Acute Coronary Syndrome
Acute Coronary Syndrome (ACS) is a life-threatening spectrum of myocardial ischaemia resulting from the acute disruption... MRCP exam preparation.
What matters first
Acute Coronary Syndrome (ACS) is a life-threatening spectrum of myocardial ischaemia resulting from the acute disruption... MRCP exam preparation.
Cardiogenic shock (SBP less than 90 mmHg, cold extremities)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Cardiogenic shock (SBP less than 90 mmHg, cold extremities)
- Acute mitral regurgitation (pansystolic murmur)
- Ventricular septal rupture (LSB harsh murmur)
- Refractory VT/VF (Electrical storm)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Aortic Dissection
- Pulmonary Embolism
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acute Coronary Syndrome (Adult)
1. Overview
Acute Coronary Syndrome (ACS) is a life-threatening spectrum of myocardial ischaemia resulting from the acute disruption of an atherosclerotic plaque and subsequent coronary thrombosis. It is classified by the 12-lead ECG into ST-Elevation Myocardial Infarction (STEMI) and Non-ST-Elevation Acute Coronary Syndrome (NSTE-ACS), the latter encompassing NSTEMI and Unstable Angina. [1]
The clinical significance of ACS is profound: it remains the leading cause of sudden cardiac death and heart failure worldwide. The "Universal Definition of Myocardial Infarction" (4th Edition) mandates evidence of myocardial necrosis (troponin rise/fall) in a clinical setting consistent with ischaemia. [2]
Management has evolved from simple observation to a high-speed "Reperfusion Era." The 2023-2024 ESC and AHA guidelines emphasise the Radial First approach, High-Sensitivity Troponin rule-out protocols, and personalised DAPT de-escalation strategies. Every minute of delay in STEMI reperfusion is associated with a 7-10% increase in 1-year mortality, cementing the mantra: "Time is Muscle." [3]
2. Epidemiology
The "Atherosclerotic Burden"
- Incidence: Approximately 3 million people per year present with ACS globally. In the UK, a "Heart Attack" occurs every 5 minutes.
- The Transition: STEMI incidence is declining in high-income countries due to aggressive statin and smoking cessation efforts, but NSTEMI is rising, partly due to the improved sensitivity of troponin assays. [4]
High-Risk Cohorts
- Diabetes: Increases ACS risk 3-fold. Diabetics often have "Multi-vessel disease" and a higher risk of "Silent" infarctions.
- South Asians: Present 5-10 years earlier than Caucasians with more diffuse atherosclerosis.
- Women: Often experience diagnostic delays due to atypical symptoms (fatigue, back pain), leading to higher mortality rates post-infarct compared to men. [5]
3. Aetiology & Pathophysiology
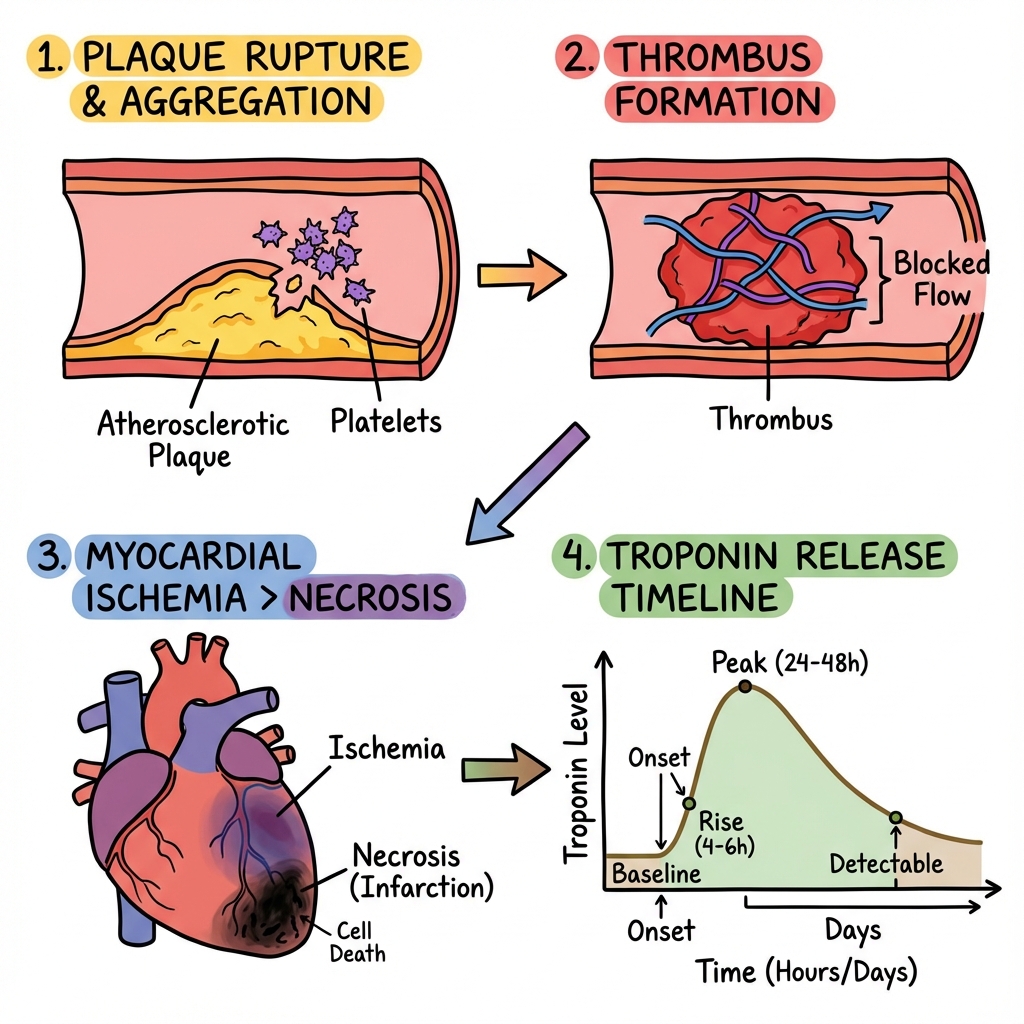
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Plaque Rupture/Erosion: The "vulnerable plaque" (thin fibrous cap, lipid-rich core) ruptures, typically at the "shoulder" region where matrix metalloproteinases (MMPs) have degraded collagen.
- Platelet Phase: Subendothelial collagen and Von Willebrand Factor (vWF) are exposed. Platelets adhere via GpIb receptors and activate, releasing ADP and Thromboxane A2.
- Coagulation Phase: Tissue factor from the plaque core activates the extrinsic pathway. Thrombin (IIa) is generated, converting fibrinogen to Fibrin, which weaves the platelets into a "Red Thrombus" (STEMI) or "White Thrombus" (NSTE-ACS).
- The Ischaemic Wavefront: Within 20 minutes of total occlusion, necrosis begins in the subendocardium (highest wall tension) and spreads like a wavefront toward the epicardium.
- Metabolic Collapse: ATP levels drop within seconds. The Na+/K+ ATPase pump fails, leading to intracellular Na+ accumulation, cellular swelling, and lethal Calcium (Ca2+) overload.
- Reperfusion Injury (The Paradox): When flow is restored, a burst of Reactive Oxygen Species (ROS) occurs. This triggers the opening of the mPTP (Mitochondrial Permeability Transition Pore), causing further mitochondrial swelling and apoptosis.
- Ventricular Remodelling: Macrophages clear necrotic tissue (Day 3-7; period of highest rupture risk). Fibroblasts eventually deposit Type I collagen, forming a non-contractile scar by 6 weeks. [6, 7]
4. Clinical Presentation
Typical Symptoms
- Crushing Retrosternal Pain: Typically lasting > 20 minutes; not relieved by rest or GTN.
- Radiation: To left arm, neck, or jaw.
- Autonomic Surge: Profuse diaphoresis (highly specific), nausea, and vomiting.
STEMI Equivalents (Must Recognise)
- De Winter T-waves: Upsloping ST depression + tall symmetric T-waves (Proximal LAD occlusion).
- Wellens' Syndrome: Deeply inverted or biphasic T-waves in V2-V3 (Impending LAD occlusion).
- Posterior MI: ST depression in V1-V3; requires V7-V9 leads showing ST elevation. [8]
5. Investigations
The 10-Minute Mandate
A 12-lead ECG must be performed and interpreted within 10 minutes of first medical contact.
- STEMI: ≥1mm ST elevation in 2 contiguous leads (or ≥2mm in V2-V3).
- New LBBB: Should be managed as STEMI if clinical suspicion is high.
High-Sensitivity Troponin (hs-cTn)
- The 0/1-hour algorithm (ESC 2023) is the standard for NSTE-ACS.
- Rule-Out: Very low baseline or no rise at 1 hour (NPV > 99%).
- Rule-In: High baseline or a significant "Delta" (change) at 1 hour. [9]
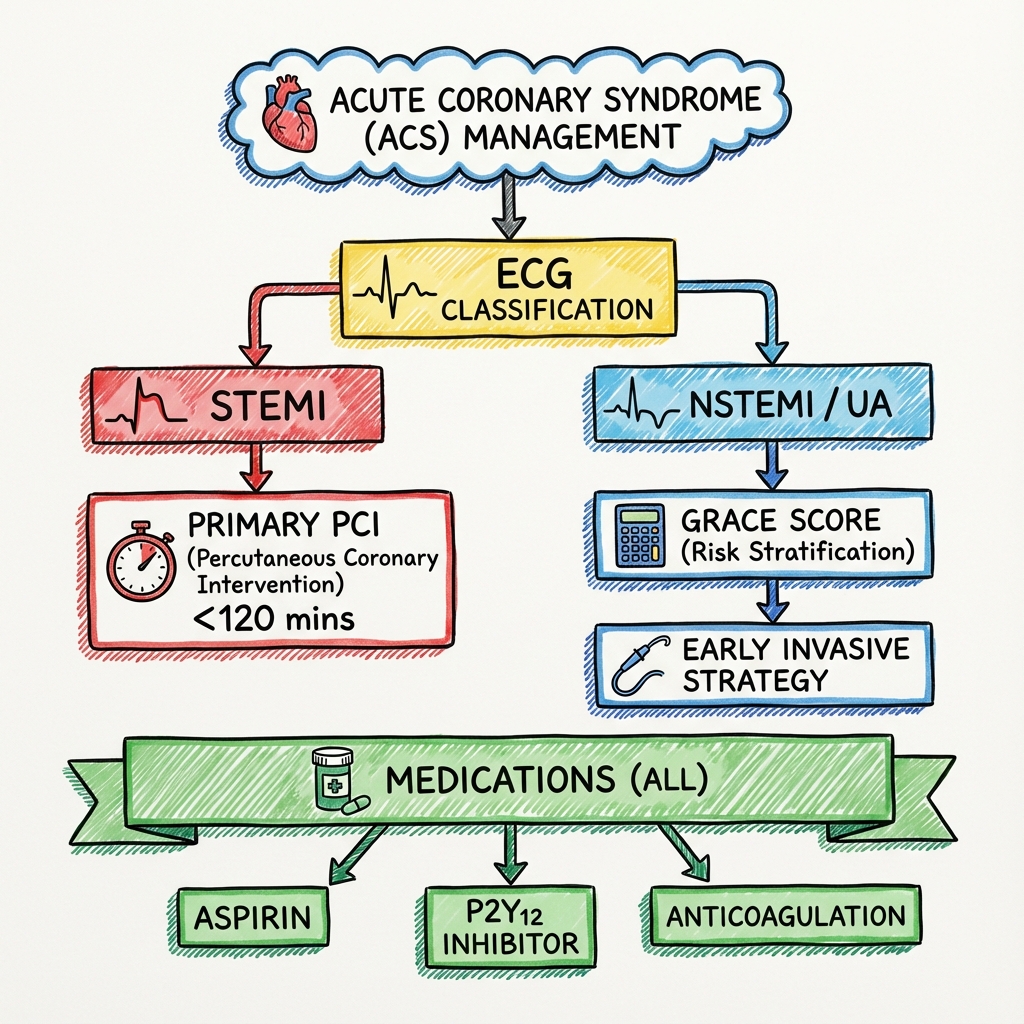
6. Management: The Reperfusion Protocol
1. STEMI (The Red Alert)
- Primary PCI: The gold standard. Goal: Wire across lesion less than 120 mins from diagnosis.
- Fibrinolysis (Tenecteplase): Only if PCI > 120 mins away. Requires subsequent "Rescue PCI" if no reperfusion.
- Antithrombotic: Aspirin 300mg + Prasugrel 60mg (if no Hx of stroke) + UFH bolus.
2. NSTE-ACS (Risk Stratification)
- Very High Risk (Shock, Arrhythmia, Dynamic ECG): Immediate Angio (less than 2 hrs).
- High Risk (GRACE Score > 140, Trop rise): Early Angio (less than 24 hrs).
- Low Risk: Selective invasive strategy.
3. Secondary Prevention ("The Big 5")
- Aspirin: 75mg OD lifelong.
- P2Y12 Inhibitor: Ticagrelor/Prasugrel for 12 months (DAPT).
- Statin: High-intensity (Atorvastatin 80mg) - aim for LDL less than 1.4 mmol/L.
- ACEi: Titrate to max dose (prevents remodelling).
- Beta-blocker: Bisoprolol/Carvedilol (reduces SCD). [10]
7. Evidence: Landmark Trials
| Trial | Population | Result | Impact |
|---|---|---|---|
| PLATO | ACS | Ticagrelor > Clopidogrel | Ticagrelor became first-line P2Y12. |
| ISAR-REACT 5 | ACS + PCI | Prasugrel > Ticagrelor | Prasugrel preferred if PCI planned. |
| COMPLETE | STEMI + MVD | Complete > Culprit only | Mandated revasc of non-culprit lesions. |
| TWILIGHT | High-Risk PCI | Ticagrelor Mono > DAPT | Supported stopping Aspirin after 3 months. |
| OASIS-5 | NSTEMI | Fondaparinux > Enoxaparin | Established Fonda as safest in NSTEMI. |
8. Complications: The "Timing" Framework
- 0-24 Hours: Ventricular Fibrillation (SCD), Cardiogenic Shock, Acute Heart Failure.
- Day 2-7 (The Rupture Window):
- Papillary Muscle Rupture: Acute severe MR (pansystolic murmur at apex).
- VSD: Left-to-right shunt (harsh murmur at LSB).
- Free Wall Rupture: Cardiac tamponade/PEA.
- Weeks-Months: Ventricular Aneurysm, Dressler's Syndrome (Autoimmune pericarditis). [11]
9. Single Best Answer (SBA) Questions
Question 1
A 62-year-old male with an inferior STEMI develops sudden shortness of breath on Day 3. Examination reveals a new 4/6 pansystolic murmur at the apex. BP is 95/60. What is the most likely diagnosis?
- A) Ventricular Septal Defect
- B) Dressler's Syndrome
- C) Papillary Muscle Rupture
- D) Acute Pulmonary Embolism
- E) Stent Thrombosis
- Answer: C. Papillary muscle rupture (causing acute MR) is a classic complication occurring 2-7 days post-infarct, particularly in inferior MIs (RCA supplies the posteromedial muscle).
Question 2
According to the 2023 ESC guidelines, which P2Y12 inhibitor is generally preferred for patients with ACS who are proceeding to PCI?
- A) Clopidogrel
- B) Ticagrelor
- C) Prasugrel
- D) Cangrelor
- E) Aspirin
- Answer: C. Prasugrel showed superiority over Ticagrelor in the ISAR-REACT 5 trial and is preferred if the coronary anatomy is known or PCI is imminent.
10. Viva Scenario: The "Normal" Angio (MINOCA)
Examiner: "You have a 45-year-old female with crushing chest pain, ST depression in V4-V6, and a troponin of 5,000. Her angiogram shows completely normal coronary arteries. What is the diagnosis and your next step?"
Candidate:
- Diagnosis: This is MINOCA (Myocardial Infarction with Non-Obstructive Coronary Arteries).
- Differential: Coronary vasospasm, plaque erosion (undetected by angio), microvascular dysfunction, or myocarditis.
- Investigation: I would perform a Cardiac MRI (CMR).
- Rationale: CMR is the gold standard to distinguish between true MI (subendocardial enhancement) and mimics like Myocarditis (subepicardial enhancement) or Takotsubo (apical ballooning).
11. Patient Explanation
"A heart attack happens when a blood vessel in your heart gets suddenly blocked by a clot, like a blocked pipe. This starves your heart muscle of the oxygen it needs to live. We've used a 'stent'—a tiny mesh tube—to prop that pipe open and restore the flow. To keep that stent from clotting again, you must take your 'blood thinners' strictly. Your heart is now healing, and our goal is to prevent another event by keeping your cholesterol and blood pressure very low."
12. References
- Byrne RA, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023. [PMID: 37622654]
- Thygesen K, et al. Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol. 2018. [PMID: 30154042]
- Schüpke S, et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes (ISAR-REACT 5). N Engl J Med. 2019. [PMID: 31475799]
- Mehta SR, et al. Complete Revascularization with Multivessel PCI for Myocardial Infarction (COMPLETE). N Engl J Med. 2019. [PMID: 31475795]
- Valgimigli M, et al. Radial versus femoral access in patients with acute coronary syndromes (MATRIX). Lancet. 2015. [PMID: 25824555]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for acute coronary syndrome?
Seek immediate emergency care if you experience any of the following warning signs: Cardiogenic shock (SBP less than 90 mmHg, cold extremities), Acute mitral regurgitation (pansystolic murmur), Ventricular septal rupture (LSB harsh murmur), Refractory VT/VF (Electrical storm), Flash pulmonary oedema (Killip III/IV).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Consequences
Complications and downstream problems to keep in mind.
- Dressler's Syndrome
- Ventricular Aneurysm