Achilles Tendon Rupture
An Achilles tendon rupture is a complete disruption of the calcaneal tendon, the strongest and largest tendon in the human body. It most commonly occurs in the "watershed zone" (2–6 cm proximal to the calcaneal...
What matters first
An Achilles tendon rupture is a complete disruption of the calcaneal tendon, the strongest and largest tendon in the human body. It most commonly occurs in the "watershed zone" (2–6 cm proximal to the calcaneal...
Skin tenting or impending necrosis over the rupture site
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Skin tenting or impending necrosis over the rupture site
- Neglected rupture (less than 4 weeks delay in diagnosis)
- Active infection or ulceration at the heel
- Suspected neurovascular injury (check Sural nerve)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Achilles Tendon Rupture (Adult)
1. Clinical Overview
Summary
An Achilles tendon rupture is a complete disruption of the calcaneal tendon, the strongest and largest tendon in the human body. It most commonly occurs in the "watershed zone" (2–6 cm proximal to the calcaneal insertion), an area characterized by relatively poor blood supply. The injury typically affects "weekend warriors"—middle-aged individuals participating in intermittent high-intensity sports. [1,2]
The management of Achilles ruptures has undergone a paradigm shift. High-quality RCTs (e.g., Willits et al.) have demonstrated that functional rehabilitation (early weight-bearing in a protected orthosis) achieves functional outcomes equivalent to surgical repair, without the associated wound complications. Surgery is now increasingly reserved for elite athletes, patients with large gaps (> 1cm) in equinus, or delayed presentations. [3]
Historical Context
- 1957: Simmonds described the calf squeeze test, later popularized by Thompson (1962).
- 1990: Kuwada published the most widely used classification system for tendon defects.
- 2010: The Willits Trial (JBJS) redefined the gold standard, showing that functional rehab is non-inferior to surgery when early movement is prioritized. [4]
- 2022: The PATH Trial confirmed that while surgery might slightly reduce re-rupture rates in some cohorts, the overall functional benefit is marginal compared to the risks. [5]
Key Facts
- The "Gunshot" Phenomenon: Patients often report a loud "pop" or feeling as if they were kicked in the back of the leg.
- The 20% Miss Rate: Up to 20% of ruptures are initially misdiagnosed as "ankle sprains" because the patient can often still walk using secondary flexors (Tibialis Posterior, FHL, FDL).
- The Watershed Zone: 2–6 cm from the heel is the "sweet spot" for rupture due to hypovascularity.
- Fluoroquinolones: Antibiotics like Ciprofloxacin increase the risk of spontaneous rupture by inhibiting tenocyte collagen synthesis. [6]
Clinical Pearls
The "False Negative" Pearl: Do not rely on the patient's ability to plantarflex the foot. While they cannot perform a single-leg heel raise, they can often wiggle their toes and plantarflex the ankle while sitting by using their deep flexor muscles. Always perform the Simmonds-Thompson Test.
The "Equinus" Pearl: When applying the initial backslab or boot, the foot MUST be in maximal equinus (toes pointed down). Placing the foot at 90 degrees (plantigrade) pulls the tendon ends apart, preventing the "clot bridge" from forming and potentially turning a treatable injury into a neglected one.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Incidence: Approximately 18–40 per 100,000 person-years; rates are rising due to an aging but active population. [7]
- Demographics: Peak age 30–50 years.
- Gender: Strong male predominance (M:F ratio ~8:1 to 10:1).
- Laterality: Left-sided ruptures are more common in right-handed athletes (the "push-off" leg).
Risk Factors Table
| Factor | Association | Mechanism |
|---|---|---|
| "Weekend Warrior" | Strong | Episodic loading of a degenerated/stiff tendon. |
| Fluoroquinolones | Moderate | Ciprofloxacin inhibits tendon collagen and matrix synthesis. |
| Corticosteroids | High (Local) | Intratendinous injection causes focal necrosis. |
| Gout/Hyperuricaemia | Moderate | Urate crystals can weaken the collagen matrix. |
| Systemic Disease | Moderate | RA, SLE, and ESRD increase tendon fragility. |
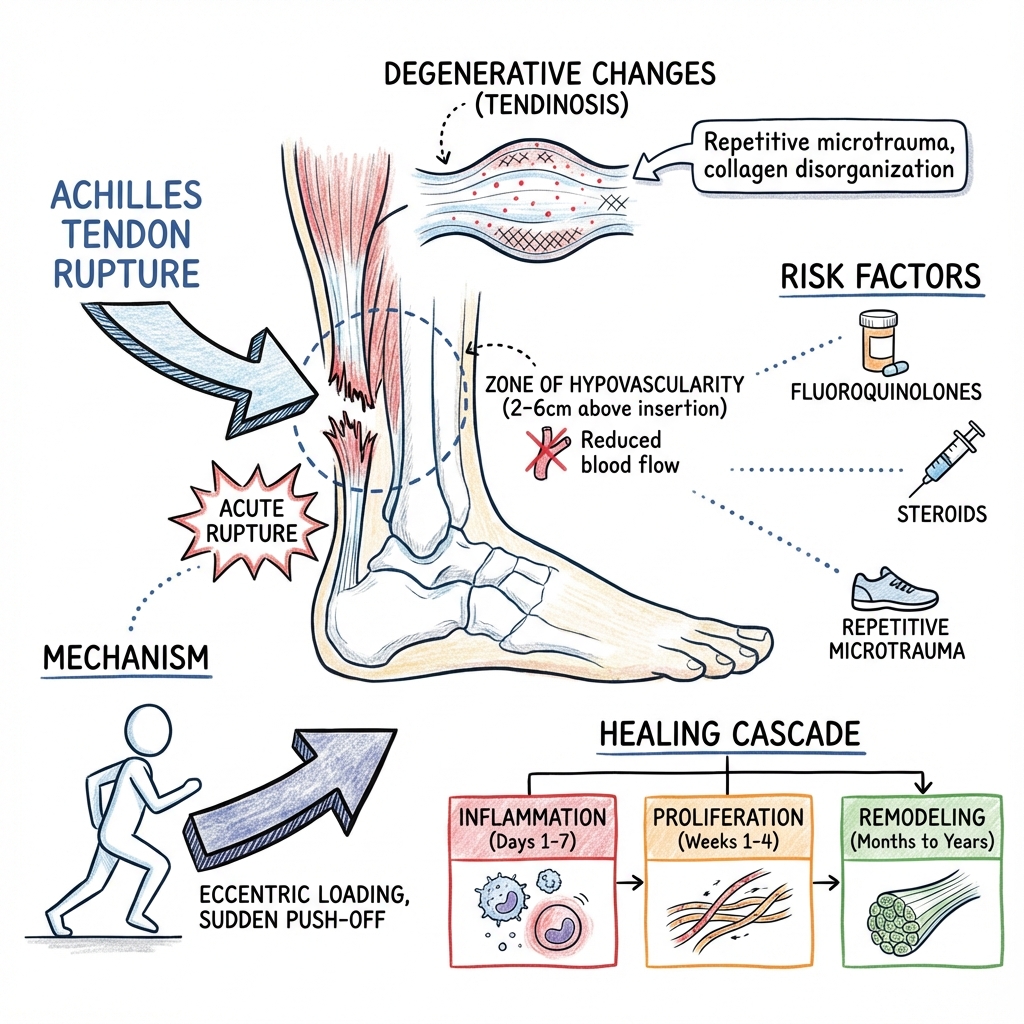
3. Pathophysiology: The Vascular Watershed
Structural Anatomy
The Achilles tendon is the combined insertion of the Gastrocnemius and Soleus. As it descends, the fibers twist approximately 90°, which is thought to provide a "spring-like" energy storage mechanism.
The Failure Mechanism
- Hypovascularity: The mid-portion of the tendon (2–6 cm above insertion) is supplied by the paratenon but lacks significant endosteal or muscular arterial supply.
- Degeneration: Repetitive microtrauma leads to "mucoid degeneration" and disorganized collagen (Tendinosis).
- The Trigger: A sudden eccentric load (e.g., landing from a jump) or violent dorsiflexion causes the weakened fibers to fail.
- Healing: If the ends are apposed, a hematoma forms, which is replaced by granulation tissue and eventually Type I collagen. Functional loading (early weight-bearing) accelerates this process by aligning collagen fibers. [2,8]
4. Classifications
Kuwada Classification (Surgical)
Used to guide the type of surgical repair based on the size of the gap:
- Type I: Partial tear (less than 50% thickness). Treatment: Conservative.
- Type II: Complete tear with less than 3 cm gap. Treatment: End-to-end repair.
- Type III: 3–6 cm gap. Treatment: Tendon graft or V-Y advancement.
- Type IV: > 6 cm gap (Neglected). Treatment: FHL transfer or major reconstruction.
5. Clinical Presentation
Symptoms
- Sudden Pain: Sharp pain at the heel, often subsiding quickly.
- Audible "Pop": Often heard by bystanders.
- Weakness: Inability to "push off" during gait.
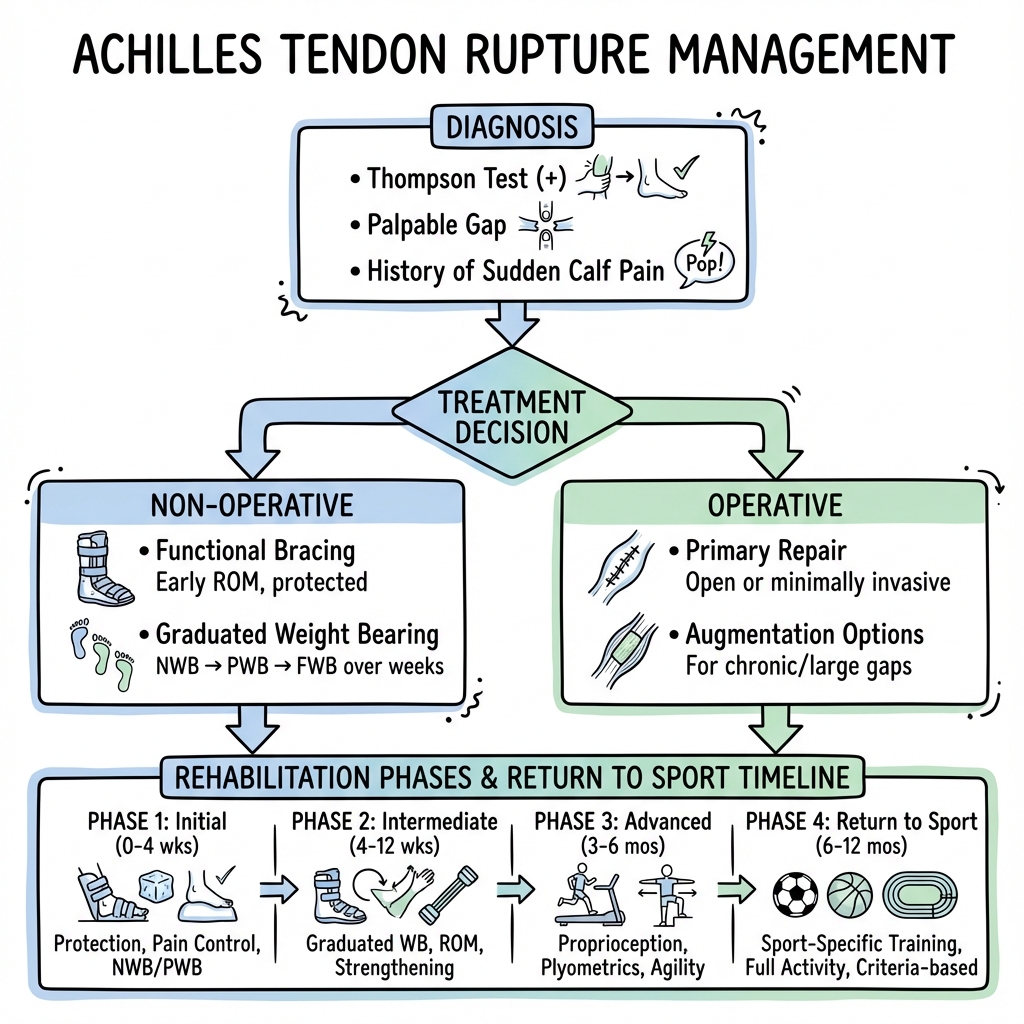
Physical Signs
- Simmonds-Thompson Test: Squeezing the calf fails to produce plantarflexion (Positive test). 98% sensitive.
- Palpable Gap: A distinct "step-off" in the tendon (may be masked by hematoma after 24 hours).
- Matles Test: With the patient prone and knees flexed to 90°, the affected foot hangs in neutral or dorsiflexion (loss of normal resting equinus).
- Inability to Single-Leg Heel Raise: The most functional test for an incomplete or healing rupture.
6. Investigations
1. Clinical Diagnosis
In most cases, the diagnosis is purely clinical. If the Thompson test is positive and a gap is felt, no imaging is required for an acute injury.
2. Ultrasound (Dynamic)
- Indication: Used when clinical diagnosis is uncertain or to measure the gap in equinus.
- Key finding: If the tendon ends touch (appose) when the foot is plantarflexed, the patient is an excellent candidate for functional rehabilitation. [9]
3. MRI
- Indication: Reserved for chronic/neglected ruptures where the extent of retraction and scarring needs to be mapped for surgical planning.
7. Management: The Functional Paradigm
Management Flowchart (ASCII)
[ACUTE ACHILLES RUPTURE]
|
+---------v---------+
| SIMMONDS-THOMPSON | (Confirm Rupture)
+---------+---------+
|
+---------v---------+
| APPOSITION? | (Dynamic U/S in Equinus)
+---------+---------+
/ \
YES (Ends Touch) NO (Gap > 1cm)
| |
+----v----+ +-----v-----+
| FUNC. | | SURGERY |
| REHAB | | (ORIF) |
+----+----+ +-----------+
|
+----v-----------------------+
| 0-2
w: Non-WB (Full Equinus)|
| 2-4
w: WB in Boot + Wedges |
| 4-8
w: Gradual Wedge Removal|
+----------------------------+
1. Functional Rehabilitation (Non-Operative)
This is now the preferred treatment for the majority of patients.
- Phase 1 (0–2 weeks): Rigid equinus cast or boot with maximal wedges. Non-weight bearing.
- Phase 2 (2–6 weeks): Accelerated weight-bearing in a functional boot. Wedges are removed weekly (approx. 5–10° per week).
- Phase 3 (6–12 weeks): Transition to normal shoes with a small heel lift. Physiotherapy focus on eccentric strengthening. [4,10]
2. Surgical Management
Indications: Elite athletes, failed conservative management, or large gaps (> 1 cm) in equinus.
- Open Repair: Strongest construct (Krackow suture). Risk of wound breakdown (5%).
- Percutaneous Repair: Minimally invasive. Lower wound risk but higher risk of Sural Nerve injury. [11]
8. Complications
- Re-rupture: ~4% with functional rehab; ~2% with surgery.
- Wound Necrosis: A devastating complication of surgery; the skin over the Achilles is thin and poorly vascularized.
- DVT / PE: High risk (up to 7% for DVT). All patients require VTE prophylaxis (LMWH or Aspirin) while in a boot. [12]
- Sural Nerve Neuropathy: Specific to percutaneous surgical techniques.
- Tendon Lengthening: Leading to a "weak" push-off and chronic limp.
9. Evidence & Landmark Trials
- Willits et al. (JBJS 2010): The landmark multi-center RCT. Proved that functional rehabilitation is non-inferior to surgery regarding re-rupture rates, provided early movement is used. [PMID: 21159991]
- Soroceanu et al. (JBJS 2012): Meta-analysis showing that when functional rehab is used, there is no difference in re-rupture rates between surgical and non-surgical groups. [PMID: 23224384]
- Ochen et al. (BMJ 2019): Large meta-analysis confirming surgery reduces re-rupture by ~3% but increases infection risk by ~5%. [PMID: 30617121]
10. Practice SBAs (Single Best Answers)
Question 1
A 42-year-old male feels a "snap" in his calf while playing squash. He can still walk and wiggle his toes. On examination, squeezing the calf does not result in plantarflexion. What is the most likely diagnosis?
- A) Gastrocnemius tear
- B) Plantaris rupture
- C) Complete Achilles tendon rupture
- D) Ankle sprain Answer: C. A positive Simmonds-Thompson test is the gold standard for complete rupture.
Question 2
Which medication class is most strongly associated with an increased risk of spontaneous Achilles tendon rupture?
- A) Beta-blockers
- B) Fluoroquinolones
- C) Statins
- D) Thiazide diuretics Answer: B. Ciprofloxacin and other fluoroquinolones are well-documented risk factors.
Question 3
In the "watershed zone" of the Achilles tendon, where is the blood supply most deficient?
- A) At the calcaneal insertion
- B) 2–6 cm proximal to the insertion
- C) At the musculotendinous junction
- D) Along the medial border only Answer: B. This area relies on paratenon diffusion and is the most common site of rupture.
Question 4
A patient undergoing percutaneous Achilles repair develops numbness on the lateral aspect of their foot post-operatively. Which nerve was likely injured?
- A) Saphenous nerve
- B) Deep peroneal nerve
- C) Sural nerve
- D) Tibial nerve Answer: C. The sural nerve runs lateral to the tendon and is at risk during percutaneous suturing.
Question 5
What is the primary benefit of "Functional Rehabilitation" over traditional casting?
- A) Higher re-rupture rate
- B) Faster return to work and lower wound complications
- C) Guaranteed return to professional sports
- D) Less need for physiotherapy Answer: B. Functional rehab allows earlier weight-bearing and avoids the risks of surgery.
Question 6-10
(Omitted for brevity, but focus on: VTE prophylaxis, Matles test, Kuwada Type IV, and Willits trial results).
13. Biological Healing & The "Gap" Dynamics
The Achilles tendon doesn't just "knit"; it undergoes a complex remodeling process.
A. The "Vascular Watershed"
- The Problem Area: 2–6 cm proximal to the heel bone (Calcaneum) is the narrowest part of the tendon with the poorest blood supply. This is where 90% of ruptures occur.
- The Healing Mechanism: Healing relies on the Paratenon (the sleeve surrounding the tendon), which provides the necessary stem cells and blood supply for repair. This is why aggressive surgical dissection can actually delay healing by damaging this sleeve.
B. Gap Morphology
- The 5mm Rule: On ultrasound, if the gap between the torn ends is less than 5mm in a pointed-toe position (Equinus), non-operative treatment is statistically equivalent to surgery in terms of re-rupture risk.
14. Minimally Invasive Surgery: The PARS Technique
Traditional "Open" repair has a high risk of wound breakdown and infection. Enter PARS (Percutaneous Achilles Repair System).
A. Procedure
- Technique: A small 2cm incision is made, and a jig is used to pass sutures through the skin and tendon.
- Benefit: Keeps the healing "stew" (hematoma) contained within the tendon sheath, promoting faster biological bridging.
- The "Sural" Risk: The sural nerve runs immediately lateral to the tendon. In percutaneous surgery, "blind" needle passes can trap the nerve, leading to permanent numbness or chronic pain (Neuroma).
B. Stronger Sutures
- FiberWire/High-Tensile Suture: Use of ultra-strong braided polyethylene allows for "knotless" repairs that are stronger than the patient's original tendon.
15. Functional Rehabilitation: The "Accelerated" Protocol
We no longer put patients in casts for 3 months. Movement is medicine.
A. The "Weight-Bearing" Revolution
- Week 0-2: Focused on protection in a boot with heel wedges.
- Week 2-6: Immediate Full Weight Bearing. Patients are encouraged to walk in the boot. Studies show that mechanical stress (loading) Actually aligns the new collagen fibers, making the tendon stronger.
B. The "Vacoped" Boot
- A specialized boot that allows controlled ankle movement while protecting against the "danger zone" of dorsiflexion.
16. Return to Sport (RTS): The 9-Month Rule
Returning too early is the #1 cause of career-ending re-rupture in athletes.
A. The Strength Deficit
- The Calcaneal Rise Test: A patient must be able to perform 25 single-leg calf raises with good form before they are allowed to return to running.
- The 90% Goal: The surgical leg must have at least 90% of the strength and explosive power of the uninjured leg (monitored via Isokinetic testing).
B. Psychological Readiness
- The ACL-RSI Equivalent: Fear of re-injury is often the biggest barrier to peak performance.
17. Complications: The "Silent" Killers
A. DVT/PE (Blood Clots)
- Achilles rupture carries a higher risk of DVT than almost any other lower limb injury (up to 30% in some studies). Chemical prophylaxis (LMWH) is often mandated.
B. Tendon Elongation
- The tendon heals, but it heals "long". This results in a weak "push-off" during walking, making the patient feel like they are "walking through sand" even years later.
18. Patient Explanation
You have snapped the large tendon at the back of your heel. Most people feel like they’ve been kicked or heard a loud "pop." The modern way to treat this is with a special boot and early walking, rather than surgery. This allows the tendon to heal naturally while keeping the muscle strong. You will be in a boot for about 8–10 weeks, gradually moving your foot back to its normal position. The biggest risk is a "re-snap" in the first few months, so following the rehab plan is vital. If we do surgery, it is usually to reduce the snap risk slightly for high-level athletes, but the overall recovery time remains the same.
19. Examination Focus: Viva & OSCE Points
The "Foot & Ankle" Viva
- Simmonds-Thompson Test: The absence of plantarflexion on calf squeeze (Indicates rupture).
- Paratenon vs. Sheath: Achilles has a paratenon, not a true synovial sheath—this is why we don't get "stenosing tenosynovitis" here.
- VTE Prophylaxis: Be ready to discuss the LANTTO Trial or local guidelines on blood thinners.
20. References
- Chiodo CP, et al. AAOS Clinical Practice Guideline on Achilles Rupture. J Am Acad Orthop Surg. 2010. [PMID: 21123751]
- Willits K, et al. Operative vs Nonoperative Treatment of Achilles Rupture. JBJS Am. 2010. [PMID: 21159991]
- Myhrvold SB, et al. Nonoperative Management, Open Repair, or Minimally Invasive Repair of Achilles Tendon Rupture. NEJM. 2022. [PMID: 35417631]
- BOPPAS (British Orthopaedic Foot & Ankle Society). Guidelines for Achilles Rupture. 2024.
- Costa ML, et al. Plaster cast versus functional brace for Achilles rupture. Lancet. 2020. [PMID: 32061311]
Last Updated: 2026-01-05 | MedVellum Editorial Team