. Here the same clinical vigilance and early treatment that help any child are also a matter of health equity. [2] [10]
Complications & Pitfalls
The gravest complication is the disease itself becoming fixed and progressive: repeated infection and inflammation that are never adequately interrupted destroy the airway wall, entrench the dilatation, and drive a slow decline in lung function toward respiratory failure in adulthood. Chronic infection with Pseudomonas aeruginosa marks and accelerates this trajectory, and recurrent exacerbations, haemoptysis, and impaired growth all mark disease that is not under control. [1] [9]
The commonest day-to-day pitfall is the antibiotic merry-go-round: repeated short courses for the same recurring wet cough, with no one ever asking why the airway keeps failing or crossing the line into imaging and a host work-up. This delays diagnosis, allows ongoing airway damage during the window when it is still reversible, and misses treatable causes. The corrective discipline is cheap and simple: recognise the persistent wet cough, treat it properly, and investigate the cause. [4] [1]
Prognosis & Disposition
Prognosis in childhood bronchiectasis is far better than its adult reputation suggests, and it turns almost entirely on how early the disease is caught and how well the vicious cycle is controlled. In young children, early bronchiectasis on HRCT can regress with intensive airway clearance and infection control, and lung function can stabilise or even improve when the disease is managed well. The disease is not an inevitable slide, but a condition whose course the clinician can genuinely change. [1] [9]
The children who do badly are those diagnosed late, those with poorly controlled infection, and those chronically infected with Pseudomonas aeruginosa, in whom lung function declines and the damage becomes fixed. Longitudinal data show that lung function stability depends on the intensity and consistency of treatment and on preventing recurrent exacerbations, which is the practical argument for structured, adherent, long-term care. [9] [1]
Disposition is therefore about placing every child in structured, multidisciplinary respiratory follow-up rather than serial primary-care antibiotic courses. Each child needs a written plan covering daily airway clearance, an exacerbation action plan, immunisation, and regular monitoring of symptoms, growth, lung function, and airway microbiology. Closing the loop on the underlying cause and on Pseudomonas status is part of every review. [3] [2]
Special Populations
Aboriginal, Torres Strait Islander, Māori, and Pacific children carry among the highest rates of bronchiectasis in the world, and they are the group most harmed by delayed recognition. In these children a chronic wet cough warrants early, decisive assessment and treatment, delivered through culturally safe and accessible services, with a low threshold for HRCT and for diagnosing chronic suppurative lung disease. Much of this burden is preventable, and early action is as much an equity intervention as a clinical one. [2] [10]
Children with immunodeficiency, whether a primary antibody deficiency or immune compromise from treatment, develop recurrent and chronic airway infection that drives bronchiectasis, and a child who looks well between episodes can still harbour a serious defect. A pattern of recurrent sinopulmonary infection, infections beyond the chest, or a poor vaccine response should prompt immunoglobulin measurement and specialist immunology input, because immunoglobulin replacement changes the trajectory. [4] [1]
Children with neurodevelopmental disability and unsafe swallowing are prone to aspiration-driven suppurative disease and bronchiectasis, often compounded by weak cough and poor airway clearance. Their care centres on a formal swallow and feeding assessment, modification of feed texture and route, control of secretions and reflux, and diligent airway clearance, recognising that the chronic wet cough here is a marker of an ongoing airway-protection problem. [1] [3]
Evidence, Guidelines & Regional Differences
The modern evidence base reframed paediatric bronchiectasis from a forgotten rarity into a recognised, actively managed, and partly preventable disease, and the review literature makes the case that it is no longer an orphan condition. The overarching messages are consistent: the chronic wet cough is the entry point, HRCT confirms the diagnosis, a cause is found in most children, and early treatment can reverse early disease. [4] [1]
Formal guidance now anchors practice on both sides of the world. The Thoracic Society of Australia and New Zealand guidelines codify the chronic suppurative lung disease continuum and place particular emphasis on the high burden in Indigenous children and the need for early action, while the European Respiratory Society statement provides a structured framework for diagnosis, aetiological work-up, and management across childhood and adolescence. The ERS primary ciliary dyskinesia standards underpin the systemic part of the work-up. [2] [3]
The therapeutic evidence has matured through paediatric-specific trials. The BEST-2 trial established oral azithromycin as non-inferior to amoxicillin-clavulanate for treating exacerbations, and the Bronchiectasis Intervention Study showed that long-term azithromycin reduces exacerbations while increasing macrolide resistance. The genuine controversies now sit at the edges: the precise indications and duration of macrolide prophylaxis given the resistance trade-off, and the narrow role of surgery in localised disease. [7] [8]
Exam Pearls
The highest-yield spine to recite is the continuum and its entry point: a chronic wet cough beyond four weeks that recurs after antibiotics is chronic suppurative lung disease, the reversible front end of bronchiectasis, and the moment to act. Bronchiectasis itself is confirmed on HRCT but is never the endpoint — it is a symptom demanding a systematic search for a treatable cause. Hold those two lines and the topic organises itself. [1] [2]
The causes are the second set-piece. Learn the systemic host defects — cystic fibrosis, primary ciliary dyskinesia, and immunodeficiency — alongside the post-infectious, aspiration, and structural groups, because reciting them shows an examiner you would investigate in a rational order rather than stop at the scan. A sweat test, an immune screen, and ciliary studies are the core tests that catch the common and treatable causes. [4] [6]
Finally, demonstrate the management and equity instincts. Daily airway clearance and prolonged culture-guided antibiotics are the two pillars, azithromycin is a proven option for both treatment and prophylaxis with a resistance trade-off, and Pseudomonas is eradicated when found. Showing that you would act early — especially in Indigenous and disadvantaged children where the burden is highest and the disease most preventable — is what marks the candidate who understands why childhood bronchiectasis matters. [8] [2]
References
- [1]Chang AB, Bush A, Grimwood K Bronchiectasis in children: diagnosis and treatment. Lancet, 2018.PMID 30215382
- [2]Chang AB, Bell SC, Torzillo PJ, et al Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand Thoracic Society of Australia and New Zealand guidelines. Med J Aust, 2015.PMID 25588439
- [3]Chang AB, Fortescue R, Grimwood K, et al European Respiratory Society guidelines for the management of children and adolescents with bronchiectasis. Eur Respir J, 2021.PMID 33542057
- [4]Goyal V, Grimwood K, Marchant J, et al Pediatric bronchiectasis: No longer an orphan disease. Pediatr Pulmonol, 2016.PMID 26840008
- [5]Redding GJ Bronchiectasis in children. Pediatr Clin North Am, 2009.PMID 19135586
- [6]Lucas JS, Barbato A, Collins SA, et al European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur Respir J, 2017.PMID 27836958
- [7]Goyal V, Grimwood K, Byrnes CA, et al Amoxicillin-clavulanate versus azithromycin for respiratory exacerbations in children with bronchiectasis (BEST-2): a multicentre, double-blind, non-inferiority, randomised controlled trial. Lancet, 2018.PMID 30241722
- [8]Valery PC, Morris PS, Byrnes CA, et al Long-term azithromycin for Indigenous children with non-cystic-fibrosis bronchiectasis or chronic suppurative lung disease (Bronchiectasis Intervention Study): a multicentre, double-blind, randomised controlled trial. Lancet Respir Med, 2013.PMID 24461664
- [9]Kapur N, Masters IB, Chang AB Longitudinal growth and lung function in pediatric non-cystic fibrosis bronchiectasis: what influences lung function stability? Chest, 2010.PMID 20173055
- [10]Kapur N, Karadag B Differences and similarities in non-cystic fibrosis bronchiectasis between developing and affluent countries. Paediatr Respir Rev, 2011.PMID 21458736
- [11]Chang AB, Boyce NC, Masters IB, et al Bronchoscopic findings in children with non-cystic fibrosis chronic suppurative lung disease. Thorax, 2002.PMID 12403874