EM · Paediatric trauma
Paediatric trauma — the modified approach
Also known as Paediatric trauma · Child trauma · Injured child
Paediatric trauma — the different injury patterns (the larger head, the compliant chest, the less-protected abdominal organs), the physiological differences (the smaller blood volume, the faster desaturation, the higher surface-area-to-mass), the weight-based drug dosing (the Broselow tape, the formula weight equals age plus 4 times 2), the paediatric assessment triangle, the fluid bolus of 10 to 20 mL per kilogram, and the non-accidental injury consideration. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Paediatric trauma is the leading cause of death in children over one year of age, and the injured child differs from the injured adult in every way that matters — the injury pattern, the physiology, the drug doses, the psychological needs, and the legal framework. The Fellowship candidate must know the anatomical and the physiological differences, the weight-based drug dosing, the paediatric assessment, and the non-accidental-injury consideration, because the application of the adult approach to a child without these modifications is a dangerous and potentially fatal error.[1][2]

The anatomical and physiological differences
The child is not a small adult.[1] The anatomical differences drive the injury pattern, and the physiological differences drive the resuscitation. The head is proportionally larger (and the brain more vulnerable — the head injury is the leading cause of death in paediatric trauma), the neck muscles are weaker (the cervical-spine injury is common, and the SCIWORA — the spinal-cord injury without a radiological abnormality — is a paediatric entity). The chest wall is compliant (the ribs bend rather than break, so a significant internal injury may exist with minimal external signs — the rib fractures in a young child suggest a severe force or a non-accidental injury). The abdominal organs are less protected (the liver and the spleen are anterior and exposed; the bladder is intra-abdominal until the age of about 4). The blood volume is smaller (about 70 to 80 mL per kilogram, so a 10 kg child has only 700 to 800 mL of blood — a 150 mL loss is a 20 per cent loss). The functional residual capacity is lower and the oxygen consumption is higher, so the child desaturates faster (the pre-oxygenation is critical). The surface-area-to-mass ratio is higher, so the child loses heat faster (the hypothermia accelerates in the exposed trauma patient). The temperature regulation is immature, and the cold child develops the coagulopathy, the arrhythmia and the slowed drug metabolism of the lethal triad.
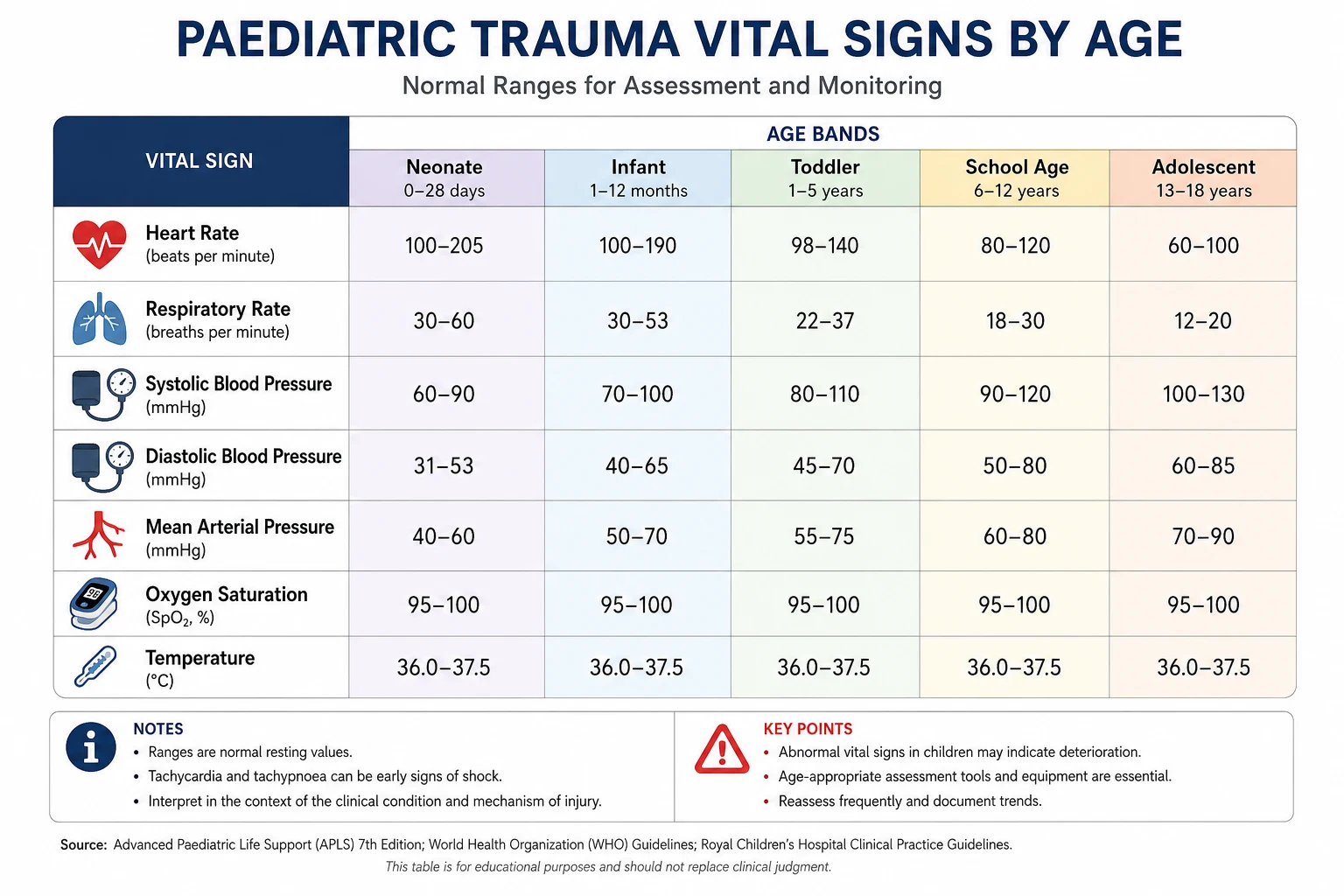
The vital signs by age — the range that flags the sick child
The vital signs in the child are age-specific, and the application of the adult normal to a child conceals the shock. The tachycardia is the early sign; the hypotension is the late (and pre-terminal) sign[2] — the child's cardiac output is heart-rate dependent, and the stroke volume is preserved until late by the vigorous vasoconstriction and the tachycardia. A drop in the blood pressure in an injured child is the sign of a 25 to 30 per cent loss of the circulating volume and the imminent cardiovascular collapse.
The age-specific paediatric vital signs (the ATLS/APLS ranges)
The body-surface-area-to-mass ratio — why the child cools fast
The surface-area-to-mass ratio is roughly three times that of the adult in the infant, and falls as the child grows — a 3 kg neonate has a surface area of about 0.2 m² (a ratio of about 0.067 m² per kilogram) compared with an adult's 0.025 m² per kilogram. The clinical consequence is the rapid heat loss in the exposed child: a fully exposed neonate can drop 1 °C in 10 minutes, and the hypothermia drives the coagulopathy (the impaired enzyme kinetics of the clotting cascade), the acidosis (the impaired catecholamine response) and the arrhythmia (the bradycardia of the cold myocardium) — the lethal triad of the trauma. Active warming is a resuscitative intervention, not a comfort measure: the forced-air warmer, the warmed fluids (the crystalloid stored at 39 °C, the blood passed through a blood warmer), the ambient temperature raised, the head covered, and the child covered between the examination steps. [1]
The compliant chest wall — the internal injury without the rib fracture
The costal cartilage is uncalcified and the ribs are elastic in the young child — they bend rather than break, so a significant deceleration force is transmitted to the underlying lung and the heart without leaving a rib fracture. A pulmonary contusion, a cardiac contusion, a pneumothorax or a haemothorax may exist with an entirely normal chest wall, and the absence of the rib fracture is NOT reassuring. The presence of a rib fracture in a child under two years, in the absence of a high-energy mechanism, is the sign of a severe force or a non-accidental injury — and warrants the safeguarding consideration. The lung itself is also more vulnerable: the alveoli are less developed and the type-II pneumocytes fewer, so the contused lung in the child deteriorates faster into the acute respiratory distress syndrome than in the adult, and the first 24 hours after the chest injury are the high-risk window for the respiratory failure. [1]
The blood volume — the smaller reservoir and the larger proportional loss
The blood volume of the child is 70 to 80 mL per kilogram[1] (the neonate closer to 90 mL/kg, the older child closer to 70 mL/kg). The arithmetic is unforgiving: a 10 kg child has a 750 mL circulating volume, and a 150 mL loss (a single adult unit of blood) is a 20 per cent loss — the threshold of the class III shock. A 3 kg infant has only 240 mL of blood, and a 75 mL loss is a 30 per cent loss — the class IV shock. The clinical implication is that the external blood loss is rarely visible in the quantities that matter — a scalp laceration can bleed 100 mL into the drapes, a femoral fracture can sequester a full blood volume into the thigh, and the intra-abdominal haemorrhage is invisible until the perfusion fails. The volume assessment is the perfusion assessment, not the visible-loss assessment.
[1]Differential diagnosis — the paediatric injury pattern
The paediatric injury pattern differs from the adult, and the differential includes the non-accidental injury. [1]
Blunt trauma (commonest)
- Falls (the commonest mechanism), motor-vehicle, bicycle, pedestrian
- Head injury is the leading cause of death
- Internal organ injury with minimal external sign
- ABCDE with the weight-based doses
Head injury
- Larger head-to-body ratio; weak neck muscles
- Diffuse brain injury (DAI) common; focal less so
- SCIWORA (the spinal-cord injury without a radiological abnormality)
- The paediatric GCS (modified verbal for the young child)
Abdominal injury
- Liver and spleen are anterior and less protected
- Handlebar injuries (the small-bowel perforation, the pancreatic injury)
- Seat-belt injuries (the Chance fracture, the mesenteric tear)
- FAST may be less sensitive in the child (smaller volume)
Non-accidental injury
- Inconsistent history; delayed presentation; changing stories
- Pattern injuries (the retinal haemorrhage, the posterior rib fracture, the metaphyseal corner fracture)
- Multiple injuries at different healing stages
- A mandatory safeguarding referral and the documentation
The lap-belt injury complex — the Chance fracture and its companions
The lap-belt syndrome is the constellation of injuries caused by the poorly positioned (or the improperly worn) lap seatbelt that rides up onto the abdomen in a sudden deceleration. The mechanism is the hyperflexion of the torso over the belt, with the spine pivoting on the belt as the fulcrum. The classic tetrad — the Chance fracture (the bony or the ligamentous flexion-distraction fracture of the lumbar spine, classically L1 to L3), the intestinal injury (the small-bowel perforation or the mesenteric tear, often a delayed presentation 24 to 72 hours later), the pancreatic injury (the crush of the pancreas against the vertebral column), and the abdominal-wall contusion (the seat-belt sign) — must be sought together, because the presence of one mandates the search for the others. A child with the seat-belt sign (the linear bruise across the lower abdomen) has a 30 per cent risk of an intra-abdominal injury and warrants the CT and the admission for the serial examination, because the hollow-viscus injury may not declare itself on the initial imaging. [1]
[1]The lap-belt injury complex — the ED workup
Recognise the mechanism
The improperly worn or the poorly fitted lap belt (no shoulder restraint, or the shoulder belt slipped under the arm) in a motor-vehicle crash. The seat-belt sign across the lower abdomen is the trigger; the high-speed mechanism with the lap-only belt in a child is the historical red flag.
Examine the spine
The palpable step and the tenderness in the thoracolumbar junction; the neurological deficit (the rare but devastating cord injury from the retropulsed bone or the epidural haematoma). The lateral thoracolumbar X-ray or the CT shows the horizontal split fracture through the pedicles, the posterior elements and the vertebral body — the Chance fracture.
Examine the abdomen
The tenderness, the guarding, the rigidity; the seat-belt sign; the rectal bleeding (the mesenteric or the bowel injury). Send the serum amylase and lipase (the pancreatic injury), the lactate (the ischaemia), and the serial abdominal examinations.
Image and consult
The CT abdomen with the intravenous contrast and the pancreatic protocol; the oral contrast if the bowel injury is suspected (the contrast extravasation, the pneumoperitoneum, the mesenteric stranding). The trauma surgery and the paediatric surgery are involved early — the bowel and the pancreatic injuries are frequently operative.
Admit for the serial examination
A child with the seat-belt sign and an initial negative scan is admitted for 24 to 48 hours of the serial abdominal examinations and the bloods (the rising white cell count, the rising lactate, the rising inflammatory markers). A delayed bowel perforation at 48 to 72 hours is the well-described trap — the peritonitis may be subtle in the child who is in pain from the other injuries.
The paediatric Glasgow Coma Scale — the verbal modification
The paediatric GCS modifies the verbal response for the pre-verbal child (under five years, or the developmentally delayed). The eye and the motor components are largely unchanged (the eye opening to the stimulus, the motor response to the command or the pain), but the verbal component uses the age-appropriate behaviours. The modified GCS retains the 15-point total and the same thresholds (the 13 to 15 as the minor, the 9 to 12 as the moderate, the 8 or less as the severe — intubate). [1]
Best verbal (the >5 yr and the adult)
- 5 — Oriented
- 4 — Confused
- 3 — Inappropriate words
- 2 — Incomprehensible sounds
- 1 — None
Best verbal (the <5 yr, the modified)
- 5 — Appropriate words, smiles, fixes and follows, appropriate cry
- 4 — Persistent cry or the inconsolable but appropriate sounds
- 3 — Persistent screams or grunts
- 2 — Inconsolable, agitated, inappropriate cry
- 1 — None
Best motor (the modified for the infant)
- 6 — Spontaneous or to command
- 5 — Localises pain or withdraws to touch
- 4 — Flexion-withdrawal to pain
- 3 — Flexion (decorticate) to pain
- 2 — Extension (decerebrate) to pain
- 1 — None
The paediatric assessment triangle and the weight estimation
The paediatric assessment triangle (the PAT) is the rapid bedside assessment that identifies the sick child before the vital signs are taken[2]: the appearance (the tone, the interactiveness, the consolability, the look, the speech — the TICLS), the work of breathing (the respiratory distress, the stridor, the wheeze, the accessory-muscle use, the abnormal airway sounds), and the circulation to the skin (the pallor, the mottling, the cyanosis). A child with an abnormal PAT is sick and needs the immediate assessment. The weight is estimated with the Broselow tape (a length-based tape that correlates the length with the weight and the drug doses) or the formula weight (kg) = (age + 4) × 2 for the child aged 1 to 10 years. Every drug dose is weight-based, and the wrong weight is the commonest source of the paediatric drug error.
The modified primary survey
The ABCDE is performed with the paediatric modifications. [1]
A — Airway. The child's airway is smaller and more easily obstructed (the tongue is proportionally larger, the secretions block the narrow airway). The airway adjuncts (the oropharyngeal sized by the corner of the mouth to the angle of the jaw; the nasopharyngeal) are used. The cuffed endotracheal tube is now standard in children (over 28 days, over 3 kg) — the uncuffed tube is no longer the default. The tube size: the age divided by 4 plus 4 (the internal diameter in mm). The intra-osseous (IO) needle is placed early — after two failed IV attempts or 90 seconds — in the proximal tibia, the distal femur or the proximal humerus. [1]
B — Breathing. The child desaturates faster (the lower functional residual capacity, the higher oxygen consumption) — pre-oxygenate for 3 minutes. The respiratory rate is age-specific (higher in the younger child). The tension pneumothorax is decompressed at the 2nd intercostal space mid-clavicular or the 4th/5th anterior axillary (the same adult landmarks, but with a paediatric cannula or a needle appropriate for the chest-wall thickness). [1]
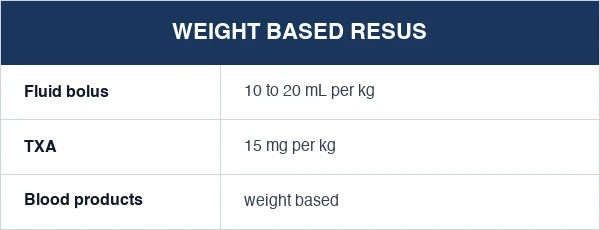
C — Circulation. The fluid bolus is 10 to 20 mL per kilogram of a balanced crystalloid (not the 250 mL adult aliquot), reassessed after each bolus. The blood products are given for the haemorrhagic shock (the 10 mL per kilogram of the packed red cells). The intra-osseous access is the rescue when the peripheral IVs are difficult (the child's veins are small and they collapse in the shock). The tranexamic acid 15 mg per kilogram intravenously (up to 1 g) is given for the haemorrhagic shock. [1]
D — Disability. The paediatric GCS (the modified verbal response for the pre-verbal child) is used. The bedside glucose is checked (the hypoglycaemia is common in the injured child from the depleted glycogen). The bradycardia in a sick child is a pre-terminal sign — it reflects the hypoxia, and the response is the ventilation and the oxygenation, not the cardiac drugs. [1]
E — Exposure. The full exposure for the examination, with the warmth preservation (the child loses heat fast). The Broselow tape provides the drug doses and the equipment sizes for the measured length. [1]
Immediate management — the weight-based drug doses
[1]The fluid resuscitation in the injured child — the warmed bolus and the early blood
The paediatric circulation is heart-rate dependent and the vasoconstriction is vigorous; the shock is recognised on the tachycardia, the capillary refill (above 2 seconds), the skin mottling and the altered mentation — NOT on the blood pressure, which is preserved until 25 to 30 per cent of the volume is lost. The fluid resuscitation is therefore driven by the clinical signs, not the numbers, and proceeds in the stepped aliquots of the paediatric volume. [1]
The stepped fluid resuscitation in the injured child
The first bolus — 20 mL/kg warmed balanced crystalloid
The Hartmann (or the Plasma-Lyte) at 20 mL/kg, warmed to 39 °C, over 10 to 20 minutes. Reassess the perfusion, the heart rate, the capillary refill and the mentation after each bolus — the clinical response, not a target blood pressure. A second bolus is given if the shock persists.
The second bolus — a further 20 mL/kg, but reassess for the bleeding
If a second 20 mL/kg is required, the suspicion of the uncontrolled haemorrhage is high. Identify and control the source (the chest tube for the haemothorax, the pelvic binder for the pelvic fracture, the direct pressure on the external bleed, the splintage of the long-bone fracture). The further crystalloid dilutes the clotting factors and worsens the acidosis — the balanced resuscitation takes over.
The blood — 10 mL/kg of the packed red cells, early
The blood products are given early in the suspected haemorrhagic shock — the 10 mL/kg of the packed red cells, with the fresh-frozen plasma (10 mL/kg) and the platelets if a massive transfusion is anticipated. The balanced ratio (1:1:1 of the PRBC:FFP:platelets) is extrapolated from the adult PROPPR evidence. The tranexamic acid 15 mg/kg (max 1 g) within 3 hours of the injury.
Permissive hypotension in the child — a cautious approach
The adult evidence for the permissive hypotension (target SBP 80 to 90) is NOT directly extrapolated to the child — the hypotension is a late and pre-terminal sign in the child, and a deliberate hypotension risks the secondary brain injury in the head-injured patient. The aim is the normotension for the age (SBP at least 70 + 2×age) in the child with the traumatic brain injury, and the cautious permissive hypotension (a SBP sufficient to maintain the consciousness and the perfusion) in the bleeding child without the head injury.
The stop point and the surgical escalation
A poor or a transient response to two crystalloid boluses (40 mL/kg) is the indication for the blood products, the surgical or the interventional-radiology control of the bleeding, and the activation of the massive transfusion protocol. The further crystalloid beyond 40 mL/kg without the blood is the sign of a failure to identify the source — escalate, do not infuse.
The non-accidental injury — the mandatory consideration
The non-accidental injury (the NAI) is considered in every injured child with an inconsistent history, a delayed presentation, a changing story, or a pattern of injuries inconsistent with the developmental stage. The red flags include: the retinal haemorrhages (the shaken-impact syndrome), the posterior rib fractures (the squeezing), the metaphyseal corner fractures (the pulling), the long-bone fractures in a non-ambulant child, the multiple injuries at different healing stages, and the burns in a glove-and-stocking or a dipping pattern. The NAI suspicion triggers a mandatory safeguarding referral, the careful documentation (the verbatim history, the body map, the photographs), and the involvement of the paediatric team and the social services. The child protection is the responsibility of the emergency physician, not an optional extra. [1]
The NAI pattern injuries — the injury that tells the story
The NAI pattern injuries are the injuries whose shape, site or mechanism reveals a non-accidental cause. They are the strongest single piece of evidence at the bedside, because they cannot be explained by a fall or a play accident. The skeletal survey (the 20-view radiographic series at the admission and the repeat at 11 to 14 days for the callus) is the standard imaging in the suspected NAI in any child under two years; the CT head and the ophthalmology review for the retinal examination are the standard in the suspected shaking. [1]
Skeletal
- The posterior rib fractures at the costovertebral junction (the squeezing — the leverage on the rib from the adult grip); the callus on the healing fracture is seen at 2 weeks
- The metaphyseal corner or the bucket-handle fracture (the pulling or the twisting of the limb — the pathognomonic lesion of the NAI)
- The long-bone fracture in a non-ambulant child (a femoral or a humeral fracture in a child not yet walking is the red flag)
- The multiple fractures at different healing stages (the repeated injury over time)
- The skull fracture in a child under one year (the most common fatal NAI fracture); the complex, the wide or the depressed fracture is the higher-risk pattern
Skin
- The bruise in a non-mobile infant (a bruise before the cruising age is unusual and warrants the workup)
- The patterned bruise (the hand, the belt, the ligature mark — the imprint of the implement)
- The bruise behind the ear, the neck, the torso or the buttocks (the TEN-4 FACES rule)
- The burn in a glove-and-stocking or a doughnut pattern (the immersion — the spared flexure creases where the child held still)
- The human-bite mark (measured and photographed for the dental match)
Head and eye
- The retinal haemorrhages (the shaken-impact syndrome — multilayered, too numerous to count, extending to the periphery; the few single haemorrhages of the birth or the CPR are different)
- The subdural haematoma (the bridging-vein tear from the shaking — often multiple and of different ages)
- The diffuse axonal injury without the impact (the acceleration-deceleration of the shaking)
- The skull fracture with the overlying swelling disproportionate to the history
- The torn frenulum or the lip laceration in a non-mobile infant (the forced feeding)
Visceral and occult
- The duodenal haematoma (the deep palpation of the abdomen — the classic NAI injury of the second part of the duodenum, presenting with the bilious vomiting)
- The pancreatic injury from the direct blow
- The liver or the splenic laceration from the kick or the punch
- The occult fracture on the skeletal survey (the 20-view radiographic series at the admission and repeated at 2 weeks for the callus)
The imaging in paediatric trauma
The FAST is performed as the standard but may be less sensitive in the smaller child (the smaller volume of the free fluid). The CT is performed for the clinical indication (the head CT for the altered conscious level or the focal neurology; the chest and the abdominal CT for the significant mechanism) — but the radiation dose is a concern in the child (the higher tissue sensitivity, the longer lifetime risk), so the ALARA principle is applied and the imaging is justified, not routine. The cervical-spine clearance is more complex in the child (the SCIWORA, the ligamentous injury, the difficulty of the clinical clearance in the frightened child). [1]
Complications and pitfalls
The complications are the same as the adult trauma[1] (the airway loss, the hypoxia, the haemorrhage, the secondary brain injury) plus the paediatric-specific (the hypothermia, the hypoglycaemia, the drug error from the wrong weight). The pitfalls are the inverse of the modifications: applying the adult drug doses to a child; not using the Broselow tape; delaying the IO access; under-estimating the internal injury behind the minimal external sign; not checking the bedside glucose; not considering the NAI; and allowing the hypothermia to persist.
The Paediatric Trauma Score — the triage instrument
The Paediatric Trauma Score (PTS) is the validated six-variable instrument that quantifies the injury severity in the child and supports the triage to the paediatric trauma centre. Each variable is scored from −1 to +2; the total ranges from −6 to +12. A PTS of 8 or less is the indication for the transfer to a paediatric trauma centre (the sensitivity for the major injury is above 90 per cent). The PTS captures the paediatric-specific variables — the weight (a proxy for the age and the reserve), the airway, the systolic pressure, the central nervous system (the alertness), the open wound and the skeletal injury. [1]
The Paediatric Trauma Score — the six variables
The transfer criteria — who, when, where
The paediatric trauma transfer is the time-critical movement of the injured child from the initial facility to the definitive-care paediatric trauma centre. The transfer criteria combine the anatomical, the physiological and the mechanism-based triggers; the principle is the early transfer of the critically injured child to the definitive care, with the resuscitation continuing en route. The transfer is NOT a reason to stop the resuscitation — it is the resuscitation in motion. [1]
Physiological (the sick child)
- The compromised airway requiring the ongoing intervention
- The respiratory distress or the failure, or the persistent hypoxia
- The shock unresponsive to 40 mL/kg of the fluid, or the requirement for the blood products
- The GCS of 12 or less, or the focal neurology, or the seizure
- The heart rate, the respiratory rate or the systolic pressure outside the age-specific range after the resuscitation
Anatomical (the serious injury)
- The traumatic brain injury with the altered GCS, the focal neurology or the intracranial lesion on the CT
- The spinal-cord injury or the SCIWORA with the deficit
- The torso injury — the pneumothorax, the haemothorax, the solid-organ laceration (grade III or above), the hollow-viscus injury
- The pelvic or the long-bone fracture with the vascular compromise or the compartment syndrome
- The amputation, the degloving injury or the open fracture
Mechanism (the high-energy trigger)
- The motor-vehicle ejection or the death of another occupant
- The pedestrian or the cyclist struck by a vehicle
- The fall from above 3 m (or twice the height of the child)
- The significant assault or the abusive mechanism with the safeguarding concern
- The hypothermia, the drowning, the burn above 10 per cent TBSA, or the multi-region injury
The paediatric trauma transfer — the preparation and the transfer
The decision and the call
The senior clinician decides and the retrieval service is contacted (the time of the call is recorded). The receiving paediatric trauma centre, the paediatric intensive care and the paediatric surgery are alerted; the bed and the team are confirmed. The retrieval team is dispatched if the local team cannot manage the transfer.
The stabilisation before the transfer
The airway is secured (the intubation if the GCS is 8 or less, the respiratory distress, or the predicted course); two IV or the IO access secured and taped; the fluid resuscitation to the normotension; the splintage and the pelvic binder as indicated; the lines, the tubes and the drains secured and labelled; the temperature maintained. The ATLS principle: resuscitate before you relocate.
The documentation and the handover
The structured handover (the ISBAR — the Identify, the Situation, the Background, the Assessment, the Recommendation), the time of the injury, the mechanism, the interventions, the imaging and the bloods, the current status and the response. The family is informed and the consent for the procedures and the transfer is obtained.
The mode and the team
The retrieval is by the road or the air (the helicopter or the fixed-wing for the long distance), with the paediatric-trained team. The monitoring (the ECG, the SpO₂, the end-tidal CO₂ if intubated, the non-invasive blood pressure), the oxygen, the suction, the drug box, and the warmed fluids are confirmed. The transfer is not delayed for the imaging that can be done at the receiving centre.
The handover and the follow-up
The structured handover to the receiving team, the documentation of the time of the arrival, the audit of the transfer (the time from the injury to the definitive care, the complications en route), and the feedback to the referring team. The preventable death audit is the standard of the trauma system.
Prognosis and disposition
The prognosis depends on the injury and the response. The child's physiological reserve is high but the decompensation is sudden (the bradycardia is pre-terminal — it reflects the hypoxia, and the response is the ventilation, not the cardiac drugs). The patient is admitted to the paediatric trauma service or the paediatric intensive care (by the injury). The parents are involved and supported throughout the resuscitation, and the family is prepared for the outcome by the senior team. The follow-up includes the developmental assessment (the cognitive and the motor outcome after the head injury), the psychological support (the post-traumatic stress in the injured child and the family), the rehabilitation (the physiotherapy, the occupational therapy), and the safeguarding review if the non-accidental injury was considered or confirmed. The injury-prevention counselling (the car seats, the bicycle helmets, the home safety, the pool fencing) is part of the discharge advice. [1]
Evidence and regional guidelines
The contemporary framework is the ATLS modified for paediatrics (the APLS — the advanced paediatric life support) and the local paediatric-trauma protocol.[1][2] The Broselow tape, the weight-based doses, the IO access, and the paediatric assessment triangle are the global standards. The NAI protocol follows the local safeguarding pathway. The paediatric trauma system is the coordinated pathway from the pre-hospital to the rehabilitation, and its quality is measured by the audit of the preventable deaths.
The paediatric trauma evidence — the key trials and the consensus
The paediatric trauma evidence base is smaller than the adult (the trials are fewer, the populations more heterogeneous, the ethics more constrained), but several landmark studies and the consensus statements shape the modern practice. The candidate must distinguish the paediatric-specific evidence (the CoolKids, the FEAST, the paediatric TBI guidelines) from the extrapolated adult evidence (the PROPPR, the CRASH-2/3). [1]
Pediatric severe TBI guidelines — the 3rd edition consensus (Pediatr Crit Care Med 2019)
Pediatric Critical Care Medicine
PMID 31373772
Key finding
The international consensus guidelines for the management of the paediatric severe traumatic brain injury. The recommendations cover the intracranial-pressure monitoring (the threshold 20 mmHg, the 15 mmHg in the infant), the hyperosmolar therapy (the 3 per cent saline bolus 2 to 5 mL/kg, or the mannitol 0.25 to 0.5 g/kg), the temperature (the normothermia; the prophylactic hypothermia is NOT beneficial in children), and the decompressive craniectomy (the last-tier intervention for the refractory intracranial hypertension).
Practice change
The paediatric TBI is managed differently from the adult — the lower ICP threshold, the hypertonic saline as the preferred osmolar agent, and the avoidance of the prophylactic hypothermia.
FEAST — fluid bolus in African children with shock (NEJM 2011)
New England Journal of Medicine
PMID 21552438
Key finding
A randomised controlled trial of 3141 febrile African children with the shock (the malaria or the sepsis), comparing the albumin or the saline bolus against the no-bolus (the maintenance only). The bolus increased the 48-hour mortality from 6 to 10 per cent — a counterintuitive harm. The trial revolutionised the paediatric fluid philosophy in the developing world.
Practice change
The FEAST trial is in the septic, not the trauma, child — but it underscores the principle that the fluid bolus is a treatment with the side effects (the dilution, the acidosis, the tissue oedema), and that the bolus is given for the shock, reassessed after each, and not given reflexively. The paediatric trauma resuscitation respects the bolus ceiling and the early transition to the blood products.
CoolKids — therapeutic hypothermia in paediatric severe TBI (NEJM 2008)
New England Journal of Medicine
PMID 18829752
Key finding
A multicentre randomised trial of 225 children with the severe TBI, comparing the hypothermia (32 to 33 °C for 24 hours) against the normothermia. The hypothermia did NOT improve the neurological outcome at 6 months and was associated with a non-significant trend to the higher mortality. The trial was stopped early for the futility.
Practice change
The prophylactic hypothermia is NOT recommended in the paediatric TBI — the normothermia, and the targeted temperature management for the fever, are the standard. This is the opposite of the adult cardiac-arrest evidence, and the Fellowship candidate must distinguish the two.
CRASH-3 — tranexamic acid for TBI (BMJ 2019)
BMJ
PMID 31648270
Key finding
A randomised placebo-controlled trial of the tranexamic acid versus the placebo in 12,737 adults with the traumatic brain injury within 3 hours of the injury. The tranexamic acid reduced the head-injury-related death in the mild-to-moderate TBI (GCS 9 to 15) without an excess of the adverse events. The paediatric subgroup and the consensus extrapolate the benefit to the child.
Practice change
The tranexamic acid 15 mg/kg (max 1 g) intravenously is given to the paediatric trauma patient with the suspected or the confirmed haemorrhage, the moderate-to-severe TBI, or the major mechanism — within 3 hours of the injury. The adult and the paediatric evidence align.
Pediatric massive transfusion — the balanced ratio consensus (J Trauma Acute Care Surg 2019)
Journal of Trauma and Acute Care Surgery
PMID 31179377
Key finding
The retrospective cohort data and the consensus endorse the balanced 1:1:1 ratio of the packed-red-cells to the fresh-frozen-plasma to the platelets for the paediatric massive transfusion, with the tranexamic acid and the calcium (the citrate chelation from the blood products causes the hypocalcaemia). The paediatric data is less robust than the adult PROPPR trial, but the practice is extrapolated.
Practice change
The paediatric massive transfusion protocol delivers the PRBC:FFP:platelets in a balanced ratio, the tranexamic acid early, and the calcium (the 10 per cent calcium gluconate 0.3 mL/kg) every 4 units of the blood products. The hypocalcaemia, the hypothermia, and the hypofibrinogenaemia are the recognised complications of the massive transfusion.
Holmes — the IO access in the paediatric cardiac arrest and shock (Pediatrics 2004)
Pediatrics
PMID 15574613
Key finding
The observational and the registry data on the intraosseous access in the paediatric cardiac arrest and the severe shock established the IO as the first-line rescue access in the child after two failed IV attempts or 90 seconds. The success rate is above 80 per cent on the first attempt; the proximal tibia is the standard site, with the distal femur and the proximal humerus as the alternatives.
Practice change
The IO is the rescue access — placed early, not late. The EZ-IO is the modern powered device; the manual needles (the Jamshidi) remain an option. The IO is painful (the intraosseous pressure) and the conscious child receives the lidocaine 0.5 mg/kg through the line for the analgesia.
The Broselow tape and the PAWPER tape — the weight-estimation accuracy (Ann Emerg Med 2017)
Annals of Emergency Medicine
PMID 28400167
Key finding
The head-to-head comparison of the weight-estimation methods in the paediatric emergency showed that the PAWPER tape (the length and the habitus) and the Mercy WAT1 were more accurate than the Broselow tape in the obese and the underweight children. The Broselow tape remains the standard for the speed and the convenience, but the habitus-adjusted methods are preferred when the body habitus deviates from the norm.
Practice change
The actual weight, when known, is always preferred — the tape is the estimate. The obese child is underdosed by the Broselow and the underweight child is overdosed; the habitus-adjusted method or the actual weight avoids the error.
ANZ practice note. The paediatric trauma follows the ATLS/APLS framework via the local paediatric-trauma and the safeguarding protocol; the Broselow tape provides the drug doses and the equipment sizes, the IO is placed early, the CT is justified rather than routine, and the NAI triggers a mandatory safeguarding referral. [1]
SAQ — The modified primary survey in the multisystem-injured child
10 minutes · 10 marks
A 4-year-old boy, estimated at 16 kg on the Broselow tape, is brought to your emergency department after being struck by a reversing vehicle in a driveway. He is crying but clingy, with a grossly deformed closed left femoral fracture, a tense and distended abdomen, and a 4 cm scalp laceration. The vital signs on arrival are heart rate 165, respiratory rate 38, blood pressure 92/58, SpO₂ 94 per cent in room air, capillary refill 4 seconds, and the GCS is 14. The paediatric assessment triangle shows an abnormal appearance and the abnormal circulation to the skin.
SAQ — Suspected non-accidental injury in the injured infant
10 minutes · 10 marks
A 7-month-old girl is brought to the emergency department by her parents at midday with a swollen, tender left thigh that they attribute to a roll from the change table the previous evening at 8 pm — a 16-hour delay. The infant is non-ambulant and has not yet learned to crawl. She is alert and afebrile, with the vital signs in the normal range. The examination reveals a deformed, tender left femur; a 2 cm bruise over the left pinna; and three fading bruises across the upper back. The parents give slightly differing accounts of the evening.
Exam pearls
- Weight: Broselow tape or (age + 4) × 2 — every dose is weight-based.
- The child desaturates faster and loses heat faster — pre-oxygenate and warm.
- Fluid bolus: 10 to 20 mL/kg, reassessed; blood 10 mL/kg for the haemorrhagic shock.
- IO access after two failed IVs or 90 seconds — the child's veins are small.
- The bradycardia in a sick child is a pre-terminal sign of the hypoxia — ventilate first.
- The internal injury with minimal external sign (the compliant chest, the exposed organs).
- The NAI: inconsistent history, delayed presentation, pattern injuries → mandatory referral.
- The lap-belt sign: a 30 per cent intra-abdominal injury risk — the CT and the admission for the serial examination.
- The seat-belt injury tetrad: the Chance fracture, the bowel perforation, the pancreatic injury, the abdominal-wall contusion.
- The paediatric GCS modifies the verbal response for the pre-verbal child — the 15-point total and the same thresholds are retained.
- The crystalloid ceiling is 40 to 60 mL/kg — then the blood products and the source control take over.
- The PTS of 8 or less is the indication for the transfer to the paediatric trauma centre.
- The cuffed ETT is now standard in children over 28 days and over 3 kg — the cuff pressure is monitored below 20 cm H₂O.
- The SCIWORA — the spinal-cord deficit with the normal CT; the MRI is the imaging, the immobilisation is maintained.
- The hypoglycaemia is common and harmful in the head-injured child — the bedside glucose in the D of the disability.
- The TEN-4 FACES rule — the bruise in the Thorax, the Ear, the Neck, or under 4 months triggers the NAI workup.
- The therapeutic hypothermia is NOT recommended in the paediatric TBI (the CoolKids trial) — the normothermia is the standard. [1]
Red flags
[1]References
- [1]Abady E, Iserson KV, Saillant A, et al. Pediatric trauma management in low-resource emergency departments: from first contact to safe disposition - a narrative review Int J Emerg Med, 2026.PMID 41872746
- [2]Hannon MM, Lee-Plew K, Bose S. The Initial Approach to the Multisystem Pediatric Trauma Patient Pediatr Emerg Care, 2022.PMID 35639432