Paeds · preventive-and-community-paediatrics
Newborn hearing screening
Also known as Universal newborn hearing screening · UNHS · Neonatal hearing screen · EHDI · Early hearing detection and intervention · Otoacoustic emissions newborn screen · Automated ABR newborn screen
Fellowship guide to universal newborn hearing screening: OAE and AABR pathways, pass versus refer counselling, 1-3-6 EHDI clocks, high-risk and NICU strategies, late-onset loss after a pass, congenital CMV interfaces, incomplete screens, equity and regional programme differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Most babies with permanent hearing loss look completely well in the first days of life. They feed. They startle to a slammed door. Families go home reassured. Without a population screen, many of those babies would only be recognised when speech is already behind. That delay costs language. [2] [7]
Universal newborn hearing screening means offering a validated screen to every newborn, not only those with risk factors. Screening is not diagnosis. Screening sorts infants into pass, refer, incomplete or invalid states. Diagnostic audiology then confirms or excludes permanent childhood hearing impairment and defines laterality and type. Early hearing detection and intervention (EHDI) is the whole system: screen, confirm, intervene, and keep high-risk infants under surveillance. [1] [9]
The programme meets classic screening principles. Permanent childhood hearing loss is important. There is an accepted early intervention pathway. There is a suitable point-of-care test. There is an agreed policy on whom to treat. And the system must be able to deliver confirmation and care, not only a machine printout. A result without follow-through is not a programme. [9] [10]
What you actually do from birth to early intervention
Screen on time
Complete a local OAE and/or automated ABR pathway before discharge when possible, and by 1 month of age at latest.
Name the result state
Record pass, unilateral refer, bilateral refer, incomplete or invalid. Never leave a blank that looks like a pass.
Counsel in plain language
Refer means more testing is needed. It does not mean the baby is deaf.
Book the next step
Diagnostic audiology for refers. Residual-risk plan for high-risk passes. Named owner for incompletes.
Close the loop
Confirm diagnosis by 3 months when loss is present, start early intervention by 6 months, and keep surveillance open for progressive risk.
Classification
Think first in result states, not disease labels. [1]
Pass or clear means continue routine care, but still counsel residual risk when the infant is high risk. Refer means a defined next test. It is not a final diagnosis. Incomplete or invalid means the screen was never done, was technically inadequate, or the family left without a completed pathway. Lost-to-follow-up means a refer occurred and diagnostic completion never happened. Each state needs a different action and a different urgency. [1] [8]
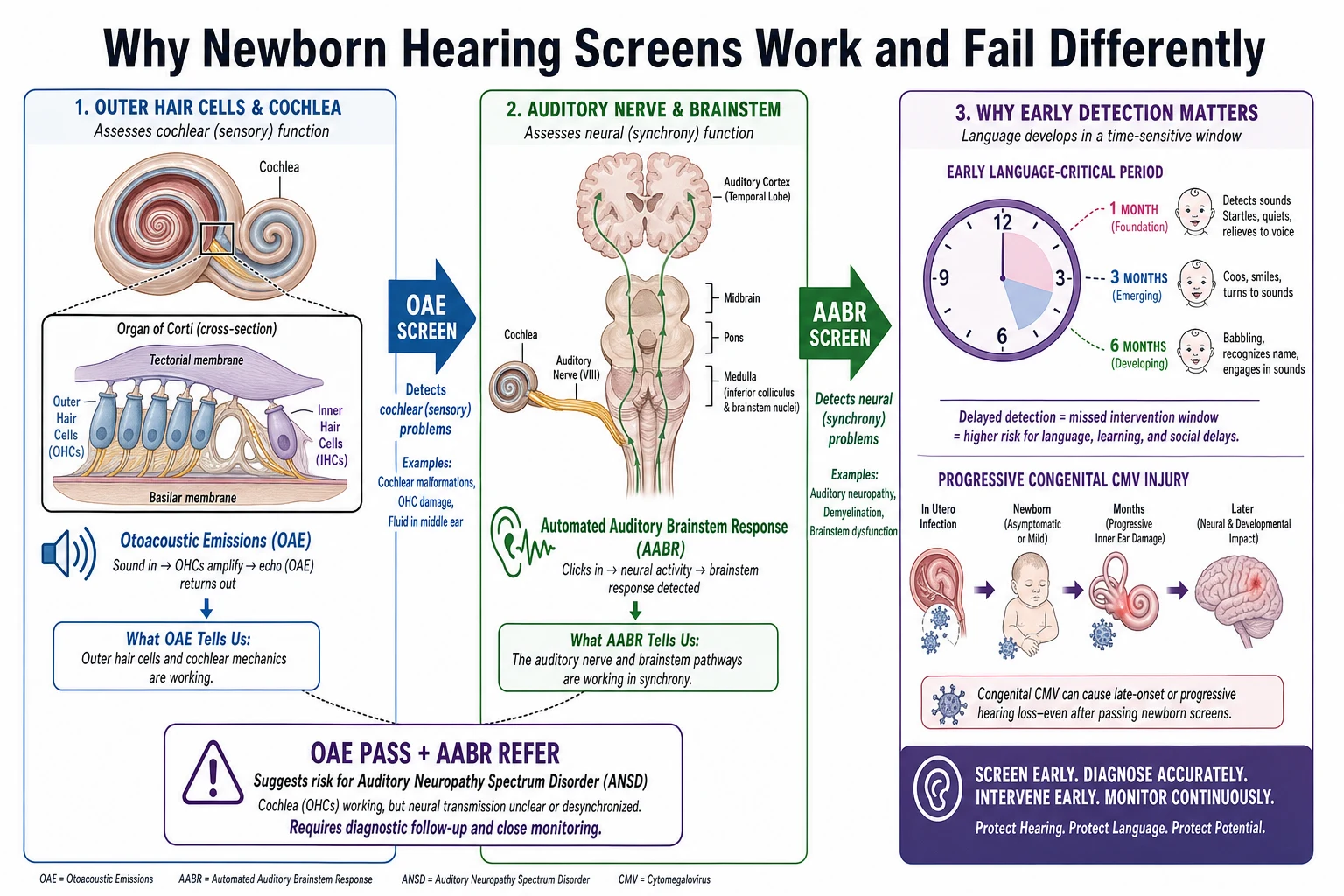
Classify the hearing problem you are trying to find. Permanent childhood hearing impairment includes permanent sensorineural loss and permanent conductive loss that will not resolve with simple middle-ear fluid. Temporary conductive loss from vernix, debris or middle-ear fluid is common around the newborn period and is a major reason for false refers. Auditory neuropathy spectrum disorder (ANSD) is different again: cochlear outer hair cell function may be preserved while neural synchrony is impaired. That is why an OAE-only pathway can miss some neural problems. [7] [17]
Programmes use different strategies. Many well-baby nurseries use otoacoustic emissions first, then automated ABR if needed. Many NICU pathways prefer automated ABR because neural pathway integrity matters more in that population. Some services use AABR for all infants. Know the pathway you work under rather than inventing a universal device algorithm. [1] [15]
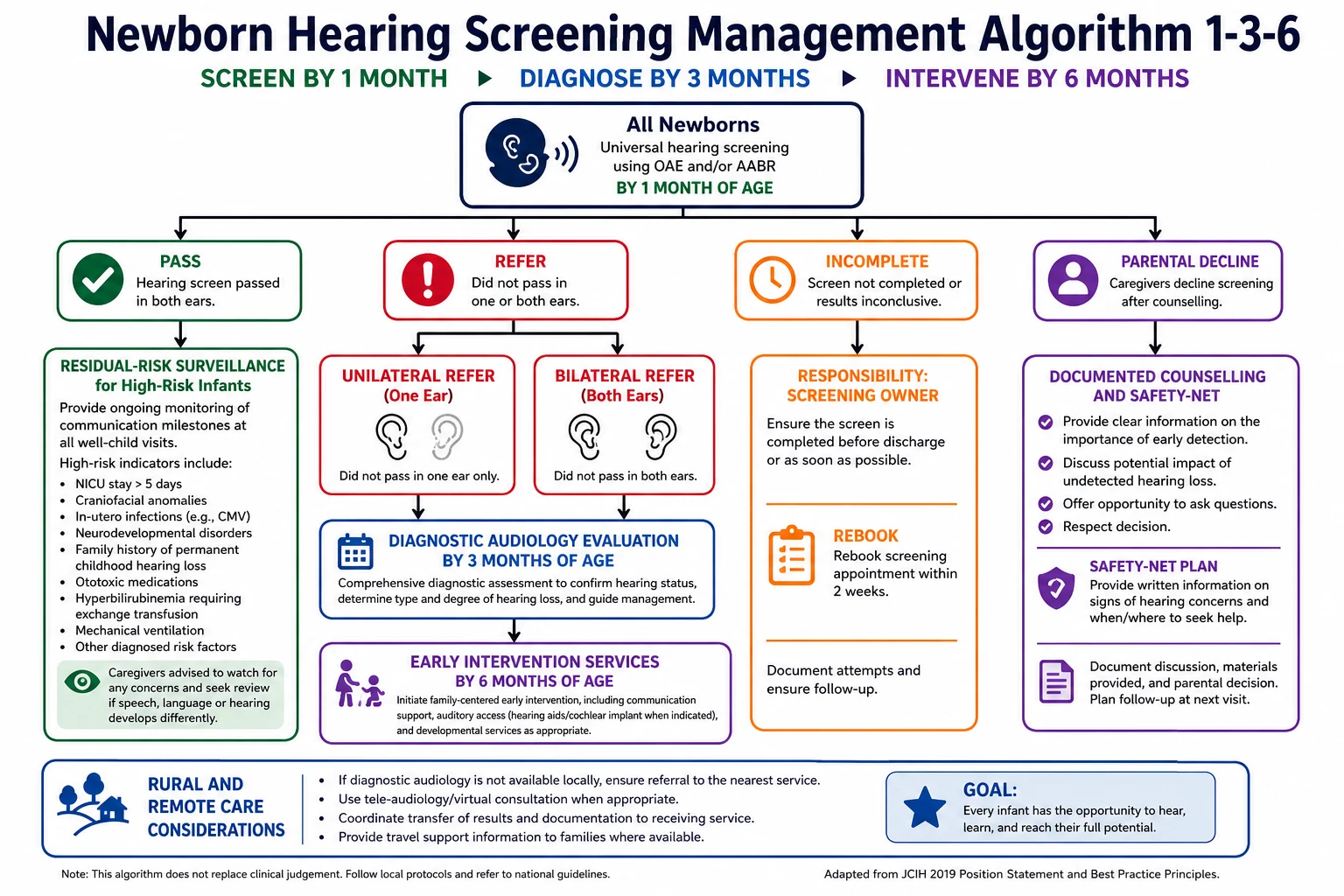
The time standard most examiners expect is 1-3-6: screen by 1 month, diagnose by 3 months, intervene by 6 months. The 2019 JCIH update encourages systems that already meet 1-3-6 to aim for 1-2-3. Always check the service standard in front of you. [1]
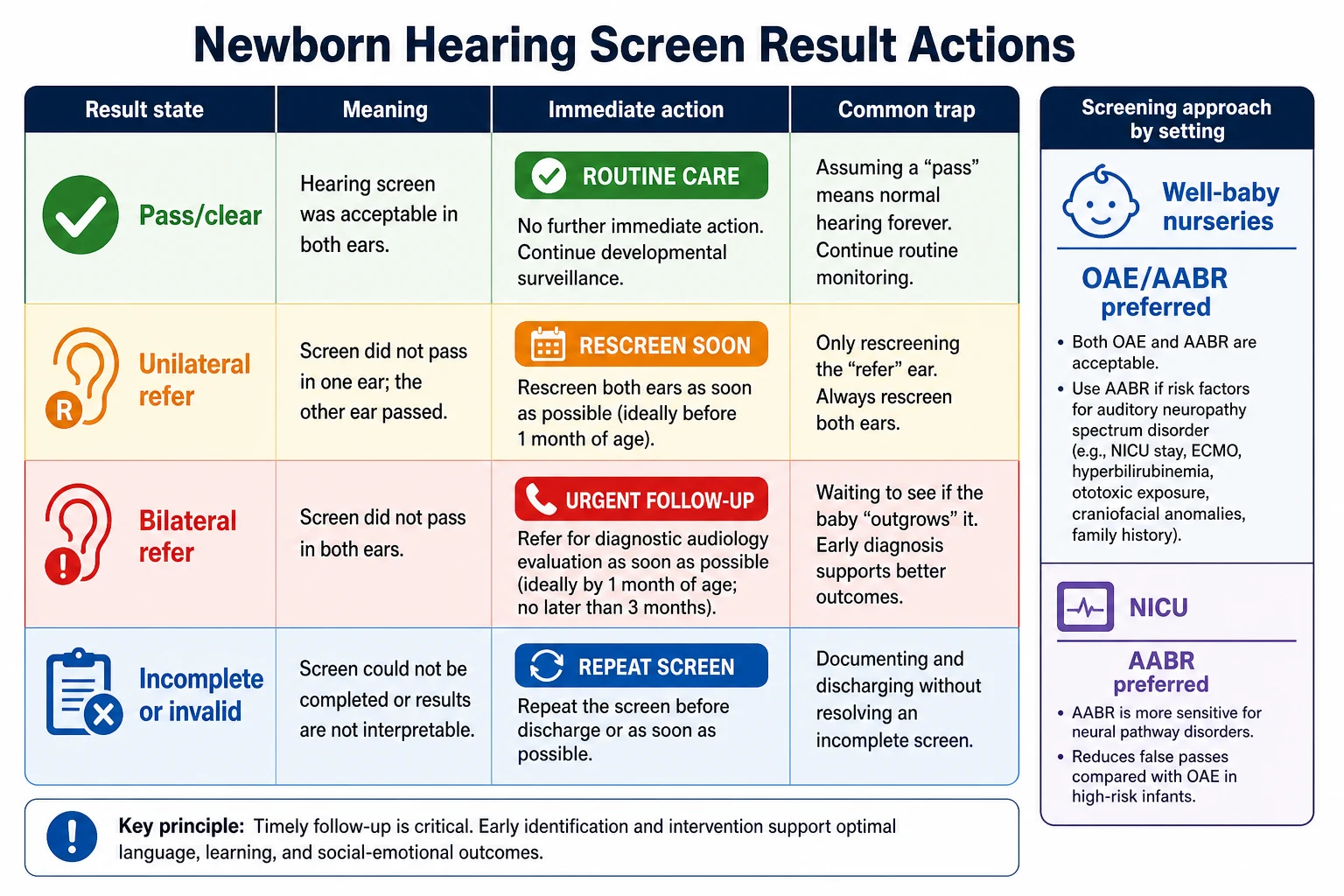
Read the figure like this: do not leave the ward with a grey incomplete cell and no name next to it. The common exam trap is treating “probably done” as done, or treating “startles to noise” as a pass. [8]
OAE
Cochlear outer hair cells
- Quick point-of-care screen
- Sensitive to debris and middle-ear fluid
- Can pass in some neural pathway disorders
- Common first step in well-baby pathways
AABR
Nerve and brainstem pathway
- Includes neural synchrony information
- Preferred in many NICU protocols
- Still a screen, not a full diagnostic ABR
- Helps reduce missed ANSD risk compared with OAE alone
Refer
Not a diagnosis
- Means more testing is required
- Book diagnostic audiology
- Counsel without over-calling deafness
- Laterality still matters
Pass
Not lifelong clearance
- Routine care if low risk
- High-risk infants need surveillance
- Late-onset and progressive loss still occur
- Caregiver concern always reopens the question
Epidemiology & Risk Factors
Permanent congenital hearing loss is uncommon enough that selective risk-factor screening alone misses many affected babies, and common enough that delayed detection creates large language costs at population level. That combination is why universal screening became standard in high-resource systems and why the USPSTF recommended screening all newborns. [4] [7]
Risk factors matter for two different jobs. First, they identify infants who need a more robust screen modality, often AABR. Second, they identify infants who need ongoing surveillance even after a newborn pass. Classic risk groups include NICU care, craniofacial anomalies, family history of childhood hearing loss, congenital infection, culture-positive sepsis or meningitis, ototoxic exposure, severe hyperbilirubinemia requiring exchange pathways, and syndromes associated with hearing loss. Exact lists are programme-defined; use the local EHDI risk schedule rather than memorising a private list. [1] [15]
Congenital cytomegalovirus (cCMV) is a leading infectious driver of childhood hearing loss and can produce progressive or fluctuating loss after a newborn pass. That is why cCMV policy and hearing pathways increasingly intersect, and why a pass never means “never think about hearing again” in an infant with proven or highly suspected cCMV. [11] [16]
System factors create missed detection as often as biology does. Early discharge, weekend staffing, home birth, interhospital transfer, incomplete contact details, transport barriers and weak result handover all raise incomplete-screen and lost-to-follow-up rates. Pandemic-era data showed how easily JCIH timeline adherence can slip when systems are stressed. [8] [14]
Equity gaps are part of the epidemiology. Rural families, language-discordant families, out-of-home care arrangements and socioeconomic disadvantage all reduce the chance that a refer becomes a completed diagnosis and early intervention package. Access barriers continue after diagnosis for deaf and hard-of-hearing children. [13]
Pathophysiology
Otoacoustic emissions come from healthy outer hair cells in the cochlea. A soft probe click or tone makes those cells “talk back.” If the outer hair cells are working and the middle ear is reasonably clear, the machine can detect that echo. Vernix, debris or fluid can block the path and create a false refer. That is a temporary conductive problem, not permanent nerve injury. [7] [17]
Automated auditory brainstem response tracks the electrical journey from the cochlea through the auditory nerve and brainstem. A baby can therefore pass an OAE-based screen and still refer on AABR if neural synchrony is impaired. That pattern is the teaching core of auditory neuropathy spectrum disorder risk. In NICU infants, where neural and global illness risks are higher, many programmes prefer AABR for that reason. [1] [7]
Language depends on early, consistent auditory access. In the first months of life the brain is building the map that later supports words, phonology and reading. Permanent hearing loss during that window degrades the map unless amplification, cochlear implant pathways or other communication access arrive early. That is the mechanistic reason the 1-3-6 clock exists. [2] [18]
Progressive disease explains residual risk after a pass. Congenital CMV can injure the inner ear over time. Some genetic losses evolve after the newborn period. Post-infectious and ototoxic injuries can appear later still. A newborn pass only says the baby passed that screen at that moment. It does not freeze hearing for life. [11] [12]
Unilateral permanent loss still matters. Localisation, classroom listening in noise and safety awareness can all suffer even when one ear is excellent. Dismissing unilateral disease because the baby “hears” is a classic pitfall. [7] [17]
Clinical Presentation
The usual “presentation” of a newborn who needs hearing follow-up is no presentation at all. The infant is pink, feeding and settled. The abnormal finding is a machine result or a missing result. That is why appearance must never cancel a refer pathway. [1] [9]
Parents often hear “refer” as “deaf.” Your first clinical task is to reframe without minimising. Say that the screen was not clear and more accurate testing is needed. Do not invent percentages at the bedside if you cannot source them. Do not cancel the booking because the baby startled to a clap. Behavioural responses in newborns are crude and can be driven by vibration or startle pathways that do not equal normal hearing thresholds. [7] [8]
Later presentations matter just as much. After a pass, progressive or late-onset loss may show as reduced babble, poor response to quiet sounds, speech delay, or caregiver concern that “something is not right.” High-risk infants can pass at birth and still need planned surveillance. An 8-month-old with no words after a missed diagnostic pathway is a systems failure presenting as language delay. [12] [15]
False-positive screens present as family distress. Sleep disruption, feeding worry and distrust of health services can all follow a poorly counselled refer. That harm is real and preventable with clear language and rapid diagnostic access. [6] [8]
Differential Diagnosis
For a refer, start with four buckets. [7]
- Technical or environmental failure — noisy room, poor probe fit, unsettled infant, equipment error.
- Temporary conductive barrier — vernix, debris, middle-ear fluid.
- Permanent childhood hearing impairment — sensorineural or permanent conductive loss.
- Neural pathway risk — auditory neuropathy spectrum disorder pattern, especially relevant when OAE and AABR disagree. [7] [17]
Do not use a clap test to choose among those buckets. The discriminating next step is diagnostic audiology, not ward theatre. [7] [17]
When language delay appears later, hearing loss sits beside global developmental delay, autism spectrum presentations, environmental language deprivation and isolated speech-language disorders. Hearing must be confirmed, not assumed, before those labels are final. [17]
When parents decline screening, the differential is not only “anti-screen.” Explore specific misconceptions, prior trauma, access barriers, consent confusion and, rarely, safeguarding concern if critical care is being avoided in a broader pattern of harm. Most declines are values or information problems, not safeguarding emergencies. [9]
When a refer coexists with microtia, ear canal atresia, craniofacial anomaly or a syndrome phenotype, permanent structural or syndromic hearing loss rises in probability and specialist pathways should open early. [7]
Clinical & Bedside Assessment
Prepare the infant. A quiet, settled baby with a clear ear canal gives the cleanest screen. Explain to parents what will happen and what pass and refer mean before the probe goes in. Document modality, laterality, time of test and exact result state. [1] [8]
Take a focused history that changes residual-risk counselling: family history of childhood hearing loss, NICU course, ototoxic drugs, severe jaundice, proven congenital infection, meningitis, craniofacial findings and caregiver concern about response to sound. Examine the pinnae, canals, tags, pits, facial symmetry and other syndromic clues. [1] [15]
Assess the family’s real ability to complete follow-up. Who has transport? Who has phone credit? Who has legal parental responsibility if the infant is in out-of-home care? Who needs an interpreter? A perfect diagnostic booking that no one can attend is not a plan. [13]
At the first community review, do not ask only “Did hearing screening happen?” Ask for the result state and whether any diagnostic appointment exists. If the answer is vague, treat it as incomplete until proven otherwise. [8]
Investigations
On the postnatal ward the investigation is the screen itself: OAE, automated ABR, or the local two-step combination. Use the modality your service specifies for well-baby and NICU populations. Do not invent pass-fail cut-offs in an exam if you cannot source the local algorithm; state that you will use the validated device pathway. [1] [9]
After a refer, the key investigation is diagnostic audiology, usually including diagnostic ABR and age-appropriate middle-ear assessment. Behavioural audiometry becomes more useful as the infant matures. Repeat casual ward screens are not a safe way to cancel a refer. [7] [17]
Congenital CMV testing can be time-critical. If cCMV evaluation is indicated after refer or confirmed loss, early postnatal samples matter because later testing may not distinguish congenital from postnatal infection. Follow the current local cCMV pathway rather than improvising specimen choice. [11] [16]
After permanent loss is confirmed, further work-up is specialist-led and may include otology review, genetics, ophthalmology and imaging selected to the phenotype. Do not delay amplification or early intervention while an endless investigation list is assembled. Investigations serve management; they do not replace it. [7] [17]
For high-risk infants who passed newborn screening, the “investigation plan” is scheduled surveillance audiology according to local EHDI risk schedules, plus low-threshold review if caregivers report concern. [1] [15]
Management — Resuscitation
Hearing screening is almost never the first action in an unstable neonate. Support airway, breathing and circulation first. Complete or reschedule screening only when the infant is stable enough for a valid test, and document the incomplete state with a named owner if transfer occurs before screening. [9]
The acute “resuscitation” moment in this topic is usually family crisis, not cardiorespiratory collapse. A bilateral refer can trigger panic. Sit down. Use plain language. Separate screen from diagnosis. Book the next step in the room if possible. If a parent becomes so distressed that discharge safety is uncertain, involve senior staff and supports rather than minimising the result. [8]
Infants with ear canal atresia or major craniofacial anomaly may not be screenable with standard probes. That is not a pass. It is a direct referral pathway to specialist audiology and otology. [7]
In rural settings, a bilateral refer with no local diagnostic ABR means early destination planning. Do not send a family home with “someone will call you sometime.” Give a service, a timeframe and a backup contact. [8] [13]
Management — Definitive & Stepwise
1. Complete the screen
Before discharge, document hearing status explicitly. If the infant is too young, too unwell or too unsettled, record incomplete and create a rebook plan that can still meet the 1-month standard. [1]
2. Pass pathway
Low-risk pass: routine well-child care plus caregiver education that new concerns reopen testing. High-risk pass: add surveillance according to local risk schedules and explain why a pass is not lifelong clearance. [1] [12]
3. Unilateral refer pathway
Explain that one ear was not clear. Book diagnostic audiology. Do not dismiss unilateral refers. Confirmed unilateral permanent loss still needs classroom and safety planning later. [7] [17]
4. Bilateral refer pathway
Higher urgency for family counselling and booking. Still not a diagnosis of deafness. Aim for complete audiologic diagnosis by 3 months, earlier if the system can. Open early intervention as soon as permanent loss is confirmed, targeting intervention by 6 months and sooner when possible. [1] [3]
5. Incomplete, invalid or declined pathway
Name an owner. Offer re-screen or direct diagnostic referral according to local rules. For decline, explore reasons, correct specific misconceptions, document residual risk and keep the door open. Do not coerce. Do not pretend the risk is zero. [8] [9]
6. After confirmed permanent loss
Coordinate audiology, medical/otology review, family support and early intervention. Amplification, cochlear implant candidacy pathways and communication choices are individualised. Paediatricians keep the medical home role: developmental surveillance, immunisation, vision, family function and school readiness. [7] [13]
Specific Subtypes & Scenarios
Early discharge within 24 hours. Screening may be deferred. Deferred is acceptable only with a booked completion plan that still meets the 1-month target. [1] [14]
Home birth or delayed first contact. Treat the first clinical contact as day zero for the package. Do not assume community services already completed screening. [9]
NICU graduate. Verify modality and completion before transfer or discharge. AABR-based strategies are often required. Ototoxic exposure and severe illness raise residual-risk surveillance needs after a pass. [1] [15]
Rural maternity unit without on-site diagnostic ABR. A bilateral refer needs an explicit destination and transport plan, not optimism. [8] [13]
Well term infant with bilateral OAE refer. Counsel carefully, examine canals, and book diagnostic audiology. Do not endlessly repeat OAE to “get a pass.” [7]
Proven or suspected congenital CMV. Even after a newborn pass, plan hearing surveillance because progressive loss is well recognised. Align with the local cCMV pathway. [11] [16]
Auditory neuropathy spectrum disorder pattern. Avoid OAE-only reassurance. Intervention choices may differ from typical cochlear loss and need specialist audiology leadership. [7] [17]
Missed diagnostic follow-up presenting in later infancy. Treat as urgent recovery of the EHDI pathway plus full developmental assessment. Do not wait for the next routine review. [8] [18]
Complications & Pitfalls
False positives create anxiety, extra visits and temporary over-medicalisation of a well baby. Mitigate with accurate language and rapid diagnostics. False negatives and missed progressive loss create false confidence and late language impairment. [6] [12]
Classic pitfalls include over-calling deafness from a screen, cancelling a refer after a clap test, treating unilateral loss as trivial, accepting “done somewhere” without documentation, discharging an incomplete screen with no owner, forgetting residual-risk surveillance after a high-risk pass, and delaying early intervention while waiting for every possible investigation. [1] [7] [8]
Lost-to-follow-up after refer is the quiet complication that destroys programme benefit. It is a systems emergency. Chase it like an abnormal critical result. [8] [14]
Prognosis & Disposition
Safe disposition is not “feeding well.” It is “hearing pathway complete or hearing pathway owned.” [1] [8]
A low-risk pass can go home with routine care and open-door advice. A high-risk pass can go home only with a surveillance plan the family can actually attend. A refer can go home only if diagnostic audiology is booked, contact details work and the family can restate the plan. An incomplete screen needs the same ownership standard as any other unfinished newborn preventive task. [1] [8]
Prognosis after permanent loss is not fixed at birth. Earlier confirmation and earlier intervention improve language and support better long-term literacy trajectories. Spoken language skill in middle childhood still predicts later reading, which is why the early years matter so much. Quality-of-life arguments also support universal programmes when follow-through works. [3] [5] [6] [19]
Special Populations
Preterm and technology-dependent infants need modality choices and timing that match stability, corrected age and local NICU protocols. Do not mark a pass by convenience. [15]
Indigenous, rural and remote families need discharge plans that match real travel times, cultural safety and family decision structures. Migrant and refugee families need interpreter-supported counselling at the moment of refer, not a translated letter days later. Out-of-home care requires clarity on who consents and who receives appointments. Socioeconomic disadvantage often decides whether a booked test is attended. [13]
Families connected with Deaf culture may frame communication goals differently from hearing families seeking spoken language. Good care is not one script. It is accurate medical information, timely audiology and respect for family communication choices within an early intervention framework. [13]
Evidence, Guidelines & Regional Differences
Yoshinaga-Itano’s classic work showed better language when hearing loss was identified by 6 months of age. Kennedy and colleagues showed better language ability when permanent childhood hearing impairment was confirmed by 9 months. Pimperton’s cohort work linked earlier confirmation with better long-term literacy outcomes. Those studies are the reason examiners care about clocks, not just machines. [2] [3] [5] [18]
The 2007 JCIH position statement remains the foundational EHDI systems document in PubMed-indexed form, with 1-3-6 benchmarks and high-risk surveillance expectations. The 2019 JCIH update, published outside PubMed as a JEHDI position statement, pushes high-performing systems toward earlier 1-2-3 targets and refreshes risk and intervention guidance. Implementation studies continue to show that standards fail when diagnostic capacity, family contactability or staffing fail. [1] [8] [14]
The USPSTF recommended universal newborn hearing screening as a B recommendation, based on accurate screening and improved language outcomes with earlier treatment. Point-of-care newborn screening still needs the governance framework Kemper described: training, documentation, follow-up and quality assurance. [4] [9]
Controversies remain. OAE-only well-baby pathways can miss some neural losses. Universal versus targeted cCMV screening strategies linked to hearing are still evolving. Exact device cut-offs and re-screen rules are local. State those uncertainties honestly. [11] [16] [17]
Australia and Aotearoa New Zealand operate widespread newborn hearing screening under national or jurisdictional frameworks. Diagnostic audiology access and Indigenous, Māori and Pacific follow-up design vary by geography. Quote local programme clocks and modalities. [1]
United Kingdom runs a national newborn hearing screening programme with defined screen and referral pathways; local diagnostic capacity still determines whether the clock is met. [3] [8]
United States uses state EHDI programmes guided by JCIH principles and USPSTF support for universal screening. Operational detail is state-based. [1] [4]
Canada uses provincial programmes; remote geography often dominates diagnostic access planning. [13]
State only differences you have checked against current official programme pages. Do not invent a universal device threshold. [9]
Exam Pearls
- Refer ≠ deaf. Pass ≠ lifelong normal hearing. [7]
- 1-3-6 is the default teaching clock; 1-2-3 is the stretch target for strong systems. [1]
- OAE checks outer hair cells; AABR includes the neural pathway. [7]
- NICU infants often need AABR-based strategies. [1]
- cCMV can cause progressive loss after a newborn pass. [11]
- Unilateral permanent loss still needs a plan. [17]
- Lost-to-follow-up after refer is a systems emergency. [8]
- Early confirmation improves language and later literacy. [3] [5]
- Counselling quality is part of the intervention. [6]
- Boards test whether you can close the loop. [9]
HEAR NOW package
References
- [1]American Academy of Pediatrics, Joint Committee on Infant Hearing Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics, 2007.PMID 17908777
- [2]Yoshinaga-Itano C Language of early- and later-identified children with hearing loss. Pediatrics, 1998.PMID 9794949
- [3]Kennedy CR Language ability after early detection of permanent childhood hearing impairment. The New England journal of medicine, 2006.PMID 16707750
- [4]US Preventive Services Task Force Universal screening for hearing loss in newborns: US Preventive Services Task Force recommendation statement. Pediatrics, 2008.PMID 18595997
- [5]Pimperton H The impact of universal newborn hearing screening on long-term literacy outcomes: a prospective cohort study. Archives of disease in childhood, 2016.PMID 25425604
- [6]Kemper AR Universal newborn hearing screening improves quality of life for children with permanent hearing impairment. The Journal of pediatrics, 2011.PMID 21482247
- [7]Grindle CR Pediatric hearing loss. Pediatrics in review, 2014.PMID 25361905
- [8]Awad R Meeting the Joint Committee on Infant Hearing Standards in a Large Metropolitan Children's Hospital: Barriers and Next Steps. American journal of audiology, 2019.PMID 31084570
- [9]Kemper AR A framework for key considerations regarding point-of-care screening of newborns. Genetics in medicine, 2012.PMID 22899090
- [10]Andermann A Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bulletin of the World Health Organization, 2008.PMID 18438522
- [11]Pollick SA Newborn congenital cytomegalovirus screening and hearing outcomes: a systematic review of current literature. Current opinion in otolaryngology & head and neck surgery, 2024.PMID 39146216
- [12]Corazzi V Late-onset, progressive sensorineural hearing loss in the paediatric population: a systematic review. European archives of oto-rhino-laryngology, 2024.PMID 38411671
- [13]Ren AZ Factors that influence health service access in deaf and hard-of-hearing children: a narrative review. International journal of audiology, 2024.PMID 37335176
- [14]Behzadpour HK COVID Effects on Adherence to Joint Committee on Infant Hearing Newborn Screening Recommendations. Otolaryngology--head and neck surgery, 2025.PMID 39887832
- [15]Lund A Newborn hearing screening in infants at risk of hearing loss: diagnostic outcomes, false-negative results, and the role of surveillance. International journal of pediatric otorhinolaryngology, 2026.PMID 42143905
- [16]Ravin K Congenital cytomegalovirus: Screening strategies and diagnostic challenges. Seminars in perinatology, 2026.PMID 42386471
- [17]Sommerfeldt J Hearing Loss Assessment in Children. Pediatrics in review, 2026.PMID 35593817
- [18]Pimperton H The impact of early identification of permanent childhood hearing impairment on speech and language outcomes. Archives of disease in childhood, 2012.PMID 22550319
- [19]Worsfold S Predicting reading ability in teenagers who are deaf or hard of hearing: A longitudinal cohort study. Research in developmental disabilities, 2018.PMID 29660589