Paeds · acute-care-resuscitation-and-toxicology
Difficult paediatric airway and emergency front-of-neck access
Also known as Difficult paediatric airway · Paediatric difficult intubation · Cannot intubate cannot oxygenate in children · Emergency front-of-neck access · Paediatric surgical airway
Fellowship guide to the difficult paediatric airway and emergency front-of-neck access: why the child's airway is anatomically and physiologically unforgiving, how to anticipate and recognise difficulty, the recognise-oxygenate-escalate-rescue sequence from a best-attempt laryngoscopy through early help and supraglottic-airway rescue to the rare emergency front-of-neck access, and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the three-year-old with Pierre Robin sequence brought to the emergency department obtunded after a seizure, or the infant with bacterial tracheitis whose stridor has turned to silence. Either child can turn a routine intubation into a crisis within seconds, and the difference between a controlled airway and a cardiac arrest is whether you anticipated the difficulty, assembled the team and equipment, and rehearsed the rescue sequence before induction. That is the territory this page owns. [3] [4]
A difficult paediatric airway is any airway in a child that is hard to visualise, hard to intubate, or hard to oxygenate with standard technique — whether the difficulty was anticipated beforehand or only declared once you have tried and failed. The crucial practical split is between anticipated difficulty, where history or anatomy warn you in advance (a syndrome, a known hard airway, or an inflamed or injured upper airway), and unanticipated difficulty, the commoner form in children, where the problem only surfaces at laryngoscopy because bedside prediction is unreliable in the young. [1] [6]
Emergency front-of-neck access (eFONA) is the final rescue — a surgical airway through the front of the neck when you cannot intubate and cannot oxygenate by any other means. It is vanishingly rare in children, technically demanding, and the dominant teaching of every modern guideline is that the best eFONA is the one you never reach, by preventing the cannot-intubate-cannot-oxygenate state through early help and supraglottic-airway rescue. [1] [10]
Why this matters at fellowship level is that airway is the commonest resuscitation task a general paediatrician faces, children tolerate hypoxia poorly, and most airway disasters are preventable — they stem from failing to anticipate, from repeating a failing laryngoscopy until the airway is destroyed, or from delaying rescue. The skill being tested is reading the child, calling help early, and never letting a difficult airway become a cannot-oxygenate airway. [3] [4]
Classification
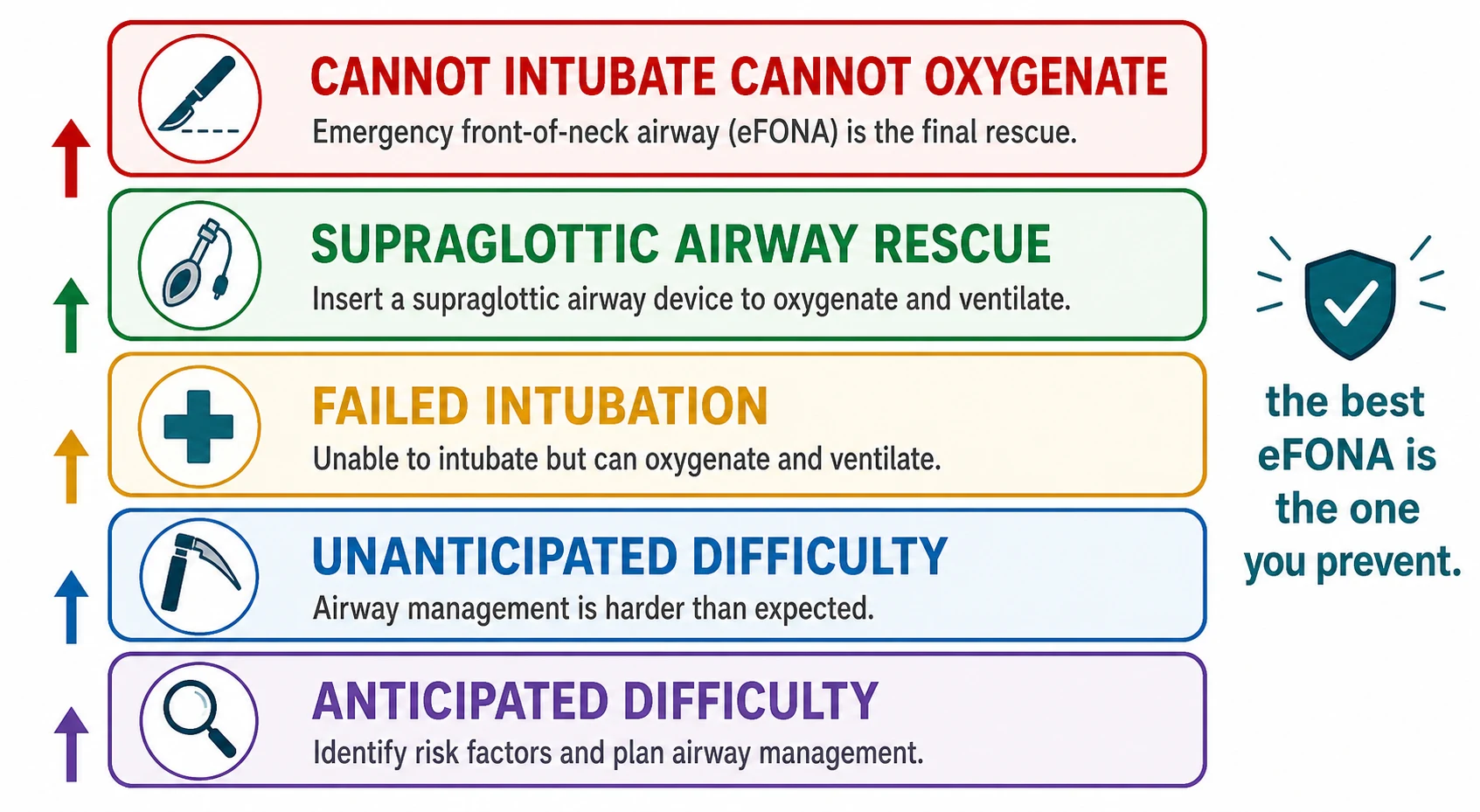
Sort the difficult airway by two axes at once: whether you saw the difficulty coming, and where the child sits on the failure ladder from a hard intubation through cannot-intubate to cannot-oxygenate, because that place drives the next move. [1] [3]
Anticipated difficulty covers the child you already know will be hard — a syndrome that distorts the airway, a documented previous difficult intubation, or an acutely inflamed, infected or injured upper airway such as epiglottitis, bacterial tracheitis, retropharyngeal abscess, burns, or facial trauma. Unanticipated difficulty is the child who looks normal but whose larynx you cannot see at laryngoscopy, and because no bedside score predicts this well in children, the whole team must be ready for it on every intubation. [1] [6]
The failure ladder is the spine of the algorithm. The child starts at difficult intubation — you cannot pass the tube easily. If laryngoscopy fails after a small number of best attempts you are at failed intubation, and the pivot is the supraglottic airway: if it oxygenates, you have time to wake an elective child or proceed with a resuscitation. If the supraglottic airway also fails to oxygenate you are in cannot-intubate-cannot-oxygenate, the peri-arrest state that demands immediate emergency front-of-neck access. [1] [10]
The numbers that anchor your viva
Epidemiology & Risk Factors
Difficult intubation is uncommon in otherwise normal children but rises steeply in the very young, the syndromic, and the acutely inflamed airway — exactly the groups that converge on the emergency department and the paediatric intensive care unit. [4] [6]
The strongest predictor is a history of previous difficult intubation, which is worth more than any bedside score, so always ask for it, read the anaesthetic chart, and document your own difficulty for the next team. The NECTARINE study across European centres confirmed that difficulty and complications cluster in neonates and infants, where the airway is smallest, the larynx highest, and the physiological reserve thinnest. [6] [3]
The syndromic and structural causes distort the upper airway or jaw and make the larynx impossible to expose: Pierre Robin sequence and other micrognathia, Treacher Collins and Goldenhar (craniofacial), mucopolysaccharidoses such as Hurler and Hunter (tissue infiltration), Down syndrome (large tongue, short neck), Beckwith-Wiedemann, and CHARGE association. Acquired risk is the inflamed or obstructed airway — epiglottitis, bacterial tracheitis, retropharyngeal abscess, peritonsillar abscess, burns, anaphylaxis, and foreign body. [3] [1]
Pathophysiology
The teaching model runs from the shape of the child's airway to the speed at which it fails, and it rests on anatomy that differs from the adult at every level and on physiology that gives you almost no time. [3] [6]
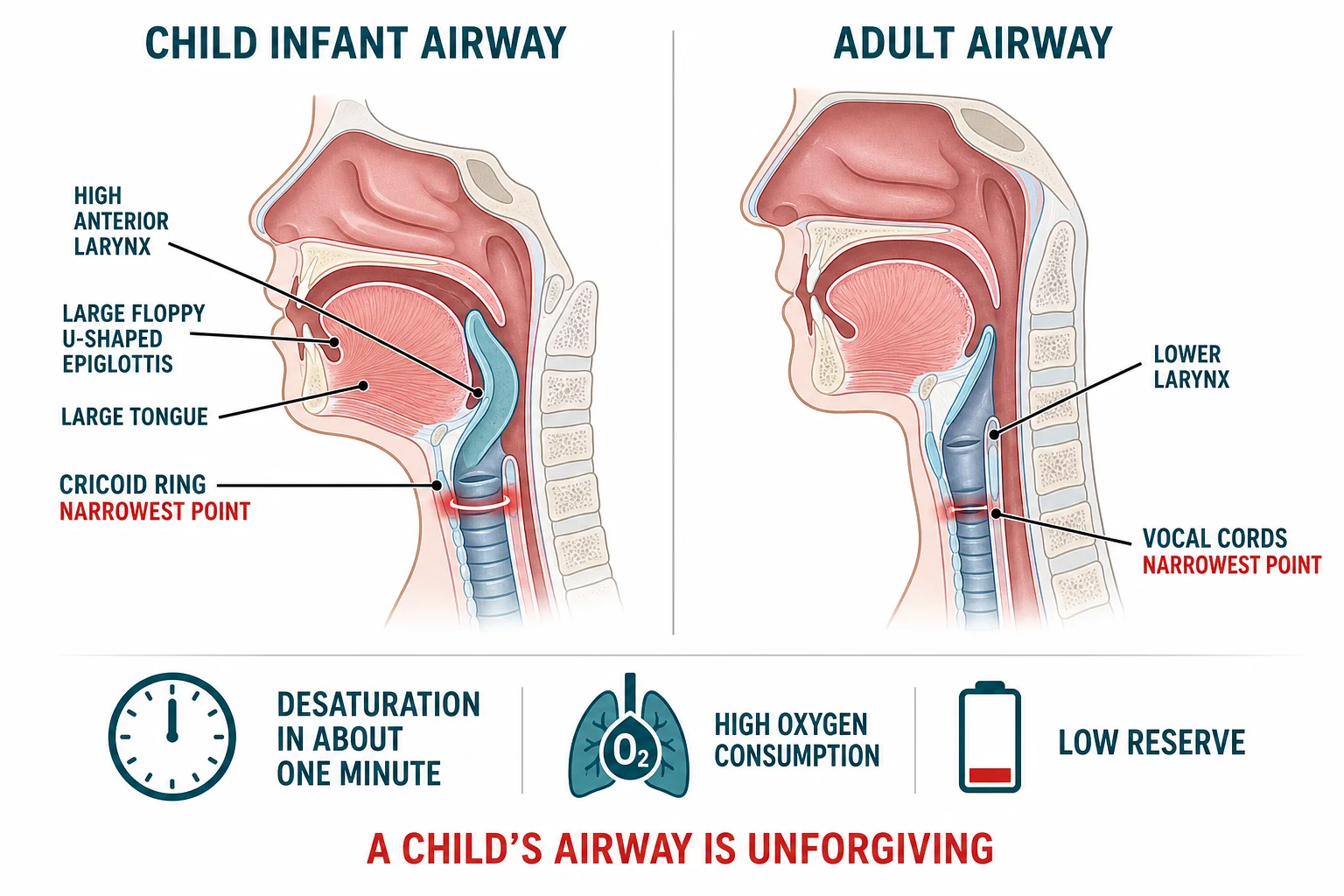
The infant is an obligate nose-breather with a large tongue that fills the small oral cavity, a relatively large occiput that flexes the neck when supine, and a large, floppy, U-shaped epiglottis that lies angled and anterior, so it folds into the view and must be lifted with the laryngoscope blade. The larynx is high and anterior — at the level of the third and fourth cervical vertebrae in the infant, descending to the sixth by adolescence — which is why the cords are hard to see and why the laryngeal inlet appears to "drop away" from you. [3] [6]
The single most testable anatomical fact is that the narrowest point of the child's airway is the cricoid cartilage, below the vocal cords, not the cords themselves as in the adult. The cricoid is the only complete ring in the trachea, so any circumferential swelling from repeated trauma, infection or a tight tube narrows it proportionally and can close it completely — a small millimetre change in a 4 mm airway is a large percentage obstruction. [3] [6]
A common misconception is that a difficult airway is mainly a problem of seeing the cords. In children the more dangerous problem is maintaining oxygenation between attempts, because the reserve is so thin that a prolonged laryngoscopy tips the child into bradycardia and hypoxia before you succeed — which is why limiting attempts and oxygenating constantly matter as much as the view itself. [4] [1]
Clinical Presentation
The classic presentation is the child who needs intubation and either telegraphs the difficulty from the history or hides it until induction. The single most useful early move is to decide, before you give any drug, whether this airway is anticipated-difficult, because that decision changes the team, the equipment and the plan. [3] [1]
Take a focused airway history and look at the child: previous difficult intubation; a syndrome or dysmorphism; snoring or sleep apnoea; recent upper-airway infection with stridor, drooling or a muffled voice; facial or neck trauma, burns or swelling; and any sign of obstruction — stertor, stridor, retractions or cyanosis. Each finding moves the airway from routine to anticipated-difficult and triggers a different preparation. [1] [3]
| Clue | What it suggests | Preparation |
|---|---|---|
| Syndrome or micrognathia | Distorted, high, anterior larynx; poor view | Senior airway help, videolaryngoscope, difficult-airway trolley ready |
| Previous difficult intubation | Recurrent difficulty is the strongest predictor | Read the chart, plan for rescue, have the supraglottic airway open |
| Stridor, drooling, tripoding | Inflamed or obstructed upper airway (epiglottitis, abscess) | Keep the child upright and calm; senior help; avoid upsetting before induction |
| Looks normal, no history | Unanticipated difficulty at laryngoscopy | Default readiness for rescue on every intubation |
The trap is the child who obstructs with sedation. A syndromic or partially obstructed child may maintain their airway awake but lose it the moment you induce, because the tone holding the soft tissues open is abolished — so an airway that seemed manageable becomes cannot-ventilate within seconds. This is why an anticipated-difficult airway is often managed with an awake, inhalational or carefully judged technique by an experienced operator, never by a junior giving a full rapid-sequence induction alone. [3] [1]
Differential Diagnosis
Frame the differential by why the airway is difficult, because the cause changes the preparation: the structurally distorted airway, the inflamed and obstructed airway, the foreign body, and the child who is simply physiologically fragile. The aim is to plan the right approach for each rather than treating every hard airway the same way. [3] [1]
Structural / syndromic
anticipated
- Pierre Robin, Treacher Collins, Goldenhar, mucopolysaccharidoses
- Micrognathia, high anterior larynx, poor view
- Plan senior help, videolaryngoscope, rescue ready
- Often known difficult from prior anaesthetics
Inflamed / infected
- Epiglottitis, bacterial tracheitis, retropharyngeal abscess
- Obstruction worsens with sedation or supine
- Keep upright and calm; senior ENT and anaesthetics
- Risk of complete obstruction on induction
Foreign body / trauma
- Sudden onset, choking, asymmetry
- Burns, facial and neck trauma, oedema
- May need rigid bronchoscopy, not intubation
- Distorted anatomy and bleeding
Physiologically fragile
- Septic or shocked infant, bronchospasm
- Desaturates and bradycardes on induction
- Oxygenation and haemodynamics drive the plan
- Avoid prolonged apnoea and deep sedation
The inflamed upper airway is the can't-miss category because induction can convert a partial obstruction into a complete one. A child with drooling, tripoding and stridor at rest may have epiglottitis or a retropharyngeal abscess, and the safe approach is to keep the child upright and calm, summon senior anaesthetic and ENT help, and often to perform an inhalational induction in a controlled setting rather than a rapid-sequence induction that abolishes airway tone. [1] [3]
A foreign body or trauma to the airway can mimic and complicate difficulty: a lodged foreign body may need rigid bronchoscopy rather than intubation, and facial or neck burns and trauma distort anatomy and bleed, so the team, the equipment and the surgical backup must be assembled before you induce. [3] [4]
Clinical & Bedside Assessment
Assessment is rapid, structured and continuous: decide anticipated versus unanticipated, prepare the child and the team, give one optimised attempt, and reassess oxygenation and heart rate after every single manoeuvre. The aim is never to be surprised, and never to repeat a failing action. [1] [4]
Objective monitoring supports but never replaces the clinical picture. Continuous pulse oximetry and heart-rate monitoring are mandatory because the infant's first response to hypoxia and airway stimulation is bradycardia — a slowing heart rate during instrumentation is a stop signal, not a nuisance. Assess mask ventilation early, because a child you can bag-mask-ventilate is a child you have time for, and a supraglottic airway that ventilates is your bridge to help. [3] [4]
Placing the child on the rescue ladder
Supraglottic airway rescues
Oxygenates — wake an elective child or proceed
Deliberately avoid what destroys the airway: do not repeat direct laryngoscopy beyond a small number of best attempts, because each pass traumatises tissue and swells the cricoid; do not induce an anticipated-difficult child alone without help or rescue equipment open; and do not let a child desaturate silently between attempts — oxygenate constantly. A child who is bradycardic or cyanosing is a child you stop and rescue, not one you push for a better view. [3] [1]
Investigations
The difficult airway is managed clinically and the priority is oxygenation, not investigation, because no test helps you in the moment the airway fails. Investigations are adjuncts that shape preparation in the anticipated-difficult child, never a reason to delay securing a threatened airway. [1] [4]
In a child with an acutely obstructed upper airway, keep them calm and upright and do not send them unescorted to imaging, lie them flat for a radiograph, or examine the throat with a tongue depressor — each can precipitate complete obstruction. Imaging such as a lateral neck radiograph or, when stable, a contrast study is reserved for the child who is safely oxygenating, to characterise a retropharyngeal abscess or foreign body before a controlled trip to theatre. [3] [1]
The most important "investigation" is the previous anaesthetic chart, because a documented difficult intubation is the single best predictor of future difficulty; read it, act on it, and after any difficult airway document the grade, the devices that worked and the plan for the next team so the knowledge is never lost. [3] [1]
Management — Resuscitation
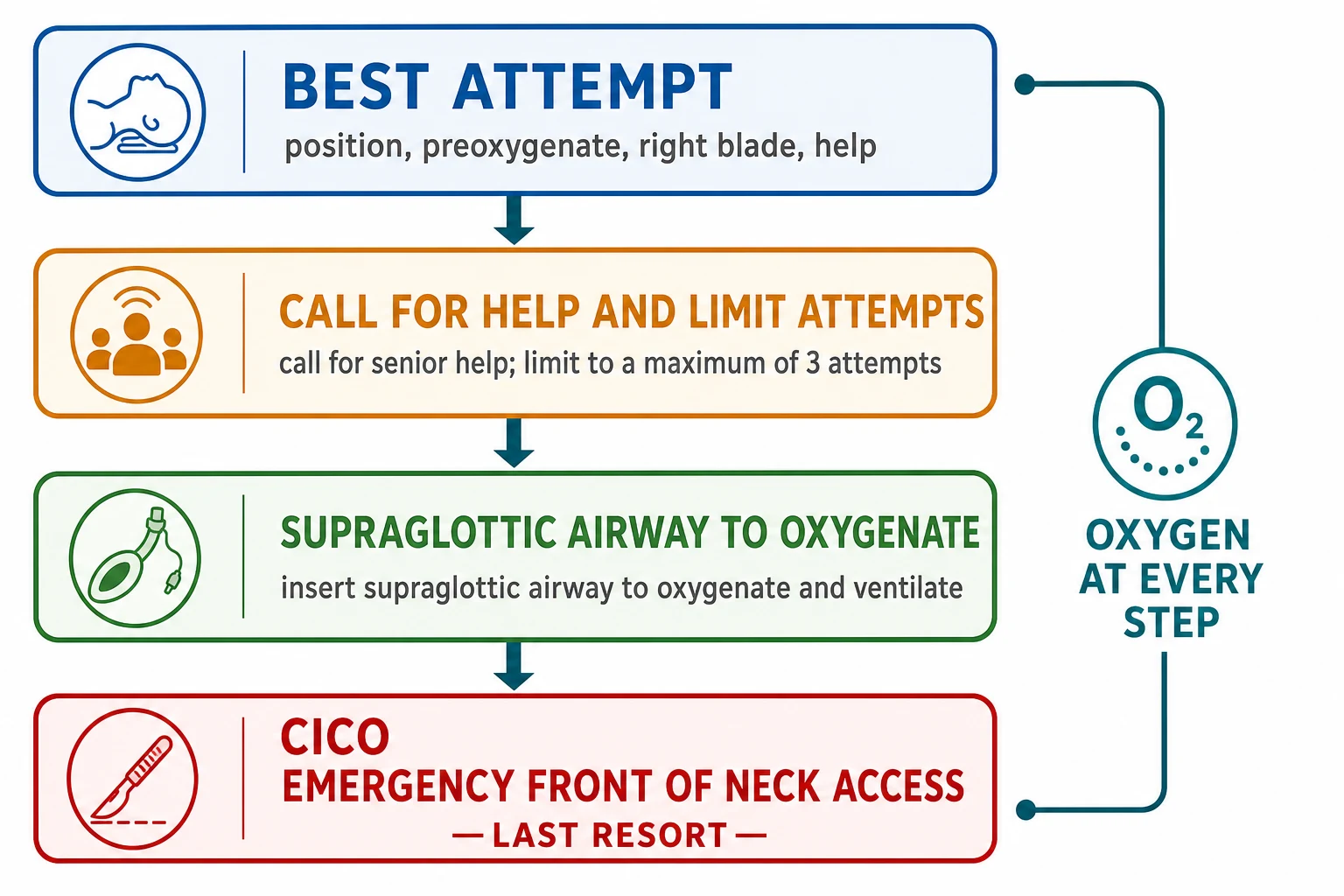
Resuscitation of the difficult airway is the recognise-oxygenate-escalate-rescue sequence applied without pause: position and preoxygenate, give one best laryngoscopy, call for help at the first failure, oxygenate with a supraglottic airway, and prepare for emergency front-of-neck access only if all else fails. The guiding rule is to keep oxygen on at every step and never let a difficult airway become a cannot-oxygenate airway. [1] [3]
Position the child in the sniffing position, adjusted for age — the infant's large occiput already places the head correctly and may need a shoulder roll rather than head tilt, while the older child needs head extension on a pillow. Preoxygenate with high-flow oxygen for as long as the child tolerates, accepting that even good preoxygenation gives only a minute or so in an infant. Assemble the team, the difficult-airway trolley, the correctly sized supraglottic airway and suction before any drug is given. [3] [1]
Airway resuscitation drugs (confirm against local protocol and patient weight)
If intubation fails, call for help immediately — the most senior anaesthetist, ENT surgeon and, in many centres, a colleague who can perform a surgical airway. Do not repeat the same direct laryngoscopy more than a small number of times; switch to the rescue sequence. The supraglottic airway is the pivotal device: if it oxygenates the child you have bought time to wake an elective case or proceed with a resuscitation, and it can serve as a conduit for intubation by an experienced operator. [1] [10]
If the supraglottic airway also fails to oxygenate and you cannot intubate, you are in cannot-intubate-cannot-oxygenate: declare it, and perform emergency front-of-neck access without delay while preparing for cardiac arrest, because the child has no further reserve. [1] [10]
Management — Definitive & Stepwise
The definitive plan is the algorithm itself — a disciplined climb up the rescue ladder where each step is given its best chance and abandoned the moment it fails. The structure is shared across the Difficult Airway Society and Association of Paediatric Anaesthetists guidance and the international consensus: optimise, rescue with a supraglottic airway, and reserve eFONA for cannot-intubate-cannot-oxygenate. [1] [5]
The first step is the optimised best attempt: correct position, full preoxygenation, the right blade, external laryngeal manipulation, a skilled assistant to pull the tube and handle the bougie, and — where available and the operator is familiar — a videolaryngoscope, which improves the view in children who are difficult to intubate. The paediatric difficult intubation registry analysis showed that GlideScope videolaryngoscopy gave a better glottic view than direct laryngoscopy in children who were difficult to intubate, though success still depends on operator experience and tube delivery. [7] [1]
The rescue ladder in order
Position, preoxygenate, assemble team, difficult-airway trolley and supraglottic airway open.
Give one optimised best-attempt laryngoscopy with the right blade and external laryngeal manipulation.
If the view fails, call for the most senior airway help now; do not repeat more than a small number of best attempts.
Insert a supraglottic airway to oxygenate; if it works, wake an elective child or proceed with the resuscitation.
If the supraglottic airway fails too, declare cannot-intubate-cannot-oxygenate and perform emergency front-of-neck access.
Supraglottic-airway rescue is the hinge of the whole algorithm, because a child you can oxygenate is a child you have time for. The device buys the minutes needed for senior help to arrive, for an elective child to wake, or for an experienced operator to intubate through the supraglottic airway with a fibrescope or exchange technique. The emphasis on the supraglottic airway over repeated laryngoscopy is the single behavioural change that prevents most airway deaths. [1] [4]
O-B-H-S-F
Emergency front-of-neck access is the last rung and is technically demanding in children because the cricothyroid membrane is small, soft and hard to identify, and the cartilage is pliable. The widely taught technique is the scalpel-bougie method, in which a transverse stab is made through the cricothyroid membrane, the scalpel is rotated to open the tract, a bougie is passed, and a cuffed tube is railroaded over it. Recent work on simulation models and institutional protocols stresses that the rarity and difficulty of paediatric eFONA make rehearsal, team preparation and a written local protocol essential. [9] [10]
The dominant teaching, echoed across guidelines, is that the best emergency front-of-neck access in a child is the one you prevent — by anticipating difficulty, giving a single best attempt, calling help early, and using the supraglottic airway before the child reaches cannot-oxygenate. [1] [8]
Specific Subtypes & Scenarios
The syndromic, anticipated-difficult child needs a planned approach, not a routine induction. Assemble senior anaesthetic and ENT help, the difficult-airway trolley, a videolaryngoscope and an open supraglottic airway, and consider an awake, inhalational or carefully judged technique by an experienced operator — because abolishing airway tone in a child with micrognathia or tissue infiltration can convert a difficult airway into a cannot-ventilate airway within seconds. [3] [1]
The acutely obstructed upper airway — epiglottitis, bacterial tracheitis, or a retropharyngeal abscess — is managed by keeping the child upright and calm, summoning the senior team to the bedside, and usually performing a controlled inhalational induction in theatre with a surgeon scrubbed, rather than a rapid-sequence induction that removes the tone holding the airway open. Upsetting the child, lying them flat, or instrumenting the throat can precipitate complete obstruction. [1] [3]
Disma 2021 — British Journal of Anaesthesia (NECTARINE; PMID 33812665)
A prospective European multicentre observational study of anaesthesia practice in neonates and infants across many centres
Key finding
Difficult intubation and airway complications were concentrated in the youngest infants, confirming that the smallest and youngest children carry the highest airway risk and that difficulty is often unanticipated.
Practice change
Anticipate difficulty especially in neonates and infants, prepare rescue equipment for every paediatric intubation, and document difficulty for the next team.
The child who reaches cannot-intubate-cannot-oxygenate is the peri-arrest scenario. Declare it, perform emergency front-of-neck access with the scalpel-bougie technique without delay, and run the resuscitation in parallel, because the child has crossed into the state where only a surgical airway restores oxygenation. The rarity of this event in children is exactly why it must be rehearsed and supported by a written institutional protocol. [10] [9]
The remote or retrieval scenario is a common exam vignette: a difficult airway a long way from a skilled team. The priorities are to anticipate the high-risk child, call for retrieval early, optimise oxygenation and the first attempt with the best available operator and equipment, and avoid inducing an anticipated-difficult airway alone — because the nearest surgical airway help may be hours away. [4] [1]
Complications & Pitfalls
The complications of a difficult airway and its management are direct: airway trauma and swelling, hypoxia, bradycardia and cardiac arrest, aspiration, oesophageal intubation, and — when ventilation fails — hypoxic brain injury or death. Each repeated laryngoscopy adds oedema to the cricoid and narrows an already small airway. [1] [6]
The dominant pitfall is repeating a failing laryngoscopy. The temptation to have "just one more look" is what turns a difficult airway into an impossible one, because each attempt traumatises and swells the tissues until the laryngeal inlet and the cricoid close. The antidote is discipline: a small, fixed number of best attempts, then rescue. [3] [1]
[1]Other avoidable errors include inducing an anticipated-difficult child alone without help or rescue equipment, failing to preoxygenate or to keep oxygen on between attempts, ignoring bradycardia and falling saturation as stop signals, and delaying the declaration of cannot-intubate-cannot-oxygenate until the child arrests. Each is a behavioural failure rather than a knowledge gap, and each is preventable by rehearsing the algorithm. [1] [3]
Prognosis & Disposition
The prognosis of a well-managed difficult airway is good: with anticipation, a single best attempt, early help and supraglottic-airway rescue, most difficult paediatric airways are secured without lasting harm, and the catastrophic outcomes cluster in the children who reached cannot-oxygenate through avoidable delay. [1] [4]
Disposition follows the airway and the child. A child whose airway is secured and stable goes to an appropriate monitored environment — paediatric intensive care for the critically ill or post-arrest child, a high-dependency setting for the fragile airway, and theatre or recovery for the elective case rescued and woken. The retrieval service is engaged early for the difficult airway in a remote setting. [4] [1]
After any difficult airway, document and communicate what happened: the view, the devices that worked and failed, the drugs, and an explicit plan for the next anaesthetist, because a future team will rely on it. Reassess the child for airway oedema, aspiration and the haemodynamic consequences of the event, and arrange the right level of monitoring for the recovery. [3] [1]
Special Populations
Neonates and infants are the highest-risk group because the airway is smallest, the larynx highest, the reserve thinnest, and difficulty and complications concentrate here — so treat every neonatal and infant intubation as one where rescue equipment must be ready and where an experienced operator gives the best attempt. [6] [3]
Children with complex, technology-dependent disease and syndromic airways face recurrent airway encounters — tracheostomy, repeated anaesthetics, and progressive airway changes — so maintain a detailed airway record, rehearse the plan, and engage the specialist airway team early for each event. [3] [4]
Children in remote, rural and under-resourced settings face the same difficult airway with a thinner safety net: less access to senior airway help, videolaryngoscopy, ENT surgery and retrieval. The equity response is to anticipate the high-risk child, train and equip the local team to the best-attempt-and-supraglottic-rescue level, and arrange retrieval before the airway collapses rather than after. [4] [1]
The child with disability or neurodiversity may be unable to cooperate with awake or inhalational techniques, compounding difficulty; a planned, calm approach with carer presence, suitable sedation where safe, and a prepared team reduces the risk of a distressed child obstructing a difficult airway. [3] [4]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Rescue emphasis | eFONA emphasis |
|---|---|---|---|
| ANZ | APLS; RCH Melbourne CPGs; DAS/APA algorithm | Early senior help, supraglottic airway as pivotal rescue | Scalpel-bougie; prevention through early rescue |
| UK | Difficult Airway Society / APA paediatric guideline | Limited best attempts, supraglottic airway, defined CICO step | Scalpel-bougie technique; rehearsed and protocolised |
| North America | ASA difficult airway guideline; SPA PeDI registry evidence | Videolaryngoscopy where available; supraglottic airway rescue | Institutional protocol; team rehearsal |
| Low-resource | WHO-aligned and APLS-adapted approaches | Best-attempt and supraglottic rescue with available kit | Early retrieval; prevention is the realistic goal |
The evidence backbone you should name begins with the Difficult Airway Society and Association of Paediatric Anaesthetists paediatric guideline, which defines the unanticipated difficult intubation algorithm around best attempts, supraglottic-airway rescue and a front-of-neck access step. The ASA difficult airway practice guidelines frame the broader difficult-airway principles, and the paediatric difficult intubation registry analysis showed videolaryngoscopy improves the view in children who are difficult to intubate. [1] [2] [7]
The NECTARINE study anchors the epidemiology — difficulty and complications cluster in neonates and infants — and the Society for Pediatric Anesthesia consensus on airway management during COVID-19 reinforced the same core principles of planning, help and rescue. Recent work on infant front-of-neck-access simulation models and institutional eFONA protocols confronts how rarely the technique is used in children and why rehearsal and written protocols matter. [6] [5] [9] [10]
The live areas of nuance are the exact number of best attempts before rescue, the role of routine videolaryngoscopy versus direct laryngoscopy, and the optimal eFONA technique and equipment for infants — areas where evidence is thin and the emphasis is on team preparation, simulation and a written local protocol. [8] [10]
Exam Pearls
The single discipline that keeps children alive is to never let a difficult airway become a cannot-oxygenate airway — by anticipating, giving one best attempt, calling help early, and rescuing with the supraglottic airway before the child reaches the front-of-neck step. [1] [4]
When you teach the paediatric airway, teach the unforgiving physiology as loudly as the algorithm — the child who desaturates in a minute, the cricoid that swells with every attempt, the bradycardia that says stop — because disasters come not from a lack of devices but from failing to respect how little reserve the child has. [3] [6]
References
- [1]Black AE, Flynn PE, Smith HL, et al. Development of a guideline for the management of the unanticipated difficult airway in pediatric practice. Paediatr Anaesth, 2015.PMID 25684039
- [2]Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology, 2013.PMID 23364566
- [3]Engelhardt T, Weiss M. A child with a difficult airway: what do I do next? Curr Opin Anaesthesiol, 2012.PMID 22499162
- [4]Hsu G, Nishisaki A. Pediatric airway management. Curr Opin Anaesthesiol, 2021.PMID 33935175
- [5]Matava CT, Kovatsis PG, Lee KA, et al. Pediatric Airway Management in COVID-19 Patients: Consensus Guidelines From the Society for Pediatric Anesthesia's Pediatric Difficult Intubation Collaborative and the Canadian Pediatric Anesthesia Society. Anesth Analg, 2020.PMID 32287142
- [6]Disma N, Tassone E, Parrin M, et al. Difficult tracheal intubation in neonates and infants. NEonate and Children audiT of Anaesthesia pRactice IN Europe (NECTARINE): a prospective European multicentre observational study. Br J Anaesth, 2021.PMID 33812665
- [7]Park R, Zanaty M, Vogelheim C, et al. The efficacy of GlideScope videolaryngoscopy compared with direct laryngoscopy in children who are difficult to intubate: an analysis from the paediatric difficult intubation registry. Br J Anaesth, 2017.PMID 29028952
- [8]Garcia-Marcinkiewicz AG. The future of pediatric airway management. Curr Opin Anaesthesiol, 2026.PMID 42013372
- [9]Flynn A, Wood S, Gray A, et al. A high-fidelity non-animal model for simulation of infant emergency front-of-neck access. Br J Anaesth, 2025.PMID 39694755
- [10]Tsuboi K, Nishiyama K, Hayashi M, et al. Emergency Front-Of-Neck Access in the Pediatric Intensive Care Unit: Development of an Institutional Protocol. Paediatr Anaesth, 2026.PMID 41195791