EM · Upper gastrointestinal bleed
Upper gastrointestinal bleed
Also known as Upper GI haemorrhage · Haematemesis and melaena · Acute upper GI bleeding · Variceal bleed · Peptic ulcer bleed
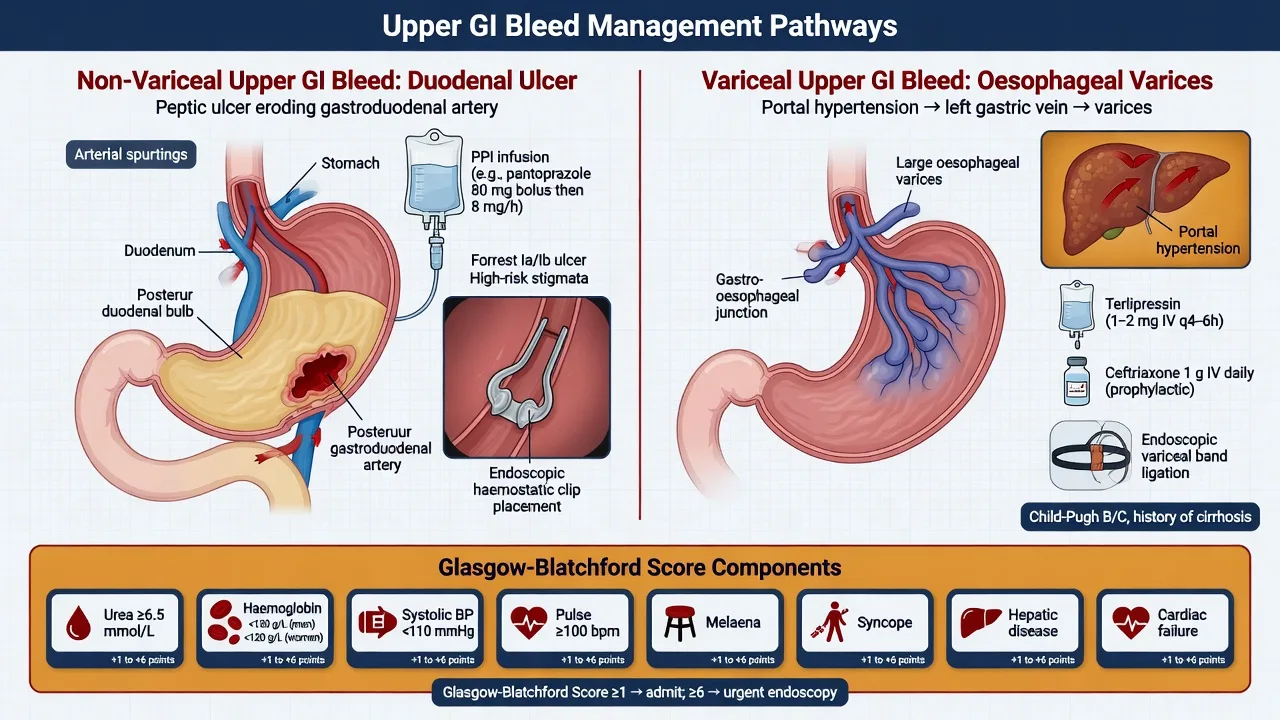
The upper gastrointestinal bleed — the haemorrhage proximal to the ligament of Treitz, divided into the variceal (the oesophageal and gastric varices of the portal hypertension) and the non-variceal (the peptic ulcer, the Mallory-Weiss tear, the erosive gastritis, the upper-GI malignancy). The Glasgow-Blatchford score for the pre-endoscopic risk stratification — the haemoglobin, the urea, the systolic blood pressure, the pulse, the melaena, the syncope, the hepatic disease, the cardiac failure. The management — the ABCDE, the large-bore IV access, the restrictive transfusion at a haemoglobin threshold 70 to 80 g/L, the terlipressin 2 mg intravenously four times daily and the ceftriaxone 2 g intravenously daily for the variceal bleed, the pantoprazole 80 mg intravenous bolus then 8 mg/h infusion, the urgent oesophagogastroduodenoscopy within 24 hours (within 12 hours for the suspected variceal bleed), and the TIPSS for the refractory variceal haemorrhage. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The upper gastrointestinal bleed — the haemorrhage from anywhere proximal to the ligament of Treitz — is one of the commonest true medical emergencies and a high-yield Fellowship topic because the candidate must, within the first minutes of the resuscitation, split the bleed into the variceal and the non-variceal pathway. The two pathways share the ABCDE and the restrictive transfusion but diverge on the vasoactive drug (the terlipressin), the antibiotic prophylaxis (the ceftriaxone), the endoscopic timing (within 12 hours versus 24 hours) and the rescue therapy (the balloon tamponade and the TIPSS). The mortalities are different — the variceal bleed carries a 15 to 25 per cent in-hospital mortality, the non-variceal around 5 to 10 per cent — and the drugs that save lives in the one are useless or harmful in the other. The Fellowship candidate who reaches for the terlipressin in every haematemesis, or who transfuses to a haemoglobin of 100 g/L "to be safe," fails the station.[2][3]


Definition and the variceal-versus-non-variceal split
An upper gastrointestinal bleed is any haemorrhage arising proximal to the ligament of Treitz. It presents as the haematemesis (the vomiting of blood — fresh red or coffee-ground), the melaena (the black, tarry, foul-smelling stool of the digested blood, classically with a melaena stool the result of at least 50 mL of blood in the upper tract), or the haematochezia (the passage of fresh red blood per rectum — when it comes from an upper source it signals a torrential, rapid-transit bleed and the patient is usually shocked). A melaena-class presentation is the commonest. [1]
The single most important early distinction is the variceal versus the non-variceal bleed, because it changes the immediate drug therapy. [1]
Variceal bleed (portal hypertension)
- Source: oesophageal or gastric varices, portal hypertensive gastropathy
- Background: cirrhosis, chronic hepatitis, alcohol, portal vein thrombosis
- Signs of chronic liver disease: jaundice, spider naevi, palmar erythema, ascites, caput
- Drugs on arrival: terlipressin + ceftriaxone; early endoscopy within 12 hours
- Rescue: Sengstaken-Blakemore tube, TIPSS
Peptic ulcer bleed
- Source: duodenal or gastric ulcer
- Background: Helicobacter pylori, NSAIDs, aspirin, stress ulcer
- Often clean-based (low-risk) or with a visible vessel (high-risk)
- Drugs on arrival: pantoprazole infusion; endoscopy within 24 hours
- Endoscopic therapy: adrenaline injection + thermal or clip
Mallory-Weiss tear
- Source: mucosal tear at the gastro-oesophageal junction
- Background: repeated retching, vomiting, binge alcohol, hyperemesis
- Bleeding usually self-limiting; preceded by non-bloody vomiting then blood
- Drugs: supportive; endoscopy if persistent
- Low mortality; conservative management usually suffices
Erosive gastritis / malignancy
- Gastritis: NSAIDs, alcohol, stress-related mucosal disease (the ICU patient)
- Malignancy: gastric or oesophageal cancer, GIST — weight loss, dysphagia
- Often oozing rather than spurting; multiple erosions at endoscopy
- Drugs: PPI infusion; treat the underlying cause
- Biopsy at endoscopy; lower transfusion threshold for chronic ooze
The variceal bleeds make up roughly 10 to 20 per cent of the upper-GI bleeds in the ANZ and UK cohorts but a disproportionate share of the mortality; the non-variceal bleeds, dominated by the peptic ulcer, make up the majority. [1]
Epidemiology and risk
The upper gastrointestinal bleed carries an overall incidence of 50 to 150 per 100,000 adults per year and a mortality that has changed little in three decades at around 5 to 10 per cent for the non-variceal and 15 to 25 per cent for the variceal. The mortality rises steeply with age, with comorbidity, and with the inpatient-onset bleed (the hospital-acquired bleed carries twice the mortality of the community-acquired). The risk factors are the NSAID and the aspirin use (the non-variceal), the anticoagulants and the antiplatelets (potentiate any source), the Helicobacter pylori infection (the peptic ulcer), the alcohol and the chronic liver disease (the variceal and the gastritis), and the critical illness with the multi-organ failure (the stress-related mucosal disease of the ICU).[1]
Pathophysiology — the two mechanisms
The non-variceal peptic ulcer bleeds when the acid and the pepsin overwhelm the mucosal defences (the prostaglandin-mediated mucus-bicarbonate barrier) and erode into a submucosal artery — classically the gastroduodenal artery in a posterior duodenal ulcer, or a branch of the left gastric artery in a gastric ulcer along the lesser curvature. The NSAIDs inhibit the cyclo-oxygenase and deplete the protective prostaglandins; the Helicobacter pylori sets up a chronic antral gastritis and the duodenitis. The bleeding stops spontaneously in 80 per cent of the ulcer bleeds — the problem is the rebleeding, which is what the endoscopic therapy and the proton pump inhibitor aim to prevent. [1]
The portal hypertension of the cirrhosis has two components — the structural (the fibrosis that distorts the hepatic sinusoids) and the functional (the splanchnic vasodilation driven by the nitric oxide, which increases the portal inflow). The terlipressin and the octreotide target the functional component; the TIPSS and the band ligation the structural and the mechanical.[3]
Clinical presentation — what the bedside tells you
The history and the examination at the bedside answer three questions: is this an upper-GI bleed, how sick is the patient, and is there a variceal background. [1]
The haematemesis confirms an upper-GI source. The melaena — the black tarry stool — also confirms an upper source but is slower; the coffee-ground vomitus suggests a slower, partially digested bleed. The haematochezia from an upper source is the danger sign — it means the bleed is so fast that the blood transits the gut before it can be digested, and the patient is usually haemodynamically compromised. The symptoms of the hypovolaemia — the postural dizziness, the syncope, the thirst, the oliguria — must be asked for directly. [1]
The examination looks for the stigmata of the chronic liver disease (the jaundice, the spider naevi, the palmar erythema, the gynaecomastia, the parotid enlargement, the ascites, the caput medusae, the asterixis) which flag the variceal pathway; for the signs of the shock (the tachycardia, the hypotension, the cool peripheries, the prolonged capillary refill, the oliguria, the altered mental state); and for the comorbidities (the cardiac failure, the renal disease, the malignancy) that raise the Glasgow-Blatchford and the mortality. A digital rectal examination confirms the melaena — do not skip it. [1]
Differential diagnosis — the causes and the mimics
The cause of the bleed is established at the endoscopy, but the bedside generates the differential and the pre-test probability. [1]
The causes of the upper gastrointestinal bleed, by the frequency and by the pathway: [1]
- Non-variceal (80 to 90 per cent): the peptic ulcer (the duodenal and the gastric, around 40 to 50 per cent of all the bleeds), the erosive gastritis or the duodenitis, the Mallory-Weiss tear (the mucosal laceration at the gastro-oesophageal junction after the retching), the oesophagitis, the upper-GI malignancy (the gastric, the oesophageal, the GIST), the angiodysplasia, the Dieulafoy lesion (the anomalous submucosal artery that erodes through a tiny mucosal defect — a trivial-looking but high-volume bleeder), and the aortoenteric fistula (the catastrophic bleed in the patient with the prior aortic graft — always think of it in the right clinical context).
- Variceal (10 to 20 per cent): the oesophageal varices (the commonest variceal source), the gastric varices (the fundal, harder to band, may need the tissue adhesive), the portal hypertensive gastropathy. [1]
The mimics — the haemoptysis (coughed, frothy, bright red, alkaline) and the epistaxis or the swallowed blood from the upper airway — are distinguished by the history; the coffee-ground appearance of the haematemesis is pathognomonic of the gastric-origin blood. [1]
[1]Bedside assessment — the ABCDE and the two-pathway triage
The resuscitation and the diagnostic pathway run in parallel. The ABCDE first; the risk stratification (the Glasgow-Blatchford) in parallel; the early activation of the endoscopy and, where the variceal background is known or suspected, the terlipressin and the ceftriaxone. [1]
- A and B: protect the airway in the torrential haematemesis (the aspiration is a leading cause of the death); give the high-flow oxygen; consider the early intubation for the encephalopathic, the shocked, or the uncontrolled variceal bleeder before the endoscopy.
- C — the circulation: two large-bore intravenous cannulae (14 or 16 gauge), the crossmatch of 2 to 4 units, the bedside haemoglobin and the venous gas (the lactate), the focused assessment (the pulse, the blood pressure, the capillary refill, the urine output via the catheter). The restrictive transfusion at a haemoglobin threshold of 70 to 80 g/L for the haemodynamically stable; transfuse earlier for the shocked or the unstable. Avoid the crystalloid overload in the cirrhotic (it raises the portal pressure and the ascites).
- D and E: assess the conscious level (AVPU) — the shock and the encephalopathy both depress the consciousness; check the glucose (the chronic liver disease and the alcohol), and the temperature (the hypothermia worsens the coagulopathy).
- The two-pathway triage: if the cirrhosis is known or the stigmata of the chronic liver disease are present, start the terlipressin 2 mg intravenously four times daily and the ceftriaxone 2 g intravenously daily at the bedside, before the endoscopy, and book the urgent endoscopy within 12 hours. If the non-variceal pathway, give the pantoprazole 80 mg intravenous bolus then 8 mg/h infusion and book the endoscopy within 24 hours. [1]
Investigations — the bloods, the score and the endoscopy
The blood panel is the full blood count (the haemoglobin may be normal early — the haemodilution lags the bleed by 6 to 12 hours), the coagulation (the INR, especially in the cirrhotic and the anticoagulated), the urea and the creatinine (the urea rises disproportionately because the digested blood is a protein load absorbed as the urea — a raised urea-to-creatinine ratio points to the upper source), the liver function tests, the crossmatch, the venous gas with the lactate, and the troponin (the demand ischaemia and the anticoagulation hold). The ECG and the chest radiograph for the older patient and the cardiac comorbidity. [1]
The Glasgow-Blatchford score — reproduced
The Glasgow-Blatchford score (GBS) is the pre-endoscopic risk-stratification tool validated to predict the need for the intervention (the transfusion, the endoscopic therapy, the surgery) and the mortality. It is calculated entirely from the bedside and the bloods — no endoscopy required — and it is the score the Fellowship examiner expects reproduced.[1]
| Component | Value | Points |
|---|---|---|
| Urea (mmol/L) | 6.5 to 7.9 / 8.0 to 9.9 / 10.0 to 24.9 / 25 or more | 2 / 3 / 4 / 6 |
| Haemoglobin men (g/L) | 120 to 129 / 100 to 119 / less than 100 | 1 / 3 / 6 |
| Haemoglobin women (g/L) | 100 to 119 / less than 100 | 1 / 6 |
| Systolic blood pressure (mmHg) | 100 to 109 / 90 to 99 / less than 90 | 1 / 2 / 3 |
| Pulse (beats per minute) | 100 or more | 1 |
| Melaena | present | 1 |
| Syncope | present | 1 |
| Hepatic disease | present (any history) | 2 |
| Cardiac failure | present (any history) | 2 |
The score ranges from 0 to 23. A score of 0 identifies a low-risk patient who may be managed as an outpatient or discharged with the early endoscopy — a strategy that is safe and reduces the admissions, validated in the original derivation and the subsequent prospective cohorts.[1] A score of 7 or more marks the high-risk group with the 50 per cent or greater need for the intervention and the higher mortality.
The endoscopy is both the diagnostic and the therapeutic gold standard. It identifies the source, applies the endoscopic therapy (the band ligation for the varix, the adrenaline injection plus the thermal coagulation or the clip for the ulcer with the high-risk stigmata — the spurting vessel, the visible non-bleeding vessel, the adherent clot), and stratifies the rebleeding risk (the Forrest classification: Ia spurting, Ib oozing, IIa visible vessel, IIb adherent clot, IIc pigmented spot, III clean base). [1]

The Rockall score — the complete and the pre-endoscopic
The Rockall score was derived from the 4185-patient national audit of the upper-GI bleeding in the United Kingdom and published in 1996. Unlike the Glasgow-Blatchford (which predicts the need for the intervention), the Rockall score predicts the mortality. It has two forms: the pre-endoscopic (initial) Rockall — scored on the age, the shock, and the comorbidity, calculable at the bedside before the endoscopy — and the complete (post-endoscopic) Rockall, which adds the endoscopic diagnosis and the stigmata of the recent haemorrhage. The pre-endoscopic Rockall ranges from 0 to 7; the complete from 0 to 11.[5]
| Variable | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Age | less than 60 | 60 to 79 | 80 or more | — |
| Shock | SBP 100 or more, pulse less than 100 | SBP 100 or more, pulse 100 or more | SBP less than 100 | — |
| Comorbidity | None | — | Cardiac failure, ischaemic heart disease, any major comorbidity | Renal failure, liver failure, disseminated malignancy |
| Diagnosis (endoscopic) | Mallory-Weiss tear or no lesion identified | All other malignancies of the upper-GI tract | — | — |
| Major stigmata of recent haemorrhage | None or dark spot only | — | Blood in the upper-GI tract, adherent clot, visible or spurting vessel | — |
The complete Rockall of 3 or more identifies the patients at the high risk of the rebleeding and the death; a score of 0 or 1 carries the near-zero mortality and the rebleeding risk below 5 per cent. The Fellowship candidate should be able to calculate both the pre-endoscopic and the complete Rockall at the viva — the pre-endoscopic for the triage on the arrival, the complete for the post-endoscopic disposition decision.[5]
Glasgow-Blatchford (GBS)
- Timing: pre-endoscopic only
- Predicts: need for intervention (transfusion, endoscopic therapy, surgery)
- Inputs: urea, Hb, SBP, pulse, melaena, syncope, hepatic disease, cardiac failure
- Range 0 to 23; score of 0 = safe for outpatient, 7 or more = high-risk
- Strength: excellent sensitivity (near 99 per cent) for identifying low-risk patients; no endoscopy needed
- Weakness: moderate specificity; over-triages some low-risk patients
Rockall
- Timing: pre-endoscopic and post-endoscopic forms
- Predicts: mortality (primary), rebleeding (secondary)
- Inputs: age, shock, comorbidity, diagnosis, stigmata of recent haemorrhage
- Range 0 to 11; 3 or more = high-risk
- Strength: incorporates endoscopic findings for the post-endoscopic risk; validated mortality prediction
- Weakness: less sensitive than GBS for identifying the safe-for-discharge group
AIMS65
- Timing: pre-endoscopic
- Predicts: in-hospital mortality (primary)
- Inputs: Albumin less than 30 g/L, INR greater than 1.5, altered Mental status, SBP 90 or less, age 65 or more
- One point per variable; range 0 to 5
- Strength: simple; predicts mortality and length of stay
- Weakness: does not predict need for intervention as well as GBS; less validated in the ANZ cohorts
Immediate management — the resuscitation and the restrictive transfusion
The resuscitation is the priority and runs in parallel with the workup. [1]
The restrictive transfusion strategy was established by the Villanueva trial of 2013 — a randomised comparison of the transfusion at a haemoglobin threshold of 70 g/L (the restrictive) versus 90 g/L (the liberal) in 921 patients with the severe upper-GI bleed. The restrictive arm had the lower six-week mortality (5 per cent versus 9 per cent), the lower rebleeding rate, and — critically in the cirrhotic subgroup with the Child-Pugh A or B — the higher survival. The over-transfusion raises the portal venous pressure, disrupts a fresh clot, and increases the rebleeding.[2]
Definitive management — the two pathways
The definitive management is the endoscopic therapy, escalated by the radiological and the surgical rescue. The drugs differ by the pathway. [1]
The non-variceal pathway
- Proton pump inhibitor: the pantoprazole 80 mg intravenous bolus then 8 mg/h infusion for 72 hours after the successful endoscopic therapy of a high-risk ulcer (the Forrest Ia, Ib, IIa, IIb). The PPI stabilises the clot (the gastric pH above 6 stabilises the platelet aggregation and the fibrinolysis) and reduces the rebleeding, the surgery and the mortality. Note: the pre-endoscopic PPI does not change the mortality, but it downstages the lesion and reduces the endoscopic therapy need.
- Endoscopic therapy: the combination of the adrenaline 1:10,000 injection with the thermal coagulation or the clip for the high-risk stigmata — the monotherapy with the adrenaline alone is inadequate.
- The aspirin and the NSAIDs: hold during the active bleed, but the aspirin is resumed early — the Sung trial of 2010 randomised the aspirin users with the peptic ulcer bleed to the continuation versus the cessation and found that the early continuation (within 7 days) reduced the 30-day cardiovascular mortality and serious thrombotic events without a significant increase in the rebleeding.[4]
- The Helicobacter pylori: test and treat at the follow-up; the eradication reduces the rebleeding from the ulcer.
Non-variceal bleed — the management sequence
1
Two large-bore cannulae, crossmatch, venous gas + lactate, GBS and pre-endoscopic Rockall. Restrictive transfusion to Hb 70 to 80 g/L.
2
Pantoprazole 80 mg IV bolus, then 8 mg/h infusion — started pre-endoscopy to downstage the lesion. Do not delay the endoscopy for the PPI.
3
Identify the source. Apply combination endoscopic therapy for the high-risk stigmata (Forrest Ia, Ib, IIa, IIb): adrenaline injection + clip or thermal coagulation.
4
Continue 8 mg/h infusion for 72 hours after the successful haemostasis of the high-risk ulcer — reduces the rebleeding, the surgery, and the mortality.
5
Stop NSAIDs; test for H. pylori (eradicate if positive); resume aspirin within 7 days for the secondary prevention. Low-risk Rockall 0 to 1 = discharge; 3 or more = high-dependency.
Lau 2000 — IV omeprazole after endoscopic therapy
N Engl J Med
PMID 10922420
RCT, 240 patients with bleeding peptic ulcers after successful endoscopic therapy
Key finding
IV omeprazole 80 mg bolus then 8 mg/h infusion for 72 hours reduced the 30-day rebleeding from 22.4 per cent to 6.7 per cent compared with placebo.
Practice change
The 72-hour high-dose PPI infusion after the endoscopic haemostasis is the standard for the high-risk ulcer.
The variceal pathway
- The vasoactive drug: the terlipressin 2 mg intravenously four times daily for 3 to 5 days (the UK and the European first-line; in the ANZ the octreotide 50 micrograms intravenous bolus then 50 micrograms per hour infusion is the common alternative). The terlipressin is the splanchnic vasoconstrictor that lowers the portal inflow and the HVPG; the evidence supports the reduction in the failure to control the bleeding and the mortality when started early, before the endoscopy.
- The antibiotic prophylaxis: the ceftriaxone 2 g intravenously daily for up to 7 days. The cirrhotic with the variceal bleed is at the high risk of the bacterial infection (the spontaneous bacterial peritonitis, the bacteraemia, the pneumonia) and the infection predicts the failure to control the bleeding, the rebleeding, and the death. The antibiotic reduces the mortality — the number-needed-to-treat is around 10 — and is given on the arrival, not after the endoscopy. The ceftriaxone has displaced the oral norfloxacin and the ciprofloxacin as the preferred agent on the strength of the trial evidence of the superior outcomes in the high-risk (Child-Pugh C) cirrhotic.
- The endoscopy within 12 hours: the endoscopic band ligation for the oesophageal varix; the tissue adhesive (the N-butyl-cyanoacrylate) injection for the gastric fundal varix (the banding of a fundal varix risks the catastrophic ulceration).
- The balloon tamponade (the rescue): the Sengstaken-Blakemore or the Minnesota tube for the refractory variceal bleed as the bridge to the definitive therapy — inflated for up to 24 hours, with the airway protected; a temporising measure, not the definitive therapy. [1]
Variceal bleed — the management sequence
1
Protect the airway — aspiration is the leading cause of death. High-flow oxygen; consider early intubation for the encephalopathic or the uncontrolled bleeder. Two large-bore cannulae, crossmatch, catheter.
2
Start BOTH before the endoscopy. Terlipressin 2 mg IV QDS (or octreotide 50 mcg bolus then 50 mcg/h). Ceftriaxone 2 g IV daily. Restrictive transfusion to Hb 70 to 80 g/L.
3
Endoscopic band ligation for oesophageal varices. N-butyl-cyanoacrylate glue injection for gastric fundal varices (never band a fundal varix).
4
Sengstaken-Blakemore or Minnesota tube as the bridge to the definitive therapy (max 24 hours, airway protected). Keep the terlipressin and the antibiotic running.
5
Transjugular intrahepatic portosystemic shunt. Consider the early (pre-emptive) TIPSS within 72 hours for the high-risk cirrhotic (Child-Pugh 10 to 13, or 7 to 9 with the active bleeding).
Sengstaken-Blakemore tube
- Three lumens: gastric aspiration, gastric balloon inflation, oesophageal balloon inflation
- No oesophageal aspiration lumen — risk of the aspiration pneumonia
- Gastric balloon inflated first (200 to 250 mL air or water); the oesophageal balloon only if the bleeding persists (at 30 to 40 mmHg)
- Maximum dwell time 24 hours — the necrosis risk beyond
- The airway must be protected — intubate the encephalopathic or the uncontrolled bleeder before insertion
Minnesota tube
- Four lumens: adds the oesophageal aspiration lumen to the SBT configuration
- Lower aspiration risk than the SBT — the preferred device where available
- Same gastric and oesophageal balloon inflation technique and pressures
- Maximum dwell time 24 hours; the traction with the 1 kg weight or the football helmet
- The definitive therapy (the TIPSS) must be planned before the insertion — the balloon is only the bridge
Fully covered self-expanding metal stent (FCSEMS)
- The modern alternative to the balloon tamponade — placed endoscopically across the gastro-oesophageal junction
- Tamponades the varices by the radial force without the balloon; no pressure necrosis
- Can stay in situ up to 7 days (versus 24 hours for the balloon)
- Not yet universally available; requires the endoscopic expertise
- The evidence is emerging; the balloon tamponade remains the default rescue in the most centres
García-Pagán 2010 — Early TIPSS in high-risk cirrhosis
N Engl J Med
PMID 20573925
RCT, 63 cirrhotic patients with the acute variceal bleeding and Child-Pugh 8 to 13 (or 10 to 13 in the pilot)
Key finding
The early (pre-emptive) TIPSS within 72 hours of the index endoscopy reduced the 1-year rebleeding from 41 per cent to 14 per cent and the mortality from 39 per cent to 14 per cent compared with the standard pharmacological plus endoscopic therapy.
Practice change
The high-risk cirrhotic (Child-Pugh C 10 to 13, or B 7 to 9 with the active bleeding) should be discussed for the early TIPSS.
Chávez-Tapia 2010 — Antibiotic prophylaxis in cirrhotic GI bleeding (Cochrane)
Cochrane Database Syst Rev
PMID 20824832
Meta-analysis of 8 RCTs, 864 patients with cirrhosis and upper-GI bleeding
Key finding
Antibiotic prophylaxis reduced all-cause mortality (RR 0.79), bacterial infections (RR 0.43), rebleeding (RR 0.58), and hospital stay. The number-needed-to-treat for the mortality was approximately 10 to 15.
Practice change
The antibiotic prophylaxis is the standard of care for every cirrhotic with the upper-GI bleed, given on the arrival. The ceftriaxone is the preferred agent.
Subtypes and scenarios
The gastric varix is harder to treat than the oesophageal — the band ligation is less effective and riskier, and the tissue adhesive (the cyanoacrylate glue) injection is the endoscopic therapy of choice. The portal hypertensive gastropathy presents with the chronic, the insidious ooze rather than the torrential haemorrhage; the management is the non-selective beta-blocker (the propranolol or the carvedilol) for the long-term portal-pressure reduction, not the endoscopic therapy. The ulcer with the spurting vessel is the highest-risk non-variceal lesion — the combined endoscopic therapy plus the high-dose PPI, with the early surgical or the interventional-radiology rescue if it fails. The Mallory-Weiss tear usually settles with the supportive care; the endoscopic therapy is reserved for the active bleed. The Dieulafoy lesion — the tiny mucosal defect over the large submucosal artery — is easy to miss at the endoscopy and often rebleeds; the endoscopic clip or the band ligation of the bleeding point is definitive. [1]
Airway protection in the massive haematemesis
The airway is the first priority in the massive haematemesis — the aspiration of the blood is the leading cause of the death in the uncontrolled variceal bleed, not the exsanguination. The encephalopathic cirrhotic, the shocked patient, and the agitated or the uncooperative bleeder are at the highest risk. The early endotracheal intubation — before the endoscopy — protects the airway from the ongoing haematemesis and the regurgitation during the procedure, and it allows the endoscopist the controlled field. The RSI (the rapid sequence induction) with the head-up tilt and the suction ready is the standard; the video laryngoscopy is the fallback for the difficult airway. The intubation is not without the risk — the cirrhotic with the ascites and the pleural effusions is the difficult physiology for the induction and the ventilation — but the unprotected airway in the torrential bleeder is worse. [1]
[1]Complications and pitfalls
The complications are the aspiration (the leading cause of the death in the uncontrolled variceal bleed — protect the airway, intubate early for the encephalopathic bleeder), the hypovolaemic shock and the end-organ failure (the acute kidney injury, the myocardial infarction), the coagulopathy (the dilutional, the liver-related, the anticoagulant-related), the rebleeding (the highest risk in the first 72 hours), the spontaneous bacterial peritonitis and the sepsis in the cirrhotic, and the post-TIPSS hepatic encephalopathy. The pitfalls: failing to identify the variceal background (and so withholding the terlipressin and the ceftriaxone); over-transfusing (the rebleeding and the raised portal pressure); giving the PPI in lieu of the endoscopy; delaying the endoscopy beyond the 24-hour window; using the Sengstaken-Blakemore tube without the airway protection; and missing the aortoenteric fistula in the patient with the prior aortic graft. [1]
Prognosis and disposition
The mortality is 5 to 10 per cent for the non-variceal and 15 to 25 per cent for the variceal. The high-risk markers are the shock at the presentation, the comorbidity (the cardiac, the renal, the hepatic), the inpatient-onset bleed, the high Glasgow-Blatchford, the high-risk endoscopic stigmata (the Forrest Ia, Ib), and — in the cirrhotic — the Child-Pugh class and the MELD score. The disposition: the low-risk (the GBS of 0 to 1, the negative endoscopy) for the discharge with the early outpatient endoscopy; the moderate-risk to the ward with the endoscopy within 24 hours; the high-risk and the variceal to the high-dependency or the intensive care after the endoscopy, monitored for the rebleeding. [1]
Special populations
The cirrhotic patient is the priority — the terlipressin, the ceftriaxone, the endoscopy within 12 hours, and the early-TIPSS consideration in the high-risk. The anticoagulated patient has the coagulopathy as the cofactor, not the cause; reverse to the safe range for the life-threatening bleed (the INR below 2 for the warfarin), identify and treat the source, and resume the anticoagulant early once the haemostasis is achieved. The antiplatelet patient on the aspirin for the secondary cardiovascular prevention should have the aspirin continued or resumed within 7 days — the Sung evidence supports the safety and the cardiovascular-mortality benefit.[4] The elderly and the cardiac-comorbid patient is at the higher risk of the demand ischaemia and the death; the transfusion threshold is set a little higher (around 80 to 90 g/L) to protect the myocardium, but still restrictive. The renal-disease patient tolerates the hypovolaemia poorly and the fluid overload even worse — the careful, the balanced resuscitation.
Evidence and regional guidelines
The contemporary framework rests on three pillars: the restrictive transfusion at a haemoglobin of 70 to 80 g/L (the Villanueva 2013, NEJM, the level-1 evidence)[2]; the vasoactive drug plus the antibiotic for the variceal bleed started on the arrival, before the endoscopy[3]; and the PPI infusion with the endoscopic combination therapy for the high-risk ulcer. The Glasgow-Blatchford remains the validated pre-endoscopic risk tool;[1] the AIMS65 and the Rockall scores are the alternatives (the AIMS65 for the mortality prediction, the post-endoscopic Rockall adding the endoscopic findings). The early aspirin resumption in the secondary-prevention patient is supported by the Sung trial.[4]
Villanueva 2013 — Restrictive vs liberal transfusion
N Engl J Med
PMID 23281973
RCT, 921 patients with the severe upper-GI bleed randomised to the restrictive (Hb threshold 70 g/L) versus the liberal (Hb threshold 90 g/L) transfusion
Key finding
The restrictive strategy reduced the 6-week mortality (5 per cent vs 9 per cent, P = 0.02), the further bleeding (10 per cent vs 16 per cent), and the adverse events. In the cirrhotic subgroup (Child-Pugh A or B), the survival was higher with the restrictive strategy (95 per cent vs 82 per cent).
Practice change
The restrictive transfusion at a haemoglobin of 70 to 80 g/L is the standard for the haemodynamically stable upper-GI bleed.
Blatchford 2000 — The Glasgow-Blatchford score
Lancet
PMID 11073021
Prospective study of 1748 patients with the upper-GI bleed, deriving and validating a pre-endoscopic risk score
Key finding
The GBS, calculated entirely from the bedside and the bloods (urea, Hb, SBP, pulse, melaena, syncope, hepatic disease, cardiac failure), identified the low-risk patients (score of 0) with the sensitivity of 99 per cent and the specificity of 35 per cent for the need for the intervention.
Practice change
The GBS of 0 identifies the patient safe for the outpatient or the early-discharge pathway; the 7 or more marks the high-risk group.
Sung 2010 — Aspirin continuation in the peptic ulcer bleed
Ann Intern Med
PMID 19949136
RCT, 156 aspirin users with the peptic ulcer bleeding after the endoscopic haemostasis, randomised to the aspirin continuation versus the placebo (cessation) for 8 weeks
Key finding
The continuation of the low-dose aspirin reduced the 30-day all-cause mortality (1 per cent vs 12 per cent) and the serious thrombotic events without a significant increase in the recurrent bleeding (10.3 per cent vs 5.4 per cent).
Practice change
In the patient on the aspirin for the secondary cardiovascular prevention, the aspirin is continued or resumed within 7 days of the ulcer bleed.
Rockall 1996 — The Rockall risk score
Gut
PMID 8675081
National UK audit of 4185 patients with the acute upper-GI bleed, deriving and validating a risk score for the mortality and the rebleeding
Key finding
The Rockall score (0 to 11), incorporating the age, the shock, the comorbidity, the diagnosis, and the stigmata of the recent haemorrhage, predicted the mortality (score of 0 to 1 = near-zero mortality; 3 or more = 15 to 40 per cent mortality) and the rebleeding risk.
Practice change
The pre-endoscopic and the complete Rockall score the risk of the death and the rebleeding, complementing the GBS.
Saltzman 2011 — The AIMS65 score
Gastrointest Endosc
PMID 21907980
Retrospective cohort of 2963 patients with the acute upper-GI bleed, deriving and validating the AIMS65 score
Key finding
The AIMS65 (Albumin less than 30 g/L, INR greater than 1.5, altered Mental status, SBP 90 or less, age 65 or more — one point each, range 0 to 5) predicted the in-hospital mortality, the length of stay, and the cost, outperforming the GBS and the Rockall for the mortality prediction in the derivation set.
Practice change
The AIMS65 is the simple, validated pre-endoscopic mortality-prediction score; it complements but does not replace the GBS for the triage.
ANZ practice note. The upper-GI bleed pathway in the ANZ departments follows the local protocol: the ABCDE, the large-bore access, the crossmatch, the Glasgow-Blatchford on the bloods, the restrictive transfusion to 70 to 80 g/L. The terlipressin (2 mg intravenously four times daily) and the ceftriaxone (2 g intravenously daily) are given early in the known or the suspected variceal bleed, before the endoscopy. The pantoprazole 80 mg intravenous bolus then 8 mg/h infusion is given for the non-variceal high-risk ulcer after the endoscopic haemostasis. The endoscopy is within 12 hours for the suspected variceal and within 24 hours for the non-variceal. The early-TIPSS is discussed for the high-risk cirrhotic within 72 hours of the index endoscopy. The Gastroenterological Society of Australia and the local hospital major-haemorrhage protocol govern the detail. [1]
SAQ — Suspected variceal haemorrhage in the cirrhotic patient
10 minutes · 10 marks
A 62-year-old man with known alcohol-related cirrhosis (Child-Pugh C) presents with massive haematemesis. BP 86/52, HR 122, RR 24, SpO2 95 per cent on room air, GCS 14, cool peripheries. He has a tense abdomen with ascites. Initial haemoglobin 72 g/L, platelets 60, INR 2.1, lactate 4.2.
SAQ — Peptic ulcer bleed with high-risk stigmata after endoscopy
10 minutes · 10 marks
A 68-year-old woman presents with melaena for 3 days. She takes ibuprofen 400 mg three times a day for osteoarthritis. BP 100/64, HR 108, haemoglobin 78 g/L, urea 18 mmol/L, creatinine 110 micromol/L. Endoscopy shows a duodenal ulcer with a non-bleeding visible vessel; adrenaline injection and dual thermal therapy achieve haemostasis.
Exam pearls
- The first decision is the variceal versus the non-variceal — it changes every drug you give on the arrival.
- The Glasgow-Blatchford 0 — the patient for the discharge or the outpatient endoscopy; the 7 or more — the high-intensity care. Reproduce the components: the urea, the haemoglobin, the systolic BP, the pulse, the melaena, the syncope, the hepatic disease, the cardiac failure.[1]
- The restrictive transfusion — 70 to 80 g/L. The over-transfusion rebleeds and, in the cirrhotic, kills.[2]
- The terlipressin and the ceftriaxone for the variceal — started before the endoscopy. The antibiotic reduces the mortality; do not wait for the endoscopy to give it.
- The pantoprazole 80 mg bolus then 8 mg/h infusion for the high-risk ulcer — after the endoscopic haemostasis, for 72 hours.
- The endoscopy within 12 hours for the suspected variceal, within 24 hours for the non-variceal.
- The TIPSS for the refractory variceal bleed and the early TIPSS for the high-risk cirrhotic (Child-Pugh 10 to 13).
- The aspirin is resumed within 7 days for the secondary cardiovascular prevention — the Sung trial.[4]
- The aortoenteric fistula in the prior aortic graft — the sentinel bleed, the CT angiography, not the normal endoscopy.
- The Sengstaken-Blakemore tube is the bridge, not the cure — protect the airway first.
- The Forrest classification guides the endoscopic therapy — the Ia (spurting) and the Ib (oozing) and the IIa (visible vessel) all need the combination therapy; the III (clean base) needs none.
- The Rockall score predicts the mortality; the Glasgow-Blatchford predicts the need for the intervention; the AIMS65 predicts the in-hospital death — know which score answers which question.[5][6]
- The adrenaline injection alone is the inadequate therapy — always combine with the clip or the thermal coagulation for the high-risk ulcer.
- The H. pylori is tested and treated in every peptic ulcer bleed — the eradication reduces the rebleeding from 20 per cent to under 5 per cent.
- The terlipressin is the splanchnic vasoconstrictor; the octreotide is the ANZ alternative; both lower the portal pressure and the HVPG.
- The early (pre-emptive) TIPSS within 72 hours for the Child-Pugh 10 to 13 cirrhotic — the García-Pagán trial showed the mortality reduction from 39 per cent to 14 per cent.[7]
- The haematochezia from the upper source is the danger sign — the torrential, rapid-transit bleed; the patient is usually shocked.
- The urea-to-creatinine ratio greater than 30:1 points to the upper source — the digested blood is the protein load converted to the urea.
- Never band a gastric fundal varix — use the N-butyl-cyanoacrylate tissue adhesive (the glue).
Model answer — the non-variceal peptic ulcer bleed
A 72-year-old man on the ibuprofen for the osteoarthritis and the aspirin 100 mg daily for the prior MI presents with the melaena and the postural dizziness, the SBP 105, the pulse 100, the Hb 92, the urea 12. ABCDE: two large-bore cannulae, the crossmatch 2 units, the venous gas (the lactate 2.8), the GBS at the bedside approximately 9 (the high-risk). Restrictive transfusion — the Hb is 92 so do NOT transfuse yet (the threshold is 70 to 80); give the crystalloid cautiously for the mild shock. Pantoprazole 80 mg IV bolus then 8 mg/h infusion started. Continue the aspirin — the secondary cardiovascular prevention (the Sung trial). Hold the ibuprofen. Book the OGD within 24 hours — the likely duodenal ulcer. At the endoscopy: the combination therapy (the adrenaline injection + the clip) for the high-risk stigmata; continue the PPI infusion for 72 hours. Test for the H. pylori and eradicate if positive. Discharge when the stable with the PPI and the aspirin, the outpatient H. pylori follow-up. [1]
Model answer — the variceal bleed on arrival
A 58-year-old man with the known alcohol-related cirrhosis presents with the haematemesis and the melaena, the systolic BP 88, the pulse 120, the GBS by the bedside around 14. ABCDE: protect the airway (the high-flow oxygen, the early-intubation decision for the encephalopathic), two large-bore cannulae, the crossmatch, the lactate, the catheter. Restrictive transfusion to 70 to 80 g/L — give one unit now for the shock, recheck. Terlipressin 2 mg intravenously four times daily and ceftriaxone 2 g intravenously daily started before the endoscopy. Correct the coagulopathy (the vitamin K, the fresh-frozen plasma). Book the urgent endoscopy within 12 hours for the band ligation. If the bleed fails the vasoactive drug and the band ligation, insert the Sengstaken-Blakemore tube as the bridge and the early TIPSS for the high-risk (Child-Pugh 10 to 13). Admit to the high-dependency or the intensive care. [1]
Red flags
[1]References
- [1]Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage Lancet, 2000.PMID 11073021
- [2]Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding N Engl J Med, 2013.PMID 23281973
- [3]García-Pagán JC, Reverter E, Albillos A, Bosch J. Acute variceal bleeding Semin Respir Crit Care Med, 2012.PMID 22447260
- [4]Sung JJ, Lau JY, Ching JY, et al. Continuation of low-dose aspirin therapy in peptic ulcer bleeding: a randomized trial Ann Intern Med, 2010.PMID 19949136
- [5]Rockall TA, Logan RFA, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage Gut, 1996.PMID 8675081
- [6]Saltzman JR, Tabak YP, Hyett BH, Sun X, Travis AC, Johannes RS. A simple risk score accurately predicts in-hospital mortality, length of stay, and cost in acute upper GI bleeding Gastrointest Endosc, 2011.PMID 21907980
- [7]García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding N Engl J Med, 2010.PMID 20573925
- [8]Lau JYW, Sung J, Hill C, Henderson C, Howden CW, Metz DC. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers N Engl J Med, 2000.PMID 10922420
- [9]Chávez-Tapia NC, Barrientos-Gutiérrez T, Téllez-Avila FI, Soares-Weiser K, Uribe M. Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding Cochrane Database Syst Rev, 2010.PMID 20824832