Achalasia
The diagnosis has been refined by High-Resolution Manometry (HRM) and the Chicago Classification (v4.0) , which divides the disease into three distinct phenotypic patterns (Types I, II, and III) with significant...
What matters first
The diagnosis has been refined by High-Resolution Manometry (HRM) and the Chicago Classification (v4.0) , which divides the disease into three distinct phenotypic patterns (Types I, II, and III) with significant...
Rapid weight loss (less than 10kg) and age less than 60 (Pseudoachalasia)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Rapid weight loss (less than 10kg) and age less than 60 (Pseudoachalasia)
- Symptom duration less than 12 months (Malignancy risk)
- Severe nocturnal regurgitation (Aspiration risk)
- Post-procedural chest pain/fever (Perforation risk)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Achalasia (Adult)
1. Clinical Overview
Summary
Achalasia is a primary oesophageal motility disorder characterized by the failure of the Lower Oesophageal Sphincter (LOS) to relax in response to swallowing and the absence of organized peristalsis in the oesophageal body. It results from the progressive degeneration of inhibitory nitrergic neurons in the myenteric (Auerbach’s) plexus. While incurable, it is highly treatable through interventions that mechanically disrupt the LOS, such as Pneumatic Dilation (PD), Laparoscopic Heller Myotomy (LHM), or Peroral Endoscopic Myotomy (POEM). [1,2]
The diagnosis has been refined by High-Resolution Manometry (HRM) and the Chicago Classification (v4.0), which divides the disease into three distinct phenotypic patterns (Types I, II, and III) with significant prognostic implications. [3]
Historical Context
- 1674: Sir Thomas Willis described the first treatment using a whalebone with a sponge to "push" food into the stomach.
- 1929: Hurt and Rake coined the term "achalasia" (Greek: "failure to relax").
- 1913: Ernst Heller performed the first cardiomyotomy, originally as a double incision (extending to the anterior and posterior walls).
- 2008: The first human POEM was performed by Haruhiro Inoue, shifting the paradigm toward scarless endoscopic myotomy. [4]
Key Facts
- Incidence: 1.6 per 100,000 person-years; prevalence is rising due to improved survival and diagnostics. [5]
- The "Bird-Beak": Classic tapering of the distal oesophagus on barium swallow.
- Cancer Risk: 10–50x increased risk of squamous cell carcinoma due to chronic stasis and inflammation. [6]
- Pseudoachalasia: A critical differential where GEJ malignancy (e.g., gastric cardia cancer) mimics achalasia.
Clinical Pearls
The "Paradoxical Dysphagia" Pearl: Unlike mechanical obstructions (like cancer) where solids are harder to swallow than liquids, achalasia patients often report that liquids are more difficult or equally difficult to swallow compared to solids.
The "Pop" Pearl: During endoscopy, if the scope meets resistance at the GEJ but then "pops" through into the stomach with gentle pressure, it is highly suggestive of achalasia. If the resistance is fixed and doesn't "give," suspect a malignant stricture.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Age: Bimodal peak (25–40 years and > 60 years), but can occur at any age.
- Gender: Equal distribution (M:F 1:1).
- Geography: Mostly idiopathic worldwide; however, Chagas Disease (Trypanosoma cruzi) is a leading cause of secondary achalasia in South and Central America. [7]
Risk Factors Table
| Factor | Association | Mechanism |
|---|---|---|
| Autoimmunity | Moderate | Genetic susceptibility + viral trigger (e.g., HSV-1) leading to immune-mediated ganglionitis. |
| Chagas Disease | Strong (Regional) | Parasitic destruction of the myenteric plexus. |
| Allgrove Syndrome | Rare (Genetic) | Triple-A: Achalasia, Alacrima, Adrenal insufficiency. |
| HLA-DQB1 | Genetic | Specific alleles associated with increased risk in Caucasian and Japanese populations. |
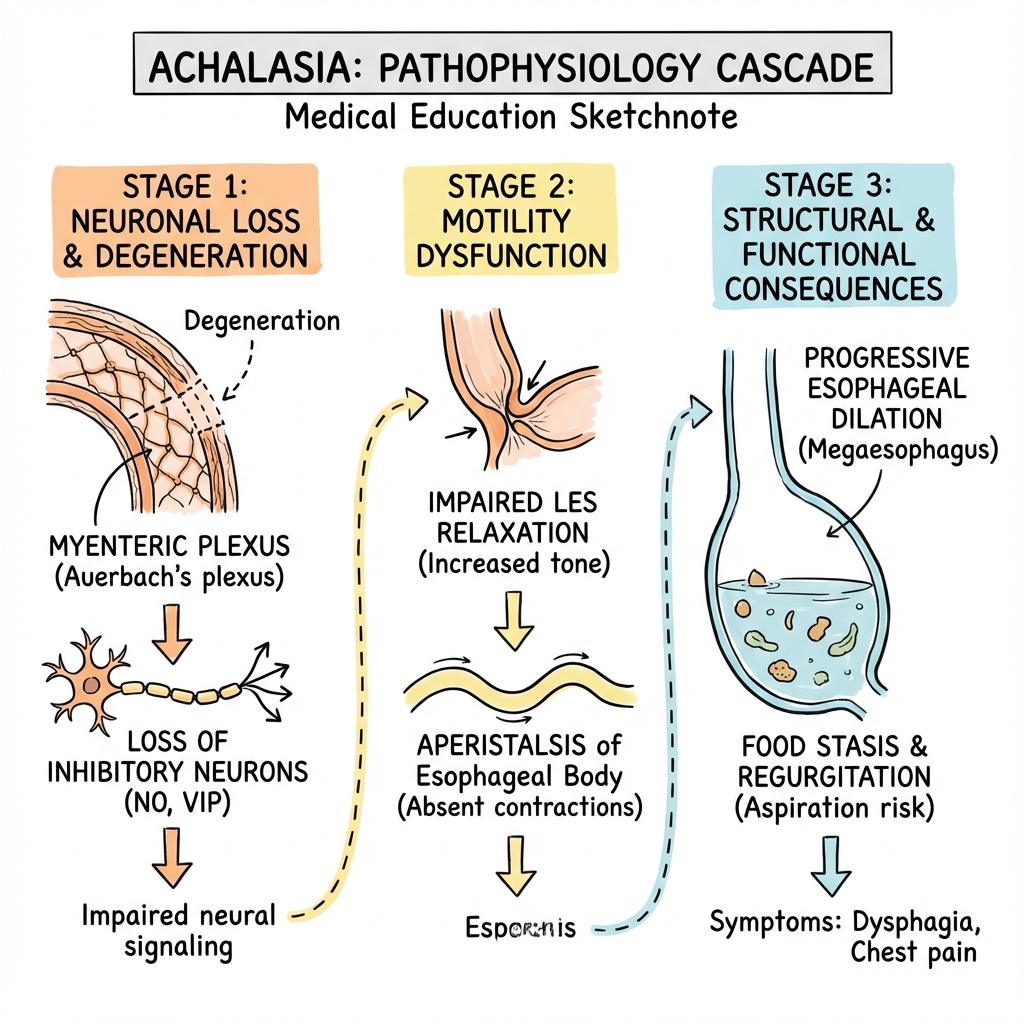
3. Pathophysiology: The Loss of Inhibition
The Myenteric Plexus Failure
Normal oesophageal relaxation is mediated by inhibitory neurons that release Nitric Oxide (NO) and Vasoactive Intestinal Peptide (VIP).
- Inflammation: An initial T-cell mediated inflammatory response (ganglionitis) targets the myenteric plexus.
- Neuronal Loss: Preferential loss of inhibitory neurons occurs, while excitatory (cholinergic) neurons are initially spared.
- The Result: The LOS remains in a state of tonic contraction (hypertension) and fails to relax. The oesophageal body loses coordinated contraction, leading to aperistalsis. [2,8]
Physics of Dilation
As the oesophagus fails to empty, it dilates. According to Laplace's Law, as the radius increases, the wall tension required to generate pressure increases. Eventually, the oesophagus becomes a massive, floppy reservoir (Mega-oesophagus or Sigmoid Oesophagus).
4. Chicago Classification v4.0 (HRM)
| Type | Pattern | IRP (mmHg) | Prognosis |
|---|---|---|---|
| Type I | Classic achalasia; no pressurization in the oesophageal body. | >ULN (usually > 15) | Good |
| Type II | Panoesophageal pressurization; > 20% of swallows show compression. | >ULN (usually > 15) | Best (> 95% response) |
| Type III | Spastic achalasia; premature or spastic contractions. | >ULN (usually > 15) | Poor (Requires POEM) |
IRP = Integrated Relaxation Pressure (median of 10 swallows).
5. Clinical Presentation
Symptoms
- Dysphagia: 99% of patients; for both solids and liquids.
- Regurgitation: 75–90%; undigested food, often nocturnal (check for "pillow soiling").
- Chest Pain: 40%; non-cardiac, often "squeezing" or spastic in nature.
- Weight Loss: Progressive; often 5–10kg by the time of diagnosis.
- Heartburn: 30%; frequently misdiagnosed as GERD, but actually due to lactic acid from food fermentation. [9]
Physical Signs
- Usually Unremarkable: Early disease has no physical signs.
- Advanced: Cachexia, halitosis (from fermented food), and signs of aspiration pneumonia (basal crackles).
6. Investigations
1. High-Resolution Manometry (HRM)
- The Gold Standard: Mandatory for diagnosis and subtyping.
- Key finding: Elevated IRP (> 15 mmHg) with 100% failed peristalsis.
2. Endoscopy (OGD)
- Mandatory: Not for diagnosis, but to exclude malignancy (Pseudoachalasia).
- Findings: Dilated lumen, retained food, and "puckered" GEJ that yields to the scope.
3. Barium Swallow (Timed Oesophagogram)
- Timed Study: Patient drinks barium; height of the column is measured at 1, 2, and 5 minutes.
- Significance: Height > 5 cm at 5 minutes suggests failure of current therapy. [10]
- Anatomy: Bird-beak tapering, air-fluid levels, and sigmoid deformity.
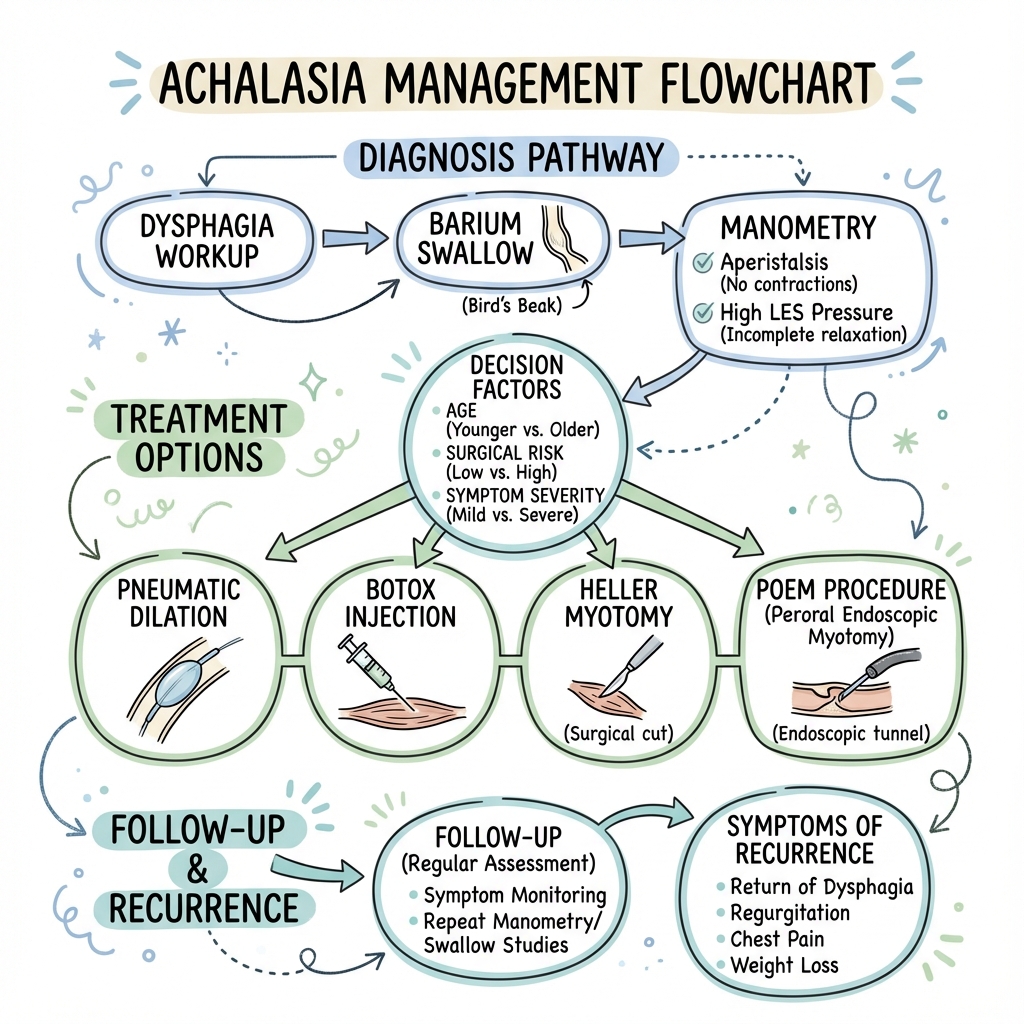
7. Management: The Treatment Algorithm
Management Flowchart (ASCII)
[CONFIRMED ACHALASIA]
|
+---------v---------+
| CHECK SUBTYPE | (HRM)
+---------+---------+
|
+----------+----------+
| |
TYPE I / II TYPE III
| (SPASTIC)
| |
+----v----+ +-----v-----+
| OPTIONS | | POEM |
+----+----+ +-----------+
|
+------+------+-------+
| | |
[LHM] [PD] [BOTOX]
(Surgery) (Balloon) (Elderly)
1. Interventional Therapies
- Laparoscopic Heller Myotomy (LHM): Cutting the LOS muscle + a partial fundoplication (Dor or Toupet) to prevent reflux.
- Peroral Endoscopic Myotomy (POEM): Endoscopic tunnel creation and myotomy. Treatment of choice for Type III. [11]
- Pneumatic Dilation (PD): Forceful stretching with 30, 35, or 40 mm balloons. Risk of perforation (1–3%).
2. Medical Management (Palliative)
- Botulinum Toxin: Endoscopic injection into LOS. Effect lasts 6–12 months. Best for elderly/comorbid patients.
- Pharmacotherapy: Calcium channel blockers (Nifedipine) or Nitrates before meals. Very low efficacy; bridge only.
8. Complications
- Aspiration Pneumonia: From nocturnal regurgitation.
- Oesophageal Perforation: Most common during Pneumatic Dilation (requires immediate surgery).
- GERD / Barrett’s: Common after POEM or LHM without a proper wrap.
- Squamous Cell Carcinoma: Requires long-term vigilance, though routine screening is not universally mandated.
9. Evidence & Landmark Trials
- European Achalasia Trial (2011): Compared LHM vs. PD. Found no significant difference in success at 2 years (90% vs 86%). However, LHM is more durable long-term. [PMID: 21561346]
- Werner et al. (NEJM 2019): POEM vs. LHM. Success rates were similar (83% vs 81.7%), but POEM had significantly higher rates of reflux oesophagitis (44% vs 29%). [PMID: 31800986]
- Ponds et al. (JAMA 2019): POEM vs. PD. POEM was superior to PD in maintaining symptom relief at 2 years. [PMID: 31287524]
10. Practice SBAs (Single Best Answers)
Question 1
A 45-year-old male presents with 2 years of progressive dysphagia to both solids and liquids. HRM shows an IRP of 22 mmHg and panoesophageal pressurization in 80% of swallows. What is the subtype and the most likely prognosis?
- A) Type I; 60% response rate
- B) Type II; > 95% response rate
- C) Type III; 40% response rate
- D) Type II; 50% response rate Answer: B. Type II (panoesophageal pressurization) has the best prognosis of all subtypes.
Question 2
Which finding on a Barium Swallow is most concerning for "Pseudoachalasia" rather than idiopathic achalasia?
- A) Bird-beak appearance
- B) Oesophageal body dilation
- C) Asymmetric, irregular mucosal thickening at the GEJ
- D) Air-fluid level in the mid-oesophagus Answer: C. Irregularity or mass-like appearance suggests malignancy.
Question 3
A 70-year-old patient with multiple comorbidities is diagnosed with achalasia but is unfit for general anesthesia. What is the most appropriate next step?
- A) Laparoscopic Heller Myotomy
- B) POEM
- C) Botulinum Toxin injection
- D) Oesophagectomy Answer: C. Botox is the treatment of choice for patients who cannot tolerate definitive surgery/interventions.
13. Advanced High-Resolution Manometry (HRM)
High-resolution manometry is not just about the numbers; it's about the waves.
A. The 3 Pillars of Diagnosis
- Integrated Relaxation Pressure (IRP): Measures the difficulty of food crossing the valve. Normal is less than 15 mmHg. In Achalasia, it is typically > 20 mmHg.
- Failed Peristalsis: The absence of any meaningful squeeze in the esophagus.
- Pressurization Types:
- Type I: No pressure (Withered).
- Type II: Full-length pressure bursts (Panoesophageal). These patients respond best to surgery.
- Type III: Spastic, high-pressure contractions. These are the hardest to treat.
B. Functional Lumen Imaging (FLIP)
- Emerging Tech: A balloon is inflated in the esophagus to measure the "stretchiness" of the valve during the actual procedure. It is becoming the "Gold Standard" for intra-operative monitoring.
14. Surgical Nuances: POEM vs. Heller Myotomy
We no longer just have "Surgery". We have incision-less surgery.
A. POEM (Peroral Endoscopic Myotomy)
- The Route: Done entirely through the mouth (endoscopically). We create a "tunnel" in the wall of the esophagus.
- The Benefit: No visible scars. Better for Type III (long spastic segments) as we can make the muscle cut much longer than in a traditional operation.
- The Catch: High risk of acid reflux post-op (GERD), as there is no "anti-reflux" wrap performed.
B. Laparoscopic Heller Myotomy (LHM)
- The Route: Traditional laparoscopic surgery through the abdomen.
- The Benefit: Always combined with a Dor or Toupet Fundoplication (a wrap to prevent reflux).
- The Catch: Requires general anesthesia and has a slightly longer hospital stay.
15. Nutritional Rehabilitation: The "Achalasia Diet"
For many, success is not just about the surgery, but how they eat.
A. The "Gravity Assisted" Lifestyle
- Posture: Patients must remain upright for at least 2 hours after any meal.
- Liquids First: Warm liquids often help to "pre-relax" the valve before solid food is introduced.
B. Avoiding the "Stasis" Trap
- Fermentation: In long-standing achalasia, food sits in the esophagus and ferments, causing "foul breath" (Halitosis). Regular flushing with water is essential.
16. Future Directions: Precision Myotomy
A. Stem Cell Therapy
- The Goal: Injecting neural progenitor cells into the lower esophageal sphincter to "regrow" the lost inhibitory neurons. (Still in animal trials).
B. AI-Driven Manometry
- Automated Scoring: Using machine learning to identify subtypes with 100% accuracy, reducing human error in reading complex pressure maps.
17. Patient Explanation
Your food pipe (oesophagus) has a valve at the bottom that is supposed to open to let food into your stomach. In your case, this valve is "stuck" closed because the nerves that tell it to relax have been damaged. We can't fix the nerves, but we can fix the valve. We do this by either stretching it with a balloon or performing a small procedure (surgery or endoscopy) to cut the muscle fibers that are keeping it tight. This allows food to drop into your stomach by gravity. After the procedure, most patients find they can eat comfortably again, though they may need to be mindful of acid reflux.
18. Examination Focus: Viva & OSCE Points
The "Gastro" Viva
- The "Bird-Beak": Be able to describe it on a barium swallow (Smooth tapering vs. irregular).
- Subtype Prognosis: Type II > I > III.
- Nutcracker Oesophagus: A common "differential" where pressure is high but the valve still relaxes.
19. References
- Vaezi MF, et al. ACG Clinical Guidelines: Achalasia. Am J Gastroenterol. 2020. [PMID: 32773454]
- Kahrilas PJ, et al. Achalasia. Lancet. 2013. [PMID: 23871239]
- Kahrilas PJ, et al. The Chicago Classification v4.0. Neurogastroenterol Motil. 2021. [PMID: 33373111]
- Inoue H, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010. [PMID: 20354937]
- Matsuda NM, et al. Chagasic achalasia. World J Gastroenterol. 2009. [PMID: 19938192]
- Khosla RR, et al. POEM for Type III Achalasia. Gastrointest Endosc. 2020. [PMID: 31926884]
Last Updated: 2026-01-05 | MedVellum Editorial Team