Paeds · respiratory-sleep-and-airway
Community-acquired pneumonia
Also known as Childhood pneumonia · Paediatric CAP · Lower respiratory tract infection with consolidation · Bacterial pneumonia in children · Bronchopneumonia
Fellowship guide to community-acquired pneumonia in children: the febrile, coughing, fast-breathing child with alveolar consolidation acquired outside hospital; the age-dependent shift from viruses and pneumococcus in the young child to Mycoplasma in the school-age child; grading severity by WHO respiratory-rate thresholds, chest indrawing, oxygenation and feeding; the differential from bronchiolitis, viral wheeze, foreign body and tuberculosis; clinical diagnosis with restrained imaging; first-line oral amoxicillin with the SAFER and CAP-IT evidence for short-course standard-dose therapy; oxygen and intravenous care for severe disease; recognising parapneumonic effusion and empyema; and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the three-year-old brought in on the third day of a fever: he is flushed and breathing fast, his lower ribs draw in with each breath, he has a wet cough and has gone off his food, and over the right base you hear fine crackles with quieter breath sounds than on the left. That scene — a febrile child breathing hard with focal chest signs — is community-acquired pneumonia, and recognising it lets you start simple antibiotics and supportive care with confidence rather than reaching first for scans and blood tests. [1] [8]
Community-acquired pneumonia is an acute infection of the lung parenchyma acquired outside hospital, in which the alveoli and small airways fill with inflammatory exudate. The name places the problem in the air sacs themselves rather than in the conducting airways, and that is why the child develops focal consolidation, hypoxaemia and increased work of breathing rather than the diffuse wheeze of bronchiolitis. [8] [3]
Why this matters at fellowship level is that pneumonia is one of the commonest serious infections of childhood and, worldwide, a leading infective cause of death in young children, yet most cases in well-resourced settings are mild and respond to oral antibiotics. The skill being examined is disciplined severity assessment, high-value care that avoids needless imaging and intravenous therapy, and the alertness to spot the child who is genuinely severe or who is developing a complication. [3] [8]
Classification
The most useful way to think about a febrile, fast-breathing child is to answer two questions together: how severe is the pneumonia right now, because severity drives oxygen, admission and route of antibiotics, and what is the likely cause, because age and pattern point to the organism and therefore the drug. [1] [2]
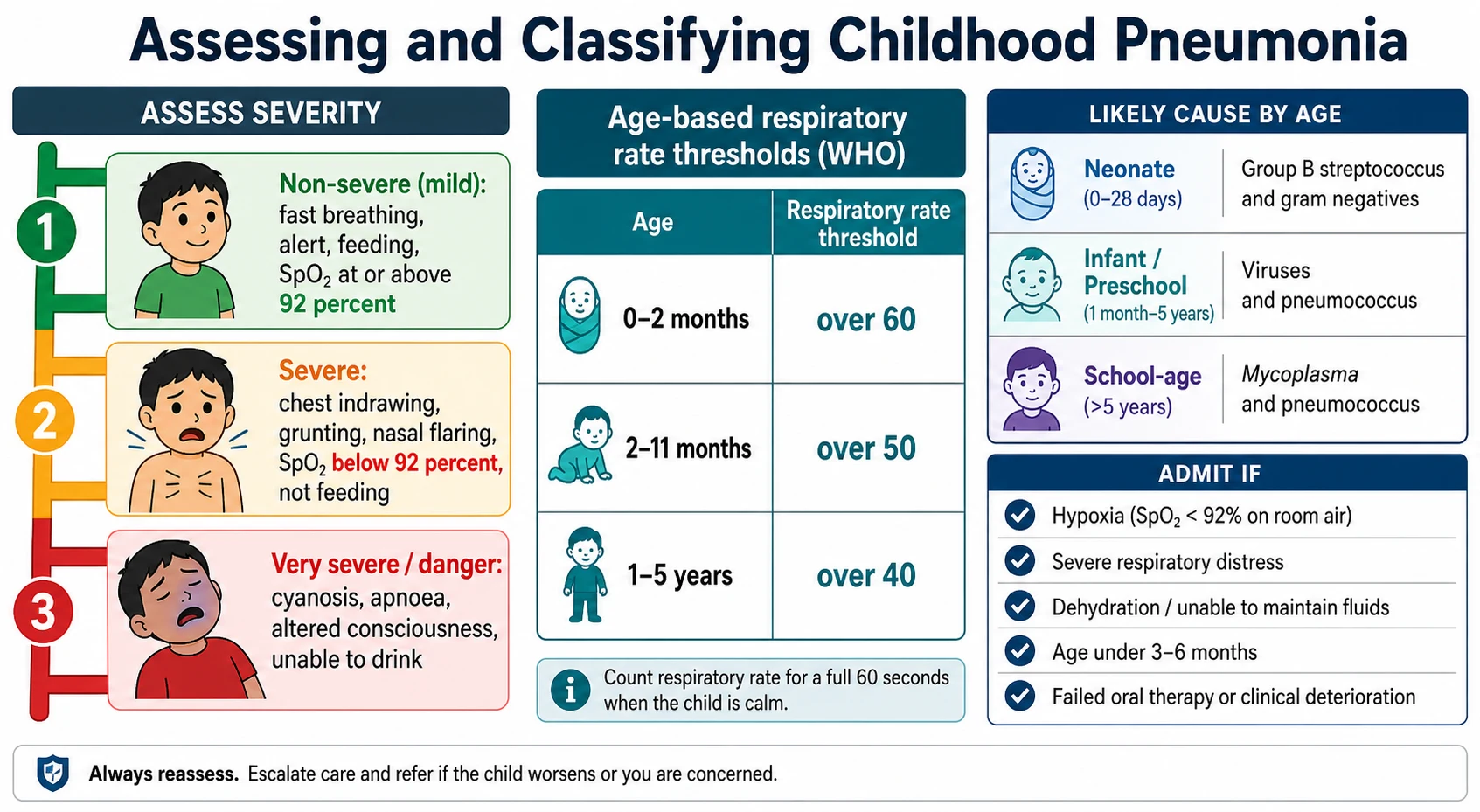
The first axis is severity, and it is largely a bedside judgement. Non-severe pneumonia is the alert child with fast breathing who is feeding and saturating well; severe pneumonia adds chest indrawing, grunting, nasal flaring, saturations below ninety-two percent or an inability to feed; and very severe disease is the child with cyanosis, apnoea, altered consciousness or an inability to drink at all. Fast breathing itself is defined against age using the World Health Organization thresholds. [2] [1]
The second axis is likely cause, which tracks age. Viruses dominate in infants and toddlers, Streptococcus pneumoniae is the leading treatable bacterial cause across the whole age range, and Mycoplasma pneumoniae and other atypical organisms become important in the school-age child and adolescent. In practice bacterial and viral pneumonia overlap and often coexist, so first-line antibiotics still target the pneumococcus. [3] [8]
The numbers that anchor your viva
Epidemiology & Risk Factors
Pneumonia is a disease of the whole of childhood, but it falls hardest on the very young. It is among the commonest reasons for a child to be admitted to hospital with an acute infection, and globally it remains a leading infective cause of death in children under five, with the burden concentrated in low-resource settings where oxygen and antibiotics are less accessible. [3] [8]
Most children who develop pneumonia are previously well, but the risk of acquiring it and of severe disease is concentrated in identifiable groups. Young age and prematurity leave the least respiratory reserve, and chronic conditions such as congenital heart disease, chronic lung disease, neurodisability with aspiration risk, immunodeficiency and sickle-cell disease all raise both the frequency and the severity of infection. [1] [8]
Environmental and social factors matter as much as host factors. Household crowding, exposure to tobacco smoke and indoor cooking pollution, malnutrition, and incomplete immunisation each increase risk, and these often cluster in disadvantaged and remote communities. The strongest modifiable protection is vaccination, and the arrival of pneumococcal and Haemophilus influenzae type b conjugate vaccines has changed the epidemiology by cutting invasive pneumococcal disease and vaccine-serotype pneumonia. [7] [8]
Pathophysiology
The teaching model runs from the pathogen reaching the alveolus to the breathless, hypoxaemic child, and it turns on one idea: the gas-exchanging air sacs fill with fluid and cells, so lung that should hold air now holds exudate. That single change explains the fever, the focal signs and the falling oxygen. [8] [3]
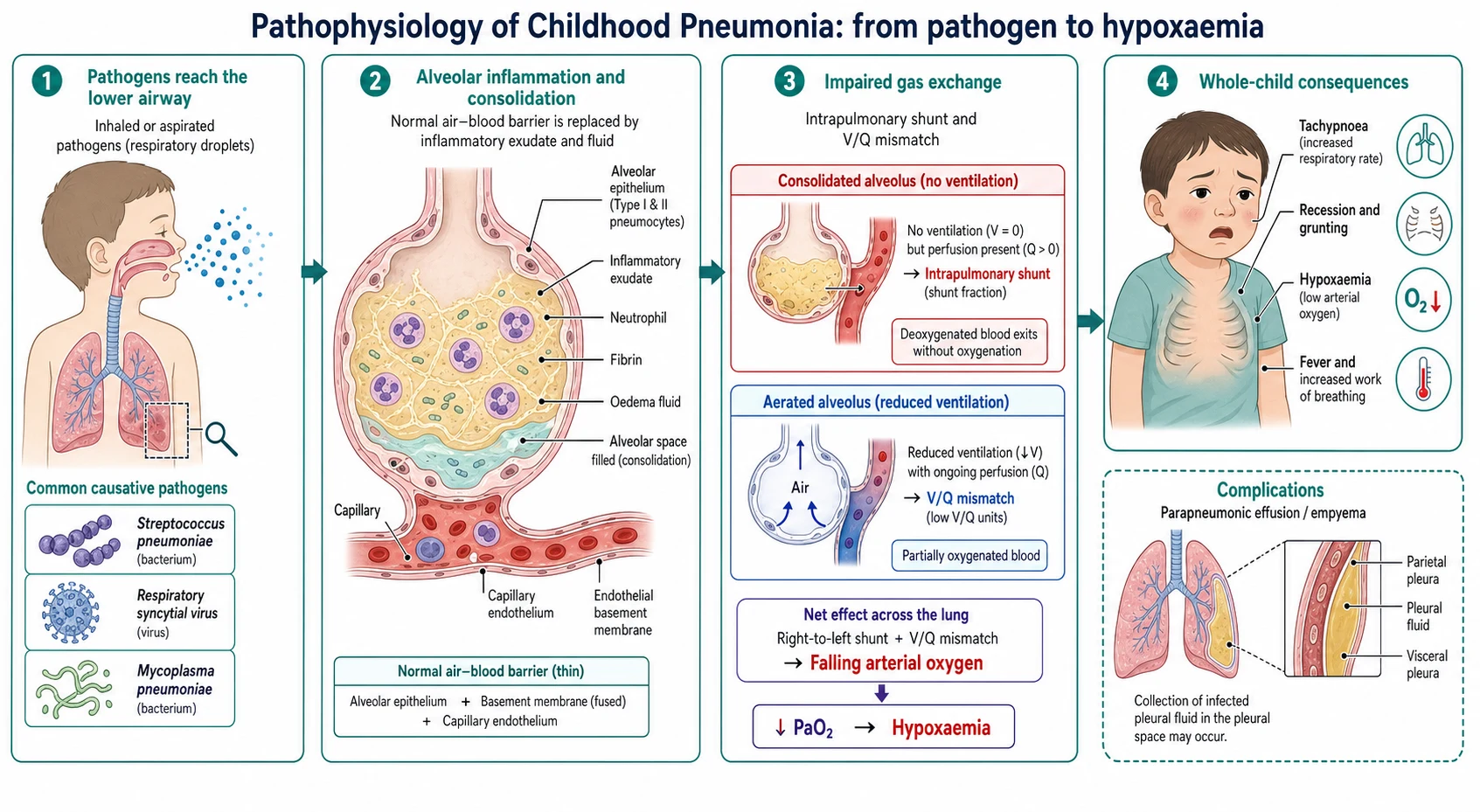
A pathogen reaches the lower airway, usually by inhalation of droplets or micro-aspiration of colonising organisms from the nasopharynx, and infects the distal airways and alveoli. The host response floods the air spaces with neutrophils, oedema fluid and fibrin, and this alveolar exudate is what we call consolidation: on examination it produces dullness to percussion, bronchial breathing and crackles because solid, fluid-filled lung conducts sound differently from aerated lung. [8] [3]
The consequences for gas exchange follow directly. Blood continues to flow past alveoli that are now filled with exudate and no longer ventilated, so deoxygenated blood returns to the systemic circulation as a right-to-left shunt, and this ventilation-perfusion mismatch is the main reason the child becomes hypoxaemic. The child breathes faster and works harder to defend oxygenation, which is why tachypnoea and recession are such reliable clinical signs. [8]
Inflammation does not always stay within the lung. It can spread to the pleural space to produce a parapneumonic effusion that may organise into an empyema, erode into lung tissue to cause necrotising pneumonia or an abscess, or drive a systemic inflammatory response with sepsis, so the same process that consolidates the lung explains the complications you must anticipate. [8] [9]
Clinical Presentation
The classic story is a child with a few days of fever and cough who is now breathing fast and working harder to breathe, often off their food and lethargic. Fever is usually prominent in bacterial pneumonia, the cough may be dry or wet, and the parents frequently notice the fast or laboured breathing before anything else. In the young infant the picture can be less specific, with poor feeding, irritability or grunting rather than an obvious cough. [1] [8]
The most useful bedside skill is to grade severity from observation before you disturb the child, because handling can worsen both distress and the numbers you record. Count the respiratory rate over a full minute, look for chest indrawing, grunting and nasal flaring, note the colour and conscious level, measure the oxygen saturation, and ask specifically about feeding and fluid intake. Focal signs — reduced air entry, crackles, bronchial breathing or dullness over one zone — point to consolidation. [2] [1]
| Severity | Bedside picture | Immediate action |
|---|---|---|
| Non-severe | Fever and cough, fast breathing for age, alert, feeding, saturations at or above 92 percent | Oral amoxicillin at home with safety-net advice |
| Severe | Chest indrawing, grunting or nasal flaring, saturations below 92 percent, or not feeding | Admit, oxygen, intravenous or oral antibiotics, support feeding |
| Very severe | Cyanosis, apnoea, altered consciousness, or unable to drink at all | Resuscitate, oxygen, broad early antibiotics, senior and intensive care review |
| Complicated | Persistent fever, worsening distress, dull quiet hemithorax | Image for effusion or empyema and involve respiratory or surgical teams |
Some presentations sit outside the classic picture and are worth naming. Lower-lobe pneumonia can present with abdominal pain that mimics appendicitis, or with neck stiffness that mimics meningism, so a febrile child with these features and no clear abdominal or neurological cause deserves a careful respiratory assessment. The school-age child with a more gradual onset, prominent dry cough, headache and relatively mild examination findings suggests atypical, often mycoplasmal, infection. [1] [8]
Differential Diagnosis
Sort the differential into three groups: the wheezing lower respiratory illnesses that are not pneumonia (bronchiolitis, viral-induced wheeze and asthma), the mimics that need a different treatment (inhaled foreign body, tuberculosis, pertussis and cardiac failure), and the complications of pneumonia itself (effusion and empyema). The aim is to treat true pneumonia confidently while never anchoring on it when the pattern is wheeze-dominant, sudden or chronic. [8] [2]
Pneumonia
the usual answer
- Fever, cough, fast breathing
- Focal crackles or bronchial breathing
- Increased work of breathing
- Amoxicillin and supportive care
Bronchiolitis / viral wheeze
- Infant with coryza then wheeze
- Diffuse wheeze and crackles
- Widespread, not focal, signs
- Supportive care, not antibiotics
Foreign body / TB / pertussis
- Sudden choke or chronic cough
- Focal persistent or recurrent signs
- Contact or exposure history
- Bronchoscopy, TB workup or macrolide
Cardiac failure
- Murmur, hepatomegaly, poor feeding
- Sweating on feeds, failure to thrive
- Cardiomegaly on imaging
- Cardiology assessment and treatment
Bronchiolitis and viral wheeze are the commonest sources of confusion, because they share fever, cough and fast breathing with pneumonia. The distinction rests on the pattern of signs: bronchiolitis and viral wheeze give diffuse, symmetrical wheeze and crackles in a younger child, whereas bacterial pneumonia tends to give focal signs and a more toxic, higher fever. Reserving antibiotics for a genuine pneumonia rather than a wheezy viral illness is a marker of good stewardship. [8] [6]
The dangerous mimics declare themselves by breaking the pattern. A sudden choking episode with focal persistent signs suggests an inhaled foreign body; a chronic cough with weight loss, night sweats or a contact history suggests tuberculosis; paroxysmal cough with a whoop suggests pertussis; and a murmur with hepatomegaly and sweating on feeds suggests cardiac failure. Recurrent pneumonia at the same site should prompt thought about a structural, aspiration or immune cause. [8] [1]
Clinical & Bedside Assessment
Assessment is largely clinical. Take a focused history — the duration and pattern of fever and cough, feeding and fluid intake, work of breathing noticed at home, immunisation status, comorbidity, and any choking, contact or travel history — and then assess severity while the child is as settled as possible. The single most valuable measurement is an accurate respiratory rate counted over a full minute against the age-specific threshold. [2] [1]
Grade severity by integrating work of breathing, oxygenation and feeding rather than relying on any single number, and use serial assessment to read the trajectory. Respiratory rate, chest indrawing, grunting, air entry, focal signs, colour, conscious level and the ability to feed together tell you far more than one observation, and repeating the assessment after antipyresis and settling reveals whether the child is improving or deteriorating. [2] [1]
Reading the child, not just the thermometer
Very severe
Cyanosis, apnoea, altered consciousness, unable to drink
Deliberately avoid the things that add nothing in a well child with non-severe pneumonia. Routine bloods, a routine chest radiograph and routine microbiology do not change management in the child who is well enough for oral antibiotics at home, and over-investigation adds cost, distress and radiation without benefit. Interpret the oxygen saturation alongside the work of breathing and feeding rather than treating a single reading in isolation. [1] [10]
Investigations
Non-severe pneumonia is a clinical diagnosis and needs no routine tests. The default in the well child treated at home is no bloods, no chest radiograph and no microbiology, because none of them changes the decision to give oral amoxicillin and follow up. A randomised trial of chest radiography in ambulatory children with acute lower respiratory infection found that imaging did not improve clinical outcome, which is the evidence behind this restraint. [10] [1]
A chest radiograph earns its place only when it will change management: in severe or complicated disease, when the diagnosis is genuinely uncertain, when there is a suspected effusion, foreign body or mass, or when pneumonia is recurrent or fails to respond. Radiographs cannot reliably separate bacterial from viral pneumonia, and consolidation may lag behind or persist after the illness, so the film supports rather than replaces clinical judgement. [2] [1]
For the child admitted with severe pneumonia, a blood culture is reasonable despite its low yield, a nasopharyngeal viral PCR can support cohorting and stewardship, and pleural ultrasound is the test of choice to detect and characterise an effusion and to guide drainage. Inflammatory markers such as C-reactive protein and procalcitonin are at best adjuncts, because they overlap substantially between bacterial and viral disease and should never override the clinical picture. [11] [9]
Management — Resuscitation
For the child in severe or very severe pneumonia with respiratory distress or shock, the priority is a structured resuscitation of airway, breathing and circulation with early oxygen and early antibiotics, not a wait for investigations. Give oxygen to correct hypoxaemia, obtain vascular access, treat shock, and summon senior paediatric and intensive care support early. [1] [2]
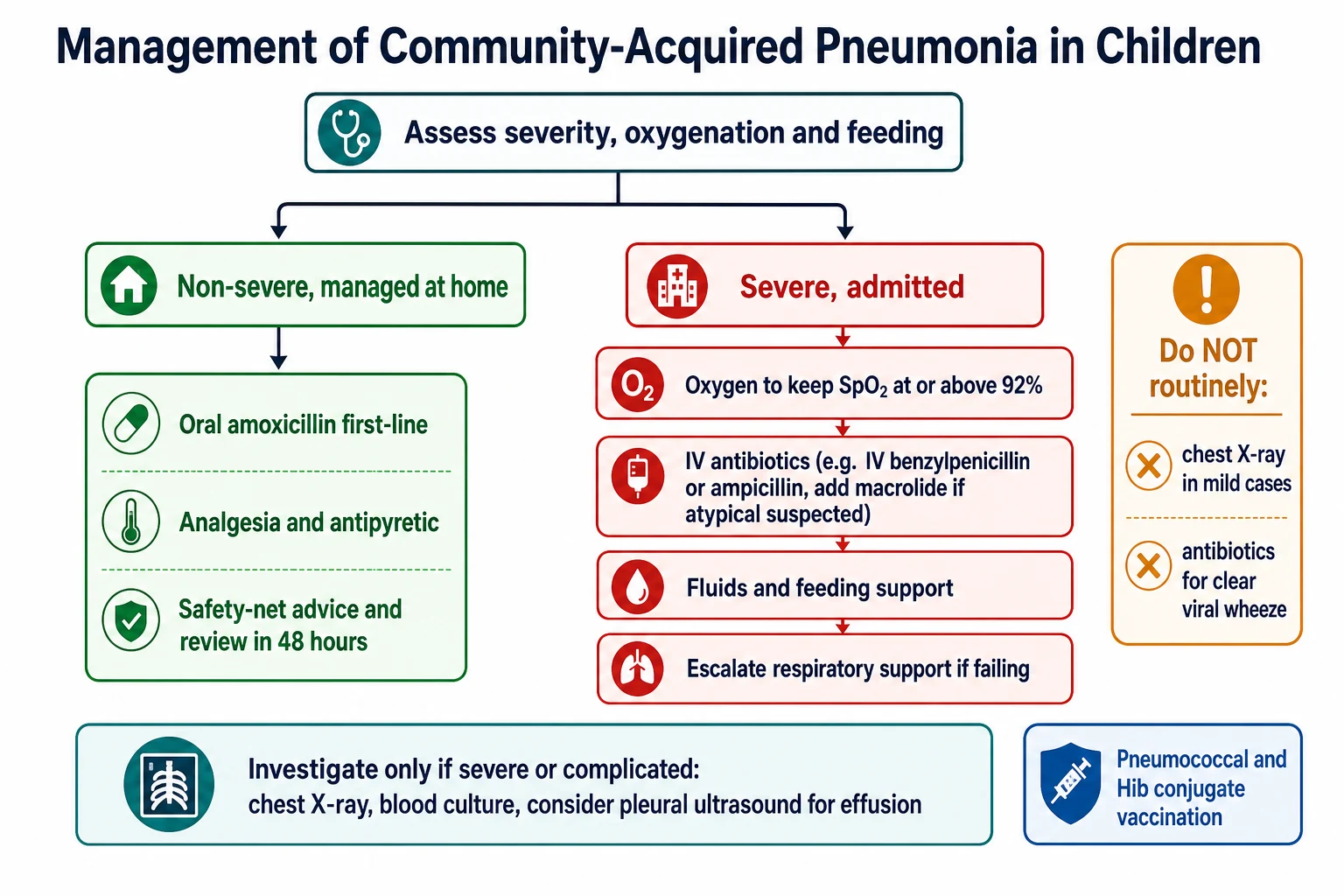
Correct hypoxaemia with supplemental oxygen titrated to a target saturation at or above ninety-two percent, and escalate breathing support to high-flow nasal cannula or continuous positive airway pressure, and ultimately intubation and ventilation, for the child who fails simpler measures or develops respiratory failure. In the child with signs of septic shock, give a carefully titrated fluid bolus and reassess frequently, remembering that over-generous fluid can worsen oxygenation, and start broad intravenous antibiotics without delay. [2] [1]
Empirical antibiotics for severe or complicated pneumonia
Antibiotic choice in severe disease still centres on the pneumococcus, so a narrow-spectrum penicillin such as intravenous benzylpenicillin or ampicillin is first-line, with a macrolide added when atypical infection is likely and broader cover reserved for suspected staphylococcal, necrotising or empyema-complicated disease. Switch from intravenous to oral therapy once the child is improving, afebrile and tolerating fluids, because prolonged intravenous treatment offers no advantage when the child can absorb oral antibiotics. [1] [6]
Management — Definitive & Stepwise
The definitive management of most childhood pneumonia is straightforward and evidence-based: give oral amoxicillin to the child well enough to take it, add oxygen and intravenous therapy only for severe disease, add a macrolide when atypical infection is likely, and drain a significant empyema. Doing this well, and resisting the reflex to image and cannulate every child, is the whole of high-value care. [1] [4]
Oral amoxicillin is first-line for non-severe pneumonia, and oral therapy is as effective as intravenous therapy for children who are well enough to absorb it, as the Cochrane review and pragmatic trials have shown. High-dose amoxicillin gives reliable pneumococcal cover, and the choice of route should turn on how sick and how orally tolerant the child is rather than on a wish to be seen to do more. [6] [1]
First-line oral therapy for non-severe pneumonia
The stepwise pathway
Assess severity by observation: respiratory rate for age, chest indrawing, oxygenation, feeding and risk factors.
Decide disposition: home for non-severe disease, admit for severe or very severe disease or high-risk children.
Start first-line antibiotics: oral amoxicillin at home, or intravenous penicillin for severe disease.
Add a macrolide when atypical (Mycoplasma) infection is likely in the older child.
Support the child: oxygen to keep saturations at or above 92 percent, antipyresis, and fluids or feeding support.
Review and escalate: reassess at 48 hours, image for effusion or empyema if fever persists, and step down intravenous to oral therapy on improvement.
Duration and dose have been simplified by strong recent trials. The SAFER trial showed that a short course of about five days of amoxicillin was non-inferior to a longer course for non-severe pneumonia, and the CAP-IT trial found that lower-dose amoxicillin and shorter duration were non-inferior to higher-dose, longer regimens. Together they support the shortest effective course at a standard dose, which reduces antibiotic exposure without harming outcomes. [4] [5]
PNEUMONIA
Specific Subtypes & Scenarios
Atypical pneumonia is the scenario that catches candidates out in the older child. A school-age child or adolescent with a gradual onset, a prominent dry cough, headache, malaise and relatively unimpressive chest signs suggests Mycoplasma pneumoniae, which does not respond to amoxicillin, so a macrolide is added or substituted when the picture and age fit. Extrapulmonary features such as rash can accompany mycoplasmal infection. [1] [8]
Parapneumonic effusion and empyema should be suspected when fever persists beyond about forty-eight to seventy-two hours of appropriate antibiotics, when respiratory distress worsens, or when a hemithorax becomes dull and quiet. Ultrasound confirms and characterises the fluid, small effusions may resolve with antibiotics alone, and a significant empyema needs drainage, with intrapleural fibrinolytics or thoracoscopic surgery guided by local expertise and the character of the collection. [9] [2]
Pernica 2021 (SAFER) — JAMA Pediatr (PMID 33683325)
Randomised, double-blind, placebo-controlled non-inferiority trial in children with non-severe pneumonia treated as outpatients
Key finding
Clinical cure at about 2 weeks was similar between the short and standard courses, meeting the non-inferiority margin.
Practice change
A short course of about 5 days of amoxicillin is sufficient for non-severe pneumonia, reducing antibiotic exposure without harming outcomes.
Necrotising pneumonia and lung abscess are the more severe parenchymal complications, presenting as a slow-to-resolve, toxic illness sometimes with cavitation on imaging; they need prolonged, often broadened antibiotics and specialist input, and usually recover well with time despite an alarming appearance. Aspiration pneumonia in the child with neurodisability or an unsafe swallow requires cover for oral flora and, importantly, attention to the underlying aspiration risk rather than antibiotics alone. [8] [1]
The remote or telehealth presentation is a common exam scenario: an unwell febrile child a long way from a hospital. The priorities are to gauge severity as best you can, ensure oxygen is available, start appropriate antibiotics early, arrange retrieval for severe disease, and give the family explicit return advice, because distance removes the safety net of easy reassessment. [2] [8]
Complications & Pitfalls
Serious complications of pneumonia are uncommon in well-resourced settings but must be anticipated. Within the chest they include parapneumonic effusion and empyema, necrotising pneumonia, lung abscess and pneumothorax; beyond it they include sepsis, the syndrome of inappropriate antidiuretic hormone secretion with dilutional hyponatraemia, and, in pneumococcal disease, occasional haemolytic-uraemic syndrome or metastatic infection. Persistent or recurring fever is the usual clue that a complication is developing. [8] [9]
The dominant pitfalls are ones of over-treatment and misclassification. The first is over-investigation, above all the routine chest radiograph and blood tests in a well child, which add cost and distress without changing management. The second is over-treatment, giving antibiotics or the intravenous route when a wheezy viral illness or a child well enough for oral therapy does not need them, which fuels resistance and admission. [10] [6]
The third pitfall is misclassification in both directions: mistaking bronchiolitis or viral wheeze for bacterial pneumonia and prescribing needless antibiotics, or dismissing genuine focal pneumonia as a simple viral illness and under-treating it. The fourth is missing a complication or a mimic — failing to image the child with persistent fever for an empyema, or anchoring on pneumonia when a foreign body, tuberculosis or recurrent same-site disease is the real problem. [8] [9]
[2]Prognosis & Disposition
The prognosis of uncomplicated childhood pneumonia is excellent. The great majority of children treated with appropriate antibiotics recover fully within one to two weeks, and even most children with an empyema recover completely with drainage and antibiotics, with good long-term lung function. Mortality in well-resourced settings is low and is concentrated in the very young, the severely unwell and children with significant comorbidity. [8] [9]
Disposition is decided by severity, oxygenation, feeding, age and risk factors rather than by a fixed rule. A child with non-severe pneumonia who is feeding, saturating well and has a family able to give oral antibiotics and return if needed can go home; a child with hypoxia, severe distress, dehydration, an inability to feed, age under about three to six months, a significant comorbidity or a failure of oral therapy should be admitted for oxygen, closer observation and often intravenous treatment. [1] [2]
Safety-net advice is part of the treatment and must be concrete: return urgently if breathing becomes harder or faster, if the child will not drink or has far fewer wet nappies, if they become drowsy, pale or blue, or if the fever persists beyond about forty-eight hours of antibiotics. Arrange review at around forty-eight hours, and reserve follow-up chest imaging for children with a complicated course, lobar collapse or recurrent same-site pneumonia. [2] [9]
Special Populations
The infant under three to six months has the least reserve and the least specific presentation, so keep a low threshold for admission, oxygen and early treatment, and remember that the neonatal and early-infant pathogen mix differs and often warrants broader initial cover and senior involvement. [1] [8]
The child with sickle-cell disease, immunodeficiency or chronic lung disease is at higher risk of severe and invasive disease and of unusual organisms, so these children need earlier senior involvement, a lower threshold for admission and imaging, and attention to their specific vulnerabilities, including acute chest syndrome in sickle-cell disease which overlaps with and is treated alongside pneumonia. [8] [1]
The child with neurodisability and an unsafe swallow is prone to recurrent aspiration pneumonia, so treatment must cover oral flora and, just as importantly, address the underlying aspiration risk through feeding assessment, positioning and secretion management rather than repeated courses of antibiotics alone. [8] [1]
Indigenous, rural, remote and disadvantaged children face the same illness with a thinner safety net and, in some communities, a higher burden of severe and recurrent respiratory disease including bronchiectasis. The equity interventions are reliable access to oxygen and antibiotics, early retrieval for severe disease, high immunisation coverage, and clear, culturally appropriate return advice suited to the family's circumstances. [7] [8]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | First-line and imaging emphasis | Notes |
|---|---|---|---|
| ANZ | RCH Melbourne and Therapeutic Guidelines | Oral amoxicillin; chest X-ray only if severe or complicated | Restrained imaging; admit by severity and oxygenation |
| UK | BTS 2011 and NICE NG138 | Amoxicillin first-line; no routine chest X-ray | Macrolide added for suspected atypical or non-response |
| North America | IDSA/PIDS 2011 | High-dose amoxicillin; ampicillin or penicillin if admitted | Emphasises pneumococcal cover and stewardship |
| Low-resource | WHO case management | Amoxicillin by respiratory rate and indrawing | Access to oxygen and antibiotics is the limiting factor |
The evidence backbone you should be able to name starts with the IDSA/PIDS and BTS guidelines, which established clinical diagnosis, restrained imaging and amoxicillin first-line, and the Cochrane review (Lodha), which confirmed that oral antibiotics are as effective as intravenous therapy for children well enough to take them. The EPIC study (Jain) defined the modern aetiology of hospitalised childhood pneumonia, showing viruses in the majority and pneumococcus as the leading bacterial cause. [1] [6] [3]
For dose and duration, the SAFER trial (Pernica) and the CAP-IT trial (Bielicki) together showed that short courses and standard, even lower, doses of amoxicillin are non-inferior for non-severe pneumonia, driving the shift to shorter stewardship-friendly regimens. Prevention rests on conjugate vaccines: the fall in pneumonia hospitalisations after pneumococcal vaccination (Griffin) is one of the clearest demonstrations of vaccine impact on childhood lower respiratory disease. [4] [5] [7]
The live areas of nuance are the exact first-line dose of amoxicillin between guidelines, the role and limits of biomarkers such as C-reactive protein and procalcitonin in guiding antibiotics, and the best drainage strategy for empyema between fibrinolysis and thoracoscopic surgery — a good example of active care refining an established framework. [11] [9]
Exam Pearls
And when you teach community-acquired pneumonia, teach it as the model of high-value paediatric care — count the breaths, treat most children with oral amoxicillin, give oxygen when it is needed and image only when it will change what you do — while never letting the routine of a common illness dull your alertness to the severe child or the child developing a complication. [8] [2]
References
- [1]Bradley JS, Byington CL, Shah SS, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis, 2011.PMID 21880587
- [2]Harris M, Clark J, Coote N, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax, 2011.PMID 21903691
- [3]Jain S, Williams DJ, Arnold SR, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med, 2015.PMID 25714161
- [4]Pernica JM, Harman S, Kam AJ, et al. Short-Course Antimicrobial Therapy for Pediatric Community-Acquired Pneumonia: The SAFER Randomized Clinical Trial. JAMA Pediatr, 2021.PMID 33683325
- [5]Bielicki JA, Stöhr W, Barratt S, et al. Effect of Amoxicillin Dose and Treatment Duration on the Need for Antibiotic Re-treatment in Children With Community-Acquired Pneumonia: The CAP-IT Randomized Clinical Trial. JAMA, 2021.PMID 34726708
- [6]Lodha R, Kabra SK, Pandey RM. Antibiotics for community-acquired pneumonia in children. Cochrane Database Syst Rev, 2013.PMID 23733365
- [7]Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med, 2013.PMID 23841730
- [8]le Roux DM, Zar HJ. Community-acquired pneumonia in children - a changing spectrum of disease. Pediatr Radiol, 2017.PMID 29043417
- [9]Long AM, Smith-Williams J, Mayell S, et al. 'Less may be best'-Pediatric parapneumonic effusion and empyema management: Lessons from a UK center. J Pediatr Surg, 2016.PMID 26382287
- [10]Swingler GH, Hussey GD, Zwarenstein M. Randomised controlled trial of clinical outcome after chest radiograph in ambulatory acute lower-respiratory infection in children. Lancet, 1998.PMID 9482294
- [11]Omaggio L, Franzetti L, Caiazzo R, et al. Utility of C-reactive protein and procalcitonin in community-acquired pneumonia in children: a narrative review. Curr Med Res Opin, 2024.PMID 39494704