Paeds · clinical-assessment-and-reasoning
Incidental findings and overdiagnosis in children
Also known as Paediatric overdiagnosis · Incidentaloma in children · Cascade testing paediatrics · Overtesting children · Low-value paediatric care · Choosing Wisely paediatrics
A fellowship approach to incidental findings and overdiagnosis in children: plain definitions, cascade mechanisms, age-aware examples from imaging, laboratories, monitors and labels, bedside re-anchor, act-observe-stop algorithms, communication of residual risk, and safe restraint without missing time-critical disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
You ordered a test for one problem. The report answers a different question. A well-looking child now has an “abnormal” flag, a tiny lesion on imaging, or a monitor alarm. Families look at you. The trap is to treat the flag as if it were the patient. The skill is to decide, out loud, what this finding means for this child tonight. [1] [5]
Overview & Definition
Picture a school-age child who had a CT after trauma. The scan answers the trauma question. It also mentions a small renal cyst or a lung nodule the family never knew about. That unexpected result is an incidental finding — something unrelated to the question that prompted the test. [19] [5]
Overdiagnosis is different. It is the detection of a true abnormality that would not have caused symptoms or harm in that child’s lifetime, yet still triggers a disease label, further tests or treatment. Brodersen’s definitional work separates this from ordinary false positives and from underdiagnosis. [2] [1]
Newman-Toker’s unified model helps keep three errors distinct. Underdiagnosis misses disease that is present. Misdiagnosis applies the wrong label. Overdiagnosis applies a disease label to a condition that would not have mattered. You can harm a child with any of the three. [3]
Overtesting is ordering tests that were unlikely to help. Overtreatment is treating disease that did not need treatment, or treating with excess intensity. Cascades link them: one low-value test can manufacture a label that forces more care. [4] [6] [28]
Coon and colleagues framed the paediatric problem clearly: our compulsion for diagnosis can harm children through labels, procedures and anxiety even when natural history is mild. Ward Platt’s commentary places the same tension inside child health more broadly. [1] [26]
Classification
These words are not interchangeable. Use them carefully at the bedside and in viva. [2] [3]

Read the figure like this: if the child is sick and you missed sepsis, that is underdiagnosis — restraint is not the lesson. If the child is well and a sensitive test invents a lifelong label, overdiagnosis is the lesson. If the report is simply noise from contamination, that may be a false positive rather than true overdiagnosis. [2] [3]
Incidental finding
Unexpected result
- Unrelated to the original clinical question
- May be true, false or uncertain
- Needs triage: act, plan, observe or ignore
- Not automatically disease
Overdiagnosis
Label without benefit
- True abnormality by some definition
- Would not have caused harm if undetected
- Still creates label, tests or treatment
- Distinct from ordinary false positive
Cascade
Downstream care
- Further visits, imaging, labs, procedures
- Driven by anxiety, protocol and defensive culture
- Can delay the real problem
- Stopping the cascade is a skill
Must-not-miss residue
What stays open
- Threats not answered by the incidental
- Named even when you choose observation
- Handed over with an owner
- Never silenced by a neat report
A practical bedside classification for any unexpected result is four bins: [1]
- Act now — the finding is time-critical or the child is unstable. [1]
- Planned follow-up — real but non-urgent; needs owner and timing. [1]
- Observe and safety-net — low pre-test risk, well child, low yield of further testing. [1]
- Stop / reclassify as noise — contamination, wrong age range, technical artefact, or result that does not change management. [5] [6]
Epidemiology & Risk Factors
There is no single incidence of “incidental findings in childhood.” Rates depend on the test, the population and how reports are coded. Trauma CT, neonatal research MRI, preoperative echo and broad laboratory panels all generate unexpected abnormalities at different frequencies. Use source-specific data rather than one global percentage. [19] [20] [27]
Paediatric overuse update series repeatedly surface low-value targets: unnecessary imaging, continuous monitoring beyond need, antibiotics and acid suppression for self-limited illness, and excess laboratory panels. European Academy of Paediatrics surveys show clinicians recognise over-investigation and overtreatment across countries, including joint work with Japan. [7] [8] [9] [10] [11]
Risk concentrates where disease prevalence is low and test sensitivity is high. Well-looking children, opportunistic screening, adult ED defaults applied to simple paediatric presentations, and defensive culture all raise cascade risk. Production pressure can paradoxically increase testing when teams substitute panels for thinking. [1] [6] [21]
Child factors
- Low pre-test probability / well appearance
- Neonatal research or high-resolution imaging
- Complex chronic disease with noisy baselines
- Trauma imaging that covers many organs
Clinician factors
- Compulsion for a label
- Fear of missing rare disease
- Anchoring on the report flag
- Adult pathways applied to children
Technology factors
- Continuous pulse oximetry and alarms
- Sensitive imaging and coronary criteria expansion
- Age-wrong laboratory reference intervals
- Electronic order-set stacking
System factors
- Defensive culture and incomplete handovers
- Copy-forward labels in records
- Limited cascade capacity in rural settings
- Family expectation of 'full work-up'
Label-based pathways also matter. Asthma can be overdiagnosed in primary care when objective support is weak. ADHD overdiagnosis has been scoped as a real risk in some settings without denying true ADHD. Mental-disorder overdiagnosis literature in developed countries raises similar caution. Infant reflux pathways show how a normal developmental pattern can become a drug cascade. [16] [17] [25] [22]
Pathophysiology
Why does more testing create more disease labels without more benefit? Three mechanisms dominate paediatric practice. [1] [4]
Sensitivity expansion. Imaging, laboratory cut-offs and continuous monitors detect smaller and smaller deviations. Some of those deviations never become clinical disease. Kawasaki coronary imaging trends have been used as a model of how apparent abnormality can rise when detection thresholds change, even without a true epidemic of harmful disease. [18]
False manufacture. Contamination, haemolysis, wrong tubes, motion artefact, adult reference intervals and bag-urine cultures create numbers that look like disease. Hypotension can be over-called when blood-pressure methods and age norms are mishandled. The child never had the disease the flag implies. [24] [6]
Cascade amplification. Deyo described cascade effects of medical technology: one finding triggers another test, then a procedure, then treatment. Ganguli’s national physician survey shows cascades after incidental findings are common in real practice and often leave clinicians uneasy. Technology can create uncertainty rather than clarity — continuous pulse oximetry in bronchiolitis is the classic paediatric example. [4] [5] [13] [14]
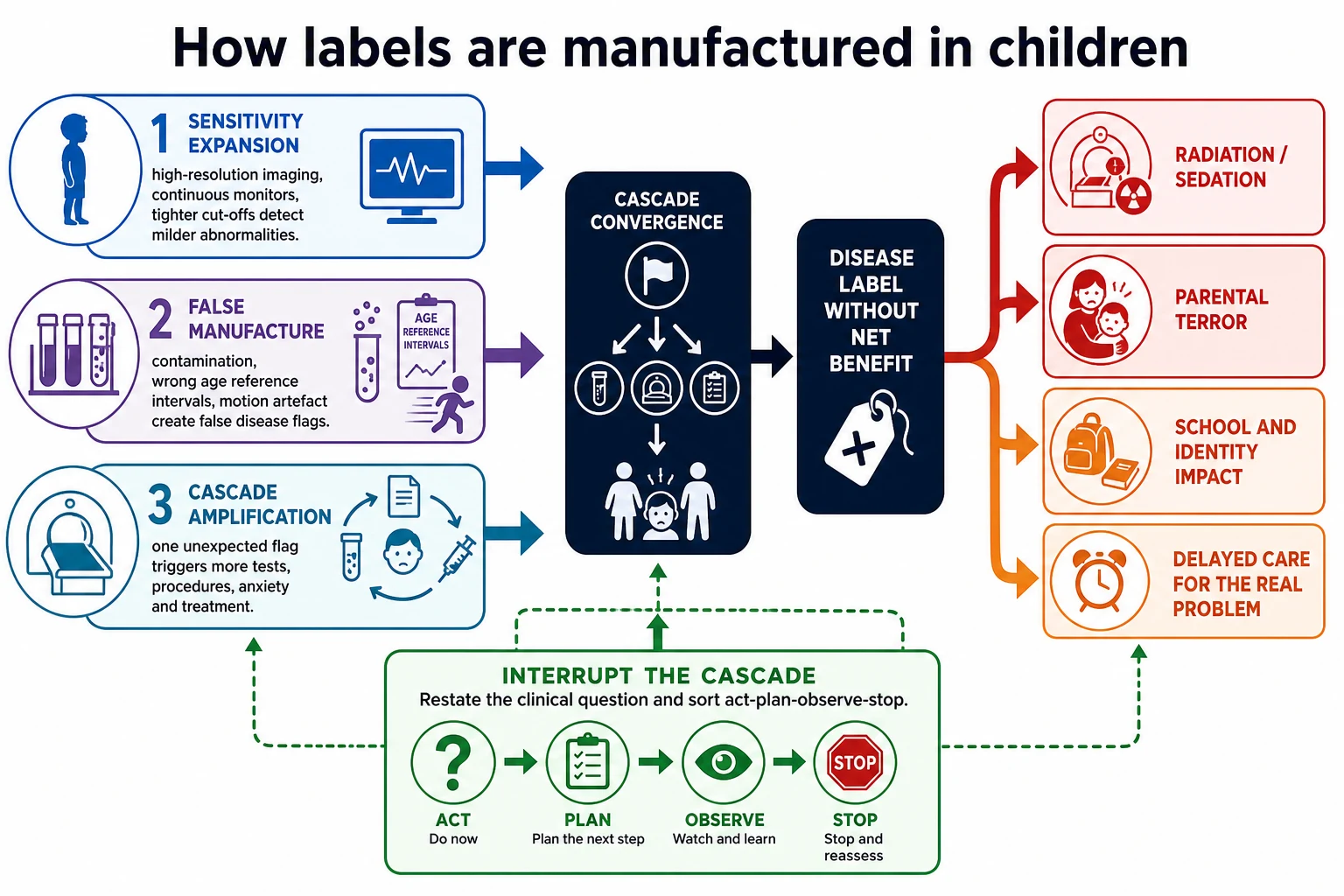
Read the figure like this: if you only ask “is the number abnormal?”, you will always find work. If you ask “would detecting this help the child?”, many cascades stop. [1] [2] [28]
Labels change behaviour. Families seek more care. Clinicians defend the label. Schools and services may reorganise around a diagnosis that was never destined to harm. Gram and colleagues’ broader taxonomy of harms of too much medicine helps name patient, practitioner, public and planetary costs without turning stewardship into slogans. [1] [28] [15]
Clinical Presentation
Incidental findings present as paperwork, not as a chief complaint. The child may look well. The family may look terrified. Your first job is still the child, not the PDF. [5] [19]
Common entry points: [1]
- Trauma or other CT/MRI reports listing extra lesions. [19]
- Neonatal research or clinical brain MRI with unexpected white-matter or structural notes. [20]
- Preoperative echocardiography with high rates of minor incidentals and a smaller yield of important anomalies. [27]
- Continuous monitor alarms during recovery from bronchiolitis or other viral illness. [13] [14] [15]
- Broad laboratory panels with age-wrong flags. [6] [24]
- Longstanding disease labels (asthma, ADHD, reflux) that never had solid support. [16] [17] [22]
Age changes the story. Neonates generate imaging incidentals and sample-volume dilemmas. Infants generate monitor and reflux cascades. Preschool children collect asthma labels. School-age children collect trauma CT extras and attention labels. Adolescents meet adult ED defaults and mental-health labelling pressure. [20] [13] [16] [17] [21]
Caregiver concern still matters. A family who says the child is different from usual is not cancelled by a pretty incidental report. Put both the concern and the incidental into the problem representation. [1]
Differential Diagnosis
When an unexpected result appears, run two differentials at once. [3] [1]
Differential for the original problem stays open until answered. Do not let a renal cyst distract you from evolving peritonitis, or a mild anaemia flag distract you from meningism. [1]
Differential for the unexpected result asks: true disease needing action; true abnormality of no clinical importance; technical artefact; contamination; wrong reference interval; colonisation; or overdiagnosis of a real but harmless entity. [2] [5]
Act-now possibilities
- Critical electrolyte or glucose abnormality
- Imaging showing true surgical emergency
- New threat signs at the bedside
- Finding that explains instability
True but non-urgent
- Stable structural variants needing timed follow-up
- Laboratory trends that need planned repeat
- Specialty review without same-day cascade
Noise / low-value
- Contaminated culture
- Adult range applied to a child
- Isolated monitor blip in a well child
- Incidental of known benign natural history
Still open original threats
- Sepsis, surgical abdomen, raised ICP
- Cardiac ductal emergency in neonates
- Safeguarding differentials
- Whatever the first test was meant to answer
Flexible differentials remain essential. After the first positive incidental, ask what else could still be true. After the first cascade test, ask whether you are solving the child’s problem or feeding the algorithm. [1] [4]
Clinical & Bedside Assessment
If the child is unstable, treat first. Unexpected potassium, glucose or tension physiology can be part of resuscitation. Cascades wait. [3]
When you can pause, use a thirty-second incidental pause: [1]
- What clinical question prompted the original test? [1]
- Is that question answered? [1]
- How does the child look and behave now, including caregiver baseline? [1]
- What is the pre-test probability that this new finding is dangerous? [1]
- Will further action change outcome more than it will create harm? [1]
- Who owns follow-up if we do not act tonight? [1] [5] [6]
Examine the child before you examine the report footnotes. Work of breathing, perfusion, consciousness, fever pattern, pain behaviour and developmental context re-anchor numbers. In complex children, ask what is different from usual and compare with personal baselines rather than population flags alone. [6] [14]
Common technique errors manufacture false disease: bag urine, difficult blood draws with haemolysis, blood pressures from the wrong cuff, monitor probes on a moving toddler, and adult laboratory ranges auto-flagging paediatric values. Fix the method before you invent a diagnosis. [24] [6]
Use professional interpreters when explaining uncertainty. Families should hear what the finding is, what it is not, and what you will watch for — not a flood of rare disease names. [15] [6]
Investigations
Further tests after an incidental finding must earn their place. Ask which active differential the next test discriminates, and whether a positive or negative result will change management. [6] [8]
Often low-value once the clinical question is answered [1]
- Chest radiography in straightforward bronchiolitis rarely changes management and can generate incidental opacities and antibiotics. [12]
- Continuous oximetry after recovery may manufacture intermittent desaturation labels and prolong stay. [13] [14] [15]
- Broad “just in case” panels in low-risk viral presentations. [6] [7]
- Adult ED default panels for simple paediatric febrile seizure pathways. [21]
Often worth planned evaluation [1]
- Incidental imaging with features that have known malignant or progressive potential — using specialty guidance, not panic same-day pan-scans. [19]
- Preoperative or clinical echo findings that are truly structural and actionable, while recognising many incidentals are minor. [27]
- Neonatal MRI findings with clear clinicoradiologic importance after specialist interpretation. [20]
Age-specific reference intervals matter. A number that is “red” on an adult-configured analyser may be normal for age. Ray’s blood-pressure work shows how measurement context changes hypotension labels. Do not treat the flag; treat the child. [24]
Repeat testing is not always safer. Timed observation with concrete return triggers can be the higher-value investigation. Pending results need an owner and a plan for residual risk. [5] [6]
Management — Resuscitation
Life threat and incomplete information often coexist. Protect airway, breathing, circulation and glucose. Call for help. Keep the differential open while you act. [3]
During resuscitation, some unexpected results are not “incidentals.” Dangerous hypoglycaemia, critical hyperkalaemia, tension physiology on imaging, or a new mass effect that explains coma must be treated as primary problems. Defer non-discriminating cascade tests until physiology stabilises. [3] [4]
Explain briefly to families: “We are treating what can harm your child right now. Some report details can wait until they are safer.” That is honest stewardship, not secrecy. [15]
Management — Definitive & Stepwise
After threat control, use a closed loop. [1] [5] [6]
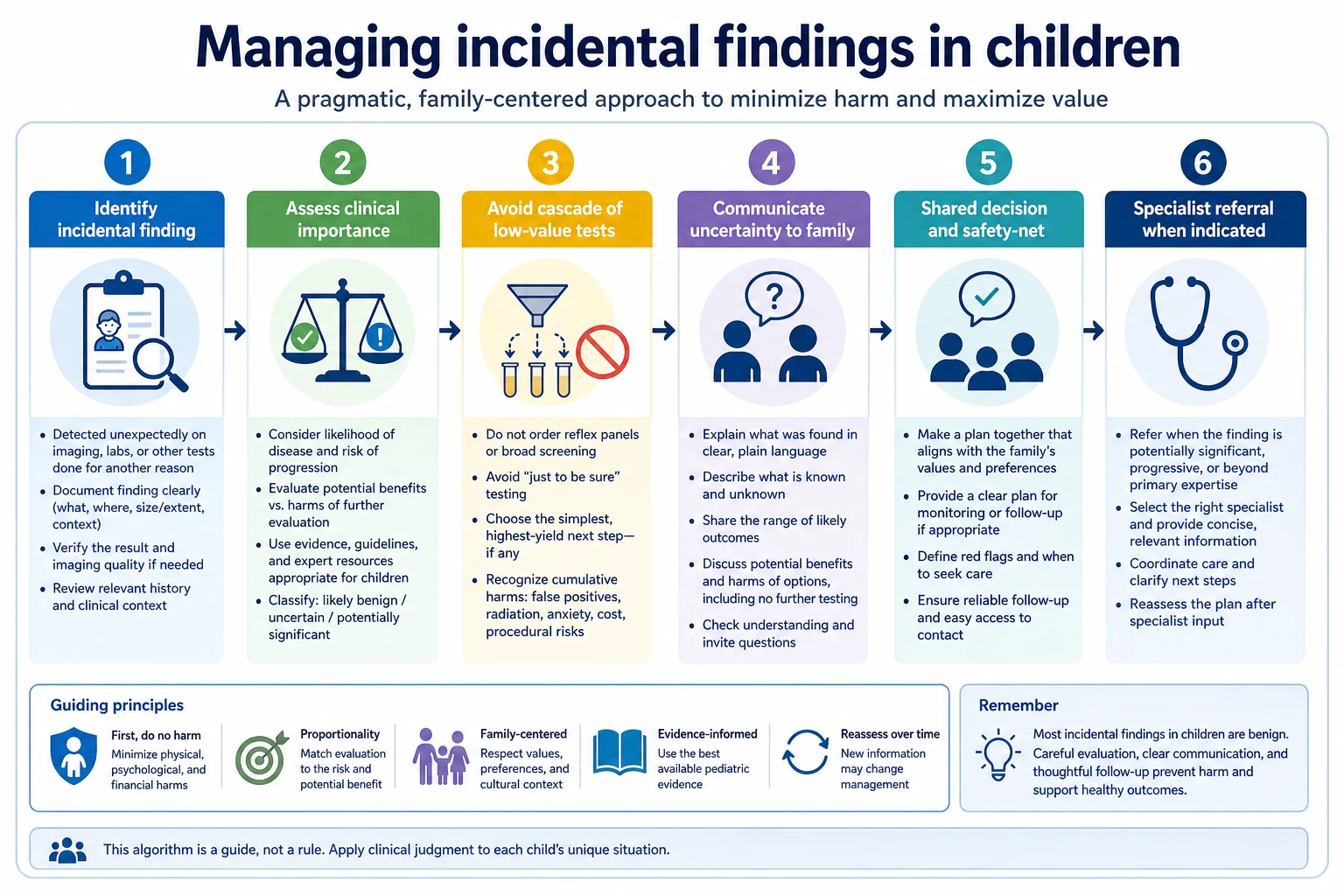
- Restate the original clinical question and whether it is answered. [1]
- Reassess the child and caregiver concern. [1]
- Classify the unexpected finding into act / plan / observe / stop. [1]
- If acting, choose the least-harm discriminating next step. [1]
- If observing, write concrete return triggers and a review time. [1]
- If stopping, document the reasoning so the next clinician does not restart the cascade automatically. [1]
- Communicate in plain language what the finding is and is not. [1]
- Hand over residual risks, pending items and the named owner. [1]
- Seek feedback when the true course becomes clear so your calibration improves. [5] [6] [23]
Shared decision-making should include radiation, sedation, sample volume, false-positive anxiety, school impact of labels, and travel burden for cascade appointments. Choosing Wisely and EAP overtesting statements support system-level restraint; they never replace individual residual-risk judgment. [6] [23] [28]
Stopping a cascade is active care. Say: “Further testing is more likely to create false alarms than to help. Here is what would make me change my mind.” That sentence is examiner gold and family-safe when the pre-test risk is truly low. [1] [2]
Specific Subtypes & Scenarios
Trauma CT incidental findings. After blunt abdominal trauma imaging, unexpected lesions are common enough that teams need a triage habit: immediate action versus outpatient specialty review versus no further imaging. Do not abandon the trauma pathway while you chase a tiny cyst. [19]
Neonatal brain MRI incidentals. Research and clinical high-field imaging can show features of uncertain importance. Interpret with neonatology and radiology expertise; avoid lifelong labels from unreviewed research reads. [20]
Continuous pulse oximetry in bronchiolitis. Intermittent desaturations in a recovering, feeding, interactive infant often reflect technology and sleep more than new disease. Parental perspectives show monitors can increase anxiety. Use oximetry when it answers a clinical question; stop when it only manufactures alarms. [13] [14] [15]
Bronchiolitis chest radiograph. Radiography rarely helps classic bronchiolitis and can drive antibiotics for incidental opacities. Reserve imaging for atypical courses. [12]
Asthma labels without objective support. Primary-care analyses show overdiagnosis risk when wheeze labels stick without appropriate testing or review. Revisit the label when the story does not fit. [16]
ADHD and mental-health labels. Scoping and review work document potential overdiagnosis in some contexts. The answer is careful assessment, not reflexive denial of distress or of true ADHD. [17] [25]
Infant reflux and PPIs. International recommendations and later practice data show acid suppression often outruns evidence for simple reflux symptoms. Prefer feeding support and time over automatic drugs. [22] [6]
Preoperative echo incidentals. Pectus and similar pathways can yield many minor findings and fewer critical anomalies. Plan follow-up for the important minority without panicking over every trivial note. [27]
Kawasaki coronary sensitivity. Expanding detection can increase “abnormal” coronary labels; interpret trends with the clinical syndrome, not imaging fashion alone. [18]
Adult ED simple febrile seizure work-ups. Overtesting and overdiagnosis risk rises when adult defaults meet a common paediatric script. Use paediatric pathways. [21]
Blood-pressure hypotension labels. Method and age norms matter before fluid or ICU labels. [24]
Rural or telehealth first contact. Limited cascade capacity can be protective if observation and clear return advice are feasible — and dangerous if residual risk is high and rescue is far. State what you cannot resolve remotely. [6] [10]
Complications & Pitfalls
Cascade harm includes radiation, sedation, needle trauma, antibiotic exposure, delayed sleep, school absence, cost and family terror. Parental experience with continuous oximetry shows how technology reshapes the hospital experience. [4] [5] [15] [28]
Label harm is quieter. A child may carry an asthma, ADHD, cardiac or “chronic disease” identity that changes sport, insurance, schooling and self-concept without changing natural history. [1] [16] [17]
Cognitive traps: [1]
- Anchoring on the incidental and missing the original disease. [1]
- Search-satisfying after the first abnormal number. [1]
- Diagnostic momentum from copy-forward problem lists. [1]
- Equating thoroughness with safety. [1]
- Using “avoid overdiagnosis” as an excuse to ignore red flags or caregiver concern. [1] [3] [6]
Handover that dumps every abnormality without prioritisation restarts the cascade on the next shift. Handover that hides residual risk creates underdiagnosis. Aim for ordered residual risk with owners. [5]
Prognosis & Disposition
Disposition follows residual risk, trajectory and rescue capability — not the neatness of a completed cascade. A well child with a low-risk incidental and a clear safety net may go home with planned follow-up. An uncertain child with high pre-test threat needs observation even if the incidental looks minor. [1] [6]
Write the plan so another clinician can continue it: what was found, why it is or is not being chased, what would change your mind, who owns the next step, and when the family should return. Pending specialty reviews need appointments, not vague “follow up later.” [5]
Later feedback calibrates restraint. If an observed finding later proved important, learn without swinging to permanent overtesting. If a cascade harmed a well child, learn without swinging to neglect. [1] [23]
Special Populations
Neonates need wide differentials for true disease and careful handling of imaging incidentals. Sample volume limits also argue against reflexive panels. [20] [6]
Infants with bronchiolitis are the textbook continuous-monitoring population. Match monitoring intensity to clinical need. [13] [14]
Medical complexity produces baseline abnormal numbers. Compare with the child’s usual. Avoid both overcalling baseline noise and undercalling true change. [6] [7]
Disability and neurodiversity can attract behavioural labels that miss medical disease — or medical labels that miss support needs. Keep both eyes open. [25] [17]
Indigenous, migrant and language-discordant families need interpreters and culturally safe uncertainty talk. A misunderstood incidental can destroy trust. [6]
Socioeconomic disadvantage and rural distance make cascade follow-up fragile. Do not design plans families cannot complete; escalate or simplify deliberately. [10]
Out-of-home care and youth justice bring fragmented records. Prior labels may be wrong or incomplete. Re-verify before cascading. [1]
Adolescents face sports screening, mental-health labelling and adult-service transitions. Confidentiality and shared decisions still apply. [17] [25]
Maltreatment contexts require both vigilance and restraint: over-calling can harm families; under-calling can harm children. Follow local mandatory pathways with documented reasoning. [3]
Evidence, Guidelines & Regional Differences
Coon’s 2014 Pediatrics paper remains a core paediatric overdiagnosis frame: compulsion for diagnosis, label harm and cascade risk. Brodersen clarifies definitions. Newman-Toker places overdiagnosis beside underdiagnosis and misdiagnosis. Deyo and later cascade surveys explain downstream care. [1] [2] [3] [4] [5]
Paediatric overuse update series (including Coon/Money work) and EAP statements translate the concept into recurring clinical targets. European and Japan-linked surveys show the problem is recognised internationally. Choosing Wisely-linked opinion continues to push pragmatic stewardship. [7] [8] [9] [6] [10] [11] [23]
Condition-specific evidence supports selective restraint without dogma: bronchiolitis radiography utility, oximetry-driven uncertainty, asthma and ADHD overdiagnosis literature, infant PPI pathways, trauma CT incidentals, neonatal MRI incidentals, and adult ED overtesting of simple paediatric scripts. [12] [13] [16] [17] [22] [19] [20] [21]
Controversies remain. Screening expansion, defensive practice, and parental expectation of comprehensive testing pull toward cascades. Rare-disease advocacy pulls toward earlier detection. The fellowship skill is threshold thinking: test when residual risk justifies it; stop when further testing mainly manufactures labels. [1] [26] [28]
Partnering-with-consumers and open-disclosure expectations shape how uncertainty and incidentals are explained. Local Choosing Wisely lists and radiation stewardship programmes change operational targets. Cultural safety for Aboriginal and Torres Strait Islander families, and Te Tiriti-informed care for Māori whānau, belong inside cascade conversations — especially when follow-up travel is burdensome. [6] [23]
MRCPCH stations reward clear residual-risk language and sensible restraint. Four-nation pathways and NICE-linked guidance may operationalise specific low-value targets; they do not replace bedside classification of incidentals. [6] [2]
ABP patient-safety domains and ACGME systems-based practice milestones treat overuse as a competency issue. Choosing Wisely culture and paediatric overuse series are core teaching sources. Malpractice climate may pressure cascades; documentation of residual-risk reasoning is the professional response, not unlimited testing. RCPSC medical-expert and communicator EPAs expect the same clarity. [7] [8] [9] [5]
Exam Pearls
- Define overdiagnosis as detection of a condition that would not have caused harm — not merely a false-positive test. [2] [1]
- Incidental finding = unexpected result unrelated to the clinical question. [5] [19]
- Always restate the original question before chasing the new flag. [1]
- Sort into act / plan / observe / stop. [5] [6]
- Low prevalence destroys positive predictive value in well children. [1] [6]
- Technology can create uncertainty — continuous oximetry is the classic example. [13] [14]
- Bronchiolitis radiographs are often low value in classic disease. [12]
- Label harm is real in asthma, ADHD and mental-health pathways; so is under-recognition — hold both truths. [16] [17] [25]
- Cascades are common after incidentals; stopping them is active care. [4] [5]
- Hand over residual risk and a named owner. [5]
- Restraint never excuses missing time-critical disease. [3]
- In communication stations, explain what you are not doing and why, with return triggers. [15] [6]
- In long case, justify every major test against the problem representation. [1] [7]
PAUSE before you chase
References
- [1]Coon ER Overdiagnosis: how our compulsion for diagnosis may be harming children. Pediatrics, 2014.PMID 25287462
- [2]Brodersen J Overdiagnosis: what it is and what it isn't. BMJ evidence-based medicine, 2018.PMID 29367314
- [3]Newman-Toker DE A unified conceptual model for diagnostic errors: underdiagnosis, overdiagnosis, and misdiagnosis. Diagnosis (Berlin, Germany), 2014.PMID 28367397
- [4]Deyo RA Cascade effects of medical technology. Annual review of public health, 2002.PMID 11910053
- [5]Ganguli I Cascades of Care After Incidental Findings in a US National Survey of Physicians. JAMA network open, 2019.PMID 31617925
- [6]Størdal K Overtesting and overtreatment-statement from the European Academy of Paediatrics (EAP). European journal of pediatrics, 2019.PMID 31506723
- [7]Money NM 2021 Update on Pediatric Overuse. Pediatrics, 2022.PMID 35059726
- [8]Money NM 2019 Update on Pediatric Medical Overuse: A Systematic Review. JAMA pediatrics, 2020.PMID 32011675
- [9]Coon ER 2018 Update on Pediatric Medical Overuse: A Review. JAMA pediatrics, 2019.PMID 30776069
- [10]Jankauskaite L Overuse of medical care in paediatrics: A survey from five countries in the European Academy of Pediatrics. Frontiers in pediatrics, 2022.PMID 36177454
- [11]Jankauskaite L Over-investigation and overtreatment in pediatrics: a survey from the European Academy of Paediatrics and Japan Pediatric Society. Frontiers in pediatrics, 2024.PMID 38455393
- [12]Schuh S Evaluation of the utility of radiography in acute bronchiolitis. The Journal of pediatrics, 2007.PMID 17382126
- [13]Quinonez RA When technology creates uncertainty: pulse oximetry and overdiagnosis of hypoxaemia in bronchiolitis. BMJ (Clinical research ed.), 2017.PMID 28814557
- [14]Coon ER Continuous Physiologic Monitoring: False Alarms and Overdiagnosis. Journal of hospital medicine, 2018.PMID 29694451
- [15]Chi KW Parental Perspectives on Continuous Pulse Oximetry Use in Bronchiolitis Hospitalizations. Pediatrics, 2020.PMID 32675334
- [16]Looijmans-van den Akker I Overdiagnosis of asthma in children in primary care: a retrospective analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2016.PMID 26917656
- [17]Kazda L Overdiagnosis of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents: A Systematic Scoping Review. JAMA network open, 2021.PMID 33843998
- [18]Coon ER Paediatric overdiagnosis modelled by coronary abnormality trends in Kawasaki disease. Archives of disease in childhood, 2018.PMID 29472194
- [19]Ugalde IT Incidental Findings on Computed Tomography in Children With Blunt Abdominal Trauma. Annals of emergency medicine, 2025.PMID 39846906
- [20]Sullivan G Brain 3T magnetic resonance imaging in neonates: features and incidental findings from a research cohort enriched for preterm birth. Archives of disease in childhood. Fetal and neonatal edition, 2024.PMID 38960453
- [21]Louie JP When less is more: Overdiagnosis and overtesting in pediatric febrile seizures in the adult emergency department. The American journal of emergency medicine, 2025.PMID 40532406
- [22]Størdal K Reducing the use of proton pump inhibitors in infants with reflux symptoms. BMJ (Clinical research ed.), 2024.PMID 38816024
- [23]Brändle G An Opinion on Medical Overuse in the Context of the European Academy of Paediatrics Choosing Wisely Initiative. Acta paediatrica (Oslo, Norway : 1992), 2026.PMID 41992654
- [24]Ray S Risk of over-diagnosis of hypotension in children: a comparative analysis of over 50,000 blood pressure measurements. Intensive care medicine, 2017.PMID 28526952
- [25]Merten EC Overdiagnosis of mental disorders in children and adolescents (in developed countries). Child and adolescent psychiatry and mental health, 2017.PMID 28105068
- [26]Ward Platt M Overdiagnosis and child health. Archives of disease in childhood, 2018.PMID 29643100
- [27]Clinker CE Preoperative Echocardiography in Pectus Excavatum: High Rate of Incidental Findings, Low but Clinically Important Yield of Significant Anomalies. Journal of pediatric surgery, 2025.PMID 40930387
- [28]Gram EG Less is more for patients, practitioners, public and planet: a taxonomy for the harms of too much medicine. BMJ evidence-based medicine, 2025.PMID 41047163