Acromegaly
The condition is insidious, with a median delay in diagnosis of 7–10 years . During this period, patients develop significant comorbidities, including hypertension, diabetes mellitus, cardiomyopathy, and obstructive...
What matters first
The condition is insidious, with a median delay in diagnosis of 7–10 years . During this period, patients develop significant comorbidities, including hypertension, diabetes mellitus, cardiomyopathy, and obstructive...
New-onset bitemporal hemianopia (Acute chiasmal compression)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- New-onset bitemporal hemianopia (Acute chiasmal compression)
- Pituitary apoplexy (Sudden severe headache, vomiting, visual loss, ophthalmoplegia)
- Severe congestive heart failure (Acromegalic cardiomyopathy)
- Large bowel obstruction or change in bowel habit (High risk of colorectal malignancy)
Linked comparisons
Differentials and adjacent topics worth opening next.
- Pituitary Apoplexy
- Diabetes Mellitus Type 2
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acromegaly (Adult)
1. Clinical Overview
Summary
Acromegaly is a rare, chronic multisystem disorder characterized by excessive secretion of Growth Hormone (GH), which subsequently stimulates the overproduction of Insulin-like Growth Factor 1 (IGF-1). In > 95% of cases, this is caused by a benign GH-secreting pituitary somatotroph adenoma. In adults, because the epiphyseal plates are fused, the hormone excess leads to the characteristic overgrowth of soft tissues and membranous bones (Acromegaly), whereas in children, it results in Gigantism. [1,2]
The condition is insidious, with a median delay in diagnosis of 7–10 years. During this period, patients develop significant comorbidities, including hypertension, diabetes mellitus, cardiomyopathy, and obstructive sleep apnea. If untreated, acromegaly is associated with a 2-to-3-fold increase in mortality, primarily from cardiovascular disease. Early biochemical control (normalizing IGF-1 and GH) restores life expectancy to that of the general population. [3,4]
Key Facts
- Insidious Progression: Facial changes are so slow that they are often only recognized by comparing old photographs.
- IGF-1: The primary screening tool; its stable half-life makes it superior to pulsatile GH measurements.
- The "Gold Standard" Diagnosis: Failure to suppress GH to less than 0.4 µg/L during an Oral Glucose Tolerance Test (OGTT).
- Cardiovascular Risk: Cardiomyopathy is the leading cause of death in uncontrolled acromegaly.
- Oncological Risk: Significant association with colorectal polyps and carcinoma; screening colonoscopy is mandatory at diagnosis. [5]
Clinical Pearls
The "Old Photo" Pearl: When acromegaly is suspected, ask the patient to bring in a driver's license or passport photo from 10 years ago. The coarsening of facial features and widening of the nose/jaw becomes strikingly obvious.
The "Ring/Shoe" Pearl: Always ask about changes in ring or shoe size. A patient needing to have their wedding ring cut off or widened is a classic presenting complaint.
The "Sweat" Pearl: Excess GH causes hypertrophy of sweat and sebaceous glands. Improvement in "doughy" skin texture and hyperhidrosis (excessive sweating) is one of the first clinical signs of successful treatment.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Prevalence: 40–125 per million inhabitants.
- Incidence: 3–11 cases per million person-years.
- Age: Most commonly diagnosed in the 4th and 5th decades of life (age 30–50).
- Gender: No significant gender predilection.
Genetic & Clinical Associations
| Association | Genetic/Molecular Feature | Clinical Context |
|---|---|---|
| Sporadic Adenoma | gsp oncogene (GNAS1 mutation) | Found in 40% of GH-secreting tumors; leads to constitutive cAMP activation. |
| MEN 1 | MEN1 gene (Menin) | Pituitary adenoma + Parathyroid hyperplasia + Pancreatic neuroendocrine tumors. |
| Carney Complex | PRKAR1A mutation | Pituitary excess + Myxomas + Spotty skin pigmentation. |
| McCune-Albright | Mosaic GNAS mutation | Polyostotic fibrous dysplasia + Café-au-lait spots + Precocious puberty. |
| FIPA | AIP gene mutation | Familial Isolated Pituitary Adenomas; often presents as large tumors in young patients. [6] |
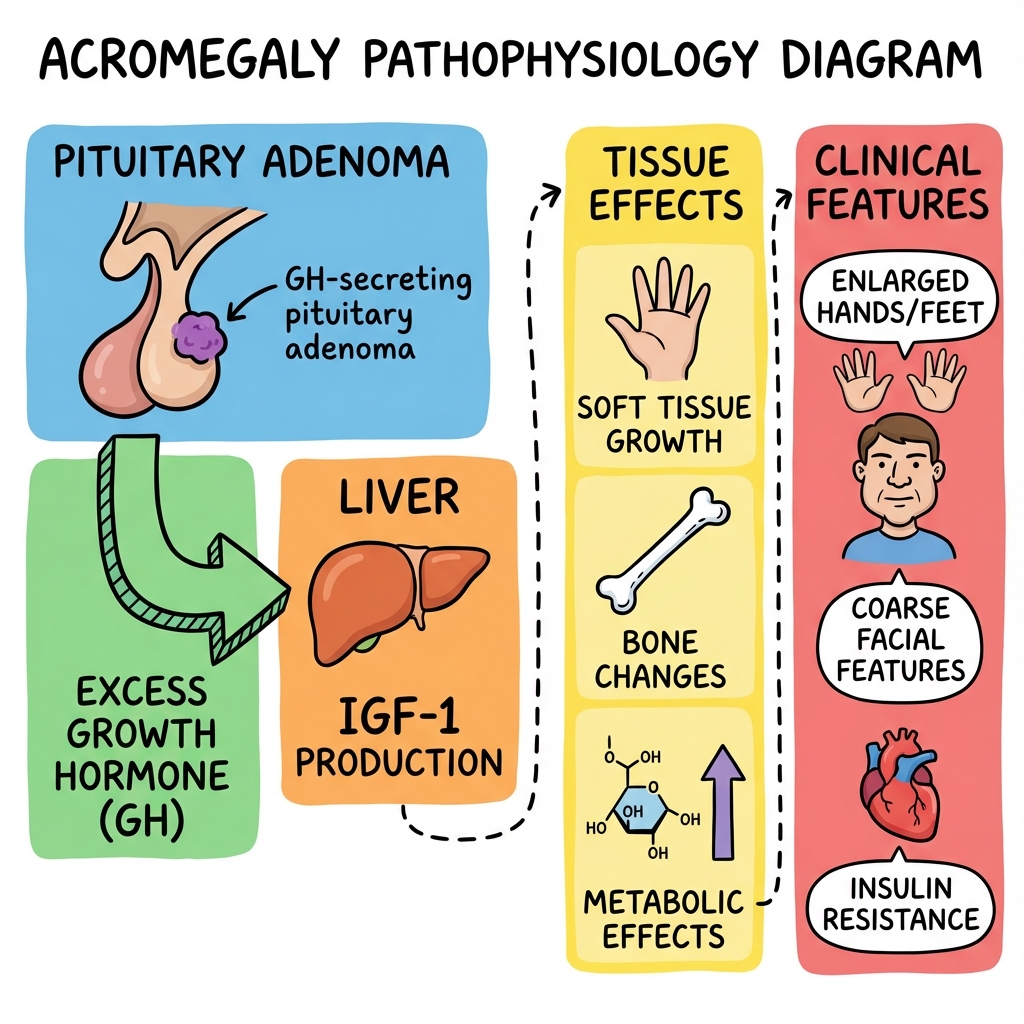
3. Pathophysiology: The GH-IGF1 Axis
1. The Source: Somatotroph Adenoma
The primary pathology is typically a monoclonal expansion of somatotroph cells in the anterior pituitary. These cells lose their normal inhibitory response to Somatostatin and become hyper-responsive to GHRH.
2. The Hormone: Growth Hormone (GH)
The tumor secretes GH in an autonomous, non-pulsatile fashion. GH exerts its effects by:
- Direct Effects: Anti-insulin actions (increased gluconeogenesis and lipolysis), leading to insulin resistance and impaired glucose tolerance.
- Indirect Effects (The Major Pathway): Stimulates the liver to synthesize and secrete IGF-1.
3. The Effector: IGF-1
IGF-1 (formerly Somatomedin C) is the primary mediator of growth. It binds to IGF-1 receptors (structurally similar to insulin receptors) and promotes:
- Chondrogenesis: Growth of articular cartilage (leading to arthropathy).
- Soft Tissue Hypertrophy: Hyperplasia of skin, tongue, heart, and visceral organs.
- Periosteal Bone Growth: Widening of bones (brow, jaw, hands). [7]
4. Feedback Failure
In healthy physiology, high IGF-1 and GH provide negative feedback to the hypothalamus (increasing somatostatin) and pituitary. In acromegaly, the adenoma is resistant to this feedback, maintaining high levels despite systemic satiety.
4. Clinical Presentation
Craniofacial Changes
- Frontal Bossing: Prominence of the supraorbital ridges.
- Prognathism: Overgrowth of the mandible leading to an underbite.
- Diastema: Widening of the spaces between the teeth.
- Macroglossia: Enlarged tongue causing speech changes and OSA.
Acral and Soft Tissue
- "Spade-like" Hands: Broad, thickened fingers with a "doughy" texture.
- Heel Pad Thickening: Measured on lateral X-ray (> 22-25mm is suggestive).
- Hyperhidrosis: Oily, sweaty skin with a characteristic odor.
Systemic Complications
- Joints: Degenerative arthropathy (large joints and spine).
- Neurological: Carpal Tunnel Syndrome (median nerve compression by soft tissue).
- Metabolic: Impaired glucose tolerance or overt Diabetes Mellitus (in 25-50%).
- Visual: Bitemporal hemianopia if a macroadenoma compresses the optic chiasm. [8]
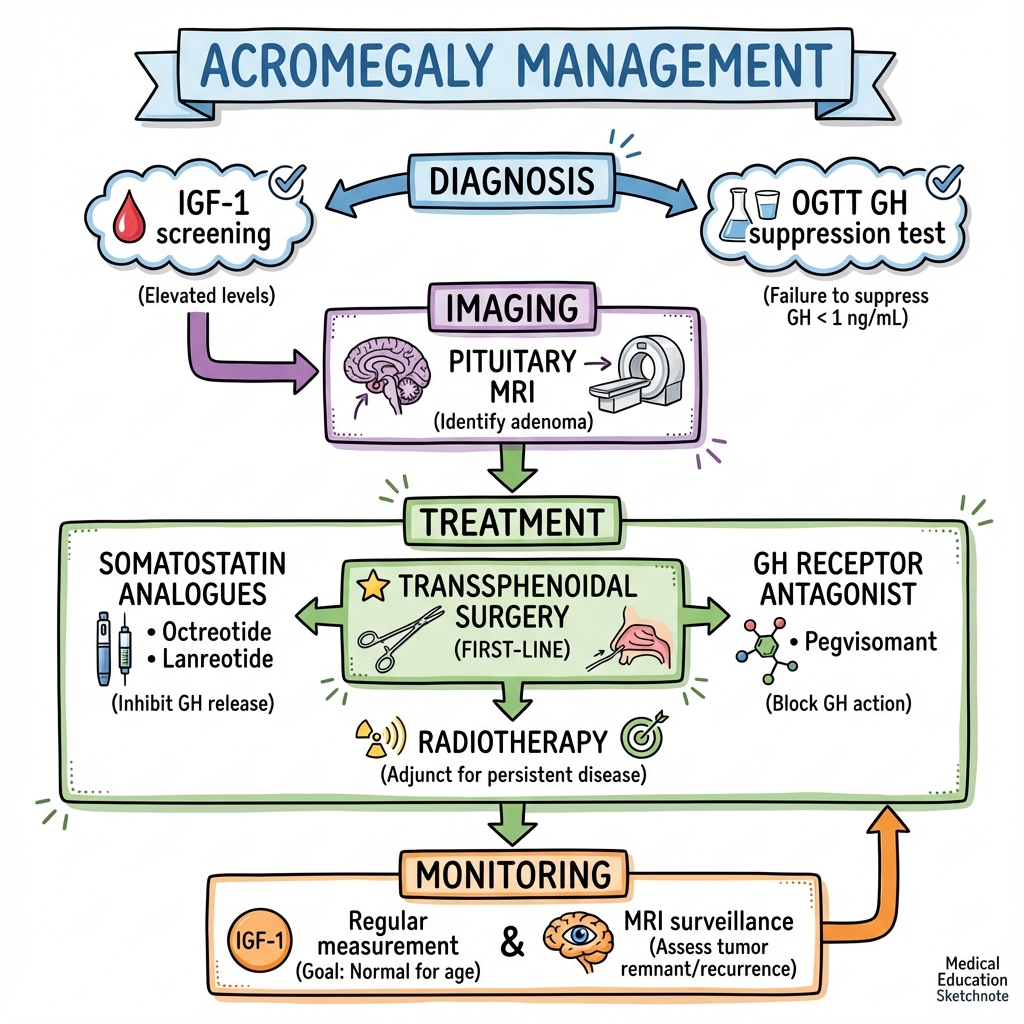
5. Investigations
1. Screening: Serum IGF-1
- Rationale: GH is secreted in pulses and has a short half-life (20 mins). IGF-1 is stable throughout the day.
- Interpretation: A normal age- and sex-matched IGF-1 level essentially rules out acromegaly.
2. Confirmation: Oral Glucose Tolerance Test (OGTT)
- Protocol: 75g oral glucose load. GH measured at 0, 30, 60, 90, and 120 minutes.
- Positive Result: Failure to suppress GH to less than 0.4 µg/L (using modern ultrasensitive assays) or less than 1.0 µg/L (older assays).
- Paradoxical Rise: In some patients, GH may actually rise in response to glucose. [9]
3. Localization: MRI Pituitary
- Goal: Identify the adenoma (usually a macroadenoma > 10mm at diagnosis) and assess invasion of the cavernous sinus or compression of the optic chiasm.
4. Comorbidity Screening (The "Mandatory 4")
- Colonoscopy: High risk of colorectal cancer.
- Echocardiography: Assess for LVH and cardiomyopathy.
- Sleep Study: High prevalence of obstructive sleep apnea (OSA).
- Visual Fields: Formal Goldmann or Humphrey perimetry if chiasmal compression is suspected.
6. Management: The Multimodal Strategy
Management Algorithm (ASCII)
[CLINICAL SUSPICION]
|
+--------v--------+
| MEASURE IGF-1 |
+--------+--------+
|
+-----------v-----------+
| IGF-1 ELEVATED? |
+-----------+-----------+
YES | NO
+-------------v--+ +----v-------+
| CONFIRM: OGTT | | EXCLUDE |
+-------+--------+ +------------+
|
+-------v--------+
| MRI PITUITARY |
+-------+--------+
|
+-------v-----------------------+
| 1st LINE: SURGERY |
| (Trans-sphenoidal Resection) |
+-------+-----------+-----------+
| |
+-------v---+ +---v-----------+
| CURE? | | RESIDUAL |
| (IGF-1 nl)| | DISEASE |
+-----------+ +-------+-------+
|
+-------v-----------+
| 2nd LINE: MEDICAL|
| - Somatostatin An.|
| - Pegvisomant |
| - Cabergoline |
+-------+-----------+
| (If failure)
+-------v-----------+
| 3rd LINE: |
| RADIOTHERAPY |
+-------------------+
1. Surgical Management
- Procedure: Endoscopic Trans-sphenoidal Surgery.
- Outcome: The primary treatment for almost all patients. Cure rates are 80-90% for microadenomas but drop to less than 50% for large, invasive macroadenomas. [10]
2. Medical Therapy
Used when surgery fails to achieve biochemical cure or as primary therapy if surgery is contraindicated.
- Somatostatin Receptor Ligands (SRLs): (e.g., Octreotide, Lanreotide). First-line medical therapy. Inhibit GH secretion and can cause tumor shrinkage in ~50%.
- GH Receptor Antagonist: (Pegvisomant). Blocks GH action in the liver. Most effective drug for normalizing IGF-1 (> 90% success) but does not shrink the tumor.
- Dopamine Agonists: (Cabergoline). Used for mild disease or if the tumor co-secretes prolactin. [11]
3. Radiotherapy
Reserved for resistant cases. Takes years to reach maximal effect. High risk of long-term hypopituitarism (50% at 10 years).
7. Complications
- Cardiovascular: Hypertension, Left Ventricular Hypertrophy (LVH), and Heart Failure.
- Respiratory: Severe OSA and upper airway obstruction.
- Endocrine: Pituitary insufficiency (Panhypopituitarism) following surgery or radiation.
- Malignancy: Increased risk of colon, thyroid, and breast cancer.
- Skeletal: Severe, irreversible osteoarthritis and vertebral fractures. [12]
8. Evidence & Landmark Trials
- Katznelson et al. (Endocrine Society Guidelines, 2014): Established the current diagnostic thresholds (GH less than 0.4 µg/L) and management hierarchy. [PMID: 25356808]
- PRIMARYS Study (2014): Demonstrated that Lanreotide Autogel can achieve significant tumor shrinkage as a primary therapy in treatment-naive patients. [13]
- The ACROSTUDY: A large global safety registry for Pegvisomant, confirming its high efficacy in normalizing IGF-1 in real-world clinical practice.
9. Single Best Answer (SBA) Questions
Question 1
A 45-year-old male presents with coarse facial features and increasing shoe size. What is the most appropriate initial screening test for the suspected diagnosis?
- A) Random Growth Hormone (GH)
- B) Insulin-like Growth Factor 1 (IGF-1)
- C) Oral Glucose Tolerance Test (OGTT)
- D) MRI of the Pituitary
- E) 24-hour Urinary Cortisol
- Answer: B. IGF-1 is the most reliable screening test due to its stability. GH is pulsatile and unreliable as a single measure.
Question 2
During an OGTT for suspected acromegaly, which GH level at 120 minutes is diagnostic of the condition using a modern ultrasensitive assay?
- A) less than 0.4 µg/L
- B) less than 1.0 µg/L
- C) > 0.4 µg/L
- D) > 5.0 µg/L
- E) Suppression to 50% of baseline
- Answer: C. Failure to suppress GH to less than 0.4 µg/L confirms acromegaly.
Question 3
Which of the following is the most common cause of death in patients with long-standing acromegaly?
- A) Colorectal Cancer
- B) Pituitary Apoplexy
- C) Cardiomyopathy
- D) Status Epilepticus
- E) Renal Failure
- Answer: C. Cardiovascular disease (cardiomyopathy and heart failure) is the leading cause of mortality.
Question 4
A patient with acromegaly is started on Pegvisomant. What is the mechanism of action of this medication?
- A) Somatostatin receptor agonist
- B) Dopamine receptor agonist
- C) GH receptor antagonist
- D) GHRH receptor antagonist
- E) Pituitary enzyme inhibitor
- Answer: C. Pegvisomant blocks the GH receptor in the liver, preventing IGF-1 production.
Question 5
Which screening procedure is mandatory for all patients at the time of acromegaly diagnosis?
- A) Annual MRI Head
- B) DEXA Scan
- C) Colonoscopy
- D) Carotid Doppler
- E) Gastroscopy
- Answer: C. Due to the significantly increased risk of colorectal polyps and cancer.
Question 6
An acromegaly patient presents with sudden severe headache, vomiting, and bitemporal hemianopia. What is the most likely diagnosis?
- A) Migraine flare
- B) Pituitary Apoplexy
- C) Ischaemic Stroke
- D) Subarachnoid Haemorrhage
- E) Cavernous Sinus Thrombosis
- Answer: B. Sudden expansion/hemorrhage of a pituitary tumor is a medical emergency.
Question 7
Why is the heel pad thickness measured in acromegaly?
- A) To assess for peripheral neuropathy
- B) To quantify soft tissue overgrowth on X-ray
- C) To look for plantar fasciitis
- D) To screen for acromegalic gait
- E) To assess for osteoporosis
- Answer: B. Heel pad thickening (> 22-25mm) is a classic radiological marker of soft tissue hypertrophy.
Question 8
Which genetic syndrome is characterized by acromegaly, parathyroid hyperplasia, and pancreatic tumors?
- A) MEN 2A
- B) MEN 1
- C) McCune-Albright Syndrome
- D) Carney Complex
- E) von Hippel-Lindau
- Answer: B. This is the classic "3 Ps" triad of MEN 1.
Question 9
What is the primary first-line treatment for a patient with a GH-secreting macroadenoma?
- A) Long-acting Octreotide
- B) Stereotactic Radiosurgery
- C) Trans-sphenoidal Resection
- D) Life-long Pegvisomant
- E) Watchful waiting
- Answer: C. Surgery is first-line for nearly all patients.
Question 10
In normal physiology, which hormone provides the primary inhibitory stimulus for GH release?
- A) GHRH
- B) Dopamine
- C) Somatostatin
- D) Prolactin
- E) Ghrelin
- Answer: C. Somatostatin (GHIH) is the "off switch" for GH.
12. Pathological Hypertrophy: The "Giga" Organ Effect
Acromegaly isn't just about bones; it's about the viscera.
A. Visceromegaly
- Hepatomegaly & Splenomegaly: Overgrowth of the liver and spleen is common but often asymptomatic.
- Thyromegaly: Up to 50% of patients develop a multinodular goiter.
- Cardiomegaly: The most dangerous form. Excess GH leads to concentric left ventricular hypertrophy, eventually progressing to high-output heart failure.
B. The Oncology Risk
- Colonic Polyps: Patients have a significantly higher rate of premalignant polyps. Mandatory screening colonoscopy is required at diagnosis and every 3–5 years.
13. Biochemical Paradox: The Oral Glucose Suppression Test
Why do we use sugar to test for a growth problem?
A. Physiologic Negative Feedback
- In a healthy person, a high blood sugar level (75g oral glucose load) triggers a release of somatostatin, which tells the pituitary to stop producing GH. GH levels should drop to less than 0.4 µg/L (or less than 1 µg/L depending on the assay).
- The Acromegalic Failure: In patients with a GH-secreting tumor, the cells are "autonomous" and ignore the sugar signal. GH levels remain elevated (> 1 µg/L), confirming the diagnosis.
B. The IGF-1 "Buffer"
- GH is released in pulses. IGF-1 is stable throughout the day. Therefore, a normal IGF-1 (age and sex adjusted) effectively rules out acromegaly, whereas a normal random GH means very little.
14. Surgical Nuances: Transsphenoidal Endoscopy (TSS)
The "Standard of Care" for nearly all GH-secreting tumors.
A. The Endoscopic Route
- Technique: Using a HD endoscope through the nostrils to reach the pituitary gland at the base of the skull.
- The "Pseudocapsule": Skilled neurosurgeons look for the "pseudocapsule"—a thin layer of compressed normal pituitary tissue—which acts as a roadmap to completely excise the tumor while preserving normal hormonal function.
B. High-Risk Anatomy
- The Carotid Arteries: The pituitary sits between the two internal carotid arteries. Injury to these during surgery is the most feared "catastrophic" complication.
15. Medical Mastery: Somatostatin Analogs vs. Pegvisomant
When surgery fails to achieve a cure (about 40% of macroadenomas).
A. Somatostatin Analogs (Octreotide/Lanreotide)
- Target: They act directly on the tumor receptors (SSTR2 and SSTR5) to inhibit GH release.
- Side Effect: "Gallstones" (biliary sludge) because they stop the gallbladder from contracting properly.
B. Pegvisomant (The Receptor Blockade)
- Mechanism: It doesn't touch the tumor. Instead, it blocks the GH receptor in the liver, preventing the production of IGF-1.
- Benefit: This is the most effective drug for lowering IGF-1 levels.
- Risk: Because it doesn't shrink the tumor, the pituitary adenoma can potentially grow while the patient "looks" biochemically cured.
16. Patient Explanation
"Acromegaly is a condition where your body produces too much growth hormone. This is usually caused by a small, non-cancerous lump on the pituitary gland, which is the 'control center' for your hormones. Because growth hormone makes tissues grow, it causes your hands, feet, and face to slowly change shape over many years. It also puts a lot of strain on your heart and can cause diabetes. The main treatment is a specialized surgery through the nose to remove the lump. If surgery doesn't completely fix the hormone levels, we have very effective injections and medications to keep the condition under control."
17. Examination Focus: Viva & OSCE Points
The "Endocrine" Viva
- The "Spade-Like" Hand: Describe the widening of the digits and thickening of the skin.
- Carpal Tunnel Syndrome: Explain how soft tissue overgrowth compresses the median nerve.
- The "Acre" triad: (Acromegaly, Carpal Tunnel, Rugose features, Enlarged organs).
18. References
- Melmed S. Acromegaly. N Engl J Med. 2006;355(24):2558-2573. [PMID: 17167139]
- Colao A, et al. Acromegaly. Nat Rev Dis Primers. 2019;5(1):20. [PMID: 30899019]
- Katznelson L, et al. Acromegaly: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2014;99(11):3933-3951. [PMID: 25356808]
- Jane JA, et al. Surgical management of acromegaly. Neurosurg Clin N Am. 2003.
- Giustina A, et al. A consensus on criteria for cure of acromegaly. J Clin Endocrinol Metab. 2010;95(7):3141-3148.
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Related Topics
Adjacent pages worth reading next.
- Pituitary Apoplexy
- Diabetes Mellitus Type 2
- Sleep Apnea