Paeds · endocrinology-diabetes-and-growth
Thyroid nodules, goitre and thyroid cancer
Also known as Paediatric thyroid nodule · Childhood thyroid cancer · Differentiated thyroid carcinoma in children · Papillary thyroid carcinoma in children · Paediatric goitre · Medullary thyroid carcinoma in children
Fellowship guide to paediatric thyroid nodules, goitre and thyroid cancer: recognise the neck mass, risk-stratify with ultrasound (TI-RADS) and FNA (Bethesda), understand the higher childhood malignancy risk and gene-fusion biology, and step through multidisciplinary surgery, risk-adapted radioiodine and surveillance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the teenager who finds a lump in the shower, or the school-age child whose paediatrician notices an asymmetric swelling on routine examination. Most such thyroid nodules are benign, yet a general paediatrician must move each one through a defined pipeline rather than watch and wait blindly, because childhood nodules carry a malignancy risk of roughly 20–25% — about twice the adult figure. [1] [5]
A thyroid nodule is a discrete focal lesion within the thyroid, distinguishable from the surrounding parenchyma on ultrasound. A goitre describes enlargement of the whole gland and may be diffuse (uniform) or multinodular. Thyroid cancer in children is overwhelmingly differentiated thyroid carcinoma (DTC), of which papillary thyroid carcinoma (PTC) accounts for the large majority; follicular and medullary subtypes are far less common but change management decisively. [1] [4]
The reason this leaf matters for a fellowship candidate is that the paediatric landscape is genuinely different from the adult one: higher pretest probability of malignancy, a different molecular driver profile (gene fusions rather than point mutations), more extensive disease at presentation yet markedly better survival, and a long surveillance horizon that spans the transition to adult care. [4] [7] [17]
Classification
Clinicians classify paediatric thyroid masses along three practical axes that feed directly into management: the nodule's ultrasound appearance, its cytology on fine-needle aspiration, and — once malignant — its histology and stage. Each axis has a named system, and an examiner expects you to name them. [1] [2]
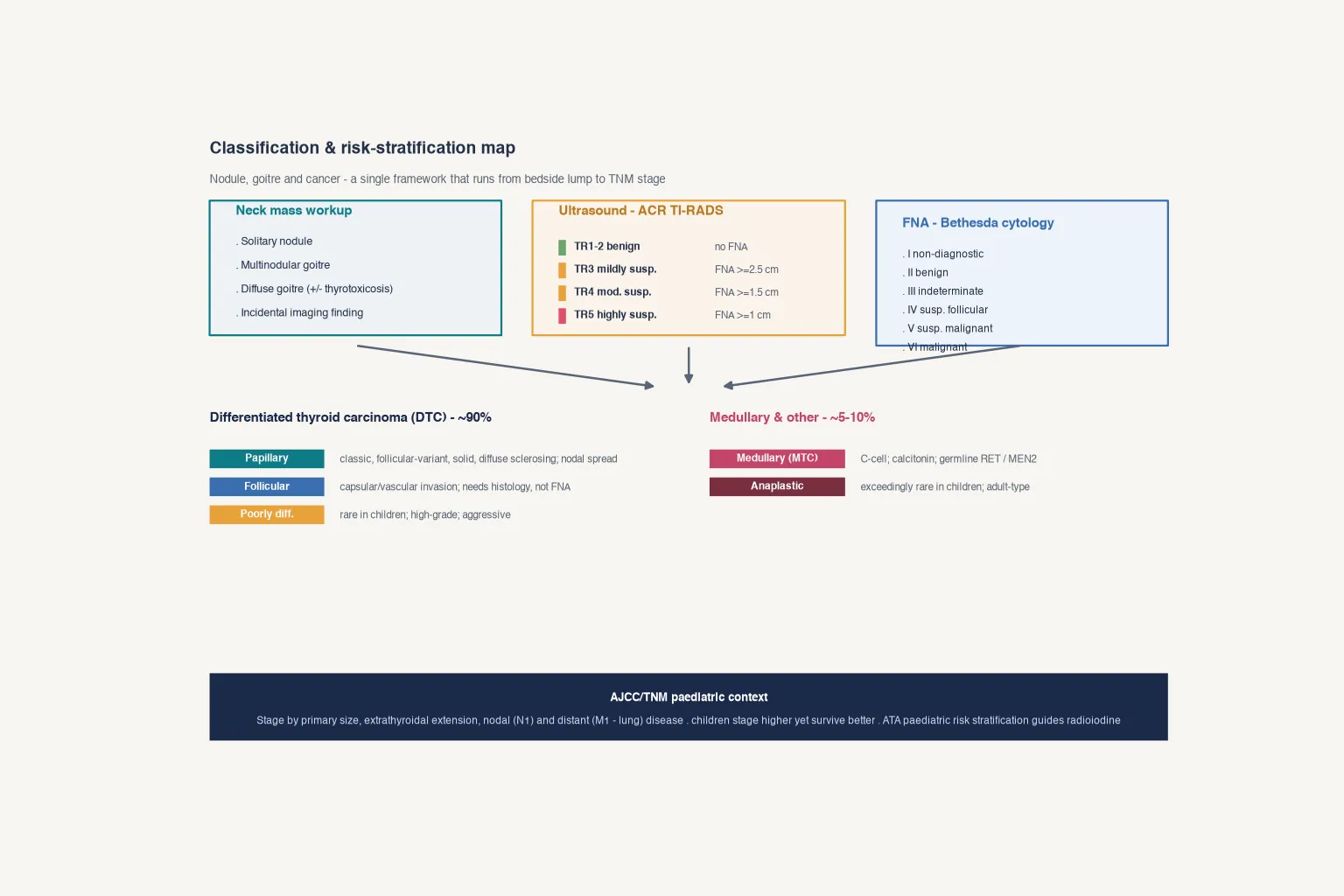
The ACR Thyroid Imaging Reporting and Data System (TI-RADS) scores five sonographic feature categories — composition, echogenicity, shape, margin and echogenic foci — into a point total that assigns each nodule a tier from TR1 (benign) to TR5 (highly suspicious) with size-based fine-needle aspiration thresholds. [2] [3]
Cytology uses the Bethesda System for Reporting Thyroid Cytopathology, whose six categories run from non-diagnostic (I) through benign (II), indeterminate (III–IV) and suspicious for malignancy (V) to malignant (VI), each carrying a malignancy risk that frames the next decision. Molecular testing increasingly resolves the indeterminate middle categories in children, where fusion events can be detected on limited aspirate material. [12] [17]
Papillary (PTC)
~90% of DTC
- Classic, follicular-variant, solid, diffuse sclerosing subtypes
- Spreads early to cervical nodes
- Driven by gene fusions (RET/PTC, NTRK, ALK) in children
- Excellent prognosis even with nodal disease
Follicular (FTC)
Minority of DTC
- Requires histology — capsular or vascular invasion
- FNA cannot distinguish FTC from follicular adenoma
- Fusion/RAS-like drivers
- Lower nodal, higher distant (bone) metastasis risk
Medullary (MTC)
C-cell origin
- Calcitonin-secreting; not radioiodine-avid
- Often germline RET / MEN2 — genetic counselling mandatory
- Prophylactic thyroidectomy in known RET carriers
- Poorer prognosis than DTC if advanced
Histology trap. Follicular carcinoma cannot be diagnosed on cytology alone — FNA cannot assess capsular or vascular invasion, so the call moves from Bethesda indeterminate to histology after surgery. Quoting "Bethesda IV equals follicular cancer" loses easy marks. [1] [5]
Epidemiology & Risk Factors
Thyroid nodules are uncommon in children compared with adults, but the few that present carry disproportionate malignancy risk. Population and registry data show a rising incidence of differentiated thyroid carcinoma in children, adolescents and young adults over recent decades, partly driven by improved imaging detection and partly by genuine increases in high-risk subsets such as childhood cancer survivors exposed to radiation. [4] [19]
Headline numbers for viva
The dominant risk factors cluster around two themes. Radiation exposure — especially therapeutic neck radiotherapy for a prior childhood cancer, or historical environmental exposure — substantially raises both nodule formation and malignant transformation. Genetic susceptibility syndromes (DICER1, PTEN-hamartoma/Cowden, familial adenomatous polyposis, Carney complex, and multiple endocrine neoplasia type 2 with germline RET) carry surveillance and surgical implications that change the whole care pathway. [1] [13] [21]
Iodine status shapes the benign side of the equation: endemic iodine deficiency produces diffuse and multinodular goitre, which remains a public-health concern in some regions and raises the differential for an enlarged gland even in iodine-replete populations. [1]
Pathophysiology
Most paediatric thyroid nodules are benign clonal expansions — follicular adenomas or colloid nodules within a multinodular goitre — that grow because of replicative drive without the capacity for invasion or metastasis. The malignant minority shares upstream biology with these benign lesions but acquires additional genetic events that unlock invasion and spread. [10] [12]
The central signalling axis in differentiated thyroid carcinoma is the MAPK pathway (RAS–RAF–MEK–ERK), with the PI3K–AKT–mTOR axis contributing especially to follicular lesions. What makes children distinctive is the type of genetic event: paediatric papillary carcinomas are dominated by gene fusions (RET/PTC rearrangements, ETV6::NTRK3, ALK and BRAF fusions) rather than the BRAF V600E point mutation that predominates in adults. This fusion biology underlies both the more aggressive histological variants seen in young patients and their excellent response to radioiodine. [10] [12] [17]
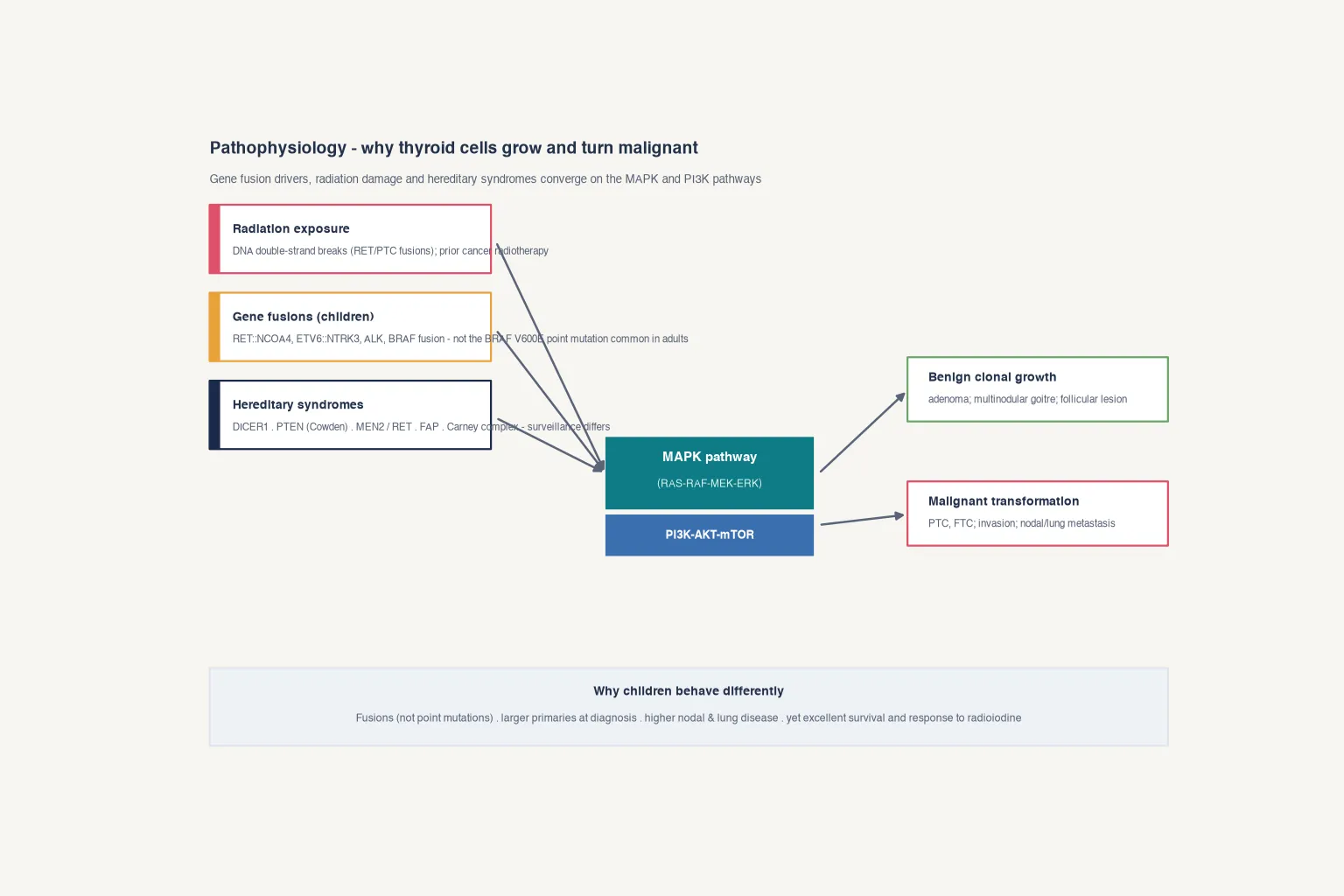
Medullary thyroid carcinoma has entirely different biology: it arises from parafollicular C-cells, secretes calcitonin, is driven by RET variants (often germline in MEN2), and is not radioiodine-avid. Recognising the C-cell lineage is essential because it redirects the workup toward calcitonin measurement, genetic testing and a different surgical and surveillance calculus. [13] [14]
A useful teaching frame: children present with larger primaries and more extensive nodal and pulmonary disease than adults, yet survive markedly better and respond briskly to radioiodine — a paradox an examiner will probe. [7] [11]
Clinical Presentation
The presentation is almost always a neck mass — either felt by the child or family, or detected incidentally on imaging performed for another reason (carotid ultrasound, cervical spine MRI, or cross-sectional imaging during cancer surveillance). Diffuse or multinodular goitre may instead surface as a visible, symmetric or asymmetric neck swelling noted on routine examination. [1] [5]
Examine for the features that raise the pretest probability of malignancy: a firm or fixed nodule, persistent rather than fluctuant, associated cervical lymphadenopathy (especially firm or matted nodes), and any sign of local invasion such as a new hoarse voice suggesting recurrent laryngeal nerve involvement. Compressive symptoms — dysphagia, dyspnoea or stridor — suggest a large goitre or an invasive mass and shift the encounter toward urgent imaging and airway assessment. [1]
Most children with a thyroid nodule are clinically euthyroid, which is why thyroid function testing does not replace structural evaluation: a normal TSH never rules out malignancy. When thyrotoxicosis accompanies a diffuse goitre, think Graves disease; when it accompanies a solitary hyperfunctioning nodule, the lesion is almost always benign but still needs documentation and functional imaging, not FNA. [1] [5]
Differential Diagnosis
The neck mass differential for a child is broad, and anchoring on thyroid malignancy too early or too late both cost marks. First separate thyroid from non-thyroid causes: thyroglossal duct cyst (midline, moves with swallowing or tongue protrusion), branchial cleft cyst (lateral), lymphadenopathy (infectious or reactive), and dermoid or sebaceous cysts all sit near the thyroid region. [1]
Within the thyroid itself, a focal lesion may be a benign follicular adenoma, a colloid or hyperplastic nodule in a multinodular goitre, a cyst, or a true neoplasm (PTC, FTC, poorly differentiated, medullary or, exceptionally rarely in children, anaplastic). Diffuse gland enlargement broadens to autoimmune thyroiditis (Hashimoto), Graves disease, simple colloid goitre and iodine-deficiency goitre. [1] [5]
The clinically decisive forks are three. First, is the patient thyrotoxic, hypothyroid or euthyroid? Functional status reframes benign (toxic nodule, Graves) versus malignant (usually euthyroid) pathways. Second, are there red-flag features (firm/fixed, nodes, voice change, rapid growth) that raise malignancy and accelerate imaging and FNA? Third, is there a syndromic or radiation context that changes the pretest probability and the surveillance plan? [1] [13]
Iodine sufficiency is the norm in Australia and New Zealand, so endemic iodine-deficiency goitre is uncommon; most diffuse goitres encountered in ANZ practice are autoimmune (Hashimoto or Graves) or simple colloid. Nonetheless, ask about diet, supplements and recent migration from iodine-deficient regions, because iodine status still shapes the benign differential. [1]
Clinical & Bedside Assessment
Take a focused history of the mass itself: onset, growth rate, pain, and any compressive or invasive symptoms (dysphagia, dyspnoea, voice change). Record a radiation history explicitly — prior cancer radiotherapy, environmental or occupational exposure, and family history of thyroid or other endocrine cancers. Elicit a family history probing for syndromes: thyroid cancer clusters, MEN2 features (phaeochromocytoma, hyperparathyroidism), and DICER1 or PTEN-associated tumours. [1] [21]
Examine the child seated and relaxed, observing the neck at rest and on swallowing. Palpate the thyroid from behind, characterising each nodule by size, consistency (firm, cystic, fixed), mobility, tenderness and relationship to surrounding structures. Perform a careful cervical lymph node examination across all neck levels, because nodal disease changes staging and surgical planning. Inspect for signs of thyrotoxicosis (tremor, tachycardia, eye signs) or hypothyroidism (bradycardia, slow-relaxing reflexes, growth concerns) that point away from a purely structural problem. [1]
Voice assessment is mandatory and often skipped: a breathy or hoarse voice before any surgery suggests recurrent laryngeal nerve involvement and warrants urgent referral. Document pubertal and growth status, because thyroid disease interacts with growth and the long surveillance horizon spans adolescence into adulthood. [1] [6]
Investigations
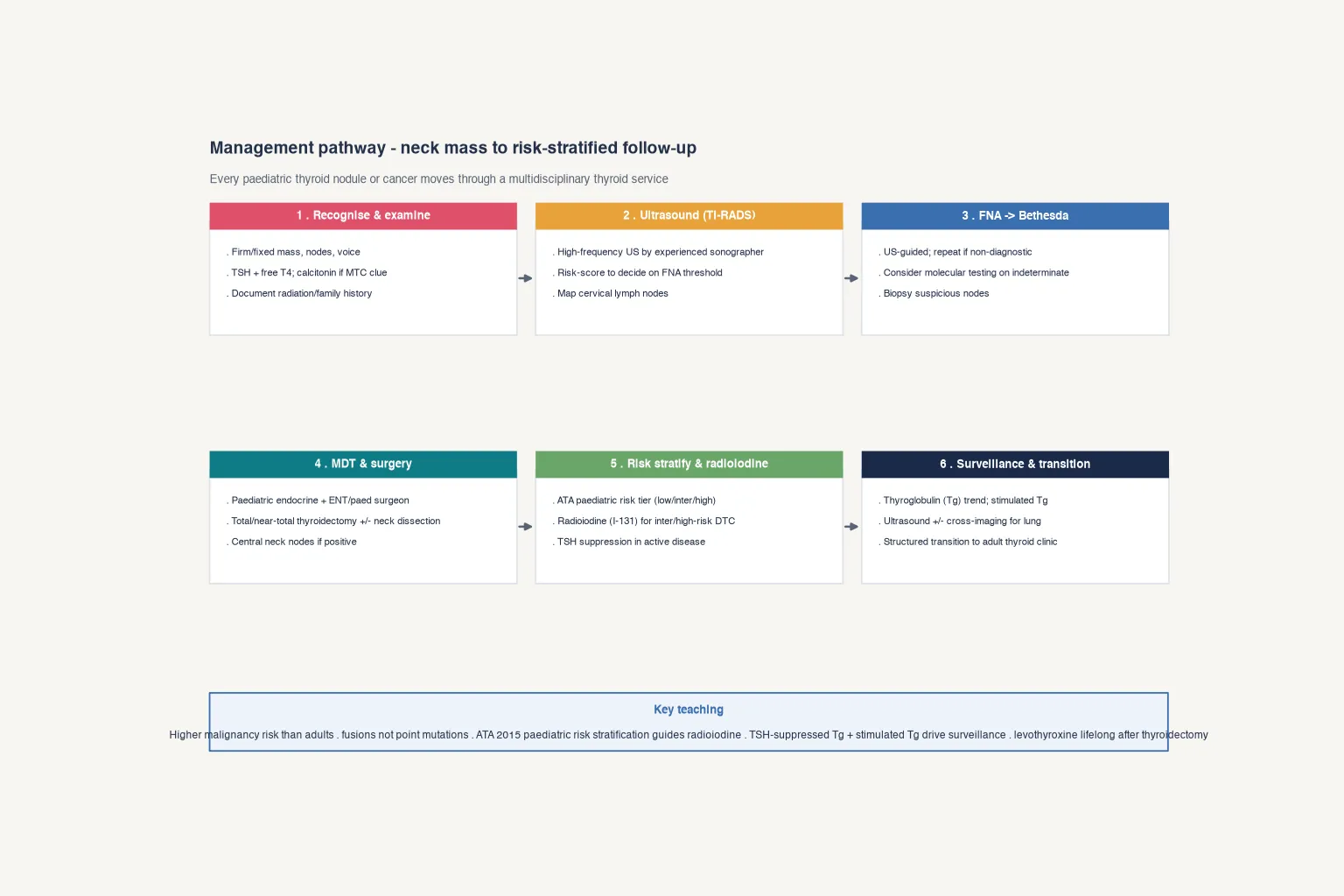
Investigation follows a fixed sequence: thyroid function, structural imaging, then sampling. Thyroid function tests (TSH with reflex free T4, and free T3 if thyrotoxic) come first to establish functional status; a suppressed TSH with a solitary nodule warrants consideration of a hyperfunctioning (almost always benign) nodule, whereas a normal or raised TSH does not exclude malignancy. [1] [5]
High-frequency thyroid ultrasound is the cornerstone structural test. Apply the ACR TI-RADS system to every discrete nodule, recording the features that drive the score (composition, echogenicity, shape, margin, echogenic foci) and the size-based FNA threshold for each tier. Map the cervical lymph nodes in the same study, because suspicious nodes are biopsied alongside the nodule. Ultrasound in children should be performed and reported by experienced sonographers using a paediatric-aware protocol. [2] [3] [16]
Ultrasound-guided fine-needle aspiration samples nodules meeting TI-RADS threshold, reported with Bethesda cytology. Indeterminate Bethesda categories (III and IV) increasingly benefit from molecular testing, which detects fusion events and point mutations that reclassify risk and inform the extent of surgery. Calcitonin is added when medullary carcinoma is a consideration (family history, MEN2, or cytology hinting at C-cell origin). [12] [13] [17]
| Step | Test | Decision it drives |
|---|---|---|
| 1 | TSH (+ free T4 / T3) | Functional status; hyperfunctioning nodule vs structural lesion |
| 2 | High-frequency ultrasound (ACR TI-RADS) | Nodule tier; FNA threshold; node mapping |
| 3 | Ultrasound-guided FNA (Bethesda) | Malignancy risk; surgery vs observation vs molecular test |
| 4 | Molecular testing (indeterminate) | Fusion/mutation; extent of surgery |
| 5 | Calcitonin ± RET testing (if MTC clue) | C-cell origin; genetic counselling |
Cross-sectional imaging (CT or MRI) is reserved for large, fixed or invasive masses, suspected retrosternal extension, or surgical planning where anatomy is distorted; it is not a first-line test for the typical nodule. Routine blood tests beyond thyroid function, and "shotgun" tumour-marker panels, add cost and false leads without changing the pathway. [1]
Management — Resuscitation
A thyroid nodule is rarely a resuscitation problem, but a handful of presentations are genuine emergencies that outrank the diagnostic pipeline. Acute airway compromise from a rapidly enlarging mass or compressive goitre (stridor, positional dyspnoea) needs urgent imaging, anaesthetic and ENT involvement and a secured airway plan before biopsy. Superior vena cava-type obstruction from a large invasive lesion is another immediate threat. [1]
Thyroid storm (thyrotoxic crisis) is the metabolic emergency that can accompany undiagnosed or poorly controlled Graves disease or, rarely, a hyperfunctioning nodule: fever, tachycardia, altered consciousness and multiorgan features need beta-blockade, antithyroid drugs, corticosteroids and supportive care in parallel with the structural workup. The general paediatrician's role in stable nodule presentations is to complete the workup and refer, not to initiate surgery or radioiodine. [1]
Management — Definitive & Stepwise
Definitive care is multidisciplinary and paediatric-specialised. Every child with a confirmed or strongly suspected thyroid malignancy, and most with an indeterminate nodule carrying significant risk, should be managed by a paediatric thyroid multidisciplinary team — paediatric endocrinology, paediatric or ENT surgeon with thyroid expertise, nuclear medicine, pathology, and genetics — because the extent of surgery and the radioiodine decision depend on integrated staging. [9] [17]
Surgery
For confirmed differentiated thyroid carcinoma, total or near-total thyroidectomy is the standard operation, with central and/or lateral neck dissection when nodal disease is present. Surgery should be performed by a high-volume thyroid surgeon because complication rates — recurrent laryngeal nerve injury and hypoparathyroidism — are operator-dependent and carry lifelong consequences in a child. [1] [20]
For medullary carcinoma, the operation is shaped by RET status and disease extent, and prophylactic thyroidectomy is offered to known germline RET carriers at an age determined by the specific RET codon risk class. [13] [21]
Radioiodine and risk stratification
After surgery, paediatric patients are risk-stratified (the 2015 ATA paediatric framework defines low-, intermediate- and high-risk categories) to guide radioactive iodine (I-131) ablation, which is reserved for intermediate- and high-risk differentiated disease rather than applied universally. TSH suppression with levothyroxine is maintained during active disease and relaxed once the patient is in durable remission. [1] [11]
Surveillance
Long-term surveillance hinges on thyroglobulin (Tg) — the serum marker of persistent or recurrent differentiated thyroid disease — interpreted alongside neck ultrasound, with stimulated Tg and cross-sectional or functional imaging when recurrence is suspected. Pulmonary metastases remain radioiodine-responsive and do not by themselves define treatment failure in children. Structured transition to adult thyroid care closes the loop, because the surveillance horizon spans decades. [6] [8]
Australian and New Zealand practice routes paediatric thyroid cancer through quaternary paediatric endocrine and surgical centres with defined shared-care pathways; radioiodine is delivered in licensed nuclear medicine facilities. State the principle in exams — multidisciplinary, paediatric-specialised, risk-adapted — without inventing local form numbers. [1] [9]
Specific Subtypes & Scenarios
Solitary Bethesda VI nodule in an adolescent. Proceed to multidisciplinary surgery after staging ultrasound; total/near-total thyroidectomy with neck dissection for nodal disease, then risk-stratified radioiodine. [1]
Bethesda III/IV indeterminate nodule. Apply molecular testing to detect fusion or mutation events that reclassify risk; surgery (diagnostic lobectomy or total thyroidectomy) follows the molecular probability and family preference within the multidisciplinary team. [12] [17]
Childhood cancer survivor with a new nodule. Treat as high pretest probability; lower the FNA threshold, biopsy promptly, and keep the lesion within a long-term survivorship surveillance program because second thyroid primaries and recurrence risk persist for life. [1] [19]
Known MEN2 / germline RET carrier. Prophylactic thyroidectomy at a codon-determined age, with biochemical (calcitonin) surveillance; refer the family for genetic counselling. [13] [21]
Paediatric medullary thyroid carcinoma. Calcitonin-based diagnosis, RET testing, total thyroidectomy with central node dissection, and lifelong calcitonin and CEA surveillance; radioiodine and Tg are irrelevant to C-cell disease. [13] [14]
Persistent neck nodal disease after initial treatment. Options include re-operative neck dissection and, for selected lesions, percutaneous ethanol ablation of neck node metastases, which has shown long-term control in paediatric papillary carcinoma series. [8]
Large compressive benign multinodular goitre. Surgery (subtotal or total thyroidectomy) for pressure symptoms or cosmetic concern after excluding malignancy; levothyroxine suppression is not recommended as routine medical therapy for benign nodular disease. [1] [20]
Rural or remote family. Coordinate imaging and FNA locally where safe, but centralise surgery and radioiodine at the paediatric thyroid centre; telehealth supports follow-up and surveillance once the acute phase is managed. [9]
Complications & Pitfalls
Classic errors include reassuring that "children rarely get thyroid cancer" without imaging a real nodule; biopsying a hyperfunctioning nodule (almost always benign) without first checking TSH; over-calling Bethesda IV as diagnostic of follicular carcinoma when histology is required; performing thyroidectomy by a low-volume surgeon and inflicting lifelong hypoparathyroidism or vocal cord palsy; and applying adult radioiodine thresholds indiscriminately to children whose risk-adapted framework is distinct. [1] [20]
Equally damaging is missing the syndromic context: a "sporadic" medullary carcinoma that is actually germline RET/MEN2 delays prophylactic thyroidectomy in at-risk younger siblings; a DICER1 or PTEN family history changes surveillance for the proband and relatives. Always ask, and always offer genetic counselling when the histology or family history warrants it. [13] [21]
Long-term, the hazards shift toward overtreatment and surveillance burden: unnecessary radioiodine, excessive TSH suppression, and cumulative imaging without a documented benefit. A balanced, risk-adapted plan — and a clean transition to adult care — protects the patient from both under-treatment and the late effects of over-treatment. [6] [17]
Prognosis & Disposition
Paediatric differentiated thyroid carcinoma carries an excellent prognosis — long-term disease-specific survival is very high even in the presence of nodal or pulmonary disease — because children present with more extensive but more radioiodine-responsive tumours than adults. This favourable natural history justifies a risk-adapted rather than maximally aggressive approach to radioiodine and TSH suppression. [7] [11]
Medullary carcinoma has a less favourable prognosis driven by stage at diagnosis and RET status, which is why prophylactic thyroidectomy in known carriers and early detection matter so much. [13] [14]
Disposition follows the disease: low-risk DTC moves toward shared surveillance with the primary paediatrician and a defined transition; intermediate- and high-risk disease stays within the specialist centre for stimulated Tg, selective imaging and re-treatment decisions. Define response by structural and biochemical remission (undetectable Tg, negative imaging), not by a single postoperative scan. [1] [6]
Special Populations
Childhood cancer survivors carry the highest nodule and cancer risk because of prior radiation; they need protocolised ultrasound surveillance and a low threshold for FNA. Syndromic families (DICER1, PTEN, FAP, Carney complex, MEN2) require cascade genetic counselling and gene-specific surveillance, including prophylactic surgery for RET carriers. [13] [19] [21]
Adolescents approaching transition need a structured handover to adult thyroid services — documented diagnosis, surgical and radioiodine history, current Tg trend, imaging plan and levothyroxine regimen — because loss to follow-up during transition is a well-described source of late recurrence detection. [6]
Rural, remote and Indigenous families face access barriers to paediatric thyroid surgery and nuclear medicine; care should be centralised for the index operation but supported by local and telehealth follow-up, with cultural safety and interpreter use where relevant. Migrant and refugee families may arrive from iodine-deficient regions with goitre, or with incomplete cancer histories — take a careful cross-border radiation and family history. [1] [9]
Evidence, Guidelines & Regional Differences
The foundational document remains the 2015 American Thyroid Association paediatric guideline (Francis and colleagues), which set the structure for risk-adapted surgery, selective radioiodine and Tg-based surveillance. The ACR TI-RADS white paper and user's guide standardised ultrasound triage, while comparison and validation studies have tested TI-RADS and other systems specifically in paediatric cohorts. [1] [2] [15] [16]
Molecular and epidemiological work has refined the picture: large series describe the landscape and predictors of invasive paediatric DTC, fusion-based molecular signatures associate with aggressive histology, and registry data document the rising incidence in adolescents and young adults. Medullary carcinoma is governed by the ATA RET/MTC guideline and by long-term MEN2 natural-history data. [10] [11] [13] [19] [21]
RISK-S
Guideline one-liner. ATA 2015 paediatric guidance structures the whole pathway — recognise, image with TI-RADS, biopsy with Bethesda, operate in a multidisciplinary team, risk-stratify for radioiodine, and surveil with thyroglobulin. [1]
Paediatric-vs-adult one-liner. Children carry roughly double the malignancy risk, present with larger primaries and more nodal/lung disease, are driven by gene fusions rather than BRAF V600E, yet survive far better and respond briskly to radioiodine. [4] [7] [12]
Contemporary consensus statements also emphasise the structure and priorities of multidisciplinary paediatric thyroid programs, reinforcing that the centre — not the individual clinician — is the unit of safe care. [9] [17]
Exam Pearls
Self-test: adolescent with a firm thyroid nodule
Measure TSH and free T4; perform high-frequency ultrasound applying ACR TI-RADS and mapping nodes; FNA any nodule meeting threshold (here likely TR4 ≥1.5 cm or TR5 ≥1 cm) with Bethesda cytology; add molecular testing if indeterminate; refer confirmed or suspicious malignancy to a paediatric thyroid multidisciplinary team for risk-adapted surgery, selective radioiodine and Tg-based surveillance; plan transition. [1] [2] [9]
References
- [1]Francis GL Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid, 2015.PMID 25900731
- [2]Tessler FN ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. Journal of the American College of Radiology, 2017.PMID 28372962
- [3]Tessler FN Thyroid Imaging Reporting and Data System (TI-RADS): A User's Guide. Radiology, 2018.PMID 29558300
- [4]Vergamini LB Increase in the incidence of differentiated thyroid carcinoma in children, adolescents, and young adults: a population-based study. The Journal of Pediatrics, 2014.PMID 24630354
- [5]Goldfarb M Differences in the management of thyroid nodules in children and adolescents as compared with adults. Current Opinion in Endocrinology, Diabetes and Obesity, 2022.PMID 35777975
- [6]Goldfarb M Survivorship, Quality of Life, and Transition to Adult Care for Pediatric and Adolescent Thyroid Cancer. Thyroid, 2022.PMID 36193568
- [7]Hay ID Papillary Thyroid Carcinoma (PTC) in Children and Adults: Comparison of Initial Presentation and Long-Term Postoperative Outcomes. World Journal of Surgery, 2018.PMID 29030676
- [8]Hay ID Long-term Effectiveness of Ethanol Ablation in Controlling Neck Nodal Metastases in Childhood Papillary Thyroid Carcinoma. Journal of the Endocrine Society, 2023.PMID 37388573
- [9]Kothari R Composition and Priorities of Multidisciplinary Pediatric Thyroid Programs: A Consensus Statement. Thyroid, 2025.PMID 39950999
- [10]Mollen KP Unique Molecular Signatures Are Associated with Aggressive Histology in Pediatric Differentiated Thyroid Carcinoma. Thyroid, 2022.PMID 34915753
- [11]Wasserman JD The Landscape of Pediatric Differentiated Thyroid Carcinoma and Predictors of Invasive Disease. The Journal of Clinical Endocrinology and Metabolism, 2026.PMID 42025318
- [12]Spaulding SL Molecular Genetics Augment Cytopathologic Evaluation and Surgical Planning of Pediatric Thyroid Nodules. Journal of Pediatric Surgery, 2024.PMID 38246817
- [13]Wells SA Jr Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid, 2015.PMID 25810047
- [14]Hensley SG Pediatric Medullary Thyroid Carcinoma: Clinical Presentations and Long-Term Outcomes. The Journal of Clinical Endocrinology and Metabolism, 2024.PMID 38441533
- [15]Yu J Comparison of ultrasound risk stratification systems for pediatric thyroid nodules. Frontiers in Endocrinology, 2024.PMID 38572472
- [16]Srivatsa S Assessing the Diagnostic Accuracy of TI-RADS in Pediatric Thyroid Nodules: A Multi-Institutional Study. Journal of Pediatric Surgery, 2025.PMID 39358076
- [17]Pillai SS Evolving trends in pediatric thyroid nodules and cancer management. Annals of Pediatric Endocrinology and Metabolism, 2026.PMID 42415554
- [18]Gest-Laurent M Clinical, Radiologic and Cytologic Predictors of Malignancy in Pediatric Thyroid Nodules. Head & Neck, 2026.PMID 42403156
- [19]Scott AR Trends in Cancer Incidence in US Adolescents and Young Adults, 1973-2015. JAMA Network Open, 2020.PMID 33258907
- [20]Bukarica S Thyroid Surgery in Children: A 5-Year Retrospective Study at a Single Paediatric Institution. Children, 2022.PMID 36553262
- [21]Castinetti F Natural history, treatment, and long-term follow up of patients with multiple endocrine neoplasia type 2. The Lancet Diabetes and Endocrinology, 2019.PMID 30660595