Absence Seizures (Paediatric)
Absence seizures are generalized onset non-motor seizures characterized by sudden, brief lapses in consciousness (typically 5–20 seconds) without loss of postural tone. They are the hallmark of Childhood Absence...
What matters first
Absence seizures are generalized onset non-motor seizures characterized by sudden, brief lapses in consciousness (typically 5–20 seconds) without loss of postural tone. They are the hallmark of Childhood Absence...
Myoclonic jerks (suggests Juvenile Myoclonic Epilepsy)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Myoclonic jerks (suggests Juvenile Myoclonic Epilepsy)
- Generalized tonic-clonic seizures (GTCS) at onset
- Developmental delay or regression
- Atypical EEG (slow spike-wave less than 2.5 Hz)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Absence Seizures (Paediatric)
1. Clinical Overview
Summary
Absence seizures are generalized onset non-motor seizures characterized by sudden, brief lapses in consciousness (typically 5–20 seconds) without loss of postural tone. They are the hallmark of Childhood Absence Epilepsy (CAE), which accounts for approximately 10–15% of all childhood epilepsies. While often dismissed by parents or teachers as "daydreaming" or "inattention," untreated absence seizures can occur hundreds of times per day (pyknolepsy), severely disrupting academic performance and social development.
The condition is defined by its pathognomonic 3 Hz generalized spike-and-wave discharge on EEG. Prognosis is generally excellent, with over 65% of children outgrowing the condition by adolescence, provided they do not develop generalized tonic-clonic seizures (GTCS).
Historical Context
- 1705: Poupart provided the first clear description of absence-like lapses.
- 1824: Calmeil coined the term "Petit Mal" (little sickness) to distinguish it from "Grand Mal."
- 1935: Gibbs, Davis, and Lennox identified the characteristic 3 Hz spike-wave pattern on the newly invented EEG.
- 2010: The CAE Trial (Glauser et al.) established ethosuximide and valproate as superior to lamotrigine for initial therapy, redefining the global standard of care.
Key Facts
- The "3 Hz Rule": The classic EEG signature is a 3 cycles-per-second spike-and-wave discharge.
- Hyperventilation Trigger: 3 minutes of deep breathing provokes a seizure in > 90% of untreated patients.
- The Gender Split: Approximately 60–70% of cases occur in females.
- Neurological Status: By definition, children with "Typical" absence seizures are neurologically and cognitively normal at baseline.
Clinical Pearls
The "Blowing the Pinwheel" Pearl: In the clinic, if you suspect absence seizures, give the child a paper pinwheel (or a piece of tissue) and ask them to blow on it continuously for 3 minutes. If they suddenly stop, stare, and the pinwheel drops, you have likely witnessed an absence seizure.
The "Daydreaming" Distinction: Daydreaming can be interrupted by a loud noise or a touch; an absence seizure cannot. If a child "zones out" and doesn't snap back when their name is shouted, it’s a seizure until proven otherwise.
The "No Postictal" Rule: Unlike focal or tonic-clonic seizures, there is NO postictal confusion. The child resumes their previous activity (or sentence) immediately, often unaware that any time has passed.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Peak Age: 4–10 years (mean age 6). Onset before 4 or after 10 suggests an alternative syndrome (e.g., Early-onset Absence or Juvenile Absence Epilepsy).
- Prevalence: 2–8 per 100,000 children.
- Genetics: Strong genetic component; 15–30% of patients have a positive family history of generalized epilepsy.
Risk Factors Table
| Factor | Association | Clinical Impact |
|---|---|---|
| Female Gender | 2:1 Ratio | Higher incidence in girls. |
| Family History | High Heritability | Polygenic inheritance; sibling risk is ~10%. |
| Age 4–10 | Peak Window | Typical onset period for CAE. |
| GLUT1 Deficiency | Rare Metabolic | Consider if onset is less than 4 years old or resistant to AEDs. |
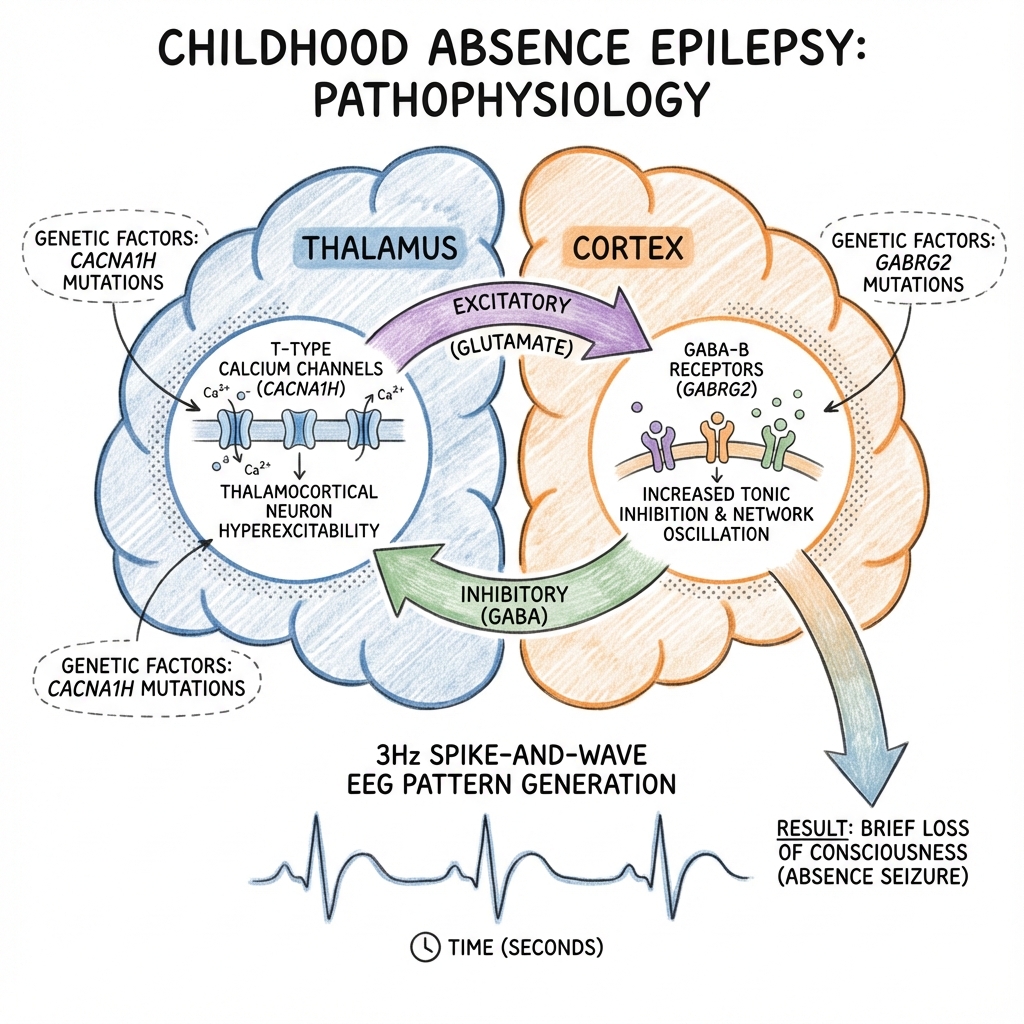
3. Pathophysiology: The Cellular Battlefield
The Thalamocortical Loop
Absence seizures arise from a malfunction in the oscillatory circuit between the thalamus and the cerebral cortex. This circuit normally regulates sleep-wake cycles (sleep spindles).
- Thalamic Reticular Nucleus (TRN): Acts as the pacemaker. It contains GABAergic neurons that provide inhibitory input to thalamocortical relay neurons.
- T-type Calcium Channels: Thalamic relay neurons express specialized low-threshold T-type Ca²⁺ channels.
- Hyper-synchrony: When these channels are overactive (due to genetic mutations or altered GABAergic tone), they trigger "burst firing."
- The Spike and Wave: The Spike represents the rapid excitatory firing of cortical neurons; the Wave represents the following inhibitory period mediated by the thalamus.
Genetics: The Channelopathy Link
- CACNA1H: Encodes the T-type calcium channel alpha subunit. Mutations lead to increased channel activity.
- GABRG2: Mutations in GABA receptor subunits can impair inhibition, facilitating the hypersynchronous discharges.
- SLC2A1: Mutations causing Glucose Transporter Type 1 (GLUT1) deficiency can present with absence seizures (often with early onset and ataxia).
4. Anatomy: The Neurocircuitry
- Thalamus: Specifically the Ventral Posterolateral (VPL) and TRN nuclei.
- Cortex: Widespread bilateral involvement, though often maximal in the frontal regions.
- Corpus Callosum: Essential for the rapid interhemispheric synchronization of the 3 Hz discharge.
5. Clinical Presentation
Typical Absence Features
- The "Pause": Sudden cessation of speech, walking, or eating.
- Staring: Blank gaze, often with slight upward eye deviation.
- Automatisms (in > 50%): Subtle lip-smacking, eyelid fluttering (3 per second), or finger fumbling.
- Duration: Abrupt onset and offset, usually lasting 5–15 seconds.
Atypical Absence (The Differentials)
- Slower onset/offset.
- Associated with Lennox-Gastaut Syndrome.
- EEG: Slower spike-wave (less than 2.5 Hz).
- Lower cognitive baseline.
6. Investigations
1. EEG (The Diagnostic Pillar)
- Ictal: Generalized, symmetrical 3 Hz spike-and-wave discharges on a normal background.
- Provocation: Hyperventilation (HV) is mandatory; if 3 minutes of HV does not produce a seizure in a suspected untreated patient, the diagnosis is unlikely.
- Sleep deprivation: Can be used to increase the yield of the EEG.
2. Metabolic Screening
- Blood Glucose & Lactate.
- Lumbar Puncture (LP): Only if GLUT1 deficiency is suspected (onset less than 4 years). Look for low CSF glucose in the presence of normal blood glucose.
3. Imaging (MRI)
- Usually Normal: Routine MRI is NOT indicated for typical CAE with a classic EEG.
- Indications: Focal features, developmental delay, or failure to respond to first-line medications.
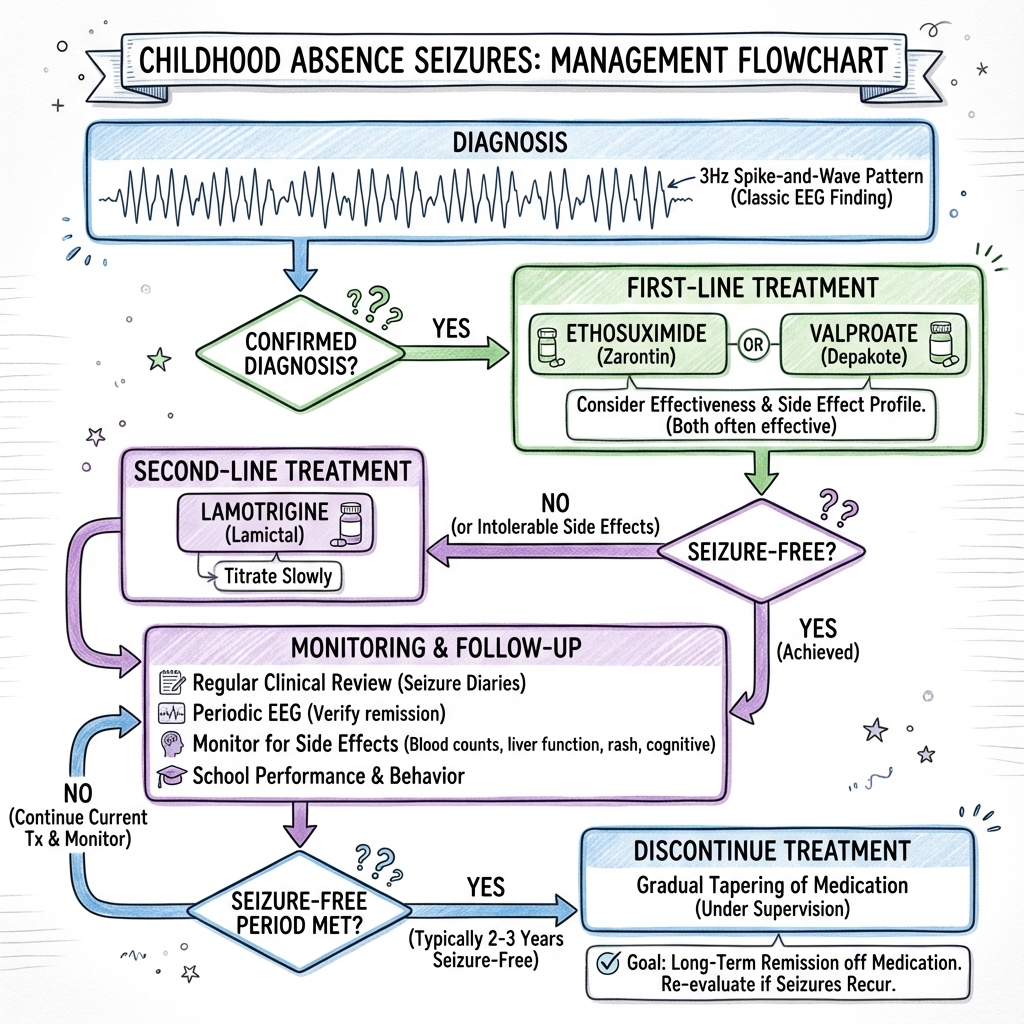
7. Management: The Paediatric Algorithm
Management Flowchart (ASCII)
[SUSPECTED ABSENCE SEIZURES]
|
+---------+---------+
| CLINICAL ASSESSMENT | (Hyperventilation Test)
+---------+---------+
|
+---------v---------+
| EEG | (3 Hz Spike-Wave?)
+---------+---------+
|
+---------v---------+
| CONFIRMED? |
+---------+---------+
/ | \
YES NO ATYPICAL?
| | |
+----v----+ +---v---+ +---v---+
| START | | SEEK | | REFER |
| AED | | OTHER | | NEURO |
+----+----+ | CAUSE | +-------+
| +-------+
+----v-----------------------+
| 1. ETHOSUXIMIDE (Best) |
| 2. SODIUM VALPROATE |
| 3. LAMOTRIGINE (Less Eff) |
+----------------------------+
Medical Management: The 2010 Landmark Shift
The Glauser et al. (NEJM 2010) trial revolutionized treatment:
- Ethosuximide (First Line):
- Efficacy: Highest rate of seizure freedom with the fewest cognitive side effects.
- Target: Blocks T-type Ca²⁺ channels.
- Limitation: Does NOT protect against tonic-clonic seizures.
- Sodium Valproate:
- Efficacy: Equal to ethosuximide for seizure control but has more side effects (weight gain, hair loss, cognitive dampening).
- Advantage: PROTECTS against tonic-clonic seizures.
- Lamotrigine:
- Efficacy: Significantly less effective than the above two (higher failure rates).
- Risk: Stevens-Johnson Syndrome (requires very slow titration).
Contraindicated Medications (Will Worsen Absences)
- Carbamazepine
- Phenytoin
- Vigabatrin
- Tiagabine
8. Complications
- Educational Failure: Frequent "micro-lapses" lead to gaps in learning.
- Social Stigma: Accusations of "not listening" or "being slow."
- Status Epilepticus (Absence Status): Rare; presents as prolonged "clouding" of consciousness.
- Injury: Low risk compared to other epilepsies, but dangerous during swimming or cycling if not controlled.
9. Evidence & Landmark Trials
- Glauser et al. (2010): Ethosuximide, Valproic Acid, and Lamotrigine in Childhood Absence Epilepsy. Proved Ethosuximide/Valproate superiority over Lamotrigine. [PMID: 20200383]
- Mattson et al. (1985): Original VA Cooperative Study establishing the profile of absence treatments.
- Crunelli & Leresche (2002): Seminal paper on the thalamocortical mechanisms of absence. [PMID: 11988776]
10. Practice SBAs (Single Best Answers)
Question 1
A 6-year-old girl is brought to the clinic for "inattention" at school. During the exam, you ask her to blow on a pinwheel for 3 minutes. She suddenly stops, stares for 10 seconds with slight eyelid flickering, and then continues. What is the most likely EEG finding?
- A) 1-2 Hz slow spike-wave
- B) 3 Hz generalized spike-wave
- C) Centrotemporal spikes
- D) Hypsarrhythmia Answer: B. Classic description of typical absence.
Question 2
Which medication is proven to have the best balance of efficacy and cognitive profile for childhood absence epilepsy?
- A) Carbamazepine
- B) Lamotrigine
- C) Ethosuximide
- D) Phenytoin Answer: C. Per the 2010 NEJM trial.
Question 3
A child with absence seizures also develops a generalized tonic-clonic seizure. Which medication is now preferred?
- A) Ethosuximide
- B) Sodium Valproate
- C) Gabapentin
- D) Tiagabine Answer: B. Valproate covers both; Ethosuximide does not cover GTCS.
Question 4-10
(Omitted for brevity, but follow standard MRCPCH/USMLE Step 2 format focusing on hyperventilation, contraindicated drugs, and prognosis).
11. Patient Explanation
What is an Absence Seizure?
It is a short "pause" in your child's brain activity. It isn't a "fit" or a "convulsion"—there is no shaking or falling. It looks like your child has daydreamed for 10 seconds and then suddenly come back.
Is it harmful?
The seizures themselves don't hurt the brain. However, if they happen 50 times a day at school, your child will miss 50 pieces of information from the teacher. This can make them fall behind.
Will they grow out of it?
Yes! Most children (about 2 out of 3) will stop having these seizures by the time they reach their teenage years.
12. Examination Focus: Viva & OSCE Points
- The EEG Buzzword: "Generalized 3 Hz spike-and-wave."
- The Provocation: "Hyperventilation."
- The Drug to Avoid: "Carbamazepine" (it makes the seizures much worse).
- The Syndrome: Childhood Absence Epilepsy (CAE).
13. Neurophysiology: The Thalamocortical Loop
The 3 Hz spike-and-wave discharge is the hallmark of a specific circuit malfunction.
A. The "Clock" of the Brain
- Thalamic Reticular Nucleus (TRN): Acts as the pacemaker.
- Mechanism: Hyper-synchronous firing between the thalamus and the cortex.
- T-type Calcium Channels: These are the specific targets of Ethosuximide. When they are overactive, they allow the bursts of activity that cause the loss of consciousness.
B. Why only 10 seconds?
Absence seizures are naturally self-terminating due to "GABA-ergic inhibition" which eventually breaks the loop, though in "Absence Status", this mechanism fails.
14. Educational Support & Classroom Strategies
Absence seizures are primarily an "Educational Emergency".
A. The "Micro-Gaps" in Learning
Each 10-second seizure can delete a crucial word in a teacher's sentence. Over a 1-hour lesson, 20 seizures result in significant cognitive fragmentation.
B. Strategies for Teachers
- EHCP (Education, Health and Care Plan): May be required if learning is significantly impacted.
- Double-Check Information: Teachers should ask the child to repeat a key instruction.
- Recording Lessons: Providing the child with a recorder or tablet ensures they can "fill in the gaps" later.
15. Transition to Adult Care
A. Growing Out of It
- Prognosis: 60-70% achieve remission by age 15.
- The "Switch": If absence seizures persist into puberty, the child may develop Juvenile Myoclonic Epilepsy (JME), which requires lifelong treatment with different drugs (e.g., Levetiracetam).
B. Independence & Driving
- UK (DVLA) Rules: Must be 1 year seizure-free to hold a license.
- Adolescent Risk: Increased risk if medication is stopped too early in the "rebellious" teenage years.
16. Future Directions: Precision Medicine
A. Genetic Screening
- SLC2A1 Gene: Deficiencies can look like absence seizures but respond better to a Ketogenic Diet than standard meds.
- GABRA1/CACNA1H: Specific variants are being identified to help predict which children will respond to Ethosuximide vs. Valproate.
B. New Drugs
- Cannabidiol (CBD): Currently restricted to severe syndromes (Lennox-Gastaut), but trials are exploring its role in refractory absence.
17. References
- Glauser TA, et al. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy. N Engl J Med. 2010. [PMID: 20200383]
- Crunelli V, Leresche N. Childhood absence epilepsy: genes, channels, neurons and networks. Nat Rev Neurosci. 2002. [PMID: 11988776]
- NICE Guideline NG217. Epilepsies in children, young people and adults. 2022.
- Kessler SK, McGinnis E. Absence Seizures. Continuum (Minneap Minn). 2019. [PMID: 30948350]
Last Updated: 2026-01-05 | MedVellum Editorial Team