Acute-on-Chronic Liver Failure (ACLF)
Key Facts Incidence : Occurs in 25–35% of patients hospitalized for acute decompensation of cirrhosis. Mortality : 28-day mortality ranges from 23% (Grade 1) to 75% (Grade 3). Pathophysiology : Massive systemic...
What matters first
Key Facts Incidence : Occurs in 25–35% of patients hospitalized for acute decompensation of cirrhosis. Mortality : 28-day mortality ranges from 23% (Grade 1) to 75% (Grade 3). Pathophysiology : Massive systemic...
New onset Grade III/IV Hepatic Encephalopathy (Airway risk)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.

Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- New onset Grade III/IV Hepatic Encephalopathy (Airway risk)
- Refractory Hypotension (Shock)
- Anuria or rapidly rising Creatinine (AKI)
- Severe Hypoxaemia (PaO2/FiO2 less than 200)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acute-on-Chronic Liver Failure (ACLF)
1. Clinical Overview
Summary
Acute-on-Chronic Liver Failure (ACLF) is a distinct clinical syndrome occurring in patients with chronic liver disease (typically cirrhosis) characterized by acute decompensation, organ failure, and high short-term mortality (> 15% at 28 days). [1] Unlike traditional decompensated cirrhosis, ACLF is driven by intense systemic inflammation and a "cytokine storm," leading to extra-hepatic organ failures (renal, cerebral, circulatory, respiratory). [2] The definition varies slightly between the EASL-CLIF (Western) and APASL (Eastern) criteria, but both emphasize the critical nature of the syndrome and the narrow window for therapeutic intervention. [3]
Key Facts
- Incidence: Occurs in 25–35% of patients hospitalized for acute decompensation of cirrhosis. [1]
- Mortality: 28-day mortality ranges from 23% (Grade 1) to > 75% (Grade 3). [1]
- Pathophysiology: Massive systemic inflammatory response syndrome (SIRS) triggered by PAMPs (infection) or DAMPs (tissue injury). [4]
- Gold Standard Score: CLIF-C ACLF Score for prognosis; CLIF-C OF Score for diagnosis. [5]
- Primary Goal: Immediate identification of the precipitant, multi-organ support in ICU, and rapid assessment for liver transplantation. [6]
Clinical Pearls
The "Silent Sepsis" Pearl: Cirrhotic patients often fail to mount a fever or leucocytosis due to immunoparesis. A "normal" temperature and WBC count do NOT exclude life-threatening infection. Always perform a diagnostic paracentesis and pan-culture on admission. [7]
The "Creatinine Trap" Pearl: Serum creatinine often underestimates renal dysfunction in cirrhosis due to low muscle mass. A creatinine of 100 µmol/L may already represent significant Stage 2 AKI. [8]
The "Early Transplant" Pearl: Transplant survival for ACLF-3 is > 80% at 1 year, compared to less than 10% without transplant. The "window of opportunity" is narrow; delay in referral usually results in the patient becoming "too sick to transplant." [9]
2. Epidemiology
Incidence and Global Burden
- Western Countries: Sepsis (33%) and active alcohol consumption (25%) are the primary precipitants. [1]
- Eastern Countries: Reactivation of Hepatitis B (HBV) is the most common trigger (up to 70%). [3]
- Impact: ACLF accounts for a significant proportion of liver-related deaths and healthcare costs globally.
Risk Factors
| Patient Factors | Acute Insults ("The Hits") |
|---|---|
| Decompensated Cirrhosis | Bacterial Infection (SBP, Pneumonia, UTI) |
| Active Alcohol Use Disorder | Active Alcoholic Hepatitis |
| Chronic Viral Hepatitis (B or C) | Variceal Haemorrhage |
| Sarcopenia / Frailty | Major Surgery / Trauma |
| Non-Alcoholic Fatty Liver (MASLD) | Drug-Induced Liver Injury (DILI) |
3. Pathophysiology
The "Cytokine Storm" Mechanism
- Trigger: Bacterial translocation from the gut (PAMPs) or sterile tissue injury (DAMPs). [4]
- Activation: Recognition by Toll-like receptors (TLRs) on innate immune cells.
- Cascade: Massive release of pro-inflammatory cytokines (TNF-α, IL-6, IL-1β). [2]
- Organ Failure: Cytopathic hypoxia, microvascular dysfunction, and mitochondrial failure lead to organ dysfunction even in the presence of adequate macro-circulation. [4]
- Immunoparesis: A subsequent "compensatory anti-inflammatory response syndrome" (CARS) leads to profound immune exhaustion and high risk of secondary fungal/MDR bacterial infections. [7]
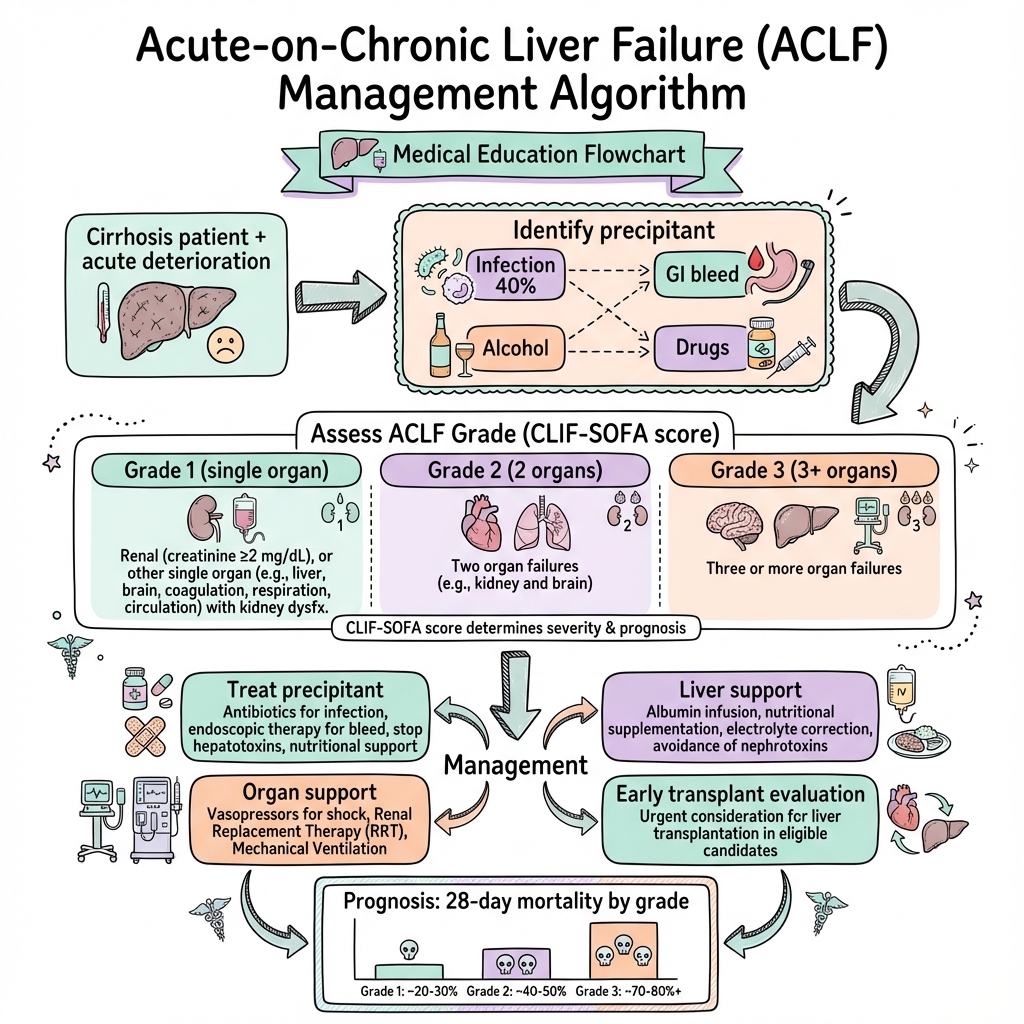
Classification (EASL-CLIF)
ACLF is graded based on the number of organ failures (Liver, Kidney, Brain, Coagulation, Circulation, Respiration): [1]
- ACLF Grade 1:
- Single kidney failure (Cr ≥ 2.0 mg/dL).
- Single non-kidney failure with kidney dysfunction (Cr 1.5–1.9) or Grade I/II HE.
- ACLF Grade 2: Two organ failures.
- ACLF Grade 3: Three or more organ failures (highest mortality).
4. Presentation
Symptoms
- Jaundice: Rapidly worsening yellowing of skin and sclera.
- Encephalopathy: Confusion, altered sleep-wake cycle, or coma.
- Oliguria: Sudden drop in urine output.
- Abdominal Pain: Often suggests Spontaneous Bacterial Peritonitis (SBP).
- Fatigue: Profound and rapidly progressive.
History Checklist
- Precipitant Hunt: Recent alcohol binge? Missed antivirals? Recent procedure?
- Infection Screen: Cough, dysuria, abdominal pain, skin redness?
- Baseline Function: Previous Child-Pugh or MELD score?
- Medication Review: Recent NSAIDs, aminoglycosides, or "liver tonics"?
5. Examination
The "ACLF Crisis" Exam
- Neuro: Grade I-IV Hepatic Encephalopathy. Check for asterixis (absent in deep coma).
- Circulation: Tachycardia, hypotension, bounding pulses (hyperdynamic circulation). Cold peripheries suggest late-stage shock.
- Abdomen: Distension (ascites), tenderness (SBP).
- Infection: Check for cellulitis, dental abscess, or infected lines.
6. Investigations
Immediate ("Golden Hour") Tests
- Bloods: FBC (WBC count), U&Es (Creatinine is critical), LFTs (Bilirubin > 200 µmol/L), INR (> 2.5), Lactate, Blood Cultures x2.
- Paracentesis: Mandatory if ascites present. Neutrophil count > 250 cells/mm³ = SBP. [10]
- Imaging: CXR (Pneumonia), Renal Ultrasound, Doppler US (Rule out Portal Vein Thrombosis).
- Prognostic Scores: Calculate CLIF-C ACLF and MELD-Na immediately. [5]
7. Management
Management Algorithm (ASCII)
+---------------------------------------------------------+
| SUSPECTED ACLF (Acute Decomp + OF) |
+---------------------------+-----------------------------+
|
+---------------V----------------+
| 1. STABILIZATION & SCREEN |
| - ABCDE (Airway if HE Gr 3/4) |
| - Aggressive Fluid (Albumin) |
| - MANDATORY Paracentesis |
+---------------+----------------+
|
+---------------V----------------+
| 2. TREAT THE PRECIPITANT |
| - Sepsis: Broad Abx less than 1hr |
| - Alc Hep: Steroids? |
| - HBV: Tenofovir/Entecavir |
+-------+----------------+-------+
| |
+-----------V-----------+ +-------V-----------+
| ORGAN SUPPORT | | TRANSPLANT |
| - Terlipressin (AKI) | | - Early Referral |
| - Vasopressors (Shock)| | - Rule out Cntra- |
| - CVVH (Renal) | | indications |
+-----------+-----------+ +-------+-----------+
| |
+-------V------------------------V-------+
| 3. MONITOR DYNAMICS (Day 3-7) |
| - Improving? Continue support. |
| - Worsening? Palliative care if |
| not a transplant candidate. |
+----------------------------------------+
Specific Therapies
- Sepsis: Piperacillin/Tazocin or Meropenem. Do not wait for cultures. [7]
- AKI / HRS: Terlipressin (IV infusion 2-12mg/day) + Albumin (20% 40g/day). [11]
- Hepatic Encephalopathy: Lactulose, Rifaximin, and Phosphate Enemas.
- Alcoholic Hepatitis: Prednisolone 40mg/day if Lille score at Day 7 suggests response (avoid if sepsis/bleed). [12]
8. Complications & Emergencies
- Cerebral Oedema: Rare in ACLF compared to ALF but possible.
- Secondary Infections: Fungal infections (Aspergillus) are common in Grade 3.
- Variceal Bleeding: Use Terlipressin + Prophylactic Abx + Early Banding. [13]
9. Prognosis
The "Day 7" Rule
Dynamics are crucial. Patients whose CLIF-C ACLF score improves between Day 3 and Day 7 have a much better prognosis. Those with Grade 3 ACLF that does not improve by Day 7 have a 28-day mortality approaching 100% without transplant. [14]
10. Evidence & Landmark Trials
- CANONIC (2013): The foundational study that defined ACLF as a distinct syndrome from decompensated cirrhosis. [1]
- STOPAH (2015): Demonstrated that Prednisolone improves 28-day survival in severe Alcoholic Hepatitis but not 90-day survival. [12]
- CONFIRM (2021): Randomized trial confirming Terlipressin's efficacy in HRS-AKI, though highlighting the risk of respiratory failure. [11]
- LIVER-HOPE (2020): Demonstrated that Simvastatin and Rifaximin may reduce systemic inflammation.
11. Professional Guidelines Comparison
| Feature | EASL-CLIF (West) | APASL (East) | AASLD (USA) |
|---|---|---|---|
| Foundation | Cirrhosis (Comp or Decomp) | Cirrhosis or Non-Cirrhotic | Similar to EASL |
| Criteria | Organ failure based (CLIF-OF) | Bilirubin/INR/Ascites/HE | Focus on SIRS/OF |
| Key Trigger | Alcohol / Sepsis | HBV Reactivation | Alcohol / Sepsis |
15. Pathophysiological Surge: The Cytokine Storm
ACLF is not just liver disease; it is a Systemic Inflammatory Response Syndrome (SIRS).
A. The "Two-Hit" Hypothesis
- Hit 1 (Chronic): The underlying cirrhosis leads to "Leaky Gut" and bacterial translocation.
- Hit 2 (Acute): A precipitant (Infection, Alcohol surge) triggers a massive release of PAMPs (Pathogen-Associated Molecular Patterns) and DAMPs (Damage-Associated Molecular Patterns).
B. The Immune Paralysis
- After the initial "storm," the immune system often crashes (CARS - Compensatory Anti-inflammatory Response Syndrome). This makes ACLF patients profoundly susceptible to secondary fungal infections (Aspergillus/Candida).
16. Critical Care: Terlipressin & Albumin Nuances
Management of the failing kidney (HRS-ACLF).
A. The Terlipressin Trial (CONFIRM)
- Mechanism: A vasopressin analog that causes potent splanchnic vasoconstriction, moving blood back into the central circulation.
- The Respiratory Risk: Potent vasoconstriction can lead to "pulmonary edema." Terlipressin should be used with caution (or avoided) in patients with severe hypoxia (PaO2/FiO2 less than 200).
B. Albumin: The "Multifunctional" Molecule
- It's not just for volume. High-dose albumin (20% solution) acts as an antioxidant and "binds" the toxic cytokines circulating in the blood.
17. Extracorporeal Support: DIALIVE vs. MARS
Can we "dialyze" the liver toxins?
A. MARS (Molecular Adsorbent Recirculating System)
- How it works: Uses albumin-coated membranes to "scrub" the blood of bilirubin and bile acids.
- Evidence: While it improves biochemistry, large trials (RELIEF) have struggled to show a definitive survival benefit compared to standard care.
B. DIALIVE (The New Frontier)
- Concept: A dual-action system that removes "damaged" albumin and replaces it with "fresh" albumin. Early Phase II trials show promising results in reversing organ failure more rapidly than standard dialysis.
18. Ethical Boundary: The "Futile" ACLF-3 & Transplant Window
When is it "too late" for a transplant?
A. The CLIF-C ACLF Score
- A prognostic score (0-100) that is superior to MELD in predicting multi-organ failure mortality.
- ACLF-3 (3+ failing organs): Has a 28-day mortality of > 50%.
B. The "Window of Opportunity"
- The Rule of 7: Many centers use a 7-day observation period. If a patient remains in ACLF-3 with no improvement after a week of "maximal" therapy, they are often deemed "too sick to transplant."
19. Patient Explanation
"Your liver disease has suddenly worsened because of an 'extra' stress like an infection. This has caused a 'fire' in your body (inflammation) that is making other organs like your kidneys struggle. We need to put out that fire with medicine and support your organs while the liver tries to recover. In some cases, if the liver doesn't get better, we may need to discuss a liver transplant."
20. Examination Focus: Viva & OSCE Points
The "Liver" Viva
- EASL-CLIF vs. APASL: Know that EASL requires organ failure (SOFA-based), while APASL focuses on the liver itself (Bilirubin/INR).
- The "Dynamic" MAP: In ACLF, the standard MAP of 65 is often not enough to perfuse the kidneys; some guidelines suggest aiming for 75-80 mmHg if there is HRS.
- Transplant Futility: If a patient has ACLF Grade 3 (3+ organ failures) and is not improving after 7 days, the transplant survival benefit drops significantly.
21. References
- Arroyo V, et al. Acute-on-chronic liver failure. Nat Rev Dis Primers. 2016. [PMID: 27278434]
- Moreau R, et al. Acute-on-chronic liver failure is a distinct syndrome... (CANONIC study). Gastroenterology. 2013. [PMID: 23542331]
- Wong F, et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome (CONFIRM Trial). NEJM. 2021. [PMID: 33657294]
- Jalan R, et al. The CLIF-C ACLF score for prognosticating outcomes. J Hepatol. 2014. [PMID: 24951929]
- Bañares R, et al. Extracorporeal albumin dialysis with the MARS system (RELIEF study). Hepatology. 2013. [PMID: 23225133]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for acute-on-chronic liver failure (aclf)?
Seek immediate emergency care if you experience any of the following warning signs: New onset Grade III/IV Hepatic Encephalopathy (Airway risk), Refractory Hypotension (Shock), Anuria or rapidly rising Creatinine (AKI), Severe Hypoxaemia (PaO2/FiO2 less than 200), Active Variceal Haemorrhage.