Paeds · respiratory-sleep-and-airway
Recurrent pneumonia and localised lung disease
Also known as Recurrent pneumonia in children · Persistent and recurrent lung consolidation · Right middle lobe syndrome · Recurrent same-site pneumonia · Localised chronic lung disease
Fellowship guide to recurrent pneumonia in children — the two-or-more-in-a-year definition, the single question that reorganises the whole work-up (same site or different sites?), the structural causes behind same-site disease, the systemic causes behind multifocal disease, and the staged investigation that turns a repeat X-ray into a diagnosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old arrives at clinic having had his third episode of pneumonia in eighteen months, each stamped on an X-ray, each treated with antibiotics, each apparently better by the follow-up visit. The parents want reassurance that he is simply unlucky with viruses. The job of the paediatrician is different and more demanding: to decide whether this is a normal run of childhood infection or the signal of a lung that cannot defend one part of itself, and the first step is to count the episodes honestly and look at where they landed. [3]
Recurrent pneumonia is defined by frequency, not severity. The accepted threshold is two or more episodes of pneumonia within a single year, or three or more episodes at any time, with each episode confirmed radiographically and, critically, with the chest film returning to normal between episodes. That interval clearing is what separates recurrent pneumonia from persistent or non-resolving pneumonia, where a single opacity simply never goes away. [1] [3]
The definition matters because it forces a search for an underlying cause. In the landmark case series, a clear majority of children meeting this threshold had an identifiable predisposing condition rather than bad luck, and the same finding has been reproduced across settings. Recurrent pneumonia is therefore treated as a symptom of something, and the diagnostic task is to name that something before repeated infection scars the lung. [1] [2]
Classification
The single most useful move is to ask whether the pneumonia keeps hitting the same lobe or segment, or whether it lands somewhere different each time, because this one distinction sorts the enormous differential into two manageable halves. Same-site recurrence points to a fixed local problem in that part of the lung, while recurrence at varying or multiple sites points to a body-wide failure of airway defence. This is the organising principle of every published approach to the problem. [1] [3]
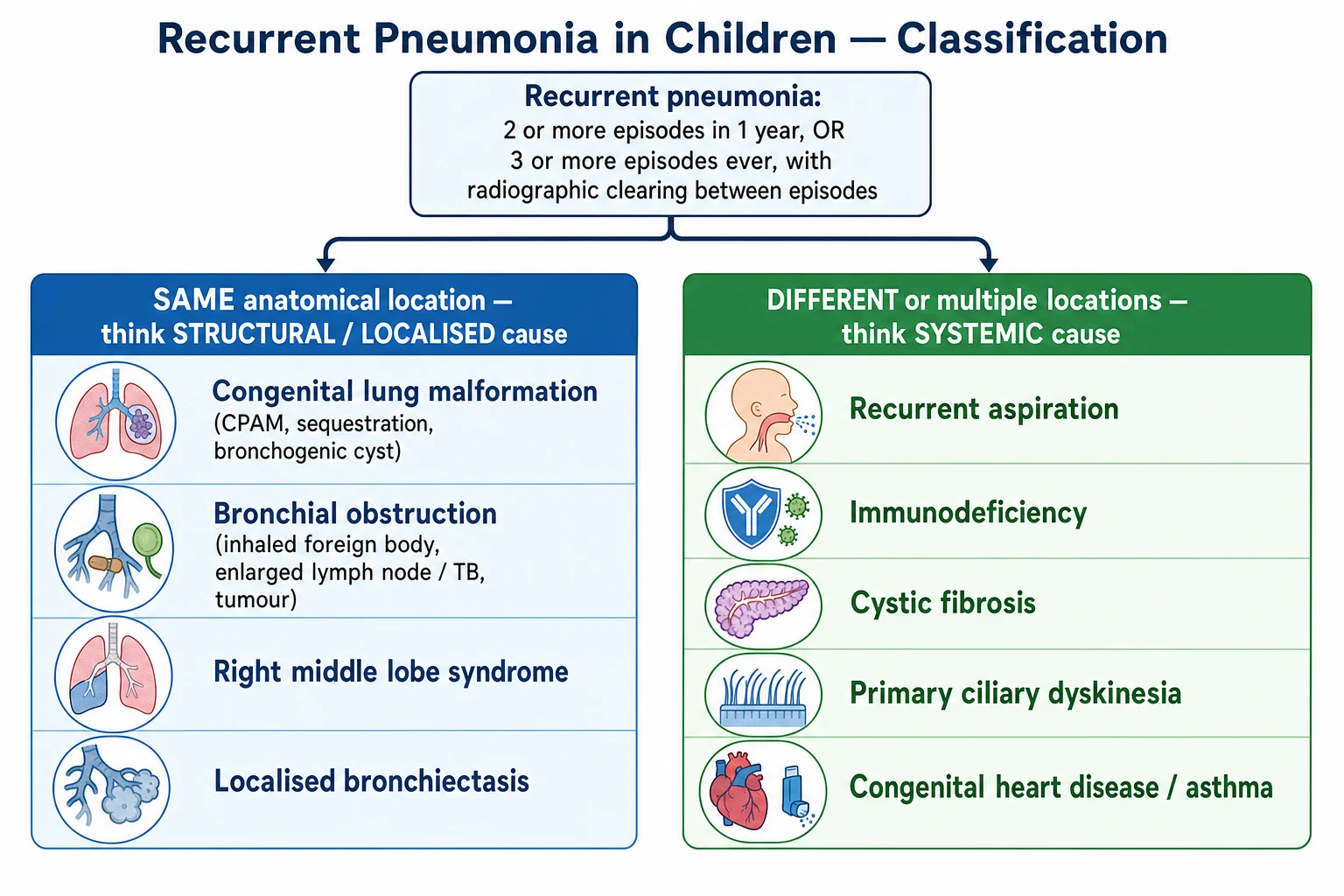
Same-site, or localised, recurrence gathers the structural causes. A congenital lung malformation such as a congenital pulmonary airway malformation, an intralobar sequestration, or a bronchogenic cyst provides a fixed reservoir for infection; a bronchus can be narrowed from within by an inhaled foreign body or from outside by an enlarged lymph node or, classically, tuberculosis; and the right middle lobe, with its long narrow bronchus and poor collateral ventilation, collapses and reinfects so reliably that it carries its own name. Localised bronchiectasis is both a cause and a consequence of this pattern. [1] [6]
Different-site, or multifocal, recurrence gathers the systemic causes. Recurrent aspiration seeds whichever dependent segment the child was lying on; immunodeficiency, whether antibody, cellular, or complement, leaves the whole lung exposed; cystic fibrosis and primary ciliary dyskinesia disable mucociliary clearance everywhere at once; and congenital heart disease, severe asthma, and neuromuscular weakness each predispose the entire respiratory tract. The location of the disease tells you which family to interrogate first. [1] [10]
Epidemiology & Risk Factors
Most children who cough and febrile their way through winter never meet the definition of recurrent pneumonia, but a meaningful minority referred to respiratory clinics do, and in that referred group an underlying cause is the rule rather than the exception. In the defining paediatric series, around nine in ten children with recurrent pneumonia had a demonstrable predisposing condition, which is why the finding should never be shrugged off as constitutional. [1] [2]
The commonest underlying categories are consistent across studies: aspiration and oropharyngeal incoordination, immune deficiency, congenital heart disease, asthma, and structural airway or lung anomalies together account for the great majority of cases. Their relative frequency shifts with the population and the age, with aspiration dominating in children with neurodisability and structural lesions dominating when the disease is confined to one site. Knowing this ranking is what lets you investigate in a rational order. [1] [2]
The risk factors are the conditions that impair any limb of lung defence: neurodevelopmental disability and unsafe swallowing, prematurity and chronic neonatal lung disease, congenital heart disease, and any immune compromise. Environmental tobacco smoke, crowding, and socioeconomic disadvantage amplify every one of these, and in Aboriginal and Torres Strait Islander and other remote-living communities the burden of recurrent infection and its endpoint, bronchiectasis, is strikingly high. [9] [2]
Pathophysiology
Pneumonia recurs when one of the lung's defences is defeated in a way that persists between infections, and the shape of the failure determines the pattern. When the defect is anatomical and fixed, the same segment is repeatedly overwhelmed while the rest of the lung stays well; when the defect is systemic, the whole tract is vulnerable and the disease wanders. The mechanism, in other words, is written in the map of where the infections fall. [3] [1]
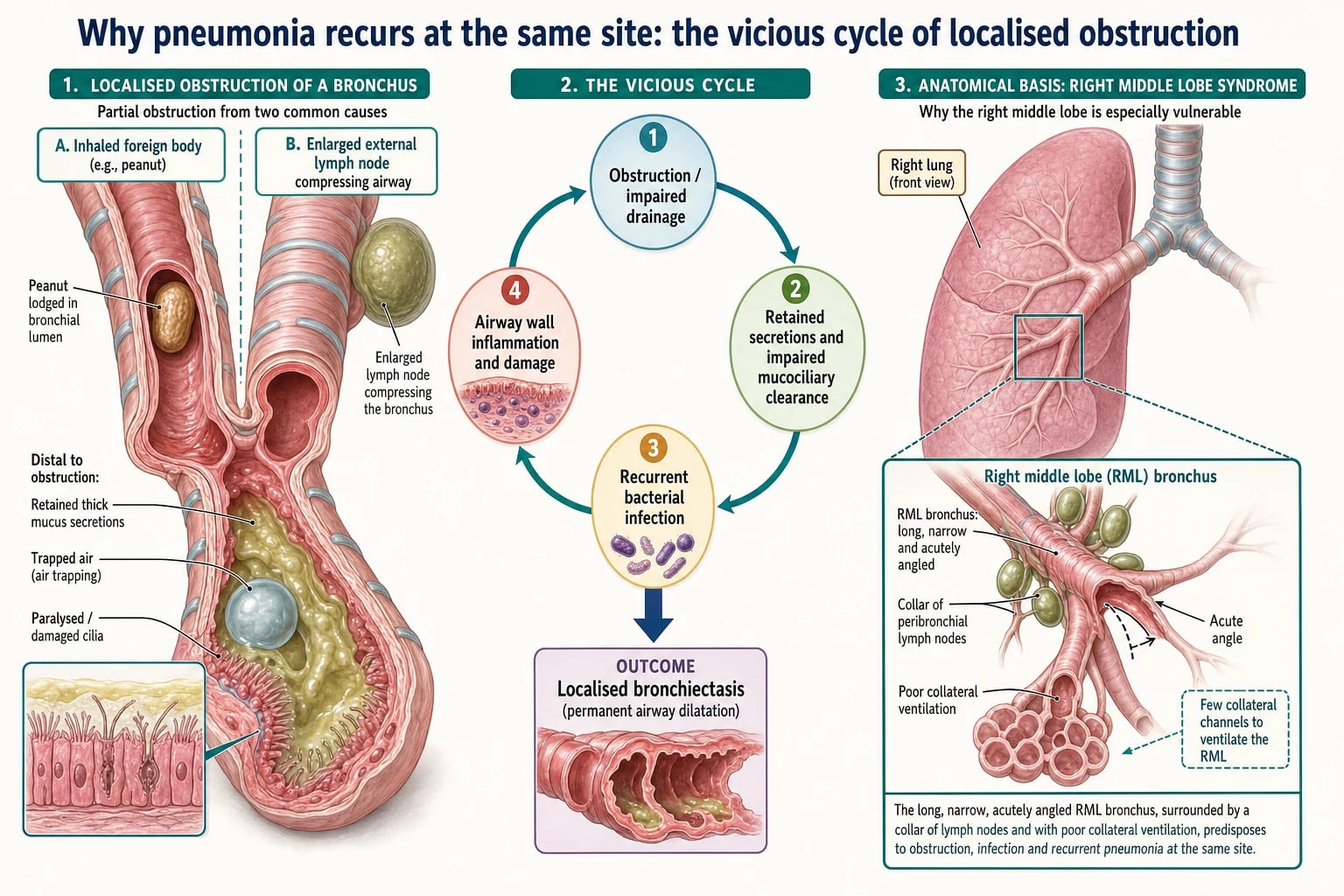
In the localised pattern, the engine is impaired regional drainage. A bronchus narrowed by a foreign body, an external node, or an intrinsic malformation cannot clear its secretions, so mucus pools distal to the obstruction, bacteria colonise the stagnant airway, and infection recurs in exactly the same territory. Each episode inflames and weakens the airway wall, dilating it, which worsens drainage further and locks in a self-perpetuating cycle that ends in localised bronchiectasis. The right middle lobe is the archetype, its slender bronchus and absent collateral ventilation making it uniquely prone to collapse, retention, and reinfection. [6] [7]
In the systemic pattern, the engine is a failure of a defence that operates everywhere. In recurrent aspiration, gastric or oropharyngeal contents repeatedly soil the airway wherever gravity carries them, injuring the mucosa and seeding infection at shifting dependent sites. In immunodeficiency, absent antibody or defective cellular immunity leaves every lobe unprotected. In cystic fibrosis and primary ciliary dyskinesia, dysfunctional mucus and immotile cilia cripple mucociliary clearance across the whole tract, so infection is diffuse and relentless rather than fixed. [10] [12]
The common endpoint, whatever the mechanism, is chronic suppurative lung disease and bronchiectasis. Repeated infection and inflammation destroy the elastic and muscular airway wall, leaving permanently dilated, poorly draining bronchi that pool secretions and perpetuate infection. This continuum is the reason recurrent pneumonia is a diagnosis to chase early: the reversible predisposition you treat today prevents the irreversible airway you cannot repair tomorrow. [9] [1]
Clinical Presentation
The presentation that should trigger the whole work-up is the child brought back for another documented pneumonia, and the history must first establish that these were genuine, radiographically confirmed episodes rather than a string of viral colds relabelled. Ask for the dates, the films, and the treatments, and establish that the child was genuinely well, with a clear chest film, between the episodes. A child who never fully recovers between attacks has persistent, not recurrent, disease and a different differential. [3] [1]
The child with same-site disease often looks well between episodes but carries clues in the pattern: the infections cluster in one region, a fixed area of crackles or reduced breath sounds persists, and there may be a history of a choking episode, a wet cough that lingers, or an incidental opacity on an old film. The child with systemic disease more often shows a background disorder — neurodisability with feeding difficulty, faltering growth, sinusitis and otitis, or infections beyond the chest — that points to the underlying cause. [1] [10]
Certain accompanying features raise the stakes and demand escalation rather than another prescription. A chronic wet or productive cough that never clears between episodes, digital clubbing, chest-wall deformity, faltering growth, or exertional breathlessness all signal that suppurative lung disease is already established and that bronchiectasis may be developing. These are the findings that convert a routine review into an urgent investigation. [9] [2]
Differential Diagnosis
For same-site recurrence, hold a short structural list. A congenital lung malformation, an inhaled foreign body, extrinsic bronchial compression by a lymph node or tuberculosis, an endobronchial lesion, and localised bronchiectasis account for nearly all of it, and right middle lobe syndrome is the pattern that unites collapse and reinfection in that particular lobe. Each of these is diagnosable and most are treatable once the site is imaged and the airway is inspected. [1] [6]
For different-site recurrence, hold a systemic list built around the failing defence. Recurrent aspiration leads in children with neurodisability, immunodeficiency must be actively excluded, cystic fibrosis and primary ciliary dyskinesia explain diffuse suppurative disease, and congenital heart disease, severe asthma, and neuromuscular weakness round out the picture. The accompanying features — feeding difficulty, growth failure, sinopulmonary infection, or a murmur — steer you to the right member of the list. [1] [12]
The most important error is to force a systemic diagnosis onto a same-site problem, or the reverse. A child with three pneumonias all in the right middle lobe does not need an immune work-up first; a child with pneumonias scattered across both lungs does not need a middle-lobe bronchoscopy. Reading the map of the disease before ordering tests is what keeps the differential efficient. [1] [3]
Clinical & Bedside Assessment
The history carries most of the diagnostic weight, and it has three tasks: verify the episodes, define the pattern, and hunt for the underlying cause. Confirm each pneumonia with its film, establish whether the sites were the same or different, and then take a focused system history — feeding and swallowing, choking episodes, cough character between illnesses, growth, stooling, sinus and ear infections, and a family history of cystic fibrosis, immune disease, or consanguinity. Environmental tobacco smoke and the child's community context belong here too. [3] [2]
The examination is a deliberate search for the fingerprints of established lung damage and of the underlying disorder. Plot growth carefully, inspect for digital clubbing and chest-wall deformity, and listen for fixed focal crackles or reduced breath sounds that betray a localised lesion. Look beyond the chest for the neurodevelopmental, cardiac, and nutritional signs of a systemic predisposition, and examine the upper airway for the chronic rhinosinusitis that accompanies ciliary disease. [9] [12]
Reviewing the actual radiographs, rather than the reports, is part of the bedside assessment and often the single most revealing step. Lining up the old films answers the pivotal question of same site versus different sites directly, may reveal a persistent opacity that was never truly cleared, and can show a malformation or a hyperlucent trapped lobe that a report glossed over. Never rely on symptomatic recovery alone to confirm clearing; ask to see the films. [1] [3]
Investigations
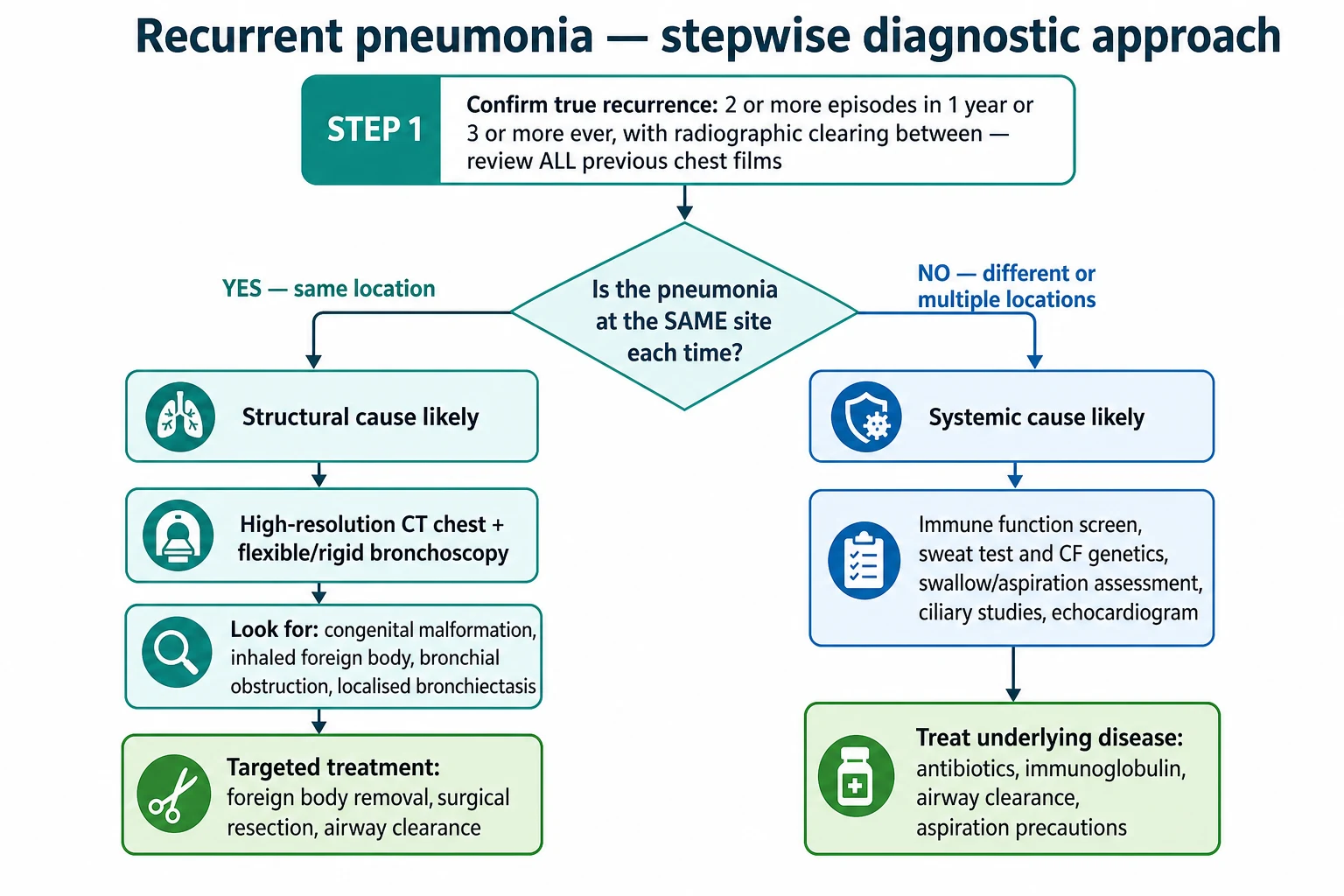
Investigation is staged and driven entirely by the pattern, not ordered as a reflex panel. Every child needs the foundational trio first: a review of all previous chest radiographs to define same versus different sites, a current chest film, and, where suppurative disease is plausible, a sputum or airway culture to define the bacteriology. A first-principles baseline that many series recommend even before subspecialty testing is a full blood count with differential and immunoglobulins, because antibody deficiency is common, treatable, and easily missed. [2] [1]
When the disease is confined to one site, the work-up turns structural. A contrast-enhanced chest CT defines a congenital malformation, sequestration, or localised bronchiectasis and shows extrinsic compression, and flexible or rigid bronchoscopy inspects the airway directly, secures microbiology by lavage, and both diagnoses and removes an inhaled foreign body. Timely bronchoscopy is emphasised in middle lobe syndrome, where clearing the obstruction and treating the infection can restore an otherwise doomed lobe. [6] [8]
When the disease is multifocal, the work-up turns systemic. Screen immune function with a full blood count, immunoglobulin levels, and specific vaccine-response titres; exclude cystic fibrosis with a sweat test and genetics whenever growth falters or the cough is suppurative; assess swallowing with a video fluoroscopic study when aspiration is suspected; and pursue primary ciliary dyskinesia with nasal nitric oxide and specialist ciliary testing when there is chronic rhinosinusitis, neonatal respiratory distress, or situs inversus. Restraint still applies — match the depth of testing to the pattern and the pointers rather than ordering everything at once. [12] [10]
Management — Resuscitation
Recurrent pneumonia is usually a clinic problem, but any individual episode can present acutely and must be stabilised on standard paediatric lines before the elective work-up resumes. A child with respiratory distress, hypoxaemia, or sepsis needs oxygen, fluid resuscitation, and prompt antibiotics guided by paediatric community-acquired pneumonia protocols, with escalation for a large effusion or empyema complicating the acute infection. Treat the sick child in front of you first, then return to the question of why this keeps happening. [4] [5]
A small number of presentations are genuine emergencies that override the diagnostic pathway. A suspected obstructing foreign body with stridor or acute distress, a tension complication of a congenital malformation, or overwhelming infection in an immunodeficient child all demand immediate airway and haemodynamic management and urgent senior and specialist involvement. The principle is unchanged: secure the physiology, then investigate the cause. [8] [5]
Where an inhaled foreign body is the suspected trigger, the urgency is diagnostic as much as therapeutic. A convincing history warrants prompt bronchoscopy even when the child is stable and the film is unremarkable, because delay allows distal infection and permanent airway damage in the affected segment. Escalate early rather than watch and wait. [8] [6]
Management — Definitive & Stepwise
Definitive management treats the specific cause the work-up uncovers rather than the recurrent pneumonia in the abstract. A structural lesion is dealt with mechanically: an inhaled foreign body is removed bronchoscopically, a symptomatic or repeatedly infected congenital malformation is resected, and localised bronchiectasis confined to one lobe may be cured by lobectomy when medical therapy fails. A systemic cause is treated on its own terms — immunoglobulin replacement for antibody deficiency, cystic fibrosis and ciliary disease under specialist multidisciplinary care, and aspiration reduced by feeding modification and, where needed, surgical measures. [11] [10]
Alongside cause-specific treatment, every child needs the acute episodes treated well and the airways kept clear. Acute pneumonia is managed to guideline, with high-dose oral amoxicillin around 90 mg/kg/day as first-line therapy for uncomplicated bacterial community-acquired pneumonia in most children, reserving broader or intravenous cover for severe or complicated disease. Between episodes, airway clearance physiotherapy, treatment of any established bronchiectasis, and prolonged targeted antibiotic courses for suppurative disease protect the lung from further damage. [4] [5]
Stepwise approach to recurrent pneumonia
Confirm true recurrence: two or more episodes in a year or three ever, with radiographic clearing between
Review every previous chest film to decide same site versus different sites
Take baseline tests for all: old films, current film, and a full blood count with immunoglobulins
For same-site disease, obtain a chest CT and proceed to bronchoscopy for anatomy, microbiology, and foreign body
For different-site disease, pursue immune screen, sweat test, swallow assessment, and ciliary studies as pointed to
Treat the specific cause and protect the lung with airway clearance and adequate antibiotic courses
The wet cough that never clears is the signal to stop re-prescribing blindly and escalate. A child whose cough persists between courses, or whose pneumonia keeps returning to the same place despite treatment, has an underlying structural or suppurative cause until proven otherwise and needs CT, bronchoscopy, and a full host work-up rather than another empirical antibiotic. The discipline is to make each step count and to reassess objectively rather than repeat. [9] [6]
RECURRENT — causes to work through
Specific Subtypes & Scenarios
Right middle lobe syndrome is the subtype to master because it recurs in the exam and the clinic alike. The right middle lobe bronchus is long, narrow, and acutely angled, and the lobe has almost no collateral ventilation, so once it collapses — often triggered by asthma, an enlarged node, or mucus plugging — it drains poorly, reinfects, and can become chronically consolidated. It is common in children with poorly controlled asthma, and timely bronchoscopy with vigorous treatment of the airway inflammation can rescue a lobe that would otherwise scar. [7] [6]
The inhaled foreign body is the scenario that punishes complacency. It classically presents as a toddler with a sudden choking episode followed by cough, wheeze, or a fixed focal sign, but the aspiration is frequently unwitnessed and the child may present weeks or months later with recurrent same-site pneumonia mimicking asthma. Because most aspirated material is radiolucent, plain films are often normal or show only indirect signs, and a convincing story mandates bronchoscopy; late diagnosis leads to distal bronchiectasis. [8] [1]
The congenital lung malformation is the subtype that links recurrence to anatomy from the start. A congenital pulmonary airway malformation, a sequestration, or a bronchogenic cyst provides a fixed, poorly draining space that becomes repeatedly infected, usually in the same location. A symptomatic or repeatedly infected lesion is resected, whereas a genuinely asymptomatic antenatally detected malformation may be managed conservatively with surveillance in selected cases, a balance that remains an area of active debate. [11] [1]
Complications & Pitfalls
The gravest complication is the one the whole approach is designed to prevent: bronchiectasis. Recurrent infection that is repeatedly treated as isolated bad luck, without a search for the cause, allows the suppurative cycle to run until the airway wall is permanently destroyed and dilated. This progression to chronic suppurative lung disease is largely preventable, and its prevention is the entire point of taking recurrent pneumonia seriously. [9] [1]
The commonest day-to-day pitfall is the antibiotic merry-go-round: a fourth or fifth course prescribed for the same recurring pneumonia without anyone ever reviewing the old films or asking whether the disease is fixed in one place. This delays the structural diagnosis, exposes the child to ongoing airway damage, and misses the treatable lesion. The corrective discipline is simple and cheap: before the next prescription, line up the radiographs and answer the same-site question. [1] [3]
Prognosis & Disposition
Prognosis depends almost entirely on the underlying cause and on how early it is found. A removed foreign body, a resected malformation, or a treated immunodeficiency can restore a child to normal lung health, and the outlook for these is excellent when the diagnosis is timely. The disposition for same-site structural disease is prompt referral for CT, bronchoscopy, and, where indicated, surgery, with the expectation of a definitive fix. [11] [6]
The children who do badly are those in whom the cause is missed until bronchiectasis is established, because permanent airway dilatation cannot be reversed and commits the child to lifelong airway clearance, recurrent infection, and progressive loss of lung function. This is why the systemic causes — immunodeficiency, cystic fibrosis, ciliary dyskinesia, and aspiration — must be actively excluded rather than assumed absent, and why children with these conditions need long-term multidisciplinary respiratory follow-up. [9] [12]
Disposition is therefore about matching the follow-up to the cause and closing the loop on resolution. Every child treated for recurrent pneumonia should have documented radiographic clearing, a clear plan for the identified cause, and safety-netting for the emergence of clubbing, faltering growth, or a persistent wet cough. Children with suppurative lung disease or a systemic predisposition belong in specialist respiratory care, not serial primary-care antibiotic courses. [9] [2]
Special Populations
Aboriginal and Torres Strait Islander children, and others in disadvantaged and remote communities, carry a far higher burden of recurrent lower respiratory infection, chronic suppurative lung disease, and bronchiectasis, and they are the group most harmed by delayed recognition. In these children a recurring wet cough or repeated pneumonia warrants early, decisive investigation and treatment, with a low threshold for chest CT and for diagnosing bronchiectasis, delivered through culturally safe and accessible services. [9] [2]
Children with neurodevelopmental disability and unsafe swallowing are the archetype of aspiration-driven, different-site recurrence, and their pneumonias track the dependent segments rather than a fixed lesion. Their management centres on a formal swallow and feeding assessment, modification of feed texture and route, control of secretions and reflux, and, in selected children, surgical measures to protect the airway. The recurrent pneumonia here is a marker of a broader airway-protection problem. [10] [1]
Immunocompromised children, whether from primary immunodeficiency or from treatment for malignancy and transplantation, present with recurrent and often opportunistic infection across the lung, and a normal-looking child between episodes can still harbour a serious defect. A different-site pattern, infections beyond the chest, or an unusual organism should prompt immunoglobulin measurement, vaccine-response testing, and specialist immunology input, because early recognition and immunoglobulin replacement change the trajectory. [1] [12]
Evidence, Guidelines & Regional Differences
The evidence base begins with the case series that defined the problem and its causes. Owayed and colleagues showed that the overwhelming majority of children with recurrent pneumonia have an identifiable underlying condition and set out the categories that still frame the work-up, a finding reproduced by Lodha and others across different health systems. These studies established recurrent pneumonia as a symptom to investigate rather than a diagnosis in itself. [1] [2]
Management of the individual episodes rests on the community-acquired pneumonia guidelines, with the British Thoracic Society and the updated Infectious Diseases Society of America and Pediatric Infectious Diseases Society statements anchoring antibiotic choice, severity assessment, and the management of complications such as empyema. These provide the acute framework within which the search for a recurrent cause proceeds. [4] [5]
The controversies cluster at the edges of management rather than the core. The optimal handling of an asymptomatic, antenatally detected congenital lung malformation — early resection versus watchful surveillance — remains genuinely debated, and the threshold for and timing of surgery in localised bronchiectasis is individualised. Across all regions, however, the message converges: verify the recurrence, map the sites, investigate the cause, and treat early to prevent bronchiectasis. [11] [9]
Exam Pearls
The definition and the pivotal question are the highest-yield facts: two or more pneumonias in a year with clearing between defines recurrence, and the opening move is to decide whether the disease is fixed in one place or wandering. Same site means a structural lesion and a CT-and-bronchoscopy pathway; different sites means a systemic defect and a host work-up. Hold these two lines and you have the spine of the topic. [1] [3]
The causes are the second set-piece. Learn the same-site structural list — malformation, foreign body, compression, right middle lobe syndrome, localised bronchiectasis — and the different-site systemic list — aspiration, immunodeficiency, cystic fibrosis, ciliary dyskinesia, heart disease — because reciting them is how you show an examiner you can investigate in a rational order. A single cheap test, the full blood count with immunoglobulins, catches the common and treatable antibody deficiency. [1] [2]
Finally, demonstrate the safety instincts. A fixed focal opacity in a toddler is a foreign body until bronchoscopy says otherwise, radiographic clearing must be confirmed on a film rather than assumed from recovery, and the wet cough that never settles is the harbinger of bronchiectasis. Showing that you chase the cause early to protect the lung is what marks the candidate who understands why recurrent pneumonia matters. [8] [9]
References
- [1]Owayed AF, Campbell DM, Wang EE Underlying causes of recurrent pneumonia in children. Arch Pediatr Adolesc Med, 2000.PMID 10665608
- [2]Lodha R, Puranik M, Natchu UC, et al Recurrent pneumonia in children: clinical profile and underlying causes. Acta Paediatr, 2002.PMID 12463313
- [3]Vaughan D, Katkin JP Chronic and recurrent pneumonias in children. Semin Respir Infect, 2002.PMID 11891521
- [4]Harris M, Clark J, Coote N, et al British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax, 2011.PMID 21903691
- [5]St Peter SD, Ampofo K, Brogan T, et al Clinical Practice Guideline by the Infectious Diseases Society of America and the Pediatric Infectious Diseases Society: 2026 Guideline Update on The Management of Community-Acquired Pneumonia in Infants and Children Older than 3 Months of Age. Clin Infect Dis, 2026.PMID 41839546
- [6]Priftis KN, Mermiri D, Papadopoulou A, et al The role of timely intervention in middle lobe syndrome in children. Chest, 2005.PMID 16236916
- [7]Sekerel BE, Nakipoglu F Middle lobe syndrome in children with asthma: review of 56 cases. J Asthma, 2004.PMID 15281327
- [8]Eren S, Balci AE, Dikici B, et al Foreign body aspiration in children: experience of 1160 cases. Ann Trop Paediatr, 2003.PMID 12648322
- [9]Chang AB, Bell SC, Torzillo PJ, et al Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand Thoracic Society of Australia and New Zealand guidelines. Med J Aust, 2015.PMID 25588439
- [10]Boesch RP, Daines C, Willging JP, et al Advances in the diagnosis and management of chronic pulmonary aspiration in children. Eur Respir J, 2006.PMID 17012631
- [11]Thorburn C, Kattini C, El Hafid M, et al The safety of conservative management of asymptomatic congenital pulmonary airway malformations (CPAMs) in children: A systematic review. J Pediatr Surg, 2026.PMID 41643769
- [12]Lucas JS, Barbato A, Collins SA, et al European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur Respir J, 2017.PMID 27836958