Paeds · adolescent-and-young-adult-medicine
Polycystic ovary syndrome in adolescents
Also known as PCOS · Polycystic ovarian syndrome · Stein-Leventhal syndrome · Hyperandrogenic anovulation · Adolescent PCOS · Functional ovarian hyperandrogenism
A fellowship approach to PCOS in adolescents: Rotterdam-based diagnosis modified for developmental physiology, exclusion of mimics, lifestyle-first management with symptom-directed pharmacotherapy, metabolic and mental health screening, and long-term partnership.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 16-year-old presents with irregular periods, acne, and weight gain. Her mother has type 2 diabetes. An ultrasound reports "polycystic ovaries" and the referring GP has already told the family she has PCOS. Your job is not to rubber-stamp the label but to determine whether this is true PCOS or normal adolescent physiology plus a common ultrasound finding. [2] [5]
Polycystic ovary syndrome is a heterogeneous endocrine disorder characterised by ovulatory dysfunction, hyperandrogenism, and polycystic ovarian morphology. The 2003 Rotterdam consensus established the most widely used diagnostic framework, requiring two of three criteria after other causes are excluded. In adolescents, that framework needs developmental modification because irregular cycles and multifollicular ovaries are physiologically normal in the first years after menarche. [4] [2]
The 2025 international adolescent-specific recommendations from Pena and colleagues bring the most current evidence to the adolescent diagnostic and management conversation, addressing why adult criteria cannot be transplanted unchanged into adolescent care. The condition carries reproductive, metabolic, and psychological consequences that span decades, making early accurate diagnosis and longitudinal management an investment in lifelong health. [1] [6]
Classification
The classification of PCOS in adolescents begins with understanding why multiple diagnostic frameworks exist and how adolescent physiology reshapes each one. [4] [2]
Diagnostic frameworks
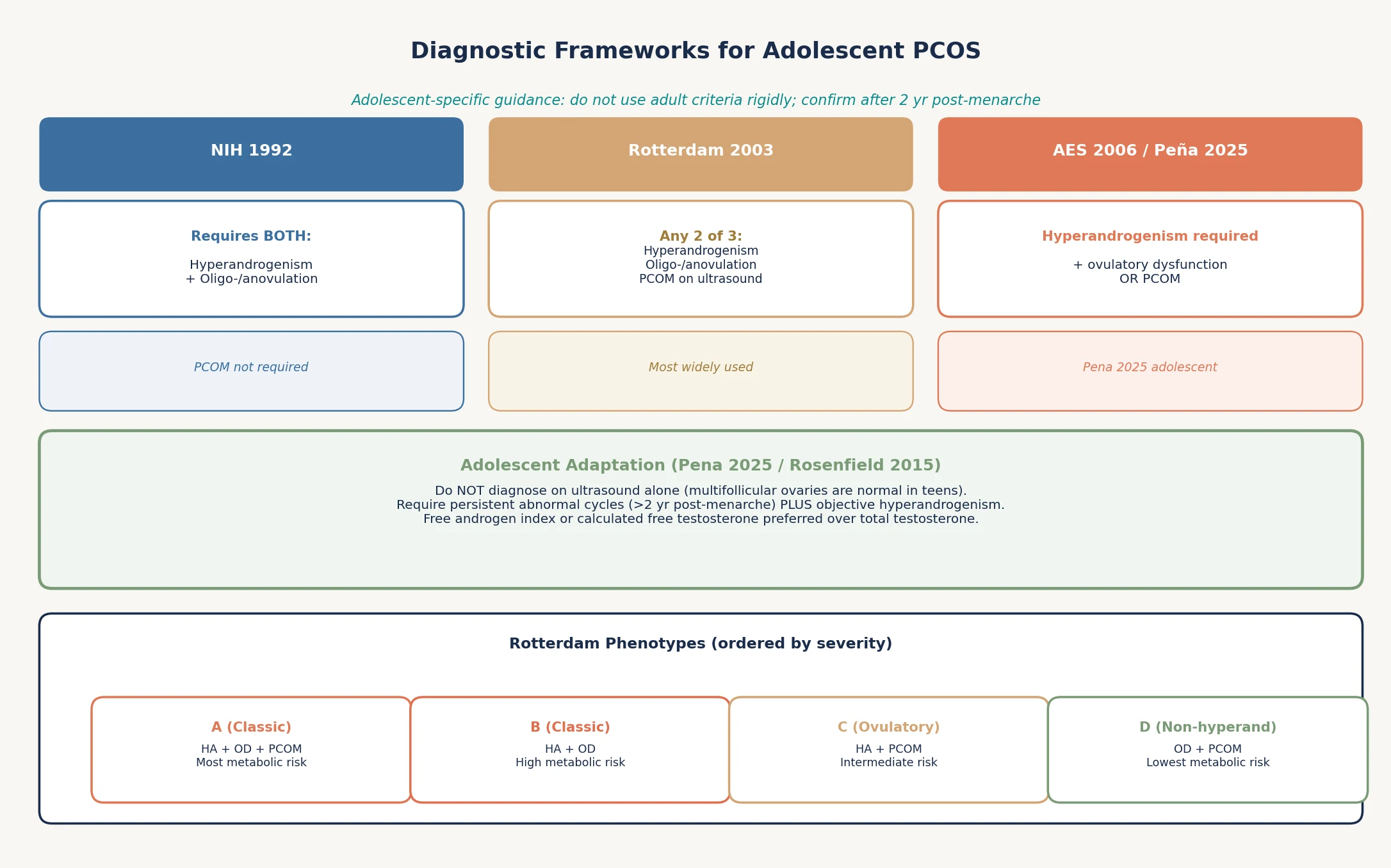
The NIH 1992 criteria require both hyperandrogenism and oligo-anovulation; ultrasound morphology is not needed. The Rotterdam 2003 consensus broadens diagnosis to any two of three features: hyperandrogenism, ovulatory dysfunction, or polycystic ovarian morphology. The Androgen Excess Society (AES) 2006 framework requires hyperandrogenism as mandatory, plus either ovulatory dysfunction or PCOM. The 2025 Pena adolescent recommendations endorse a modified Rotterdam approach with explicit cautions against ultrasound-based diagnosis in this age group. [4] [1] [6]
Rotterdam phenotypes
Once diagnosed, PCOS can be classified into four phenotypes by which criteria are present. Phenotype A (all three features) and B (hyperandrogenism plus ovulatory dysfunction) carry the highest metabolic risk. Phenotype C (hyperandrogenism plus PCOM) has intermediate risk, and phenotype D (ovulatory dysfunction plus PCOM without hyperandrogenism) carries the lowest metabolic burden. Phenotype assignment guides surveillance intensity. [4] [11]
Adolescent-specific caution
Normal adolescent physiology includes irregular cycles for up to two years post-menarche as the hypothalamic-pituitary-ovarian axis matures. Multifollicular ovaries are common in this period. The adolescent-specific framework therefore demands persistence of symptoms beyond the perimenarchal window and the presence of objective hyperandrogenism before applying the PCOS label. Rosenfield and colleagues articulated this principle clearly in their 2015 Pediatrics statement, which remains a cornerstone of adolescent PCOS reasoning. [2] [1]
NIH 1992
Hyperandrogenism + anovulation
- Both features required
- PCOM not part of criteria
- Identifies classic PCOS
- High metabolic risk phenotype
Rotterdam 2003
Two of three criteria
- Most widely used globally
- Broadens the diagnosis
- Four phenotypes possible
- Adolescent modification essential
AES 2006 / Pena 2025
Hyperandrogenism required
- Hyperandrogenism mandatory
- Plus ovulatory dysfunction or PCOM
- Aligns with adolescent guidance
- Pena 2025 cautions ultrasound in teens
Epidemiology & Risk Factors
PCOS is the most common endocrine disorder in reproductive-age women, with community prevalence estimates ranging from 8% to 13% depending on diagnostic criteria and population studied. March and colleagues found prevalence varied dramatically under contrasting diagnostic frameworks, highlighting how the choice of criteria changes who gets labelled. [9] [10]
In adolescents, prevalence is harder to pin down because of the physiological overlap with normal pubertal development. Risk factors include obesity, family history of PCOS or type 2 diabetes, low birth weight followed by rapid postnatal catch-up growth, and premature adrenarche. Indigenous, South Asian, and Middle Eastern populations show higher prevalence and metabolic severity, making PCOS a condition where cultural and ethnic context modifies both presentation and management priorities. [10] [9]
The metabolic risk burden is substantial. Dokras and colleagues demonstrated that metabolic syndrome prevalence in women with PCOS far exceeds background rates, and this risk tracks with obesity and phenotype severity. Insulin resistance is present in 60–80% of women with PCOS regardless of body weight, creating a self-reinforcing loop of hyperinsulinaemia and ovarian androgen production that accelerates over time if unaddressed. [11] [3]
Pathophysiology
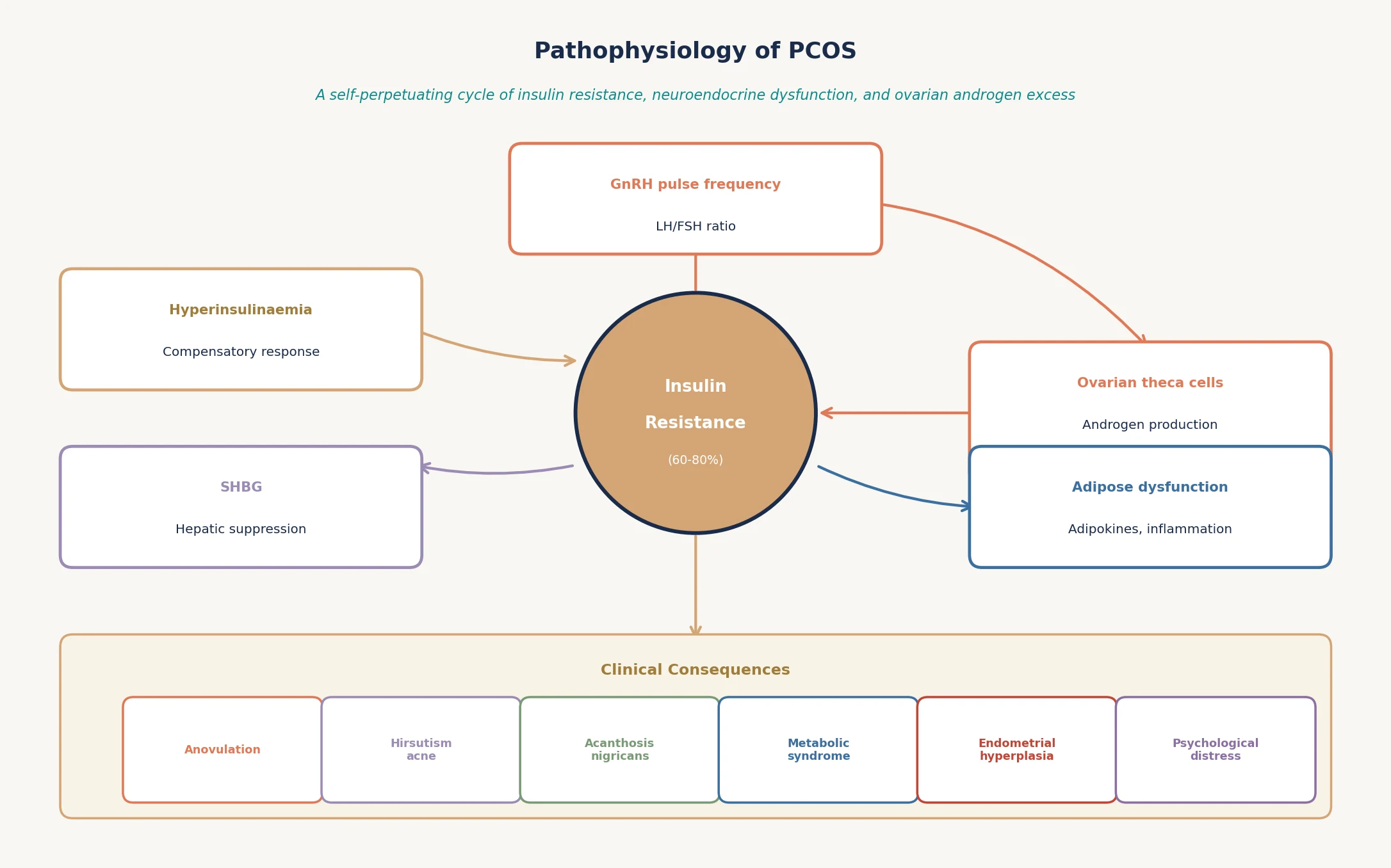
The pathophysiology of PCOS is a self-perpetuating cycle linking insulin resistance, neuroendocrine dysfunction, and ovarian androgen excess. Understanding the mechanism explains why a single treatment rarely addresses all features. [3] [5]
Insulin resistance is the central metabolic driver in most cases. Compensatory hyperinsulinaemia acts directly on ovarian theca cells to stimulate androgen production and suppress hepatic sex hormone-binding globulin synthesis. Lower SHBG increases the fraction of free, bioactive testosterone, amplifying the clinical hyperandrogenic signal even when total testosterone is only mildly elevated. [3] [5]
At the neuroendocrine level, increased gonadotropin-releasing hormone pulse frequency raises luteinising hormone relative to follicle-stimulating hormone. This elevated LH/FSH ratio promotes theca cell androgen production while relatively under-stimulating follicular maturation, contributing to anovulation and the polycystic ovarian morphology. Adipose tissue dysfunction adds inflammatory adipokines that worsen insulin resistance, completing the vicious cycle. [5] [3]
The genetic architecture is polygenic with significant heritability. First-degree relatives of women with PCOS have higher rates of hyperandrogenism and insulin resistance, and genome-wide association studies have identified loci involved in gonadotropin signalling and insulin action. Intrauterine exposures, including hyperandrogenaemia and hyperinsulinaemia, may programme fetal ovarian and metabolic development. [5] [6]
Clinical Presentation
A 15-year-old presents to her GP with acne that has not responded to topical treatments. Her periods started at 12 and are irregular, sometimes skipping two or three months. She has gained 8 kg over the past year. Her mother is concerned about facial hair. This is the classic PCOS presentation in adolescents: a cluster of common complaints that individually are common but together form a recognisable pattern. [2] [5]
The presentation is heterogeneous. Some adolescents present primarily with menstrual irregularity — oligomenorrhoea, amenorrhoea, or unpredictable bleeding. Others present with dermatological concerns: hirsutism (excess terminal hair in androgen-dependent areas), severe or treatment-resistant acne, or acanthosis nigricans. Weight gain and difficulty losing weight are frequent presenting complaints, and the obesity-PCOS association is bidirectional. [2] [5]
Psychological symptoms are under-recognised but central to the adolescent experience. Barry and colleagues showed in their meta-analysis that anxiety and depression rates in PCOS are markedly higher than in controls. Quality-of-life studies in adolescents with PCOS confirm significant impairment across body image, emotional, and social domains. The adolescent may present with mood symptoms, eating concerns, or body image distress before mentioning any menstrual or dermatological problem. [12] [14]
The physical examination findings to actively look for include hirsutism (scored using the modified Ferriman-Gallwey system), acne distribution and severity, acanthosis nigricans in the neck folds and axillae, central adiposity, and blood pressure. Signs that suggest an alternative diagnosis include clitoromegaly, deepening voice, temporal balding, or Cushingoid features — these are red flags for androgen-secreting tumours or Cushing syndrome rather than PCOS. [2] [3]
Differential Diagnosis
The differential diagnosis for adolescent PCOS centres on conditions that mimic one or more Rotterdam criteria. The exclusion of mimics is not optional — it is part of the diagnostic process itself. [3] [2]
PCOS mimics in the adolescent
Non-classic congenital adrenal hyperplasia due to 21-hydroxylase deficiency is the most important mimic to exclude because it requires different management. A basal 17-hydroxyprogesterone level screens for this; values above the assay-specific threshold prompt ACTH stimulation testing. Thyroid dysfunction and hyperprolactinaemia are common, easily tested, and reversible causes of menstrual irregularity. [3] [6]
Androgen-secreting tumours are rare but must not be missed. The red flags are rapid onset of severe virilisation (clitoromegaly, voice deepening, temporal balding), very high androgen levels (total testosterone above 5–6 nmol/L or DHEAS above 700 micrograms/dL), and a palpable adrenal or ovarian mass on imaging. Cushing syndrome enters the differential when the presentation includes central obesity, purple striae, proximal myopathy, or hypertension. [2] [3]
Clinical & Bedside Assessment
The clinical assessment of a suspected adolescent PCOS case has three layers: a careful menstrual history, a targeted examination for hyperandrogenism and metabolic risk, and a structured approach to what to measure and what to defer. [2] [1]
Menstrual history
Ask about age at menarche, cycle length and variability, bleeding pattern, and duration of irregularity. Cycles shorter than 21 days or longer than 35 days, fewer than eight cycles per year, or amenorrhoea beyond 90 days after two years post-menarche are abnormal. Document the timeline precisely because persistence is the key adolescent diagnostic principle. A menstrual calendar or app history adds objectivity. [2] [5]
Examination
Score hirsutism using the modified Ferriman-Gallwey scale (a score of 4–6 depending on ethnicity is the common threshold, with lower cut-offs for East Asian populations). Examine for acne severity and distribution, acanthosis nigricans in the posterior neck and axillae, central adiposity (waist circumference), blood pressure, and any signs of virilisation. Measure height, weight, and BMI, and plot on appropriate charts. [2] [3]
Confidential and psychosocial elements
Conduct the sensitive parts of the assessment in private. Ask about body image distress, disordered eating, mood, and sexual health. The adolescent PCOS population has elevated rates of anxiety, depression, and eating disorders, and these are often undisclosed if the parent is present. Frame the conversation around health and function, not appearance. [12] [14]
Investigations
The investigation strategy for adolescent PCOS serves two purposes: confirming the diagnosis by documenting hyperandrogenism and excluding mimics, and screening for metabolic comorbidity that guides management. [3] [1]
Diagnostic bloods
Measure total and calculated free testosterone (or free androgen index) to document biochemical hyperandrogenism. AMH has been investigated as a diagnostic biomarker but the 2024 systematic review by van der Ham and colleagues found insufficient accuracy to replace standard criteria in adolescents. Screen for mimics with TSH, prolactin, and 17-hydroxyprogesterone. Consider DHEAS and androstenedione if androgen excess is severe or atypical. [15] [3]
Metabolic screening
Check fasting glucose and HbA1c, with an oral glucose tolerance test if BMI is elevated or risk factors are present. Request a fasting lipid panel. Consider liver function tests and an ALT to screen for non-alcoholic fatty liver disease, which Liu and colleagues linked to PCOS through genetic evidence of a hepato-ovarian axis. Baseline insulin or HOMA-IR can be useful but is not universally required. [11] [17]
Ultrasound — when and why
Pelvic ultrasound should not be the primary diagnostic tool in adolescents. Multifollicular ovaries are normal in this age group, and the transabdominal route commonly used in adolescents limits sensitivity. If performed, report follicle count and ovarian volume using the 2018 international threshold of 20 or more follicles per ovary or ovarian volume above 10 mL. An ultrasound that shows PCOM adds supportive evidence but does not diagnose PCOS in isolation. [1] [2] [15]
Investigation pathway for suspected adolescent PCOS
Document history
Menstrual pattern >2 yr post-menarche; hirsutism timeline; weight trajectory; family history.
Confirm hyperandrogenism
Total + free testosterone or free androgen index; consider SHBG.
Exclude mimics
TSH, prolactin, 17-hydroxyprogesterone; DHEAS if severe.
Metabolic screen
Fasting glucose, HbA1c, lipids, ALT; OGTT if obese or risk factors.
Ultrasound (selective)
Not diagnostic alone; transvaginal if sexually active and acceptable.
Mental health screen
PHQ-9 or equivalent; body image and eating risk assessment.
Management — Resuscitation
PCOS in adolescents is a routine, non-emergency condition. There is no resuscitation phase in the traditional sense. However, two acute clinical scenarios require urgent action. [1] [3]
First, severe mental health deterioration — active suicidal ideation or a recent attempt — overrides all routine management priorities. The adolescent PCOS population has markedly elevated depression and anxiety rates, and the psychological burden can be life-threatening. Secure safety first, then return to the PCOS management plan. [12] [14]
Second, suspected androgen-secreting tumour with rapidly progressive virilisation or very high androgen levels is a diagnostic emergency requiring urgent imaging and endocrinology referral. Do not start antiandrogen therapy in this scenario until the tumour is excluded, because treatment would mask the underlying diagnosis. [2] [3]
Management — Definitive & Stepwise
Step 1 — Lifestyle as foundation
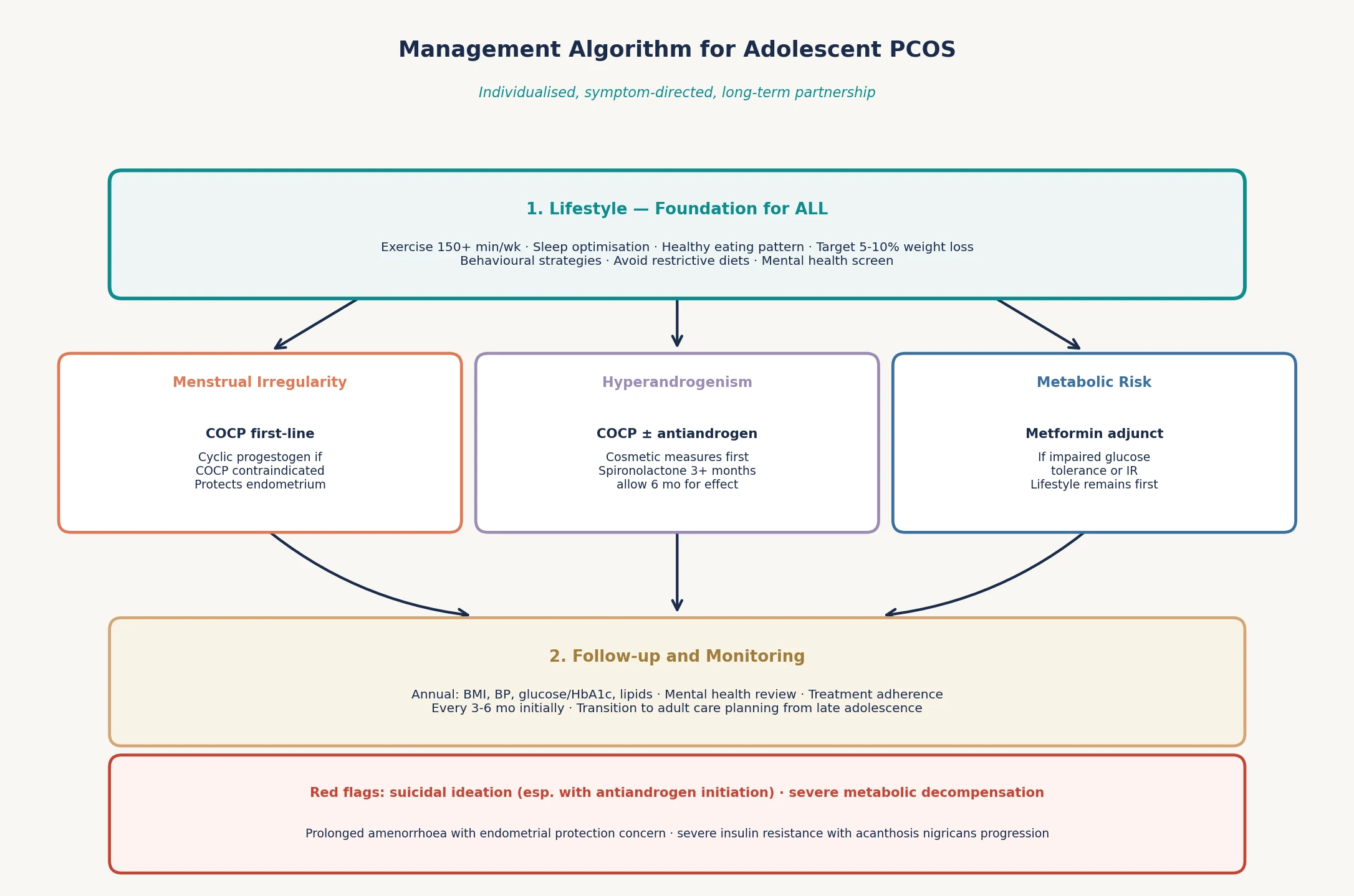
Lifestyle modification is first-line for every adolescent with PCOS, regardless of phenotype or symptom profile. The 2020 international guideline evidence summary from Moran and colleagues supports a focus on sustainable behaviour change rather than restrictive dieting. Target 150 minutes or more of moderate-intensity exercise per week, prioritise sleep, and support healthy eating patterns. A 5–10% weight reduction meaningfully improves menstrual regularity, ovulation, and metabolic markers even when the adolescent remains overweight. [7] [8]
Avoid framing lifestyle as "lose weight" because this risks triggering or worsening disordered eating in a population already vulnerable to body image distress. Frame the conversation around health behaviours, energy, and function. Involve an exercise physiologist, dietitian, or psychologist where available, and recognise that socioeconomic and cultural factors shape what "healthy eating" means for each family. [7] [14]
Step 2 — Menstrual regulation and endometrial protection
The combined oral contraceptive pill is first-line for menstrual regulation and endometrial protection in adolescents with PCOS. It reduces ovarian androgen production, raises SHBG, regularises withdrawal bleeding, and protects the endometrium from unopposed oestrogen. If COCP is contraindicated or declined, cyclic oral progestogen (such as medroxyprogesterone or norethisterone for 10–14 days every 1–2 months) provides endometrial protection without the oestrogen component. Prolonged amenorrhoea beyond 90 days warrants active endometrial management. [3] [1]
Step 3 — Hyperandrogenism management
For hirsutism and acne, start with cosmetic measures (topical treatments, laser hair removal, threading). The COCP provides first-line pharmacological antiandrogen effect. If symptoms persist after 6 months of COCP, add spironolactone as an antiandrogen — allow at least 3–6 months to see effect, and counsel on teratogenicity requiring reliable contraception. Finasteride and flutamide are alternatives used in specialist settings. Cyproterone acetate is used in some COCP formulations available in Australia and New Zealand. [3] [13]
Step 4 — Metabolic adjuncts
Metformin is an adjunct, not a first-line treatment, in adolescent PCOS. The Hoeger randomised trial in obese adolescent women showed that metformin plus lifestyle modification improved menstrual cyclicity and insulin sensitivity beyond lifestyle alone, but the effect was modest and adjunctive. Metformin is most useful when impaired glucose tolerance, significant insulin resistance, or weight management difficulty is present. It does not reliably treat hirsutism or provide endometrial protection. [8] [3]
Step 5 — Mental health and quality of life
Screen for anxiety and depression at diagnosis and at every follow-up visit, because up to 50% of women with PCOS experience these. Cinar and colleagues showed that COCP treatment itself can improve emotional distress in some patients, linking the metabolic and psychological dimensions of the condition. Quality-of-life impairment in adolescent PCOS is substantial and deserves direct attention, not dismissal as a cosmetic concern. [12] [13] [14]
Specific Subtypes & Scenarios
Obese adolescent with metabolic syndrome. This is the highest-risk phenotype. Prioritise lifestyle and metformin alongside COCP. Screen aggressively for type 2 diabetes with annual OGTT, monitor lipids and blood pressure, and consider ALT for NAFLD screening. The hepato-ovarian axis evidence supports recognising liver health as part of PCOS care. [8] [11] [17]
Lean adolescent with hyperandrogenism. PCOS is not exclusively an obesity condition. Lean adolescents can have insulin-resistant PCOS driven by post-receptor defects. The management approach is the same: lifestyle reinforcement, COCP for cycles, and cosmetic or antiandrogen therapy for hirsutism. Metformin has a smaller role in the absence of metabolic dysfunction. [5] [3]
Adolescent with eating disorder risk. The intersection of PCOS and eating disorders is dangerous. Restrictive dieting, body dissatisfaction, and insulin-driven hunger create vulnerability. Avoid weight-centric language, screen for disordered eating, and never prescribe appetite-stimulating or weight-promoting treatments without addressing the psychological context first. [14] [7]
Culturally and linguistically diverse adolescent. Hirsutism thresholds vary by ethnicity — South Asian, Middle Eastern, and Mediterranean populations have higher baseline terminal hair. Use ethnicity-specific Ferriman-Gallwey cut-offs where available. Family expectations around menstruation, fertility, and body image may differ, and interpreter use is essential when needed. [10] [9]
Gender-diverse adolescent assigned female at birth. PCOS can affect anyone with ovaries regardless of gender identity. Testosterone therapy used in gender-affirming care will suppress menstruation, complicating the menstrual history. Frame all care around the person's identity and anatomy, use chosen names and pronouns, and adapt physical examination accordingly. [1]
Transition to adult care. PCOS is a lifelong condition. Begin transition planning in late adolescence: ensure the young person understands their diagnosis, has a portable summary, knows their medication regimen, and has identified an adult GP or endocrinology pathway. Transition is a process, not a single referral letter. [1] [6]
Complications & Pitfalls
- Premature labelling based on ultrasound alone. Multifollicular ovaries are normal in adolescents. A PCOM report without persistent menstrual dysfunction and objective hyperandrogenism is not PCOS. [2] [15]
- Missing an androgen-secreting tumour. Rapid virilisation or very high testosterone is never typical PCOS. Image and refer urgently. [2] [3]
- Failing to exclude non-classic CAH. A 17-OHP level is cheap, fast, and changes management. Omitting it is a preventable error. [3]
- Weight-centric messaging that triggers eating disorders. The PCOS population is vulnerable. Frame around health behaviours, not the scale. [14] [7]
- Neglecting mental health screening. Up to 50% have anxiety or depression. If you do not ask, you will not find it. [12] [14]
- Prescribing antiandrogens without contraception counselling. Spironolactone and similar agents are teratogenic. Reliable contraception is non-negotiable. [3]
- Over-relying on metformin as a primary treatment. Metformin is an adjunct for metabolic dysfunction, not a substitute for COCP or lifestyle. [8] [3]
- Forgetting endometrial protection in prolonged amenorrhoea. Three months or more without a bleed in the setting of chronic anovulation warrants active management. [3] [16]
- Dismissing sleep apnea risk. Abdul Jafar and colleagues confirmed elevated OSA prevalence in PCOS. Ask about snoring and daytime somnolence. [18]
- Failing to plan transition. PCOS does not end at 18. A young person lost to follow-up is a long-term complication waiting to unfold. [1]
Prognosis & Disposition
PCOS is a chronic condition with a trajectory measured in decades, not visits. The prognosis depends on phenotype, metabolic burden, and the quality of longitudinal care. [6] [1]
Reproductive prognosis is generally good with appropriate management. Most adolescents with PCOS will ovulate with lifestyle modification alone or with ovulation induction when fertility is desired later. The key reproductive risks are endometrial hyperplasia from chronic unopposed oestrogen and, later, subfertility. Barry and colleagues quantified the endometrial cancer risk elevation in their meta-analysis, making endometrial protection a long-term priority. [16] [3]
Metabolic prognosis is determined by insulin resistance, obesity, and lifestyle engagement. Type 2 diabetes risk is 2–4 times higher than background, and cardiovascular risk factors (dyslipidaemia, hypertension) cluster. NAFLD adds hepatic risk through the hepato-ovarian axis. The metabolic trajectory is modifiable with sustained lifestyle engagement and appropriate pharmacotherapy. [11] [17] [18]
Psychological prognosis is highly variable and depends on whether mental health is addressed as a core part of care. Quality of life in adolescent PCOS is impaired, and untreated anxiety or depression worsens every other outcome — adherence, lifestyle engagement, follow-up attendance. [14] [12]
Disposition is outpatient and longitudinal. Review every 3–6 months initially, then annually once stable. Each visit should address menstrual control, metabolic screening, mental health, and adherence. Transition to adult care planning begins in late adolescence and completes in the early twenties. [1] [6]
Special Populations
Indigenous adolescents. Aboriginal, Torres Strait Islander, Maori, and Pacific Islander populations have higher PCOS prevalence and metabolic severity. Cultural safety, community engagement, and recognition of the social determinants of health are as important as the pharmacological plan. Frame screening and management within a holistic health model. [10] [9]
Migrant and refugee adolescents. Language barriers, differing health beliefs around menstruation and body image, and trauma exposure complicate assessment. Professional interpreters are mandatory for sensitive content. Family expectations around fertility and marriage may shape how the diagnosis is received. Build trust slowly and avoid assumptions. [1]
Adolescents in out-of-home care. Incomplete medical histories, trauma exposure, and care discontinuity are common. Reconstruct the menstrual and growth history actively. Be vigilant for eating disorders and self-harm, and ensure continuity of contraception and mental health care across placements. [14]
Socioeconomically disadvantaged adolescents. Access to exercise facilities, healthy food, specialist services, and medications is shaped by income. Before attributing "non-adherence," ask about cost, transport, and living circumstances. A management plan that ignores material reality will fail regardless of its pharmacological sophistication. [7]
Gender and sexual diversity. PCOS affects anyone with ovaries. Testosterone therapy in gender-affirming care suppresses menstruation and may alter metabolic markers, complicating assessment. Use chosen names and pronouns, adapt examination to anatomy and identity, and integrate PCOS care into holistic gender-affirming care. [1]
Evidence, Guidelines & Regional Differences
The 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS, hosted by Monash University, is the most comprehensive contemporary synthesis. Its adolescent-specific recommendations, published by Pena and colleagues in 2025, address the unique diagnostic and management challenges of this age group. These documents form the current evidence backbone for adolescent PCOS care globally. [1] [7]
The 2013 Endocrine Society clinical practice guideline from Legro and colleagues remains a widely cited framework for diagnosis and treatment, though it predates some of the adolescent-specific refinements. The 2014 European Society of Endocrinology position statement from Conway and colleagues adds a European perspective on long-term health risks. The 2004 Rotterdam consensus is the foundation upon which all current criteria are built. [3] [6] [4]
Controversies in adolescent diagnosis. The central debate is whether and how to apply adult diagnostic criteria to adolescents. Rosenfield and colleagues argued forcefully in 2015 that ultrasound morphology should not anchor an adolescent diagnosis because of the high background rate of multifollicular ovaries. The 2025 Pena recommendations endorse this caution and emphasise persistence of symptoms and objective hyperandrogenism. Anti-Mullerian hormone has been proposed as a diagnostic biomarker, but van der Ham and colleagues' 2024 systematic review found insufficient accuracy for adolescent use. [2] [1] [15]
Lifestyle evidence. Moran and colleagues' 2020 evidence summary confirms that lifestyle intervention improves metabolic outcomes, though the magnitude of menstrual and reproductive improvement varies. Hoeger's 2008 randomised trial in obese adolescent women showed that metformin adds modest benefit to lifestyle, positioning it as an adjunct rather than a standalone treatment. [7] [8]
ANZ: Monash CRE in PCOS drives the international guideline; RCH Melbourne has adolescent-specific clinical pathways; PBS-subsidised options include COCP, spironolactone, and metformin; cultural safety for Indigenous populations is embedded in care frameworks. UK: NICE recognises PCOS in its women's health guidance; RCPCH curriculum includes adolescent reproductive endocrinology; COCP and metformin are first-line; local specialist adolescent gynaecology services vary by region. US: Endocrine Society and AES guidelines apply; ACOG committee opinions address adolescent PCOS; insurance coverage for antiandrogens and laser varies; open-notes and portal confidentiality issues apply to adolescent reproductive health documentation. Canada: CPS-aligned guidance; provincial formularies determine access; Greig Health Record includes adolescent reproductive screening; transition to adult care varies by province.
Exam Pearls
- Open your answer with Rotterdam criteria plus the adolescent caveat: two of three features, persisting beyond two years post-menarche, mimics excluded. [4] [2]
- Ultrasound does not diagnose PCOS in adolescents. Multifollicular ovaries are normal. This is the single most testable adolescent point. [2] [15]
- Always exclude non-classic CAH with a 17-OHP level. It is cheap, fast, and changes management. [3]
- Lifestyle is first-line for every patient. State this before reaching for the COCP or metformin. [7]
- COCP does four things: regulates cycles, protects endometrium, raises SHBG, treats hirsutism. [3]
- Metformin is an adjunct, not a primary treatment. It addresses metabolic dysfunction, not hirsutism or endometrial protection. [8]
- Screen for mental health at every visit. Up to 50% have anxiety or depression. This is not optional. [12] [14]
- Spironolactone requires contraception. It is teratogenic. State this explicitly. [3]
- Rapid virilisation is not PCOS. Think tumour, image urgently, refer to endocrinology. [2]
- Transition planning starts in late adolescence. PCOS is a lifelong condition. [1]
PCOS adolescent answer FRAME
Four management pillars
References
- [1]Pena AS International evidence-based recommendations for polycystic ovary syndrome in adolescents. BMC medicine, 2025.PMID 40069730
- [2]Rosenfield RL The Diagnosis of Polycystic Ovary Syndrome in Adolescents. Pediatrics, 2015.PMID 26598450
- [3]Legro RS Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. Journal of clinical endocrinology and metabolism, 2013.PMID 24151290
- [4]Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertility and sterility, 2004.PMID 14711538
- [5]Witchel SF Curtailing PCOS. Pediatric research, 2020.PMID 31627209
- [6]Conway G The polycystic ovary syndrome: a position statement from the European Society of Endocrinology. European journal of endocrinology, 2014.PMID 24849517
- [7]Moran LJ Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: Lifestyle management. Obesity reviews, 2020.PMID 32452622
- [8]Hoeger K The impact of metformin, oral contraceptives, and lifestyle modification on polycystic ovary syndrome in obese adolescent women in two randomized, placebo-controlled clinical trials. Journal of clinical endocrinology and metabolism, 2008.PMID 18728175
- [9]March WA The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Human reproduction, 2010.PMID 19910321
- [10]Azziz R The prevalence and features of the polycystic ovary syndrome in an unselected population. Journal of clinical endocrinology and metabolism, 2004.PMID 15181052
- [11]Dokras A Screening women with polycystic ovary syndrome for metabolic syndrome. Obstetrics and gynecology, 2005.PMID 15994628
- [12]Barry JA Anxiety and depression in polycystic ovary syndrome: a systematic review and meta-analysis. Human reproduction, 2011.PMID 21725075
- [13]Cinar N Effect of an oral contraceptive on emotional distress, anxiety and depression of women with polycystic ovary syndrome: a prospective study. Human reproduction, 2012.PMID 22473394
- [14]Wilson NA Quality of life in adolescent girls with polycystic ovary syndrome. Journal of paediatrics and child health, 2020.PMID 32810373
- [15]van der Ham K Anti-mullerian hormone as a diagnostic biomarker for polycystic ovary syndrome and polycystic ovarian morphology: a systematic review and meta-analysis. Fertility and sterility, 2024.PMID 38944177
- [16]Barry JA Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: a systematic review and meta-analysis. Human reproduction update, 2014.PMID 24688118
- [17]Liu D The hepato-ovarian axis: genetic evidence for a causal association between non-alcoholic fatty liver disease and polycystic ovary syndrome. BMC medicine, 2023.PMID 36800955
- [18]Abdul Jafar NK Obstructive sleep apnea syndrome in polycystic ovary syndrome: a systematic review and meta-analysis. Frontiers in endocrinology, 2025.PMID 40255502