Paeds · investigations-procedures-and-technology
Abscess drainage and minor procedures
Also known as Incision and drainage · I and D · Cutaneous abscess drainage · Loop drainage technique · Minor surgery in children · Skin and soft tissue infection drainage
Fellowship guide to abscess drainage and minor surgical procedures in children. Covers the bedside decision between a drainable cutaneous abscess, cellulitis and a necrotising soft tissue infection that must never be loosely drained; the loop drainage technique and its superiority over classical incision and drainage with packing in larger abscesses; the safe maximum doses of plain lidocaine (3 mg/kg) and lidocaine with adrenaline (7 mg/kg) and of bupivacaine (2 mg/kg); the indications for adjuvant antibiotics after drainage and the empiric choice of cephalexin, clindamycin or trimethoprim-sulfamethoxazole for suspected MRSA; the red flags of necrotising fasciitis that mandate urgent surgical referral; and the common minor procedures of paediatrics including paronychia drainage, ingrown toenail wedge resection with phenolisation, foreign body removal and suture removal timing, with their analgesia, technique and aftercare.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
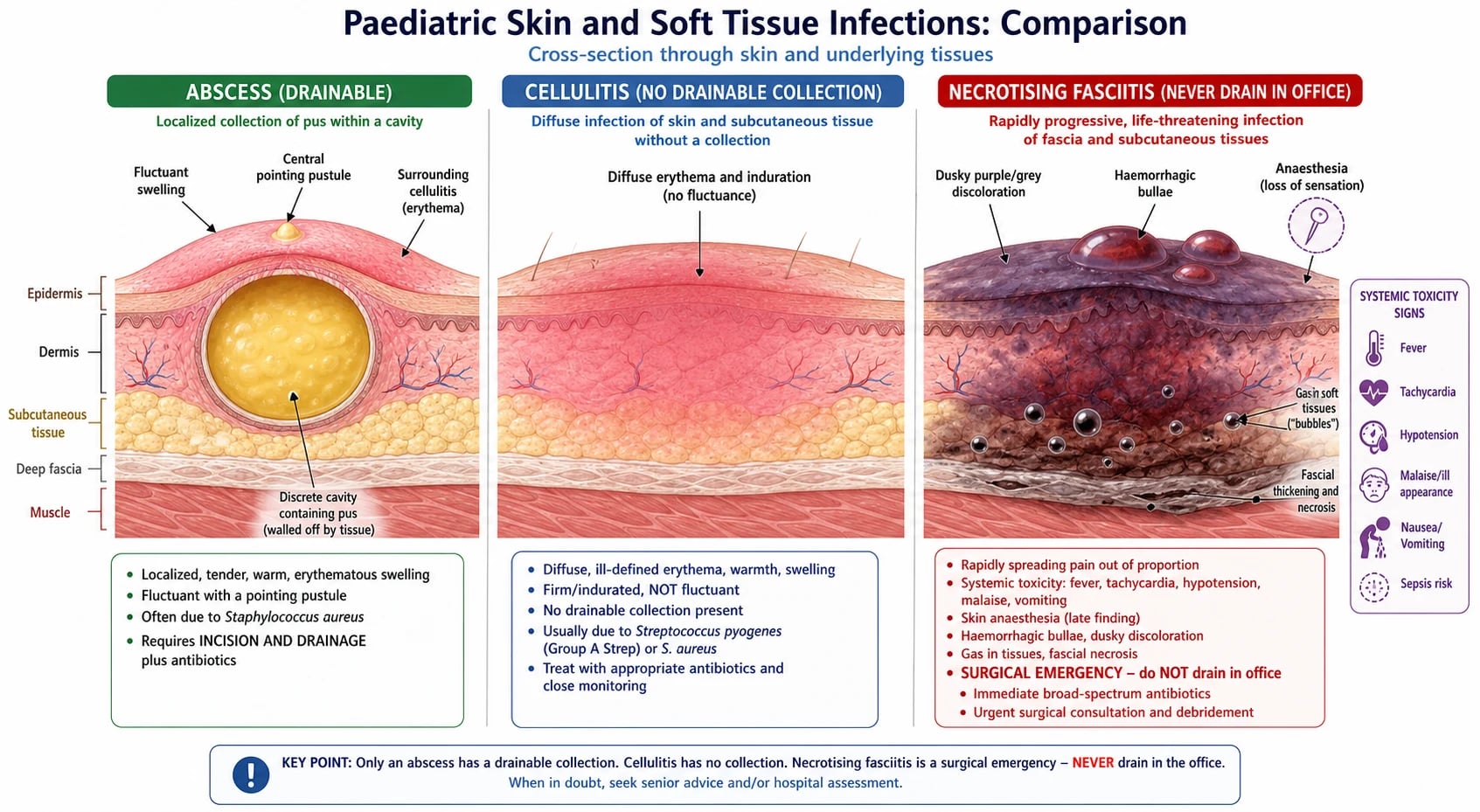
Picture the five-year-old who comes in with a tender, red, domed lump on the thigh that has been growing for three days and now has a yellow pointing centre. The parent asks whether it needs to be "popped". The decision the registrar must make at the bedside is the one this page exists to teach: is this a drainable abscess, in which case incision and drainage relieves the pain and cures the infection; is it cellulitis without a collection, in which case drainage does nothing and antibiotics are the treatment; or is it a necrotising soft tissue infection, in which case office drainage is dangerous and the child needs urgent surgical exploration? [1] [2]
A cutaneous abscess is a localised collection of pus within the dermis and subcutaneous tissue, walled off by a rim of inflamed granulation tissue called the pyogenic membrane. The pus itself is avascular — a mixture of viable and dying neutrophils, necrotic debris and bacteria — which is why systemic antibiotics cannot sterilise an established abscess and why the cavity must be opened, unroofed, and left to heal by secondary intention. Incision and drainage (I&D) is the deliberate opening of the cavity, the breakdown of internal loculations, and the evacuation of pus; the modern variant is the loop drainage technique, in which a small silicone vessel loop is passed through two stab incisions and tied with light tension to keep the cavity open as it heals. [2] [6]
What makes paediatric abscess drainage a distinct skill from adult drainage is the child's pain tolerance, the smaller body that makes local anaesthetic overdose a real risk, the atypical organisms of the neonate, and the developmental stage that determines whether the procedure is done awake with topical anaesthesia, under nitrous, or under dissociative sedation. The fellowship skill being tested is reading the child, recognising the abscess that can be drained safely in the office versus the one that needs theatre, calculating the safe dose of local anaesthetic in milligrams from the weight in kilograms, and completing a calm, complete drainage that does not need to be repeated. [1] [7]
Classification
Sort an abscess by what is in it, by how big and deep it is, and by where it sits, because each axis changes the technique, the anaesthesia, and the team. [1] [2]
By pathogen, the commonest organism in a paediatric cutaneous abscess is Staphylococcus aureus, including community-acquired methicillin-resistant S. aureus (CA-MRSA) in many regions; Streptococcus pyogenes (group A strep) is the second commonest, and anaerobes and enteric gram-negatives join the picture in perineal, perianal and head-and-neck sites. The Panton-Valentine leucocidin (PVL) toxin carried by some S. aureus strains is associated with larger, recurrent and more necrotising abscesses. [3] [5]
By drainage strategy, a simple I&D with light packing suits a small single-cavity abscess under about 5 cm; the loop drainage technique — two small stab incisions joined by a silicone vessel loop tied with tension — is preferred for larger, multi-loculated or thick-walled abscesses, where the systematic review evidence shows it has lower failure and recurrence rates than packing; needle aspiration is reserved for the small, tense, fluctuant collection and for abscesses where an incision is best avoided, such as a breast abscess in a lactating adolescent where a needle under ultrasound preserves the breast parenchyma. [2] [11]
By site, a limb or trunk abscess is straightforwardly drained in the treatment room; a perianal abscess in a male infant is drained at the mucocutaneous junction but managed conservatively first because most resolve; a breast abscess in an adolescent or neonate is aspirated under ultrasound where possible; a peritonsillar or deep neck abscess needs ear, nose and throat or surgical assessment and is never a treatment-room procedure in a small child. [10]
The numbers that anchor your viva
Epidemiology & Risk Factors
Skin and soft tissue abscesses are among the commonest reasons a child presents to an emergency or primary care service, and they are one of the commonest procedural indications in paediatric practice. The risk of a recurrent or severe abscess rises with MRSA colonisation, atopic dermatitis with an impaired skin barrier, immunocompromise (primary immunodeficiency, oncology, transplant), diabetes, obesity, varicella, an indwelling device, and the social determinants of skin care. [1] [3]
Community-acquired MRSA has reshaped the epidemiology of paediatric SSTI since the early 2000s. In regions where CA-MRSA is endemic — much of Australia, Aotearoa New Zealand, North America and parts of the United Kingdom — it is now the dominant cause of cutaneous abscess, and the empiric antibiotic choice must reflect local resistance patterns. The lesson is that empiric therapy is a regional decision, not a universal one. [3] [5]
A specific epidemiological point that examiners test is the perianal abscess of male infants under one year. Most of these present as a tender, fluctuant swelling at the anal margin, the majority resolve or heal after a single simple drainage, and only the minority that develop a communicating fistula-in-ano need surgical referral. The conservative-first approach is well supported by recent narrative review evidence. [10]
A second point is the post-pandemic rise in paediatric head and neck abscesses — a measurable increase in peritonsillar, retropharyngeal and parapharyngeal abscesses after the COVID-19 era, attributed to altered pathogen exposure. This is a useful viva "current evidence" point but does not change the procedural principle. [1]
Pathophysiology
The teaching model runs from the shape of the abscess cavity to the reason a cavity that has been opened must be left open, and it rests on a single fact: pus is avascular. [1] [6]
A cutaneous abscess begins when bacteria — usually S. aureus or S. pyogenes — gain entry through a break in the skin barrier (a fissure, an insect bite, an atopic dermatitis flare, a hair follicle) and multiply in the dermis or subcutaneous tissue. The host neutrophil response walls off the infection with a rim of granulation tissue — the pyogenic membrane — and the centre becomes a cavity of pus: viable and dying neutrophils, necrotic debris, and bacteria. Because no blood vessel penetrates the pus itself, systemically delivered antibiotics cannot reach therapeutic concentrations inside the cavity; this is why an established abscess does not respond to antibiotics alone, and why the cavity must be opened and unroofed. [1] [6]
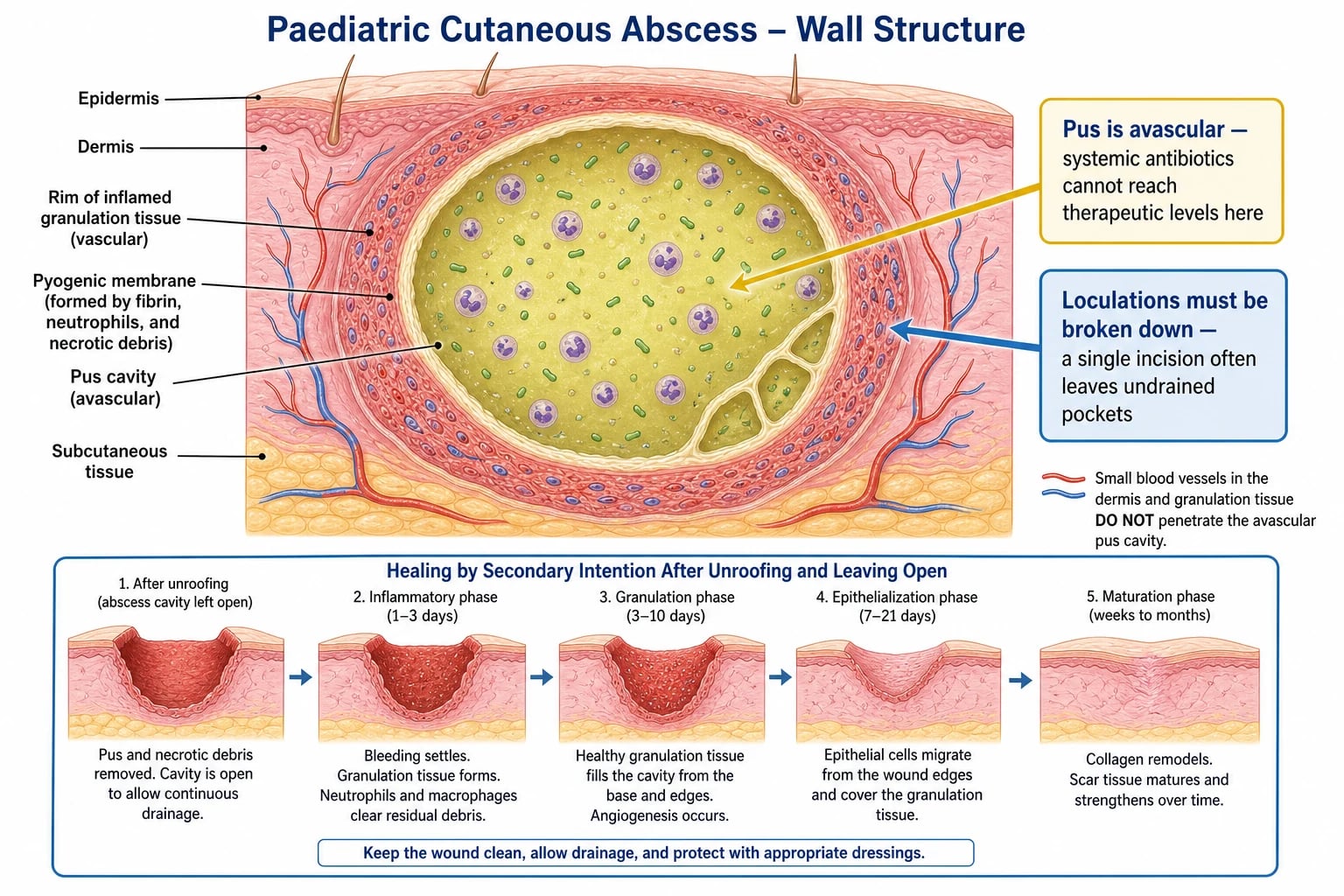
A second feature of the cavity is loculation: the pus is rarely a single open pool but is divided by fibrinous septa into multiple small pockets. A single linear incision that does not break these loculations leaves undrained pus behind, and the abscess recurs. This is why the disciplined operator palpates the cavity with a finger or a haemostat and breaks every septum before closing the case. [1] [2]
The local anaesthetic pharmacology is the second mechanism the fellowship candidate must own. The amide local anaesthetics (lidocaine, bupivacaine, ropivacaine) are weak bases that cross the nerve membrane in their un-ionised form and block sodium channels from inside. Inflamed, infected tissue is acidic (pH around 6), and the acidic environment ionises more of the anaesthetic, so less crosses the membrane — which is why local anaesthetic works poorly in the wall of a septic abscess. Adrenaline (epinephrine) causes local vasoconstriction, slows systemic absorption, and raises the maximum safe dose — from 3 mg/kg for plain lidocaine to 7 mg/kg for lidocaine with adrenaline. The historical and now-discredited teaching that adrenaline must never be used in digits, nose or penis comes from old studies of high-concentration adrenaline with chlorhexidine or cocaine preservatives; modern low-dose adrenaline with lidocaine is widely used and safe for digital blocks, although the conservative exam answer in a child remains a plain lidocaine digital block. [1] [12]
Clinical Presentation
The presenting feature of a drainable abscess is a tender, erythematous, fluctuant swelling, often with a central pustule that has begun to "point". The overlying skin is warm, the child guards the area, and there is often regional lymphadenopathy. A pointing pustule indicates that the pus is close to the surface and is the natural place to make the incision. The history is usually of a lump that grew over days, became more painful, and may have ruptured spontaneously. [1] [2]
The trap is the child whose presentation is not a simple abscess. The four dangerous patterns to recognise are a rapidly progressing, exquisitely tender swelling with skin that looks worse than the lump itself; a child who is systemically unwell out of proportion to the visible infection; a periorbital or orbital collection that threatens the eye; and an immunocompromised child in whom the usual signs are blunted. Each of these changes the urgency, the team, and the location of the procedure. [1]
The red flags of necrotising fasciitis are the single most important bedside discriminator in paediatric SSTI, and the candidate must be able to list them without hesitation. They are: pain out of proportion to the visible skin findings; induration extending beyond the visible margins of erythema; skin anaesthesia (the infected cutaneous nerves have infarcted); crepitus from gas-forming organisms; a rapidly evolving course over hours; systemic toxicity with tachycardia, hypotension or an altered conscious state; and skin changes of grey or dusky discolouration, haemorrhagic bullae, or frank necrosis. A child with any of these is not a treatment-room candidate — they need urgent surgical consultation, blood cultures, empiric intravenous antibiotics, imaging if time allows, and theatre. [1] [1]
| Pattern | What it is | What it dictates |
|---|---|---|
| Tender fluctuant lump with pointing pustule | Drainable cutaneous abscess | Treatment-room I&D or loop drainage; send pus for culture; antibiotics only if indicated |
| Diffuse warmth and induration without fluctuance | Cellulitis without collection | Antibiotics (oral if well, IV if unwell); no drainage |
| Pain out of proportion, rapidly evolving, systemic toxicity | Necrotising fasciitis until proven otherwise | Urgent surgical referral, IV fluids, empiric IV antibiotics, imaging, theatre — never drain in the office |
| Fluctuant swelling in a lactating adolescent | Breast abscess | Ultrasound-guided needle aspiration; continue breastfeeding; convert to I&D only if recurrent |
| Fluctuant perianal swelling in a male infant under 1 year | Perianal abscess | Conservative first; simple drainage at the mucocutaneous junction; surgical referral only if a fistula develops |
The child's developmental stage and pain tolerance are part of the clinical presentation because they determine the analgesia and the setting. A neonate tolerates a small procedure with oral sucrose, a dummy and containment; an infant or young child needs topical anaesthesia and a calm parent present; a school-age child can usually cooperate with a clear explanation and a digital block; an anxious or uncooperative child needs nitrous or dissociative sedation by a trained team with full monitoring. [7] [8]
Differential Diagnosis
The differential at the bedside is not "what bug" but what is this lump, and is it safe to drain. Frame the decision around four questions and the right answer follows. [1] [2]
Drainable abscess
drain it
- Fluctuance on palpation; pointing pustule; surrounding cellulitis; regional lymphadenopathy
- Bedside ultrasound confirms a hypoechoic collection
- I&D or loop drainage with appropriate analgesia
- Send pus for culture; antibiotics only if indicated
Cellulitis (no collection)
- Diffuse warmth, erythema, induration; no fluctuance
- Bedside ultrasound shows cobblestoning or no discrete collection
- Antibiotics are the treatment; drainage does nothing
- Mark the margins and review at 24–48 h for failure to respond
Necrotising fasciitis
- Pain out of proportion; rapidly evolving; skin anaesthesia; crepitus
- Grey or dusky skin, haemorrhagic bullae, systemic toxicity
- Never drain in the office; urgent surgical referral
- IV fluids, empiric IV antibiotics (vancomycin or clindamycin + a beta-lactam + gram-negative cover), imaging, theatre
Not an abscess — do not drain
- Vascular malformation, haemangioma, thrombosed vein
- Mycotic aneurysm, necrotic tumour, hernia
- Aspirate or image first if there is any doubt
- Draining causes catastrophic bleeding or tumour seeding
A second layer of differential is what kind of abscess. An infected epidermoid (sebaceous) cyst has a central punctum and a history of a longstanding subcutaneous lump that has now become inflamed; drainage in the acute phase relieves the infection, but definitive excision of the cyst wall must wait until the inflammation has settled. A pilonidal abscess in an adolescent sits in the natal cleft and demands drainage with consideration of definitive surgical excision later. A hidradenitis suppurativa lesion sits in the axilla, groin or buttock and is part of a chronic relapsing pattern that needs dermatology, not a single drainage. A paronychia sits at the nail fold, often with a subungual extension that requires partial nail removal. [1] [9]
A third differential is the perianal mass in an infant. A perianal abscess sits at the anal margin and is fluctuant; an anal fissure is a painful linear tear with bright bleeding on defecation; a thrombosed haemorrhoid is rare in an infant and should prompt consideration of portal hypertension; and in any case of unexplained perianal findings, non-accidental injury must be considered and the safeguarding pathway followed if the history and findings do not fit. [10]
Clinical & Bedside Assessment
Assessment before drainage is short, structured and explicit: it asks four questions, names the answer to each, and either proceeds, defers, or escalates. The aim is never to be surprised once the drape is on. [1]
Begin with a focused history and examination. Ask about the onset, the rate of progression, prior episodes (recurrent SSTI suggests MRSA colonisation or an immunocompromise), predisposing conditions (atopic dermatitis, diabetes, immunosuppression), and systemic symptoms (fever, rigors, malaise suggest more than a simple abscess). Examine the lump for fluctuance (the cardinal sign of a drainable collection), a pointing pustule (the natural incision site), surrounding cellulitis (mark the margins with a pen), and regional lymphadenopathy. Examine the child as a whole for signs of systemic toxicity — tachycardia, hypotension, an altered conscious state — that change the setting from a treatment room to theatre. [1] [2]
Use bedside ultrasound whenever the clinical picture is uncertain. A hypoechoic, often loculated collection with posterior acoustic enhancement confirms a drainable abscess; cobblestoning of the subcutaneous fat without a discrete collection suggests cellulitis; and a thickened, oedematous soft tissue layer with gas locules and fluid tracking along fascial planes is the ultrasonographic clue to necrotising fasciitis. Ultrasound also estimates the abscess volume and identifies the deepest pocket for drainage. A practical teaching from the Neal 2026 study is that the expressed abscess volume is systematically less than the operator estimated before drainage, so the operator should plan the incision, the loculation breakdown, and the follow-up on the assumption that there is more pus than appears obvious. [11]
Check the red flags of necrotising fasciitis explicitly before draining anything: pain out of proportion, induration beyond the margins, skin anaesthesia, crepitus, rapidly evolving course, systemic toxicity, and grey or dusky skin or haemorrhagic bullae. If any are present, escalate rather than drain. The LRINEC score (CRP, white cell count, haemoglobin, sodium, creatinine, glucose) is a laboratory adjunct that has been validated in adults but has important limitations in children and should not replace clinical judgement — a necrotising infection can be present with a low LRINEC score. [1] [1]
Assess the child's likely tolerance of the procedure and plan the analgesia accordingly. Calculate the weight-based maximum local anaesthetic dose before the procedure and write it on the drape; a 10 kg infant's plain lidocaine limit is 30 mg, which is 3 mL of one-percent lidocaine — a tiny volume that is easily exceeded by an operator who is not thinking in milligrams per kilogram. Document consent, including assent for the older child, and plan the post-procedure review. [1] [12]
The pre-drainage checklist
Is this a drainable abscess, cellulitis, or a necrotising infection? → if necrotising, stop and refer
Is the child systemically well enough for a treatment-room procedure? → if septic or shocked, resuscitate and escalate
Have I calculated the weight-based local anaesthetic dose in mg before drawing it up? → if not, do it now
Is the developmental stage and pain tolerance matched to the analgesia plan (topical, infiltration, nitrous, dissociative sedation)?
Have I marked the incision over the pointing pustule, planned to break loculations, and chosen between packing and a loop?
Have I documented consent, prepared a pus pot for culture, and planned a 24 to 48 hour review?
Investigations
Most simple paediatric cutaneous abscesses need no investigations before drainage. The diagnosis is clinical, and the treatment is mechanical. The role of investigations is to recognise the complicated or atypical case, to guide antibiotics when they are needed, and to plan the drainage of a deep or uncertain collection. [1] [6]
Send pus for culture in every drained abscess. The result guides antibiotics if there is recurrence, worsening, or a complicated course, and the local MRSA prevalence drives empiric choice. A Gram stain and culture with susceptibility testing is the minimum; in the immunocompromised child, add an acid-fast bacillus culture and a fungal culture, and lower the threshold for biopsy of atypical or non-healing lesions. [3] [5]
Blood tests are reserved for the child who is systemically unwell, immunocompromised, or at the severe end of the SSTI spectrum. A full blood examination, C-reactive protein, electrolytes and a blood culture are the standard panel for the child receiving intravenous antibiotics for a severe SSTI; serial CRP helps track response. A glucose and an HbA1c may unmask diabetes in a child with recurrent abscesses. In the well child with a simple abscess, none of these are needed. [1] [1]
Bedside ultrasound is the imaging modality of choice for the typical cutaneous abscess, and is increasingly performed by the treating paediatrician or emergency physician. It confirms the collection, estimates the volume, identifies loculations, and guides needle aspiration of a deep or small collection. A formal ultrasound or an MRI is reserved for a suspected deep neck space, retropharyngeal, pilonidal, or perianal abscess where the anatomy is complex, the drainage is surgical, and the imaging guides the operative approach. A CT is occasionally needed in the unstable child with a suspected necrotising infection where MRI would delay theatre. [11] [1]
Management — Resuscitation
When a child presents with a large or rapidly progressing SSTI with systemic toxicity, the priority is resuscitation and urgent surgical referral — not drainage. The ordered bundle is airway, breathing, circulatory access, a blood culture, and empirical intravenous antibiotics, with analgesia, fluid resuscitation for shock, and an urgent surgical opinion. [1] [1]
The single most important resuscitation principle in suspected necrotising fasciitis is that office incision and drainage is contraindicated. The child needs urgent surgical exploration in theatre, where the necrotic tissue is excised back to healthy bleeding tissue and the extent of the infection is defined. Empirical intravenous antibiotics are given immediately after a blood culture: a regime for a child covers a beta-lactam (such as piperacillin-tazobactam or a third-generation cephalosporin) plus MRSA cover (vancomycin or clindamycin) plus group A streptococcal and toxin suppression (clindamycin), with the addition of an antitoxin agent (intravenous immunoglobulin) in severe toxin-mediated disease. The antibiotic plan is adjusted once cultures and susceptibilities return. [1] [1]
Empirical intravenous antibiotics for severe paediatric SSTI with suspected MRSA (ANZ / NICE / IDSA)
If local anaesthetic systemic toxicity (LAST) develops during infiltration — early perioral tingling, metallic taste, agitation, progressing to seizures and cardiovascular collapse — stop injecting immediately, call for senior and anaesthetic help, secure the airway and breathing, give intralipid 20 percent (1.5 mL/kg bolus, then 15 mL/kg/h infusion by the local lipid-rescue protocol), and prepare for a prolonged cardiovascular resuscitation because bupivacaine in particular binds cardiac sodium channels and the toxicity can be refractory. The discipline that prevents LAST is the weight-based dose calculation, aspiration before every injection, and slow injection. [12]
For a peritonsillar or retropharyngeal abscess that threatens the airway, the priority is airway, breathing and urgent ear, nose and throat or anaesthetic assessment; drainage is performed by the specialist team in a controlled setting once the airway is safe. [1]
Management — Definitive & Stepwise
Once the bedside assessment has settled the diagnosis and excluded the red flags, the procedure itself is an ordered sequence that should run the same way every time: consent, preparation, analgesia, skin preparation, incision, loculation breakdown, drainage, packing or loop, dressing, and aftercare. [1] [2]
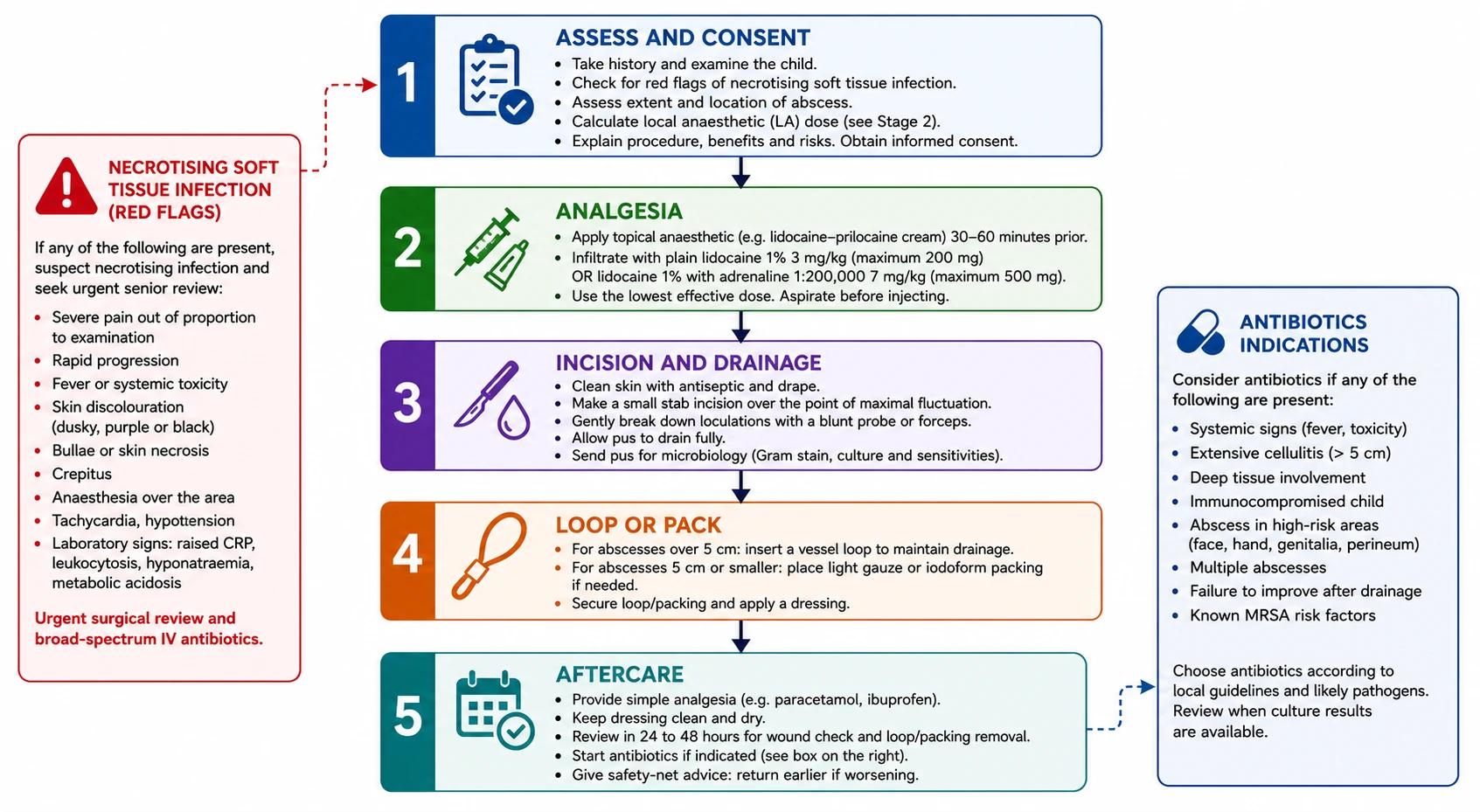
Begin with consent and analgesia. Explain to the parent and, where developmentally appropriate, the child, what the procedure involves, the common discomforts (local pain, pressure, the sight and smell of pus), the serious but rare risks (bleeding, recurrence, scarring, infection, local anaesthetic toxicity), and the alternatives. Document the consent. Apply a topical anaesthetic at the planned incision site early — EMLA (eutectic lidocaine 2.5% and prilocaine 2.5%) under an occlusive dressing for at least 60 minutes, or amethocaine 4% (Ametop) for 30 to 45 minutes — and plan the procedural sedation if needed (nitrous 50/50 by trained staff, or intranasal fentanyl or ketamine by the local protocol) with full monitoring. [7] [8]
Calculate the weight-based local anaesthetic dose before you draw it up. For plain lidocaine the maximum is 3 mg/kg; for lidocaine with adrenaline it is 7 mg/kg; for bupivacaine it is 2 mg/kg (3 mg/kg with adrenaline). A one-percent lidocaine solution contains 10 mg per mL, so a 12 kg toddler's plain lidocaine limit is 36 mg, which is 3.6 mL — write the number on the drape and do not exceed it. Infiltrate slowly around the abscess wall, aspirating before each injection to avoid intravascular delivery; remember that local anaesthetic works poorly in acidic, inflamed tissue, so do not expect perfect anaesthesia of the abscess wall, and do not chase it by exceeding the dose. [1] [12]
DRAIN-IT
Under sterile conditions, make the incision. The classic teaching is a small linear incision over the pointing pustule, along the skin tension lines where possible to minimise scarring; for the loop technique two small stab incisions are made at opposite ends of the cavity. The incision must be large enough to allow complete drainage — a too-small incision is one of the commonest reasons for failure. Express the pus, send a sample in a sterile container for Gram stain, culture and susceptibility, and break the loculations by passing a finger or a blunt haemostat around the cavity and dividing every septum. This step is the single most important determinant of whether the abscess will recur. [2] [11]
Choose between light packing and a loop. For a small single-cavity abscess, light packing with iodoform ribbon or a calcium alginate wick holds the cavity open and prevents premature skin closure; the packing is removed or replaced at 24 to 48 hours. For a larger abscess — typically over about 5 cm, or any thick-walled or multi-loculated cavity — the loop drainage technique is preferred. The systematic review and meta-analysis by Gottlieb and colleagues in 2021 showed that the loop technique reduced the need for a secondary procedure and the recurrence rate compared with packing, without increasing complications. The technique is to make two small stab incisions at the poles of the abscess, pass a vessel loop through the cavity with a haemostat, and tie it with light tension over the skin; the loop stays in place for several days to a week and keeps the cavity open as it heals by secondary intention, then is removed in the outpatient review. [2]
For a breast abscess in a lactating adolescent or neonate, ultrasound-guided needle aspiration is preferred over an incision wherever possible, because it preserves the breast parenchyma and the lactating ducts; the adolescent continues to breastfeed or express from the affected side. Repeated aspirations may be needed, and conversion to I&D is reserved for an abscess that recurs despite aspiration or is too thick to aspirate. [1]
For a perianal abscess in a male infant under one year, the conservative-first approach is well supported: most abscesses resolve or heal after a single simple drainage at the mucocutaneous junction, and only the minority that develop a communicating fistula-in-ano need surgical referral. The family is counselled that a perianal fistula in an otherwise well male infant is a different entity from adult fistula-in-ano and is usually managed expectantly. [10]
Handle the incomplete drainage, the uncooperative child, and the recurrence deliberately. An incomplete drainage — the cavity has not been fully unroofed, the loculations have not been broken, or the incision was too small — presents as ongoing pain, swelling, and a failure to settle; the answer is a repeat drainage with attention to technique. An uncooperative child is best managed by stopping, regrouping, and returning with adequate sedation rather than fighting the child through an inadequate procedure. A recurrence is the cue to ask about MRSA colonisation, to culture the pus, and to consider an underlying epidermoid cyst or a fistula. [1] [2]
Specific Subtypes & Scenarios
The approach to drainage changes with the abscess and the child, and the fellowship candidate must adjust the technique and the timing to the subtype in front of them. [1] [2]
The breast abscess in a lactating adolescent presents with a tender, fluctuant, often erythematous lump in an actively breastfeeding young person. The preferred management is ultrasound-guided needle aspiration with culture of the aspirate, continued breastfeeding or expression from the affected side, and oral antibiotics active against S. aureus; conversion to I&D is reserved for an abscess that recurs despite two or three aspirations or is too thick to aspirate. A neonatal breast abscess — usually from S. aureus or, in the very young infant, group B streptococcus or Escherichia coli — is managed with inpatient intravenous antibiotics and needle aspiration or a small incision, with attention to preserving the breast bud. [1]
The perianal abscess in a male infant under one year presents as a tender, fluctuant swelling at the anal margin, sometimes with visible discharge. The conservative-first approach is the modern teaching: most resolve or heal after a single simple drainage at the mucocutaneous junction, and only the minority that develop a communicating fistula-in-ano need surgical referral. The 2026 narrative review by Alligood and colleagues summarises the evidence that conservative management reduces the fistula rate without increasing recurrence, and is the default for the well infant. [10]
The paronychia is a common paediatric minor procedure. A digital block at the base of the finger (plain lidocaine, no adrenaline if the conservative answer is required, although modern low-dose adrenaline is widely used and safe) provides anaesthesia. An acute paronychia is drained by gently elevating the nail fold from the nail plate with a small blade or a flat probe; if there is a subungual extension, a portion of the proximal or lateral nail is removed to unroof the collection. The cavity is washed, a non-adherent dressing is applied, and the family is reviewed at 24 to 48 hours. [1]
The ingrown toenail (onychocryptosis) in a child is managed conservatively first — warm soaks, an antiseptic, a cotton wedge or a gutter splint to lift the nail edge, and oral antibiotics only if there is surrounding cellulitis. For recurrent or severe disease, the modern treatment algorithm (Matter 2026) recommends a wedge resection of the offending nail edge with phenolisation of the matrix under digital block, which destroys the corner of the germinal matrix and prevents regrowth of the ingrown spicule; the procedure is well tolerated, has a low recurrence rate, and is the definitive treatment after the acute inflammation has settled. [9]
Foreign body removal is the third common paediatric minor procedure. A wooden splinter is removed with a small incision along its long axis and fine forceps; a fish hook is removed by the retrograde technique (back it out along the entry path if the barb has not engaged), the string-yank technique, or the advance-and-cut technique (push the hook through the skin, cut off the barb, and withdraw the shaft); an embedded tick is removed by grasping the head with fine forceps close to the skin and pulling steadily upward without twisting, followed by cleaning and a watch for local or systemic signs of tick-borne disease; glass is located by a plain radiograph if radiopaque, then removed through a small incision along the long axis. Always consider the possibility of a retained foreign body in any paediatric wound that fails to heal, and image if there is any doubt. [1]
The infected epidermoid (sebaceous) cyst has a central punctum and a history of a longstanding subcutaneous lump. The acute inflammation is managed by drainage of the pus through the punctum or a small incision, but definitive excision of the entire cyst wall is deferred until the inflammation has settled — usually four to six weeks — because excision in the acute phase is more likely to leave cyst wall behind and to recur. [1]
In the immunocompromised child, the threshold for drainage is lower, the organism list is broader (including gram-negatives, anaerobes, mycobacteria and fungi), and atypical or non-healing lesions need biopsy as well as culture. The empiric antibiotic plan is broader and is guided by the local infectious-diseases team. [1]
Complications & Pitfalls
The complications of paediatric abscess drainage run from the common and self-limiting to the rare and catastrophic, and the discipline is to anticipate the serious ones and prevent them through the pre-drainage check, while managing the common ones with honesty and technique. [1] [2]
The common complications are local pain at the incision site, mild bleeding that settles with pressure, a transient surrounding cellulitis that improves after drainage, scarring, and recurrence from an incomplete drainage. Most of these settle with simple measures — analgesia, a dressing, and a planned review. A recurrence is the cue to ask whether the loculations were broken, whether there is an underlying cyst or fistula, and whether the child is colonised with MRSA. [1]
The serious complications are rare but worth knowing exactly. Local anaesthetic systemic toxicity from exceeding the weight-based dose or from accidental intravascular injection is prevented by the dose calculation, by aspiration before every injection, and by slow injection; it is treated with intralipid. Damage to a neurovascular structure — a digital nerve, a facial nerve in a parotid region abscess, the anal sphincter in a perianal abscess — is prevented by a sound knowledge of the anatomy and by blunt dissection within the cavity. Progression to a necrotising infection after a delayed diagnosis is the catastrophic failure: a child sent home with what was thought to be a simple abscess, who returns with a necrotising fasciitis hours later. The protection is the explicit red-flag check at the first encounter. Fistula formation in perianal disease is managed by surgical referral. [12] [10]
A frequently tested technical pitfall is the too-small incision. A small stab that does not fully unroof the cavity cannot drain the collection, and the abscess recurs; the incision must be large enough to express the pus and to allow loculation breakdown. A second pitfall is routine packing of every abscess, including small ones: a small single-cavity abscess needs only light packing or no packing, and routine tight packing causes unnecessary pain without reducing recurrence. The loop technique has replaced packing for larger abscesses for exactly this reason. [2]
Prognosis & Disposition
The prognosis after an uncomplicated abscess drainage is excellent: the pain usually settles within hours of drainage, the cavity heals by secondary intention over one to two weeks, and most children return to normal activity within a day or two. The disposition is driven more by the underlying diagnosis than by the procedure itself. [1] [3]
For a simple abscess in a well child, the disposition is home with simple analgesia, a dressing, and a planned review at 24 to 48 hours to remove or replace the packing or to check the loop. Adjuvant oral antibiotics are given if there is surrounding cellulitis over 5 cm, fever, an abscess over 2 cm, immunocompromise, a suspected MRSA-endemic region, or a failure of a prior drainage; the choice is cephalexin first-line, with clindamycin or trimethoprim-sulfamethoxazole for suspected MRSA, guided by the local antibiogram and the pus culture result. The safety-net advice is to return urgently for worsening pain, spreading redness, fever, or recurrence. [3] [5]
For the child with a severe SSTI or a necrotising infection, the disposition is paediatric inpatient or intensive care for the duration of intravenous antibiotic therapy, serial surgical review of the wounds, and a planned rehabilitation pathway for any skin or soft tissue defect. [1]
For the child with a perianal abscess and a fistula-in-ano, the disposition is paediatric surgical outpatient review; most fistulae in male infants close spontaneously or with conservative measures, and only the persistent or recurrent fistula needs operative management. [10]
The loop drainage technique has changed the prognosis of larger abscesses: the systematic review evidence shows lower failure and recurrence rates than classical I&D with packing, fewer return visits, and a shorter total treatment course. The loop is usually removed at the one-week review in the outpatient clinic, and the cavity has usually closed by then. [2]
Special Populations
The approach to drainage is adjusted for the child in front of you, and the fellowship candidate must show that they can match the technique and the timing to the population. [1] [10]
In the neonate, abscesses are smaller, the atypical organisms (group B streptococcus, E. coli, S. aureus) must be covered, and the threshold for inpatient management and intravenous antibiotics is lower. The local anaesthetic dose is tiny — a 3 kg neonate's plain lidocaine limit is 9 mg, which is 0.9 mL of one-percent lidocaine — and the procedure is usually done with topical anaesthesia, oral sucrose, and containment rather than infiltration. [8]
In the immunocompromised child, including the oncology patient, the transplant recipient, and the child with a primary immunodeficiency, the threshold for drainage is lower, the organism list is broader (gram-negatives, anaerobes, mycobacteria, fungi), the empiric antibiotic plan is guided by the infectious-diseases team, and any atypical or non-healing lesion needs biopsy as well as culture. [1]
In the child with diabetes or a metabolic disease, the risk of a severe SSTI is higher, the threshold for intravenous antibiotics is lower, and the glycaemic control during the acute infection needs active management. [1]
In the anticoagulated child or the child with a bleeding disorder, the procedure is coordinated with the haematology team: the anticoagulant is held for the appropriate interval where possible, the coagulation and platelet count are checked and corrected before drainage, small stab incisions are preferred over large ones, and the anticoagulant is restarted after an interval that balances procedural bleeding against thrombosis. [1]
In the Indigenous, remote, or under-resourced setting, the indications are the same but access to ultrasound, to clindamycin or TMP-SMX, and to a skilled proceduralist may not be. The equity intervention is to triage the child for severity, to drain what can be drained safely in the community, to treat empirically with oral antibiotics where appropriate, and to arrange retrieval for the child with a necrotising infection or a deep space abscess. [1]
In the child with disability, neurodivergence, or complex chronic disease, the procedure is planned with extra time, a communication strategy appropriate to the child, an assent process where possible, and a sedation plan that the child and family can support; a "one-and-done" approach under dissociative sedation may be preferable to a series of traumatic awake procedures. [7]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric abscess drainage has matured in three areas: the role of adjuvant antibiotics, the loop drainage technique, and paediatric procedural analgesia. The candidate should know each one and the regional deltas that follow. [1] [3]
The adjuvant-antibiotic evidence is the most tested. Two landmark trials and a network meta-analysis frame the question. The Talan 2016 NEJM trial randomised adults and children with an uncomplicated skin abscess (median around 2 to 3 cm) to trimethoprim-sulfamethoxazole or placebo after I&D, and found a modest improvement in cure at 7 to 10 days with antibiotics, with the largest benefit in abscesses over 2 cm and in those with surrounding cellulitis. The Daum 2017 NEJM trial (smaller abscesses, median under 2 cm) found a smaller and less consistent benefit. The Wang 2018 network meta-analysis pooled the trials and concluded that adjuvant antibiotics modestly improve cure rates, with clindamycin and TMP-SMX both effective against MRSA where the local resistance allows. The teaching is that adjuvant antibiotics are not universal — a small, well-drained abscess in a well child does not need them — but they are indicated for the larger abscess, the surrounding cellulitis, the fever, the immunocompromised child, and the MRSA-endemic region. [3] [4] [5]
The loop-drainage evidence is the strongest single procedural change in modern practice. The Gottlieb 2021 systematic review and meta-analysis showed that the loop drainage technique reduced the need for a secondary procedure and the recurrence rate compared with classical I&D with packing, particularly for abscesses over about 5 cm, without increasing complications. The teaching is now that the loop technique is the default for larger abscesses and that routine packing of every abscess is no longer evidence-based. [2]
The paediatric procedural analgesia evidence continues to mature. The Cochrane review on topical anaesthesia for needle-related pain in newborn infants (Foster 2017) confirmed that amethocaine and EMLA both reduce procedural pain, with amethocaine favoured for onset and efficacy; the 2025 Arch Dis Child clinical practice guideline on topical analgesia during needle-related procedures in children gives a contemporary framework for combining topical anaesthesia with non-pharmacological measures. The clear teaching is that an untreated paediatric drainage is ethically and evidence-wise indefensible. [7] [8]
Loop technique vs incision and drainage with packing (systematic review and meta-analysis, Acad Emerg Med 2021)
PMID 33037713
Population: Adults and children with skin and soft tissue abscesses drained by the loop technique or by I&D with packing
Comparator: Classical incision and drainage with packing
Key finding
The loop technique reduced the need for a secondary procedure and the recurrence rate, with the largest benefit in abscesses over about 5 cm, without increasing complications. Recommendation: loop technique is the default for larger abscesses.
Where the evidence is weak or contested: the routine use of antibiotics after small well-drained abscesses (the absolute benefit is small); the role of routine packing in small abscesses (probably unnecessary); the optimal timing of cyst wall excision after an acute infection (usually four to six weeks, but individualised); the routine use of bedside ultrasound for every abscess (helpful when the picture is uncertain, but not always necessary); and the role of MRSA decolonisation for recurrent SSTI (a bundle of chlorhexidine washes, nasal mupirocin, and family screening is used but the evidence for sustained decolonisation is modest). Each is a defensible topic for the viva. [1] [5]
Exam Pearls
The fellowship examiner expects a candidate who knows the bedside decision, the local anaesthetic pharmacology, the loop technique, and the red flags, and can defend the procedure at the bedside. [1] [2]
The single most testable fact is the weight-based local anaesthetic dose: plain lidocaine 3 mg/kg, lidocaine with adrenaline 7 mg/kg, bupivacaine 2 mg/kg (3 mg/kg with adrenaline). Calculate the milligrams from the weight in kilograms and write it on the drape. The corresponding volume of one-percent lidocaine is the dose in milligrams divided by ten — a 12 kg toddler's plain lidocaine limit is 36 mg, which is 3.6 mL. [1] [12]
The loop drainage technique is the modern default for larger abscesses. Two small stab incisions are made at the poles, a vessel loop is passed through the cavity, and it is tied with light tension; the loop stays in for several days to a week and keeps the cavity open as it heals. It reduces failure and recurrence compared with packing. [2]
The red flags of necrotising fasciitis are the single most important safety discriminator: pain out of proportion, induration beyond the margins, skin anaesthesia, crepitus, rapidly evolving course, systemic toxicity, and grey or dusky skin with haemorrhagic bullae. A child with any of these is not a treatment-room candidate. [1] [1]
The indications for adjuvant antibiotics after I&D are: surrounding cellulitis over 5 cm, fever, an abscess over 2 cm, immunocompromise, a MRSA-endemic region, and a failure of a prior drainage. The first-line agent is cephalexin; for suspected MRSA it is clindamycin or trimethoprim-sulfamethoxazole. Send pus for culture in every drain. [3] [5]
The perianal abscess of the male infant is managed conservatively first: most resolve or heal after a single simple drainage at the mucocutaneous junction, and only the minority that develop a fistula-in-ano need surgical referral. [10]
The classic distractors the exam rewards for naming: draining an abscess without calculating the weight-based local anaesthetic dose; using a cutting needle to break loculations instead of a finger or a haemostat; closing a drained cavity with sutures; packing every abscess routinely instead of using a loop for larger ones; prescribing antibiotics for every drainage regardless of size or severity; missing a necrotising infection by not asking about pain out of proportion; and forgetting to send pus for culture. Each is wrong for a specific evidence-based reason. [1] [2]
References
- [1]Melnick A, Friedman J, Sokoloff WC Office Minor Surgeries and Procedures Pediatr Rev, 2025.PMID 41173309
- [2]Gottlieb M, DeMott MJ, Peksa GD Comparison of the Loop Technique With Incision and Drainage for Skin and Soft Tissue Abscesses: A Systematic Review and Meta-analysis Acad Emerg Med, 2021.PMID 33037713
- [3]Talan DA, Mower WR, Prikis J, et al Trimethoprim-Sulfamethoxazole versus Placebo for Uncomplicated Skin Abscess N Engl J Med, 2016.PMID 26962903
- [4]Daum RS, Miller LG, Immergluck L, et al A Placebo-Controlled Trial of Antibiotics for Smaller Skin Abscesses N Engl J Med, 2017.PMID 28657870
- [5]Wang W, Chen W, Liu Y, et al Antibiotics for uncomplicated skin abscesses: systematic review and network meta-analysis BMJ Open, 2018.PMID 29437689
- [6]Singer AJ, Talan DA Systemic antibiotics after incision and drainage of simple abscesses: a meta-analysis Emerg Med J, 2014.PMID 23686731
- [7]Stavleu DC, Rehman M, Paterson R, et al Topical analgesia during needle-related procedures in children: a clinical practice guideline Arch Dis Child, 2025.PMID 39933876
- [8]Foster JP, Taylor C, Spence K Topical anaesthesia for needle-related pain in newborn infants Cochrane Database Syst Rev, 2017.PMID 28160271
- [9]Matter A, Koleilat T, Catalano M, et al Pediatric Ingrown Toenails: A Practical Treatment Algorithm Dermatol Surg, 2026.PMID 41343273
- [10]Alligood DM, Saufley AS, Huerta CT Conservative versus operative management of perianal abscess and fistula-in-ano in infants: a narrative review Transl Gastroenterol Hepatol, 2026.PMID 41675342
- [11]Neal JT, Cleary D, Coates WC, et al Discrepancies Between Estimated and Expressed Abscess Volume in Pediatric Incision and Drainage Pediatr Emerg Care, 2026.PMID 41422417
- [12]Lee SH, Shin S, Sohn JT Local Anesthetic Systemic Toxicity Caused by Non-Anesthesiologists: A Narrative Review of Case Reports J Korean Med Sci, 2025.PMID 41185577