ACL Injury
An Anterior Cruciate Ligament (ACL) injury is a complete or partial disruption of the primary intra-articular stabilizer of the knee. The ACL's primary role is to resist anterior translation of the tibia relative to...
What matters first
An Anterior Cruciate Ligament (ACL) injury is a complete or partial disruption of the primary intra-articular stabilizer of the knee. The ACL's primary role is to resist anterior translation of the tibia relative to...
Locked knee (Inability to fully extend, suggesting bucket-handle meniscal tear)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Locked knee (Inability to fully extend, suggesting bucket-handle meniscal tear)
- Multi-ligamentous instability (Rule out knee dislocation/Popliteal artery injury)
- Inability to weight-bear or gross deformity (Associated fracture)
- Neurovascular deficit in the foot/ankle (Peroneal nerve or vascular injury)
Linked comparisons
Differentials and adjacent topics worth opening next.
- Meniscal Tears
- PCL Injury
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
ACL Injury (Adult)
1. Clinical Overview
Summary
An Anterior Cruciate Ligament (ACL) injury is a complete or partial disruption of the primary intra-articular stabilizer of the knee. The ACL's primary role is to resist anterior translation of the tibia relative to the femur and to provide rotational stability. Injuries are predominantly non-contact in nature, occurring during sudden deceleration, pivoting, or sidestepping maneuvers. [1,2]
The management of ACL injuries has evolved from "surgery-for-all" to a more nuanced approach. High-quality evidence (e.g., the KANON Trial) suggests that for many recreational athletes, a period of high-quality rehabilitation (Pre-hab) followed by delayed reconstruction (if needed) yields functional outcomes equivalent to early surgery. However, for elite athletes or those with "coper" failure (recurrent instability), ACL Reconstruction (ACLR) remains the gold standard. Diagnosis is primarily clinical, supported by the Lachman test, and confirmed by MRI. [3,4]
Key Facts
- Mechanism: 70% are non-contact pivot/deceleration injuries.
- The "Pop": 70% of patients report an audible "pop" at the time of injury.
- Haemarthrosis: Tense swelling within 0–2 hours is highly predictive of an ACL tear.
- Gender Gap: Female athletes have a 4–6x higher risk compared to males in similar sports. [5]
- Pathognomonic Sign: The Segond fracture (lateral tibial avulsion) is 100% specific for ACL disruption.
- Graft Choice: Bone-Patellar Tendon-Bone (BPTB) and Hamstring (HT) are the most common constructs.
Clinical Pearls
The "Locked Knee" Pearl: If a patient presents with an acute ACL injury and the knee is "locked" in flexion (unable to fully extend), assume a displaced bucket-handle meniscal tear until proven otherwise. This is a surgical semi-priority to preserve the meniscus. [6]
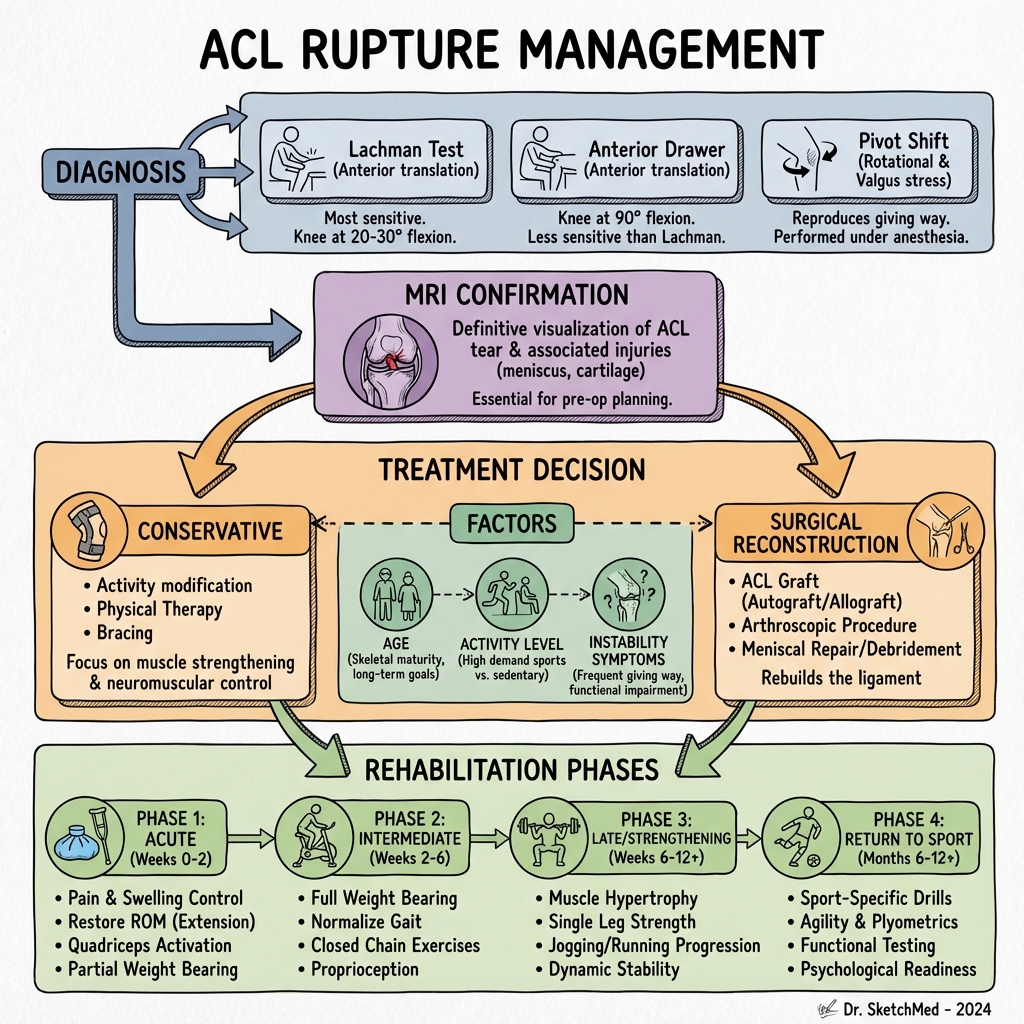
The "Lachman" Pearl: The Lachman test (at 20–30° flexion) is significantly more sensitive than the Anterior Drawer test (at 90°). At 90°, the posterior horns of the menisci can "wedge" against the femoral condyles, giving a false sense of stability.
The "Bone Bruise" Pearl: MRI "kissing contusions" on the lateral femoral condyle and posterior lateral tibial plateau are nearly pathognomonic for an ACL rupture, representing the impact of the pivot-shift event.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Incidence: 30–80 per 100,000 person-years. Approximately 250,000 ACLRs are performed annually in the US.
- Demographics: Peak incidence in the 15–25 age group.
- Sports High-Risk: Soccer, basketball, rugby, and netball (pivot-heavy sports).
Risk Factors Table
| Category | Factor | Mechanism |
|---|---|---|
| Anatomical | Narrow Intercondylar Notch | Impingement of the ligament against the lateral condyle. |
| Biomechanical | "Dynamic Valgus" | Landing with knee in valgus, hip internal rotation, and foot pronation. |
| Hormonal | Menstrual Cycle | Increased risk during the pre-ovulatory (ovulatory) phase due to oestrogen/relaxin effects on collagen. [7] |
| Environmental | High-Friction Turf | Increased shoe-surface interface torque during pivoting. |
| Neuromuscular | Quad Dominance | Relative weakness of hamstrings (which act as ACL agonists). |
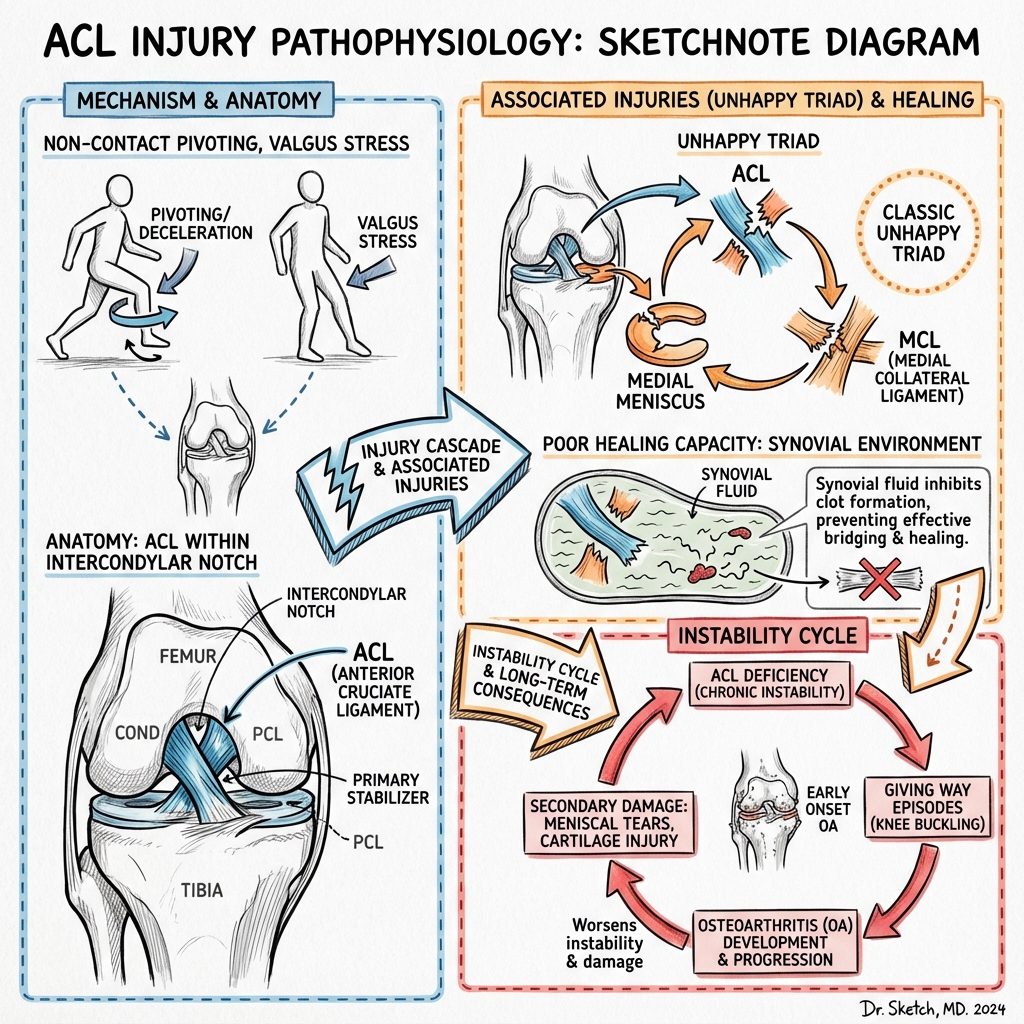
3. Pathophysiology: Anatomy & Mechanics
Structural Anatomy
The ACL is an extra-synovial, intra-articular ligament originating from the medial wall of the lateral femoral condyle and inserting into the anterior tibial eminence.
- Anteromedial (AM) Bundle: Tight in flexion; primarily resists anterior translation.
- Posterolateral (PL) Bundle: Tight in extension; primarily resists rotational torque (internal rotation).
- Blood Supply: Predominantly from the middle genicular artery. The poor blood supply is why the ACL has zero potential for primary healing. [8]
Mechanism of Rupture
- Pivot-Shift Event: A combination of valgus stress, knee flexion, and internal rotation of the tibia.
- The "Bone Bruise" Sequence: As the ACL fails, the tibia translates anteriorly and rotates. The lateral femoral condyle impacts the posterior aspect of the lateral tibial plateau, creating the characteristic MRI contusions.
- Secondary Stabilizers: Once the ACL is gone, the Medial Meniscus (posterior horn) and the MCL become the primary resistors to anterior translation. Chronic ACL deficiency inevitably leads to medial meniscal failure. [9]
4. Clinical Presentation
Symptoms
- Sudden "Pop": Often loud enough to be heard by others.
- Immediate Swelling: Tense haemarthrosis within 2 hours.
- "Giving Way": Feeling that the knee is "disjointed" or unstable.
- Inability to Continue: Most patients cannot return to the game.
Physical Signs
- Lachman Test: (Most Sensitive) Anterior pull on the tibia at 25° flexion. Positive = Increased excursion and soft/absent endpoint.
- Pivot Shift Test: (Most Specific) Starting in extension with internal rotation and valgus stress, the knee is flexed. At 30°, the tibia "clunks" as it relocates from its subluxed anterior position.
- Anterior Drawer: Performed at 90°. Often false negative due to hamstring guarding or meniscal wedging.
- Effusion: Significant "sweep" or "patellar tap" signs.
5. Investigations
1. Plain Radiography (X-ray)
- Standard Views: AP, Lateral, Tunnel (Notch), and Skyline.
- Segond Fracture: An avulsion of the lateral tibial plateau (attachment of the Anterolateral Ligament). 100% pathognomonic for ACL tear. [10]
- Deep Sulcus Sign: A notch on the lateral femoral condyle > 1.5mm deep (represents the impact site).
2. MRI (The Gold Standard)
- Direct Signs: Discontinuity of ACL fibers, horizontal orientation of the remaining stump, or "empty notch" sign.
- Indirect Signs: "Kissing contusions" (bone marrow oedema) on the lateral femoral condyle and posterior lateral tibia.
- Associated Injuries: Check for meniscal tears (Lateral in acute, Medial in chronic) and MCL sprains.
6. Management: The Modern Algorithm
Management Flowchart (ASCII)
[ACUTE ACL RUPTURE]
|
+------------v------------+
| "PRE-HAB" (3-6 WEEKS) | (Restore ROM, Reduce Swelling)
+------------+------------+
|
+------------v-----------------------+
| PATIENT SELECTION |
| - Age/Activity Level? |
| - Instability Symptoms? |
| - Associated Injuries (Meniscus)? |
+------------+-----------+-----------+
| |
+------------v---+ +---v-----------+
| SURGICAL | | CONSERVATIVE |
| (RECONSTRUCT) | | (REHAB) |
+-------+--------+ +-------+-------+
| |
+-------v-------+ +-------v-------+
| GRAFT CHOICE: | | - Physio |
| 1. BPTB | | - Propriocep. |
| 2. Hamstring | | - Activity |
| 3. Quadriceps | | Modification|
+---------------+ +---------------+
1. Conservative Management
- Indications: Sedentary patients, older age, or "copers" (individuals who can stabilize their knee via neuromuscular control).
- Protocol: Intensive physiotherapy focusing on hamstring strengthening (ACL agonist) and proprioceptive training.
- Success Rate: The KANON trial showed that approx. 50% of recreational athletes could avoid surgery with this approach. [3]
2. Surgical Reconstruction (ACLR)
- Timing: Ideally performed after the "inflammatory phase" (once ROM is restored and swelling is gone) to avoid arthrofibrosis.
- Graft Options:
- Bone-Patellar Tendon-Bone (BPTB): "Gold Standard" for athletes. Bone-to-bone healing. Highest stability. Disadvantage: Anterior knee/kneeling pain.
- Hamstring (HT): Semitendinosus/Gracilis. Strong, but slower soft-tissue-to-bone healing. Less kneeling pain.
- Quadriceps Tendon: Increasingly popular; thick graft with consistent results. [11]
7. Complications
- Arthrofibrosis: Loss of extension (Cyclops lesion). Most common when surgery is performed too early.
- Graft Rupture: 5–10% risk. Highest in the first 2 years post-op.
- Septic Arthritis: less than 1% but devastating. Requires urgent washout and often graft removal.
- Tunnel Widening: A biological response that can complicate revision surgery.
- Post-Traumatic Osteoarthritis: Risk is high (~50% at 10–15 years) regardless of surgery, though ACLR may slow progression by preventing secondary meniscal damage. [12]
8. Evidence & Landmark Trials
- Frobell et al. (KANON Trial, NEJM 2010): Landmark RCT comparing early ACLR vs. Rehab + Delayed ACLR. Found no significant difference in patient-reported outcomes (KOOS) at 2 or 5 years. [PMID: 20660401]
- Willits et al. (2010): While focused on Achilles, this trial design influenced the "Functional Rehab" mindset in ACL management.
- The MOON Cohort (2013): Large prospective study identifying risk factors for graft failure and the impact of smoking/BMI on outcomes.
9. Single Best Answer (SBA) Questions
Question 1
A 22-year-old soccer player feels a "pop" in her knee while pivoting. She develops a large, tense effusion within 60 minutes. On examination, the Lachman test is positive with a soft endpoint. What is the most likely diagnosis?
- A) Medial Meniscus tear
- B) MCL Rupture
- C) ACL Rupture
- D) Patellar dislocation
- E) Tibial plateau fracture
- Answer: C. The "pop", rapid haemarthrosis, and positive Lachman are classic for ACL injury.
Question 2
An AP X-ray of the knee shows a small avulsion fracture of the lateral tibial plateau. What is this sign called and what does it indicate?
- A) Pellegrini-Stieda lesion; MCL injury
- B) Segond fracture; ACL injury
- C) Stieda process; Ankle injury
- D) Hoffa fracture; Femoral condyle injury
- E) Maisonneuve fracture; Fibular injury
- Answer: B. A Segond fracture is pathognomonic (100% specific) for an ACL tear.
Question 3
Which of the following describes the role of the Anteromedial (AM) bundle of the ACL?
- A) It is tight in extension and resists rotational torque
- B) It is tight in flexion and primarily resists anterior translation
- C) It is the primary stabilizer against valgus stress
- D) It is intra-synovial and has a high potential for healing
- E) It originates from the medial femoral condyle
- Answer: B. The AM bundle is the primary stabilizer against anterior translation in flexion.
Question 4
Why is the Lachman test considered more sensitive than the Anterior Drawer test for acute ACL tears?
- A) It is performed in full extension
- B) It eliminates the "wedging" effect of the posterior horn of the meniscus
- C) It requires less strength from the examiner
- D) It assesses the MCL simultaneously
- E) It is not affected by quadriceps spasm
- Answer: B. At 90° (Drawer), the meniscus can block anterior translation, leading to false negatives.
Question 5
A 30-year-old female is diagnosed with an ACL tear. She is a recreational runner and does not participate in pivot sports. What does the KANON trial suggest regarding her management?
- A) Immediate surgery is mandatory to prevent arthritis
- B) A trial of structured rehabilitation is a valid first-line option
- C) Surgery is superior to rehab for all age groups
- D) Bracing is equivalent to surgery for return to sports
- E) She should never run again
- Answer: B. The KANON trial showed no difference between early ACLR and rehab + optional delayed ACLR.
Question 6
Which MRI finding is an "indirect" sign of an ACL rupture?
- A) Horizontal orientation of the ACL fibers
- B) Bone bruising on the lateral femoral condyle and posterior lateral tibia
- C) Longitudinal split tear of the MCL
- D) Baker's cyst in the popliteal fossa
- E) Increased signal in the patellar tendon
- Answer: B. "Kissing contusions" represent the pivot-shift impact.
Question 7
What is the most common complication of performing ACL reconstruction too early (within 2 weeks of injury) in a stiff knee?
- A) Graft rupture
- B) Septic arthritis
- C) Arthrofibrosis
- D) Peroneal nerve palsy
- E) Patellar fracture
- Answer: C. Surgery in an inflamed, stiff knee significantly increases the risk of permanent stiffness.
Question 8
Which graft type is associated with the highest incidence of post-operative kneeling pain?
- A) Hamstring (HT)
- B) Allograft
- C) Bone-Patellar Tendon-Bone (BPTB)
- D) Quadriceps tendon
- E) Synthetic (LARS)
- Answer: C. Due to the harvest of the bone plug from the patella and tibial tuberosity.
Question 9
In the female athlete, which anatomical factor is most strongly associated with the increased risk of ACL injury?
- A) Smaller Q-angle
- B) Wider intercondylar notch
- C) Narrower intercondylar notch
- D) Increased hamstring strength
- E) Decreased ligamentous laxity
- Answer: C. A narrow notch can "guillotine" the ligament during extreme maneuvers.
Question 10
The "Pivot Shift" test primarily assesses which component of knee stability?
- A) Simple anterior translation
- B) Valgus stability
- C) Rotational stability
- D) Varus stability
- E) Posterior translation
- Answer: C. It is the most specific test for the rotational instability caused by ACL deficiency.
12. Surgical Nuances: Graft Selection
The choice of "spare part" determines the long-term outcome and morbidity.
A. Bone-Patellar Tendon-Bone (BPTB)
- Pros: Gold standard for "rock-solid" stability; bone-to-bone healing is faster.
- Cons: Significant risk of Anterior Knee Pain and pain when kneeling.
- Ideal for: Elite athletes (footballers, NBA players).
B. Hamstring Autograft (Semitendinosus/Gracilis)
- Pros: Smaller incision; no kneeling pain.
- Cons: Risk of hamstring weakness; slightly higher "stretch" (laxity) over time.
- Ideal for: Recreational athletes and general population.
C. Quadriceps Tendon
- Role: Emerging as a "middle ground" with high graft volume and low morbidity.
13. Rehabilitation Science: Beyond the Exercises
Success is 20% surgery and 80% physiotherapy.
A. Blood Flow Restriction (BFR) Training
- Concept: Using a tourniquet during low-load exercises to simulate high-load muscle hypertrophy.
- Benefit: Allows the patient to build muscle without stressing the new graft.
B. The 9-Month Rule
- Evidence: Each month return to sport is delayed (up to 9 months), the risk of re-rupture drops by ~50%.
- Biological Healing: The "Ligamentization" process (where the tendon graft turns into a ligament) takes 12-24 months.
14. Injury Prevention: FIFA 11+
A. Neuromuscular Training
- Concept: Teaching the brain to control the knee during landing and cutting.
- The "Valgus" Trap: Training out the "knees-in" landing pattern.
B. FIFA 11+ Program
- Impact: Implementing this 20-minute warm-up reduces ACL injuries by up to 50% in youth and amateur teams.
15. Psychology of Sport: Kinesiophobia
A. The "Fear of Re-injury"
- TSK (Tampa Scale of Kinesiophobia): A vital metric. High scores corelate with failure to return to previous level of play, even if the knee is physically perfect.
B. ACL-RSI (Return to Sport after Injury) Scale
- Mental readiness is now considered as important as physical strength for "Clearance" to play.
16. Patient Explanation
"The ACL is the main 'seatbelt' inside your knee that keeps it stable when you turn or pivot. You have snapped this ligament. Most people feel a 'pop' and the knee swells up very quickly because of bleeding. We don't have to rush into surgery. In fact, it's often better to do 6 weeks of physiotherapy first to get the knee moving. If the knee still feels wobbly after that, we can discuss a 'reconstruction' where we use a piece of your own tendon to build a new ligament. If you don't do pivoting sports, you might find that physiotherapy alone is enough."
17. Examination Focus: Viva & OSCE Points
The "Orthopaedic" Viva
- The "Unhappy Triad" (O'Donoghue's): ACL tear, Medial Meniscus tear, and MCL tear.
- Segond Fracture: A small avulsion of the lateral tibial plateau. It is pathognomonic (proves) an ACL tear on X-ray.
- Graft Ligamentization: Explain the 4 phases (Ischaemia, Necrosis, Proliferation, Remodelling).
18. References
- Griffin LY, et al. Noncontact ACL injuries: risk factors and prevention. J Am Acad Orthop Surg. 2000;8(3):141-150.
- Spindler KP, et al. Anterior Cruciate Ligament Tear. N Engl J Med. 2018;378(10):960-961.
- Frobell RB, et al. A randomized trial of treatment for acute ACL tears. N Engl J Med. 2010;363(4):331-342. [PMID: 20660401]
- Ardern CL, et al. Return to sport following ACL reconstruction. Br J Sports Med. 2014.
- Prodromos CC, et al. Incidence of ACL tears as a function of gender and sport. Arthroscopy. 2007.
- Shelbourne KD, et al. Arthrofibrosis in acute ACL reconstruction. Am J Sports Med. 1991.
- Hewett TE, et al. Biomechanical measures of neuromuscular control and valgus loading. Am J Sports Med. 2005.
- Barrett GR, et al. The "watershed" lesion of the ACL. Arthroscopy. 1991.
- Daniel DM, et al. Fate of the ACL-injured patient. Am J Sports Med. 1994.
- Segond P. Reserches sur les epanchements sanguins du genou. Progres Med. 1879.
- Magnussen RA, et al. Graft failure after ACL reconstruction. Am J Sports Med. 2012.
- Lohmander LS, et al. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007.
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Related Topics
Adjacent pages worth reading next.
- Meniscal Tears
- PCL Injury
- Knee Dislocation