Achondroplasia
While patients have normal intelligence and a near-normal life expectancy, the condition is associated with significant neurological and orthopaedic complications. The most critical period is infancy, where foramen...
What matters first
While patients have normal intelligence and a near-normal life expectancy, the condition is associated with significant neurological and orthopaedic complications. The most critical period is infancy, where foramen...
Central apnea or sudden infant death risk (Foramen magnum stenosis)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Central apnea or sudden infant death risk (Foramen magnum stenosis)
- Rapidly increasing head circumference (Hydrocephalus)
- New onset limb weakness or clonus (Cervicomedullary compression)
- Neurogenic claudication in adults (Spinal stenosis)
Linked comparisons
Differentials and adjacent topics worth opening next.
- Foramen Magnum Stenosis
- Spinal Stenosis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Achondroplasia (Paediatric)
1. Clinical Overview
Summary
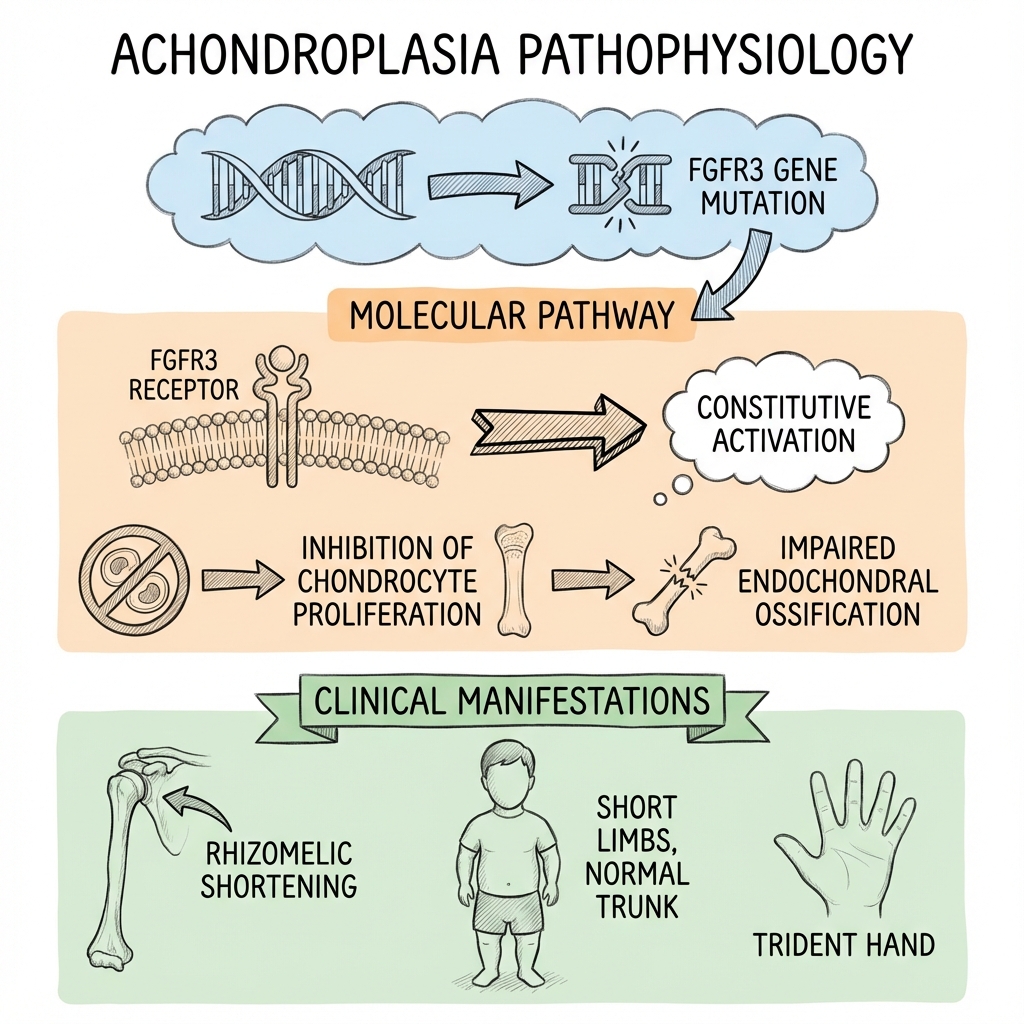
Achondroplasia is the most common form of skeletal dysplasia and the leading cause of disproportionate short stature (dwarfism). It is characterized by rhizomelic (proximal) limb shortening, macrocephaly, and characteristic midface hypoplasia. The condition is caused by a specific gain-of-function mutation in the FGFR3 gene, which constitutively inhibits chondrocyte proliferation at the growth plate. [1,2]
While patients have normal intelligence and a near-normal life expectancy, the condition is associated with significant neurological and orthopaedic complications. The most critical period is infancy, where foramen magnum stenosis poses a risk of cervicomedullary compression and sudden death. In adulthood, lumbar spinal stenosis is nearly universal due to congenitally short pedicles. Management is multidisciplinary, focusing on surveillance for complications and the recent introduction of targeted medical therapy with Vosoritide. [3,4]
Key Facts
- Incidence: 1 in 15,000 to 1 in 40,000 live births.
- Inheritance: Autosomal Dominant; however, 80% are de novo mutations associated with advanced paternal age.
- Pathophysiology: FGFR3 mutation (G380R) causing constitutive inhibition of endochondral ossification.
- The "Trident Hand": A classic finding where the 3rd and 4th fingers cannot be approximated.
- Spinal Hallmark: Decreasing interpedicular distance from L1 to L5 (the opposite of normal).
- Lethal Form: Homozygous achondroplasia (two affected parents) is lethal in the neonatal period due to thoracic restriction.
Clinical Pearls
The "Bouncer" Warning: Parents of infants with achondroplasia should be strictly advised against using "baby bouncers" or unsupported upright sitting. These positions exacerbate the natural tendency toward thoracolumbar kyphosis, which can lead to permanent vertebral wedging. [5]
The "Normal Intelligence" Pearl: It is vital to reassure parents that achondroplasia does not affect cognitive development. Any developmental delay is usually purely motor (due to a large head and ligamentous laxity) and typically resolves by age 2.
The "Anesthesia" Pearl: Always warn anesthesiologists about the risk of foramen magnum stenosis. Excessive neck extension during intubation can cause catastrophic spinal cord injury.
2. Epidemiology & Risk Factors
Incidence & Genetics
- Prevalence: Approximately 250,000 people worldwide.
- Inheritance: Autosomal Dominant with 100% penetrance.
- The Paternal Link: 80% of cases arise from de novo mutations in the sperm. The risk increases linearly with advanced paternal age (> 35–40 years) due to "selfish spermatogonial selection" where mutated cells have a proliferative advantage in the testes. [6]
Risk Factors Table
| Scenario | Risk to Offspring | Clinical Outcome |
|---|---|---|
| One Parent Affected | 50% | Heterozygous Achondroplasia (Standard phenotype). |
| Both Parents Affected | 25% | Homozygous Achondroplasia (Lethal). |
| Both Parents Affected | 50% | Heterozygous Achondroplasia. |
| Both Parents Affected | 25% | Average Stature. |
| Average Stature Parents | Low (~1/30,000) | De novo mutation (linked to paternal age). |
3. Pathophysiology: The FGFR3 Brake
Molecular Mechanism
- The Gene: Fibroblast Growth Factor Receptor 3 (FGFR3) on chromosome 4p16.3.
- The Mutation: Over 99% of cases are caused by a single point mutation: c.1138G>A or c.1138G>C, both resulting in the substitution of Glycine to Arginine at codon 380 (p.Gly380Arg). [1,7]
- The "Brake" Function: Normally, FGFR3 acts as a negative regulator of bone growth. When activated by FGF, it inhibits chondrocyte proliferation and hypertrophy in the physis (growth plate).
- Gain of Function: The G380R mutation causes the receptor to be constitutively active (independent of ligand). It's like a "brake" that is permanently stuck in the "on" position.
- Selective Inhibition:
- Endochondral Ossification: Severely inhibited. Affects long bones (limbs) and the skull base.
- Intramembranous Ossification: Unaffected. Affects the cranial vault and facial bones. This mismatch explains the large head (normal vault) and small face/base. [8]
Biomechanical Consequences
- Rhizomelia: Preferential shortening of the proximal segments (Humerus > Femur).
- Spinal Stenosis: Short, thick pedicles reduce the cross-sectional area of the spinal canal. The interpedicular distance narrows caudally, further crowding the cauda equina.
4. Clinical Presentation
Physical Characteristics
- Stature: Disproportionate short stature. Mean adult height: 131 cm (males), 124 cm (females).
- Craniofacial: Macrocephaly, frontal bossing, midface hypoplasia with a depressed nasal bridge.
- Hands/Feet: Short, broad digits. Trident hand appearance (persistent space between 3rd and 4th fingers).
- Spine:
- Infants: Thoracolumbar kyphosis (resolves with walking).
- Adults: Exaggerated lumbar lordosis.
- Legs: Genu varum (bowing) is extremely common in childhood.
Symptoms by Age
- Infancy: Sleep apnea (central or obstructive), delayed motor milestones, recurrent otitis media.
- Childhood: Leg pain, exercise intolerance, hearing loss.
- Adulthood: Neurogenic claudication (back/leg pain relieved by sitting), obesity.
5. Investigations
1. Radiology (Skeletal Survey)
- Skull: Large calvarium with a small foramen magnum and shortened skull base.
- Spine: Decreasing interpedicular distance from L1 to L5. Posterior vertebral scalloping.
- Pelvis: "Champagne glass" pelvis (square iliac wings, horizontal acetabular roofs, narrow sciatic notch).
- Long Bones: Short, thick tubular bones with "Chevron" metaphyses (v-shaped appearance where the epiphysis meets the shaft). [9]
2. Neuroimaging (MRI)
- Indication: Mandatory for all infants to assess the craniocervical junction.
- Findings: Stenosis of the foramen magnum, effacement of the CSF space, or cord signal change (myelomalacia).
3. Sleep Study (Polysomnography)
- Indication: Routine in the first year of life or if snoring/apnea is present.
- Significance: Distinguishes between central apnea (brainstem compression) and obstructive apnea (midface hypoplasia).
4. Genetic Testing
- Role: Confirms the diagnosis (G380R mutation). Essential for prenatal diagnosis if both parents are affected (to identify lethal homozygous state).
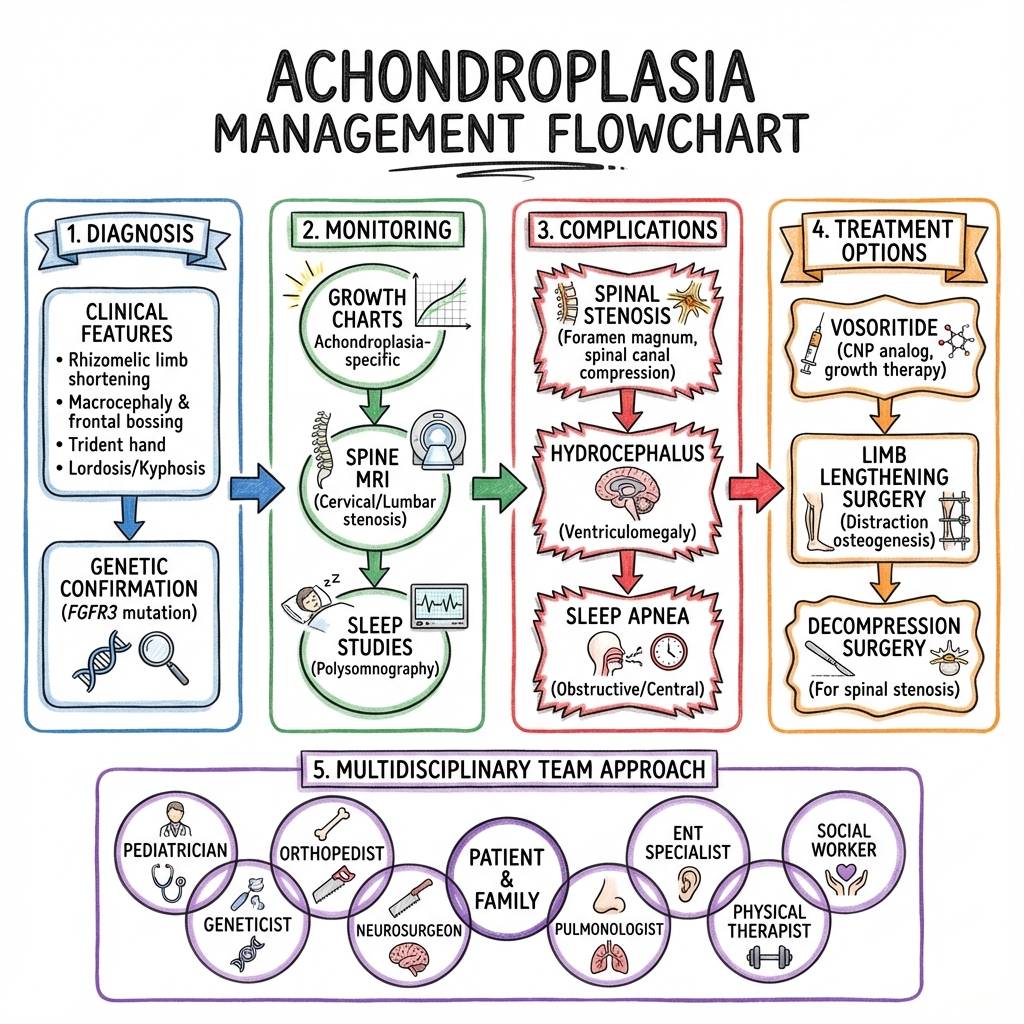
6. Management: The Multidisciplinary Approach
Management Algorithm (ASCII)
[SUSPECTED ACHONDROPLASIA]
|
+-----------v-----------+
| CONFIRM DIAGNOSIS | (Clinical + Genetic)
+-----------+-----------+
|
+-----------v-----------------------+
| INFANT SURVEILLANCE (0-2 yr) |
| - MRI Craniocervical Junction |
| - Sleep Study (Polysomnography) |
| - Monitor Head Circumference |
+-----------+-----------+-----------+
| |
+-----------v---+ +---v-----------+
| COMPLICATION | | ROUTINE |
| IDENTIFIED | | FOLLOW-UP |
+-----------+---+ +-------+-------+
| |
+-----------v-----------+ | +-----------------------+
| INTERVENTION OPTIONS | | | MEDICAL THERAPY |
| - FM Decompression | < ---+ | - Vosoritide (Voxzogo)|
| - Adenotonsillectomy | | (Ages 5-16) |
| - Bracing (Kyphosis) | +-----------------------+
| - Leg Realignment |
+-----------------------+
1. Medical Management
- Vosoritide (Voxzogo): A C-type Natriuretic Peptide (CNP) analogue.
- Mechanism: Antagonizes the FGFR3 pathway by inhibiting the MAPK/ERK signal downstream.
- Efficacy: Increases annualized growth velocity by approx. 1.5 cm/year.
- Indication: Children ≥5 years with open growth plates. [10]
2. Surgical Management
- Neurosurgery: Foramen magnum decompression if evidence of cord compression or symptomatic apnea.
- ENT: Pressure-equalizing (PE) tubes (grommets) are almost always required due to Eustachian tube dysfunction.
- Orthopaedics:
- Kyphosis: Avoid upright sitting until trunk strength is adequate. Bracing for persistent curves.
- Limb Lengthening: Highly controversial. Can add 10–15 cm but involves high complication rates and multiple surgeries over years.
7. Complications
- Sudden Infant Death: 2–5% risk in infancy due to brainstem compression.
- Hydrocephalus: Communicating type, due to impaired venous drainage at the jugular foramina.
- Obesity: Starts in early childhood; significantly worsens joint pain and spinal stenosis.
- Conductive Hearing Loss: Due to chronic otitis media with effusion.
- Neurogenic Claudication: Universal risk in adults; requires wide multi-level laminectomy.
8. Evidence & Landmark Trials
- Savarirayan et al. (Lancet 2020): Phase 3 RCT of Vosoritide. Demonstrated a mean difference in growth velocity of 1.57 cm/year vs placebo. Established the first targeted therapy. [PMID: 32891212]
- Hoover-Fong et al. (Pediatrics 2020): Updated AAP health supervision guidelines. Emphasized the need for MRI screening and specific growth charts. [PMID: 32457214]
- Willits et al. (2010): Though often cited in ortho, the most relevant natural history data comes from the CLARITY study (2021) which mapped lifetime complications in achondroplasia.
9. Single Best Answer (SBA) Questions
Question 1
A 2-week-old infant with achondroplasia is noted to have poor head control and frequent episodes of snoring. What is the most appropriate next step in management?
- A) Reassure parents that motor delay is normal
- B) Order a skeletal survey
- C) Urgent MRI of the craniocervical junction
- D) Start Vosoritide
- E) Perform a diagnostic paracentesis
- Answer: C. These are red flags for foramen magnum stenosis and cervicomedullary compression.
Question 2
The specific mutation (G380R) in achondroplasia results in which of the following molecular changes?
- A) Loss of function of a growth stimulator
- B) Gain of function of a growth inhibitor
- C) Truncation of a structural collagen protein
- D) Deficiency of an enzyme in the heme pathway
- E) Inactivation of the growth hormone receptor
- Answer: B. FGFR3 is a negative regulator (inhibitor) of bone growth. The mutation causes it to be constitutively active (gain of function).
Question 3
What is the inheritance risk for a child born to two parents who both have achondroplasia?
- A) 100% chance of being affected
- B) 50% chance of being affected, 50% average stature
- C) 25% average stature, 50% heterozygous achondroplasia, 25% lethal homozygous achondroplasia
- D) 75% chance of being affected, 25% average stature, all survivors being heterozygous
- E) 50% chance of being average stature
- Answer: C. Standard Mendelian inheritance for an autosomal dominant trait with two heterozygous parents.
Question 4
Which radiological finding is pathognomonic for the spinal changes in achondroplasia?
- A) Widening interpedicular distance from L1 to L5
- B) Bamboo spine
- C) Decreasing interpedicular distance from L1 to L5
- D) Atlanto-axial subluxation
- E) Spondylolisthesis at L5/S1
- Answer: C. Normal spines widen caudally; achondroplasia spines narrow.
Question 5
A 4-year-old child with achondroplasia is being reviewed for bowing of the legs (genu varum). Which segment of the limb is most significantly shortened?
- A) Tibia (Mesomelia)
- B) Radius (Mesomelia)
- C) Femur (Rhizomelia)
- D) Hand (Acromelia)
- E) Foot (Acromelia)
- Answer: C. Achondroplasia is a rhizomelic dysplasia (proximal segments).
Question 6
What is the primary mechanism of action of Vosoritide?
- A) Recombinant growth hormone replacement
- B) Inhibition of the RANK-L pathway
- C) Analog of C-type Natriuretic Peptide (CNP) that antagonizes FGFR3 signaling
- D) Monoclonal antibody against FGF-23
- E) Enzyme replacement for alkaline phosphatase
- Answer: C. It targets the downstream signaling of the overactive FGFR3 receptor.
Question 7
Advanced paternal age is associated with achondroplasia primarily because:
- A) Older men have more exposure to environmental toxins
- B) Spermatogonial stem cells with FGFR3 mutations have a competitive advantage (selfish selection)
- C) Maternal eggs are less receptive to mutated sperm
- D) Nondisjunction is more common in older fathers
- E) Oestrogen levels drop in the father
- Answer: B. This explains why the G380R mutation occurs so frequently at the same locus.
Question 8
Which type of bone formation is primarily impaired in achondroplasia?
- A) Intramembranous ossification
- B) Endochondral ossification
- C) Heterotopic ossification
- D) Cortical remodeling
- E) Primary intention healing
- Answer: B. Growth plates rely on endochondral ossification, which is inhibited by overactive FGFR3.
Question 9
In an infant with achondroplasia, what is the significance of "Trident Hand"?
- A) It predicts future surgical need for finger separation
- B) It is an incidental finding with no clinical significance
- C) It is a classic phenotypic marker of the condition
- D) It indicates underlying nerve entrapment
- E) It is only found in the lethal homozygous form
- Answer: C. It is a characteristic physical finding (persistent space between 3rd and 4th fingers).
Question 10
Which of the following describes the "Champagne Glass" pelvis?
- A) Deep, narrow pelvic inlet
- B) Square iliac wings and a wide, shallow pelvic inlet
- C) Excessive tilting of the sacrum
- D) Protrusio acetabuli
- E) Widening of the pubic symphysis
- Answer: B. A descriptive radiological term for the characteristic pelvic morphology.
12. Molecular Pathogenesis: The FGFR3 "Brake"
The pathology of Achondroplasia is not about a "lack" of growth, but an "overactive" brake.
A. The FGFR3 Switch
- Normal Function: Fibroblast Growth Factor Receptor 3 (FGFR3) normally acts as a negative regulator of bone growth. It tells the growth plate when to slow down.
- The Mutation (G380R): This Gain-of-Function mutation makes the FGFR3 receptor "hyper-active." It is constantly sending the "stop growing" signal to the chondrocytes (cartilage cells).
- Result: Cartilage cells in the growth plate (Endochondral ossification) fail to proliferate and organize into columns, leading to stunted longitudinal bone growth.
B. Why Only the Limbs?
- FGFR3 is most active in the long bones. The Intramembranous ossification (which forms the flat bones of the skull and the clavicle) is largely unaffected, which is why the head and torso appear relatively large compared to the limbs.
13. Complication: Foramen Magnum Stenosis & Sleep Apnea
The most life-threatening complication in infancy.
A. The "Base of Skull" Trap
- Mechanism: The bones at the base of the skull (occiput) grow via endochondral ossification. In Achondroplasia, this growth is restricted, leading to a narrow Foramen Magnum.
- Compression: This leads to Cervicomedullary Compression. Symptoms include sleep apnea, failure to thrive, and in severe cases, Sudden Infant Death Syndrome (SIDS).
B. Screening Protocol
- Mandatory MRI: Current guidelines (AAP) recommend screening MRI/CT of the craniocervical junction for all infants with achondroplasia to assess for stenosis.
14. Surgical Nuances: The Limb Lengthening Debate
Modern orthopaedics allows us to "add" height, but at a cost.
A. Distraction Osteogenesis
- Process: The bone is cut (osteotomy), and a frame (circular or internal nail) is used to slowly pull the ends apart (1mm per day).
- The Gain: It is possible to add 10-15cm of height over multiple stages.
- The Debate: It remains controversial due to high complication rates (nerve stretch, infection, joint stiffness) and the intense psychological burden on the child.
B. Spinal Stenosis
- As these children reach adulthood, Lumbar Spinal Stenosis becomes almost universal due to short pedicles. Decompression is frequently required.
15. Future Therapeutics: Vosoritide (Beyond Growth Hormone)
For decades, we had no medical treatment. That changed in 2021.
A. Vosoritide (Voxzogo)
- Mechanism: A C-type Natriuretic Peptide (CNP) analog. It works by inhibiting the downstream signaling of the overactive FGFR3 "brake."
- Impact: Clinical trials show an average of 1.57 cm per year of additional growth compared to placebo.
- Window of Opportunity: It must be given while the growth plates are still open (before puberty).
B. Meclozine
- Repurposed Drug: A common anti-motion sickness medication (Meclozine) has been found in early studies to inhibit FGFR3 signaling. It is Currently under investigation as an oral alternative to injections.
16. Patient Explanation
"Achondroplasia is the most common cause of short stature. It is a genetic condition where the 'brake' that controls bone growth in the arms and legs is stuck in the 'on' position. This leads to shorter limbs, but the head and torso are usually closer to average size. Intelligence is completely normal. In babies, we watch very closely for any pressure on the spinal cord at the base of the skull. There is a new once-daily injection called Vosoritide that can help children grow a bit faster, and we would be happy to discuss if this is right for your child."
17. Examination Focus: Viva & OSCE Points
The "Paediatric Ortho" Viva
- The "Champagne Glass" Pelvis: (Wide, shallow inlet with square iliac wings).
- Rhizomelic Shortening: (Proximal limb segments—humerus/femur—are most affected).
- Trident Hand: (Persistent space between the long and ring fingers).
18. References
- Horton WA, et al. Achondroplasia. Lancet. 2007;370(9582):162-172. [PMID: 17630040]
- Hoover-Fong J, et al. Health Supervision for People With Achondroplasia. Pediatrics. 2020;145(6). [PMID: 32457214]
- Savarirayan R, et al. Phase 3 Trial of Vosoritide for Achondroplasia. Lancet. 2020;396(10252):684-696. [PMID: 32891212]
- Pauli RM. Achondroplasia: a comprehensive clinical review. Orphanet J Rare Dis. 2019;14(1):1. [PMID: 30606190]
- Rousseau F, et al. Mutations in the gene encoding FGFR3 in achondroplasia. Nature. 1994. [PMID: 7915449]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Related Topics
Adjacent pages worth reading next.
- Foramen Magnum Stenosis
- Spinal Stenosis
- Skeletal Dysplasia Overview