Paeds · respiratory-sleep-and-airway
Chronic cough: diagnostic approach
Also known as Persistent cough in children · Chronic paediatric cough · Prolonged cough · Wet cough in children · Chronic wet cough evaluation
Fellowship guide to chronic cough in children — the four-week threshold, the wet-versus-dry split that drives the whole work-up, protracted bacterial bronchitis as the commonest cause, the specific-cough pointers that flag serious disease, and the evidence-based algorithm that turns a vague symptom into a diagnosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent brings a four-year-old to clinic exhausted, describing a cough that has run for six weeks, wakes the household, and has already earned two courses of salbutamol that did nothing. The temptation is to reach for the adult reflexes — asthma, reflux, post-nasal drip — but in a child that instinct is usually wrong. The first move is quieter and far more powerful: listen to the cough and ask whether it is wet or dry, and count how long it has truly lasted. [1]
Chronic cough is defined by duration, and the paediatric threshold is a daily cough persisting for more than four weeks. This is deliberately shorter than the eight-week adult definition, because a child who is still coughing at a month rarely has a lingering viral tail and more often has an identifiable, treatable cause. Between three and four weeks sits a grey zone of "prolonged acute cough," most of which is post-viral and settles, but the four-week mark is the point at which a systematic work-up becomes mandatory. [1] [2]
The reason the definition matters is that it forces a decision rather than a wait. An isolated dry cough in an otherwise well, thriving child with a normal examination and chest X-ray is usually non-specific and self-limiting, and the safest management is watchful review. A wet cough, by contrast, almost always signals airway secretions that need explaining, and it is the finding that should never be waved away as "just a virus." [2]
Classification
The classification that drives everything is not by cause but by the character and context of the cough. First, split it by quality: a wet or productive cough implies excessive airway secretions and suppurative disease, while a dry cough points toward airway irritation, hyperresponsiveness, or a non-specific process. Second, split it by whether there are pointers to specific underlying disease. This wet-versus-dry, specific-versus-non-specific grid is the scaffold of every published paediatric cough algorithm. [1] [5]
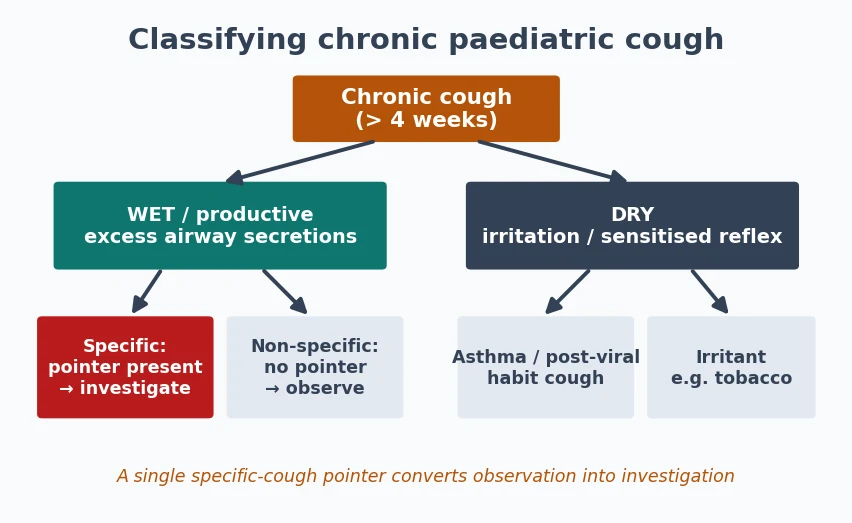
Specific cough describes a cough accompanied by any pointer to an underlying diagnosis — a wet cough, digital clubbing, failure to thrive, chest-wall deformity, exertional dyspnoea, a cardiac murmur, recurrent pneumonia, neurodevelopmental disease with aspiration risk, or a history of choking. Non-specific cough is a dry cough in a well child with none of these pointers, a normal examination, and a normal chest radiograph. The two demand entirely different responses: one is investigated, the other is observed. [1] [2]
There is a further practical split by age. Cough dating from birth or the neonatal period raises congenital airway malformation, tracheo-oesophageal fistula, primary ciliary dyskinesia, or cardiac disease, whereas cough beginning in the toddler years after a choking episode raises retained foreign body. The same duration means different things at different ages, and the history must anchor the cough in time. [1]
Epidemiology & Risk Factors
Cough is the single most common symptom bringing children to primary care, and while most is acute and viral, a meaningful minority crosses the four-week line into chronic territory. In pooled paediatric cohorts, protracted bacterial bronchitis is consistently the leading cause of chronic wet cough in preschool children, ahead of asthma and far ahead of the reflux and upper-airway causes that dominate adult series. Knowing this prevalence gradient is what stops you from mis-mapping an adult framework onto a child. [3] [6]
The risk factors cluster around airway exposure and host defence. Environmental tobacco smoke is the strongest and most modifiable, roughly doubling the risk and worsening every cough it touches; day-care attendance, older siblings, indoor air pollution, and biomass exposure add to the burden. Recurrent or severe early respiratory infection, prematurity, and any condition impairing airway clearance raise the risk of a cough that will not settle. [1] [10]
Certain populations carry a disproportionate burden of suppurative airway disease, and the cough that heralds it is easy to under-treat. Aboriginal and Torres Strait Islander children, and children in other socioeconomically disadvantaged and remote communities, have markedly higher rates of chronic wet cough, protracted bacterial bronchitis, and bronchiectasis. In these children a wet cough is a red flag demanding early, decisive treatment rather than serial reassurance. [10] [6]
Pathophysiology
Cough is a protective reflex, and understanding its arc explains why a child coughs differently from an adult. Sensory receptors in the larynx, trachea, and large airways — responding to mechanical touch, secretions, and chemical irritants — fire along vagal afferents to the cough centre in the brainstem, which drives the explosive expiratory effort that clears the airway. When that reflex is triggered persistently, either by ongoing secretions or by a sensitised pathway, the cough becomes chronic. [1]
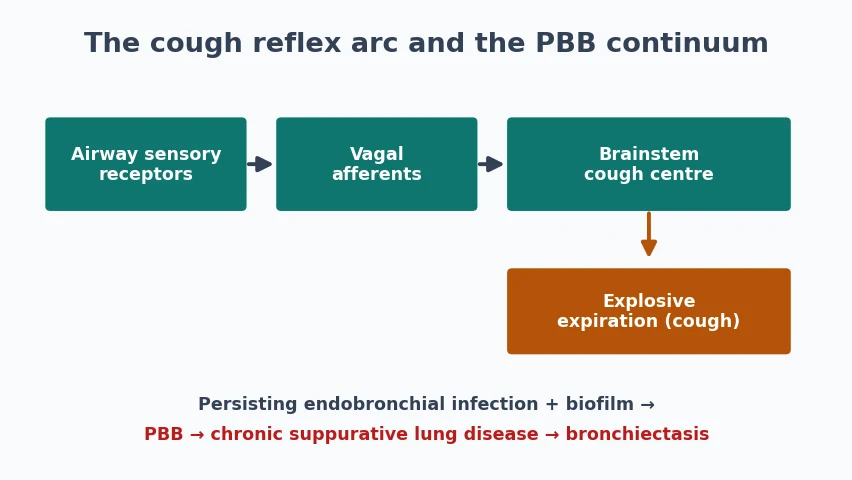
In protracted bacterial bronchitis, the dominant paediatric mechanism, the problem is a persisting endobronchial infection. Bacteria — typically non-typeable Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis — establish a biofilm on the airway mucosa, provoking neutrophilic inflammation and mucus production that keep the cough wet and productive. The immature or transiently impaired mucociliary clearance of the young airway allows this cycle to persist, which is why the cough responds to a prolonged rather than a short antibiotic course. [6] [4]
If that infective-inflammatory cycle is left to run, it feeds a continuum toward permanent airway damage. Persistent neutrophilic inflammation and repeated infection dilate and scar the bronchi, converting reversible protracted bacterial bronchitis into chronic suppurative lung disease and ultimately bronchiectasis. This continuum is the single most important concept in the topic: the wet cough you dismiss today can become the dilated airway you cannot repair tomorrow. [6] [4]
A separate mechanism explains cough hypersensitivity. In some children, and more commonly in adolescents, the cough reflex pathway becomes sensitised so that trivial stimuli provoke cough long after any trigger has resolved — the basis of post-viral cough and of the habit or somatic cough that persists in the absence of disease. Recognising this sensitised, non-suppurative mechanism keeps you from over-investigating a dry cough in a thriving child. [1]
Clinical Presentation
The presentation that should reassure you is the well child with a dry, non-specific cough. Growth is on track, the chest is clear, exercise is unlimited, and the cough — though it worries the family and disrupts sleep — carries no accompanying signs. This picture, especially following a viral illness, is the commonest reason for referral and the one most likely to resolve with time and a clear explanation rather than a prescription. [1]
The presentation that should mobilise you is the wet cough. A cough that sounds rattly or productive, that clears mucus, and that has run for weeks is the signature of protracted bacterial bronchitis and, at the severe end, of suppurative lung disease. The parent may describe the child as "always chesty," a cough that never fully clears between colds, and it is precisely this failure to return to a cough-free baseline that distinguishes pathology from recurrent viral illness. [6] [4]
Between these poles lie the presentations that carry specific pointers, and the history must actively seek them. Ask about cough from the first days of life, a sudden choking or gagging episode, exertional breathlessness, blood in the cough, recurrent pneumonias, feeding difficulty or aspiration risk, and any faltering of growth. Each of these shifts a benign-sounding cough into the specific category that must be investigated. [1] [2]
Differential Diagnosis
Hold the differential as a short, prioritised list built around cough quality and age, and the diagnoses fall into place. For the chronic wet cough, protracted bacterial bronchitis leads by a wide margin, followed by the suppurative spectrum of chronic suppurative lung disease and bronchiectasis, then recurrent aspiration, retained foreign body, and, in the right setting, cystic fibrosis or primary ciliary dyskinesia. The wet cough is a diagnosis-rich symptom and every one of these is treatable if named. [6] [4]
For the chronic dry cough in a well child, the list is shorter and more benign: non-specific isolated cough and post-viral cough dominate, with asthma, tic or habit cough, and irritant exposure such as tobacco smoke behind them. The crucial caveat is that a dry cough alone, without wheeze or exertional symptoms, is a poor predictor of asthma in children, and reflexively labelling it asthma leads to years of futile inhalers. [1] [2]
The adult "diagnostic triad" of asthma, gastro-oesophageal reflux, and upper-airway cough syndrome deserves explicit demotion. These entities cause the great majority of adult chronic cough but rarely explain isolated chronic cough in a young child, and empirical treatment for them — inhaled steroids, acid suppression, antihistamines — is a common and evidence-poor detour. Reserve these diagnoses for children with the specific symptoms that genuinely accompany them. [2] [10]
Clinical & Bedside Assessment
The history is the highest-yield investigation, and it has three tasks: characterise the cough, place it in time, and hunt for pointers. Establish whether it is wet or dry, its true daily duration, its relationship to feeds, exercise, sleep, and posture, and whether it ever fully clears. Then take a birth, developmental, immunisation, and environmental history — tobacco exposure above all — and ask directly about choking episodes and family history of atopy, cystic fibrosis, or immune disease. [1] [2]
The examination is a deliberate search for the specific-cough pointers rather than a routine listen. Plot growth on a centile chart, inspect for digital clubbing and chest-wall deformity, and observe the work and pattern of breathing. Auscultate for focal or persistent added sounds, wet crackles, or wheeze, and examine the upper airway and cardiovascular system. A single positive pointer — clubbing, a focal sign, faltering growth — converts the whole assessment from observation to investigation. [1] [2]
Watching and listening to the cough itself is often diagnostic. A wet, loose cough directs you to the suppurative pathway; a barking, brassy cough suggests tracheomalacia or croup-like disease; a honking cough that vanishes during sleep and concentrates when observed suggests a habit cough; and a paroxysmal cough with a whoop points to pertussis. If you cannot hear the cough in clinic, a smartphone recording from the family is a legitimate and validated substitute. [1] [10]
Investigations
Investigation is staged and driven by the clinical category, not ordered as a reflex battery. Every child with a genuine chronic cough deserves two baseline tests: a chest radiograph and, where the child is old enough to perform it, spirometry with bronchodilator response. A normal chest X-ray and normal spirometry in a well child with a dry cough strongly support a non-specific cough and justify watchful review. [2] [1]
When the cough is wet or a specific pointer is present, the work-up deepens in a logical order. Collect a lower-airway sample — sputum in the older child, or airway cultures at bronchoscopy in the younger — to define the bacteriology and guide antibiotics. Pursue a sweat test and cystic fibrosis genetics, immune function screening, and, where suppurative disease is suspected, a chest CT to define bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage assesses airway anatomy, secures microbiology, and excludes a retained foreign body or airway malformation. [6] [4]
Restraint is as important as thoroughness. There is no place for a shotgun panel of allergy tests, reflux studies, and empirical trials in a well child with a non-specific dry cough, and each unnecessary investigation carries cost, radiation, or a false lead. Match the depth of the work-up to the presence of pointers and to the response to a rational first treatment. [2] [5]
Management — Resuscitation
Chronic cough is rarely an emergency, but a small number of presentations demand immediate action rather than a diagnostic pathway. A child with acute respiratory distress, stridor, drooling, or a suspected complete airway foreign body needs urgent airway assessment and stabilisation before any elective work-up, following standard paediatric airway and resuscitation priorities. Recognising when a "chronic cough" referral is actually an acute airway threat is the safety net of the topic. [1]
Massive or recurrent haemoptysis, severe hypoxaemia, or acute decompensation of underlying suppurative lung disease also override the elective algorithm. These children need oxygen, monitoring, senior and specialist involvement, and urgent imaging, not a symptomatic cough medicine. The principle is simple: treat the physiology first, then return to the diagnosis. [1]
Finally, the "resuscitation" of a suspected inhaled foreign body is diagnostic urgency rather than pharmacology — a witnessed choking episode with ongoing cough warrants prompt bronchoscopy even when the child looks stable and the film is clear, because delayed retrieval risks distal infection and airway damage. Escalate early rather than observe. [1]
Management — Definitive & Stepwise
Definitive management follows the diagnosis, and for the commonest cause it is refreshingly concrete. A chronic wet cough with no other pointer is treated as protracted bacterial bronchitis with a trial of appropriate oral antibiotics for at least two weeks, and amoxicillin-clavulanate is the agent with the strongest randomised evidence. Resolution of the cough within this period both treats the child and confirms the diagnosis. [7] [4]
The wet-cough pathway has a built-in decision point. If the cough clears with the first course, the diagnosis is protracted bacterial bronchitis and no further action is needed beyond safety-netting. If it partially responds or recurs, extend to a four-week course; if it still fails to clear after adequate antibiotics, escalate to flexible bronchoscopy, chest CT, and a full search for underlying suppurative lung disease, immunodeficiency, aspiration, or a retained foreign body. Persistent wet cough despite treatment is the signal to investigate deeply, never to keep re-prescribing blindly. [4] [6]
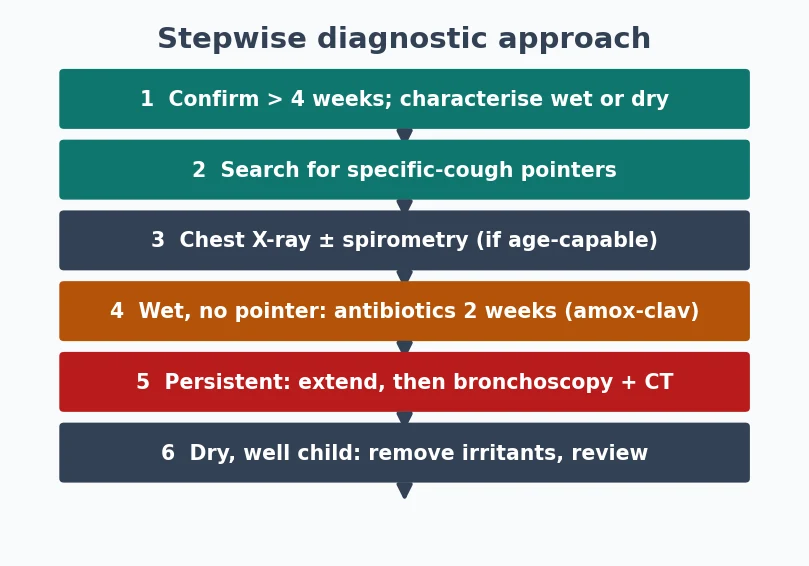
Stepwise diagnostic approach to chronic cough
Confirm a daily cough of more than four weeks and characterise it as wet or dry
Search systematically for specific-cough pointers on history and examination
Obtain a chest X-ray and, if age-capable, spirometry with reversibility
For a wet cough with no other pointer, trial appropriate antibiotics for two weeks
If the cough persists, extend the course then escalate to bronchoscopy and chest CT
For a dry, non-specific cough in a well child, observe, remove irritants, and review in weeks
The dry, non-specific cough is managed by explanation, exposure control, and review rather than by medication. Eliminate tobacco smoke and other irritants, reassure the family about the benign natural history, and arrange a defined review because the cough that later turns wet or acquires a pointer reveals its diagnosis over time. Only if a specific cause such as asthma emerges on that review is targeted treatment started, and then it is monitored for a genuine response rather than continued indefinitely. [1] [2]
Over-the-counter cough and cold medicines have no role. They are ineffective for chronic cough and carry real risk of harm in young children, and prescribing them substitutes a placebo for the diagnostic work the child actually needs. Naming this explicitly to families is part of good management. [2] [10]
CHRONIC — pointers that make a cough specific
Specific Subtypes & Scenarios
Protracted bacterial bronchitis is the subtype to master because it recurs in the exam and the clinic alike. It is defined by an isolated chronic wet cough, absence of pointers to an alternative diagnosis, and resolution with two to four weeks of appropriate antibiotics. Recurrent episodes — more than three a year — should prompt investigation for underlying bronchiectasis or immune deficiency rather than repeated empirical courses. [6] [4]
The inhaled foreign body is the scenario that punishes complacency. Classically a toddler with a sudden choking episode followed by persistent cough, wheeze, or focal signs, it may present late and mimic asthma or recurrent pneumonia. Because most aspirated material is radiolucent, a normal chest X-ray never excludes it, and a convincing history mandates bronchoscopy. Late diagnosis leads to distal bronchiectasis in the affected segment. [1]
The habit or tic cough is the subtype that spares the child from over-investigation once recognised. It is typically a loud, honking, repetitive cough that is absent during sleep and often disappears when the child is distracted or absorbed, occurring in a well child with a normal examination and normal tests. Its recognition rests on the classic pattern and the absence of pointers, and its management is reassurance and, where needed, behavioural techniques rather than drugs or imaging. [1] [2]
Complications & Pitfalls
The gravest complication is the one the diagnosis is designed to prevent: bronchiectasis. A chronic wet cough that is repeatedly dismissed as viral, under-treated, or managed with cough suppressants can progress along the suppurative continuum to irreversible airway dilatation, and this progression is largely preventable with timely antibiotics and follow-through. The complication is not the cough itself but the missed opportunity to treat it. [6] [4]
The commonest day-to-day pitfall is the empirical-treatment merry-go-round: successive trials of bronchodilators, inhaled steroids, antihistamines, and acid suppression, none monitored for response and none stopped when they fail. This adult-style approach delays the correct diagnosis, exposes the child to unnecessary drugs, and erodes the family's confidence. The discipline is to make one rational intervention at a time and to reassess objectively. [2] [5]
Prognosis & Disposition
For the non-specific dry cough the prognosis is excellent. The great majority resolve spontaneously within weeks to a few months, and the family's main need is a confident explanation and a clear review plan rather than treatment. Documenting the benign natural history and safety-netting for the emergence of pointers is the disposition, and most of these children are managed entirely in primary or general paediatric care. [1] [3]
Protracted bacterial bronchitis also carries a good prognosis when treated properly, with most children clearing on a single adequate antibiotic course. The caveat is recurrence: a subset relapse, and repeated episodes flag the children who are travelling toward bronchiectasis and who need specialist respiratory assessment. Timely, adequate treatment and structured follow-up are what separate the good outcome from the bad. [6] [4]
The burden of chronic cough on the family is real and measurable, and it justifies taking the symptom seriously even when the cause is benign. Validated child cough-specific quality-of-life measures show substantial impact on sleep, school, and parental anxiety, all of which improve as the cough is diagnosed and treated. Acknowledging this impact, and following up to confirm resolution, is part of good disposition. [11] [10]
Special Populations
Aboriginal and Torres Strait Islander children, and children in other disadvantaged and remote settings, carry a far higher burden of chronic wet cough, protracted bacterial bronchitis, and bronchiectasis, and they are the group in whom under-treatment causes the most harm. In these children a wet cough warrants early, decisive antibiotic treatment and close follow-up, with a low threshold for investigating for suppurative lung disease. Culturally safe, accessible care and attention to household tobacco smoke are central. [10] [6]
Children with neurodevelopmental disability and impaired airway protection are prone to recurrent aspiration, which presents as a chronic wet cough often related to feeds and posture. The evaluation extends to a feeding and swallow assessment and to strategies that reduce aspiration, and the cough is a marker of a broader airway-protection problem rather than a primary lung disease. [1] [2]
Children with immunodeficiency, whether primary or acquired, and those with underlying conditions such as cystic fibrosis or primary ciliary dyskinesia, present with recurrent or persistent wet cough that resists standard treatment. A chronic cough that recurs despite adequate antibiotics, or that is accompanied by faltering growth or other infections, should trigger an immune and genetic work-up rather than another empirical course. [6] [4]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by the CHEST guidelines, which established the systematic, algorithm-based evaluation of paediatric chronic cough, the central role of cough quality, and the diagnosis and treatment of protracted bacterial bronchitis. The 2017 CHEST reports on chronic wet cough and on the use of management pathways codified the two-week antibiotic trial and the escalation to bronchoscopy when the cough persists. [4] [5]
The value of using an algorithm rather than clinical intuition has been tested directly. Randomised and multicentre studies showed that managing children with a standardised cough algorithm led to earlier resolution and better outcomes than usual care, both for established chronic cough and at the transition from acute to chronic cough. This is unusually strong evidence that the process, not just the diagnosis, changes outcomes. [8] [9]
Regional guidance converges on the core algorithm but differs in emphasis. The Australian CICADA position statement foregrounds the high prevalence of suppurative lung disease and bronchiectasis in Aboriginal and Torres Strait Islander and remote-living children and the imperative to treat wet cough early, while the European Respiratory Society statement focuses on defining and managing protracted bacterial bronchitis. Across all of them the message is identical: characterise the cough, hunt for pointers, treat the wet cough, and follow up. [10] [6]
Exam Pearls
The definition and the first branch point are the highest-yield facts: a daily cough beyond four weeks is chronic, and the opening move is to classify it as wet or dry. Wet means suppurative disease and, in a preschooler, protracted bacterial bronchitis at the top of the list, treated with a two-week course of amoxicillin-clavulanate that both cures and confirms. Hold these two lines and you have the spine of the topic. [1] [7]
The pointers are the second set-piece. Learn the specific-cough pointers as a list you can recite — wet cough, cough from birth, a choking episode, failure to thrive, clubbing, chest-wall deformity, haemoptysis, recurrent pneumonia — because naming them is how you convert observation into investigation and how you avoid missing serious disease. A single pointer changes the whole plan. [1] [2]
Finally, resist the adult reflexes. The asthma-reflux-upper-airway triad that dominates adult cough rarely explains an isolated cough in a young child, over-the-counter cough medicines are ineffective and unsafe, and a normal chest X-ray never excludes an inhaled foreign body. Demonstrating that you manage a child's cough by a paediatric algorithm rather than an adult one is what marks the candidate who understands the topic. [2] [1]
References
- [1]Chang AB, Landau LI, Van Asperen PP, et al Cough in children: definitions and clinical evaluation. Med J Aust, 2006.PMID 16618239
- [2]Chang AB, Glomb WB Guidelines for evaluating chronic cough in pediatrics: ACCP evidence-based clinical practice guidelines. Chest, 2006.PMID 16428719
- [3]Marchant JM, Masters IB, Taylor SM, et al Evaluation and outcome of young children with chronic cough. Chest, 2006.PMID 16685002
- [4]Chang AB, Oppenheimer JJ, Weinberger MM, et al Management of Children With Chronic Wet Cough and Protracted Bacterial Bronchitis: CHEST Guideline and Expert Panel Report. Chest, 2017.PMID 28143696
- [5]Chang AB, Oppenheimer JJ, Weinberger M, et al Use of Management Pathways or Algorithms in Children With Chronic Cough: CHEST Guideline and Expert Panel Report. Chest, 2017.PMID 28104362
- [6]Kantar A, Chang AB, Shields MD, et al ERS statement on protracted bacterial bronchitis in children. Eur Respir J, 2017.PMID 28838975
- [7]Marchant J, Masters IB, Champion A, et al Randomised controlled trial of amoxycillin clavulanate in children with chronic wet cough. Thorax, 2012.PMID 22628120
- [8]Chang AB, Robertson CF, Van Asperen PP, et al A cough algorithm for chronic cough in children: a multicenter, randomized controlled study. Pediatrics, 2013.PMID 23610200
- [9]Chang AB, Oppenheimer JJ, Irwin RS, et al Effectiveness of a chronic cough management algorithm at the transitional stage from acute to chronic cough in children: a multicenter, nested, single-blind, randomised controlled trial. Lancet Child Adolesc Health, 2019.PMID 31635952
- [10]Chang AB, Cheng AT, O'Grady KF, et al Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA). Summary of an updated position statement on chronic cough in Australia. Med J Aust, 2024.PMID 38600861
- [11]Newcombe PA, Sheffield JK, Petsky HL, et al A child chronic cough-specific quality of life measure: development and validation. Thorax, 2016.PMID 26842959