Addison's Disease (Primary Adrenal Insufficiency)
Addison's disease is primary adrenal insufficiency (PAI) caused by destruction or dysfunction of the adrenal cortex, res... MRCP exam preparation.
What matters first
Addison's disease is primary adrenal insufficiency (PAI) caused by destruction or dysfunction of the adrenal cortex, res... MRCP exam preparation.
Adrenal crisis (hypotension, collapse, confusion)
9 Jan 2025
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Adrenal crisis (hypotension, collapse, confusion)
- Severe hyperkalaemia (less than 6.5 mmol/L)
- Hypoglycaemia (less than 3.0 mmol/L)
- Unexplained shock refractory to fluids
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Secondary Adrenal Insufficiency
- Chronic Fatigue Syndrome
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Addison's Disease (Primary Adrenal Insufficiency)
1. Clinical Overview
Summary
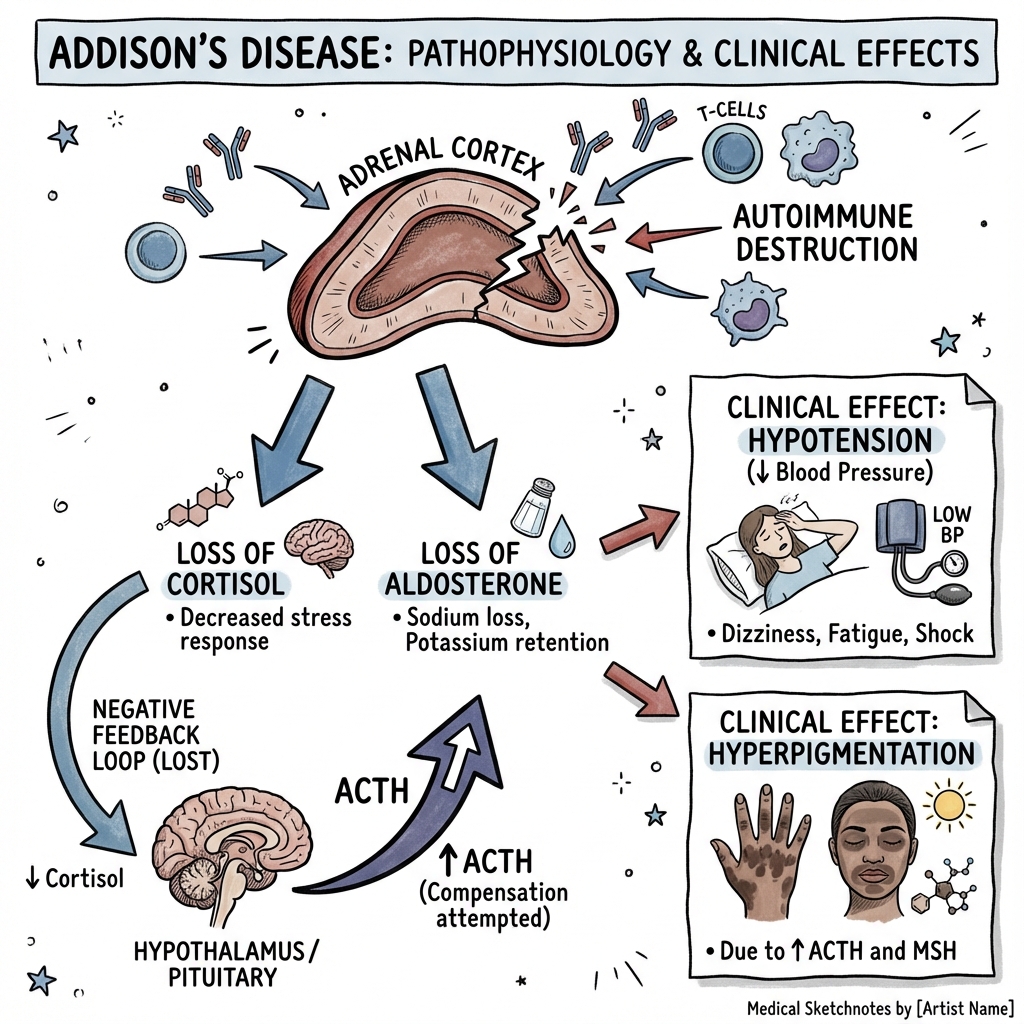
Addison's disease is primary adrenal insufficiency (PAI) caused by destruction or dysfunction of the adrenal cortex, resulting in deficiency of glucocorticoids (cortisol), mineralocorticoids (aldosterone), and adrenal androgens (DHEA/DHEAS). The condition was first described by Thomas Addison in 1855 in his seminal publication on the constitutional effects of disease of the suprarenal capsules. [1]
In developed countries, autoimmune adrenalitis accounts for approximately 80-90% of cases, while tuberculosis remains the leading cause in regions with high TB prevalence. [2,3] The hallmark biochemical abnormality is elevated adrenocorticotropic hormone (ACTH) due to loss of negative feedback, which drives the characteristic hyperpigmentation through melanocyte-stimulating hormone (MSH) co-secretion from the proopiomelanocortin (POMC) precursor.
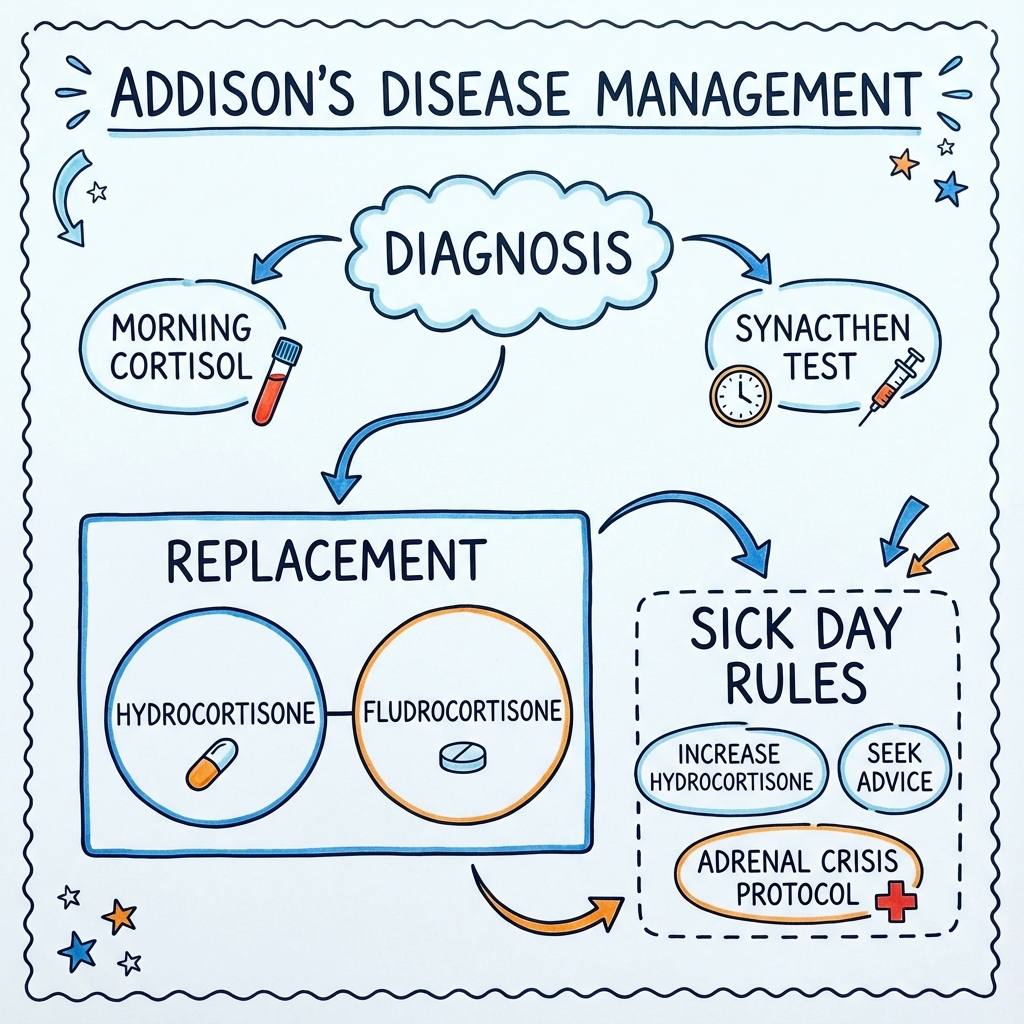
Diagnosis is confirmed by the short Synacthen test (SST), demonstrating failure of cortisol to rise following synthetic ACTH stimulation. Lifelong physiological replacement with hydrocortisone and fludrocortisone is essential, along with comprehensive patient education on "sick-day rules" to prevent the potentially fatal complication of adrenal crisis. [4]
Key Facts
| Parameter | Value | Notes |
|---|---|---|
| Definition | Primary adrenal insufficiency | Destruction/dysfunction of adrenal cortex |
| Prevalence | 93-144 per million | Varies by population [5] |
| Annual Incidence | 4-6 per million | Increasing with improved detection [5] |
| Main Cause (Developed) | Autoimmune adrenalitis | 80-90% of cases [2] |
| Main Cause (Developing) | Tuberculosis | Still predominant in endemic regions |
| Key Autoantibody | 21-hydroxylase (CYP21A2) | Present in ~90% of autoimmune cases [6] |
| Diagnostic Test | Short Synacthen test | Gold standard [4] |
| Treatment Backbone | Hydrocortisone + Fludrocortisone | Lifelong replacement |
| Crisis Mortality | 0.5% per year | Reduced with education [7] |
Clinical Pearls
"Addisonian Pigmentation": Hyperpigmentation in sun-exposed areas, palmar creases, buccal mucosa, and recent scars is pathognomonic. It results from elevated ACTH and α-MSH (both cleaved from POMC). This finding distinguishes primary from secondary adrenal insufficiency, where ACTH is low and pigmentation is absent. [8]
"The Salt Craving Clue": Up to 64% of patients report intense salt craving due to aldosterone deficiency and renal sodium wasting. This symptom is frequently overlooked but highly suggestive when present with fatigue and weight loss. [9]
"Sick Day Rules Save Lives": The majority of adrenal crises occur due to inadequate glucocorticoid dosing during intercurrent illness. Patients MUST be educated to double or triple hydrocortisone during febrile illness, and to use parenteral hydrocortisone if vomiting. [7]
"The 3 Ps of Adrenal Crisis": Profound weakness, Postural hypotension, and Pigmentation — think primary adrenal insufficiency.
Why This Matters Clinically
Addison's disease exemplifies a condition that is easily missed due to non-specific early symptoms (fatigue, weight loss, nausea) but is fatal if untreated during crisis. The annual rate of adrenal crisis is approximately 6-8 per 100 patient-years, with mortality of 0.5% per crisis episode. [7] Early recognition, appropriate diagnostic testing, lifelong hormone replacement, and comprehensive patient education are the pillars of excellent care.
2. Epidemiology
Incidence & Prevalence
Contemporary epidemiological studies demonstrate increasing recognition of primary adrenal insufficiency:
| Parameter | Value | Source |
|---|---|---|
| Prevalence (Europe) | 93-144 per million | Erichsen et al. (Norway) [5] |
| Prevalence (UK) | ~140 per million | Estimated from registry data |
| Annual Incidence | 4.4-6.2 per million | Meta-analysis [5] |
| Trend | Increasing | Better detection, rising autoimmune disease |
| Female:Male Ratio | 2.6:1 (autoimmune) | Autoimmune predominance in females [10] |
The apparent increase in incidence likely reflects improved diagnostic awareness and increased prevalence of autoimmune diseases rather than a true increase in disease occurrence. [5]
Demographics
| Factor | Details | Clinical Relevance |
|---|---|---|
| Peak Age | 30-50 years | Working-age adults predominantly affected |
| Paediatric | May present at any age | Consider adrenoleukodystrophy in young males |
| Sex (Autoimmune) | Female predominance 2-3:1 | Consistent with autoimmune disease epidemiology |
| Sex (TB) | Male predominance | Reflects TB epidemiology |
| Ethnicity | All ethnicities | TB more common in endemic regions |
| Geography | TB predominant in developing countries | Autoimmune in developed nations |
Risk Factors
Autoimmune Adrenalitis (80-90% in Developed Countries)
Major Risk Factors:
- Pre-existing autoimmune disease (odds ratio 3-5×)
- First-degree relative with autoimmune endocrinopathy
- Female sex
- HLA associations: DRB104:04, DRB103:01, DQB1*03:02 [6]
Associated Autoimmune Conditions (Autoimmune Polyglandular Syndromes):
| Condition | Frequency in PAI | Notes |
|---|---|---|
| Autoimmune thyroid disease | 40-50% | Hashimoto's or Graves' |
| Type 1 diabetes mellitus | 10-20% | Screen with HbA1c/fasting glucose |
| Vitiligo | 10-20% | Visible marker of autoimmunity |
| Premature ovarian insufficiency | 10-20% | In females with PAI |
| Coeliac disease | 5-10% | Screen with TTG-IgA |
| Pernicious anaemia | 5-10% | B12 and IF antibodies |
| Alopecia areata | 5-10% | May be localised or totalis |
| Autoimmune hepatitis | less than 5% | Rare association |
Non-Autoimmune Causes (10-20%)
| Cause | Mechanism | Key Features |
|---|---|---|
| Tuberculosis | Caseating granulomatous destruction | Adrenal calcification on CT; bilateral enlargement early, atrophy late; remains most common cause globally [3] |
| Adrenal haemorrhage | Haemorrhagic infarction | Waterhouse-Friderichsen syndrome (meningococcal sepsis); anticoagulation; trauma; pregnancy |
| Metastatic cancer | Bilateral adrenal infiltration | Lung, breast, melanoma, renal, GI; requires > 90% destruction for clinical AI |
| Adrenoleukodystrophy (ALD) | X-linked peroxisomal disorder | Young males; very long chain fatty acids (VLCFA) elevated; neurological involvement [11] |
| Drugs | Enzyme inhibition/adrenal suppression | Ketoconazole, etomidate, mitotane, rifampicin (accelerates cortisol metabolism) |
| HIV/AIDS | CMV adrenalitis; MAC; Kaposi's | Opportunistic infections in advanced disease |
| Fungal infections | Histoplasmosis, blastomycosis | Endemic mycoses in immunocompromised |
| Congenital adrenal hyperplasia | 21-hydroxylase deficiency (most common) | Salt-wasting form; presents in neonates/infancy |
| Adrenal hypoplasia congenita | DAX1 mutation (X-linked) | Presents in infancy with salt wasting |
| Bilateral adrenalectomy | Surgical removal | Cushing's disease, bilateral phaeochromocytoma |
3. Pathophysiology
Adrenal Cortex Anatomy and Zones
The adrenal cortex comprises three distinct zones with specific steroidogenic functions:
| Zone | Location | Primary Hormone | Regulation | Deficiency Effects |
|---|---|---|---|---|
| Zona Glomerulosa | Outer | Aldosterone | RAAS (Angiotensin II, K⁺) | Hyponatraemia, hyperkalaemia, hypotension |
| Zona Fasciculata | Middle | Cortisol | ACTH (HPA axis) | Fatigue, hypoglycaemia, poor stress response |
| Zona Reticularis | Inner | DHEA/DHEAS | ACTH | Reduced libido, decreased axillary/pubic hair (females) |
Molecular Mechanism of Autoimmune Adrenalitis
Exam Detail: Step 1: Autoimmune Targeting
Autoimmune adrenalitis involves T-cell mediated destruction of the adrenal cortex. The primary autoantigen is 21-hydroxylase (CYP21A2), an enzyme essential for cortisol and aldosterone synthesis. Antibodies against 21-hydroxylase are detected in 86-90% of patients with autoimmune PAI and may predate clinical disease by years. [6]
Immunological Features:
- CD4+ and CD8+ T-lymphocyte infiltration of adrenal cortex
- Complement-fixing antibodies against adrenocortical cells
- HLA class II associations (particularly DRB1*04:04)
- Shared epitopes with other autoimmune conditions (APS-1, APS-2)
Step 2: Progressive Cortical Destruction
Clinical symptoms typically manifest when > 90% of adrenal cortex is destroyed. The zona glomerulosa (aldosterone) may be affected earlier or later than the zona fasciculata (cortisol), leading to variable presentations:
- Isolated glucocorticoid deficiency (early): Fatigue, weight loss, ACTH elevation
- Combined deficiency (later): Added hyponatraemia, hyperkalaemia, hypotension
Step 3: Loss of Negative Feedback
Low circulating cortisol removes negative feedback at:
- Hypothalamus (CRH secretion increases)
- Anterior pituitary (ACTH secretion increases)
ACTH is cleaved from proopiomelanocortin (POMC) along with:
- α-melanocyte-stimulating hormone (α-MSH)
- β-endorphin
Elevated α-MSH binds to melanocortin-1 receptors (MC1R) on melanocytes, stimulating eumelanin synthesis → hyperpigmentation.
Hormonal Deficiencies and Clinical Correlates
| Hormone | Normal Function | Deficiency Manifestations |
|---|---|---|
| Cortisol | Gluconeogenesis, stress response, immune modulation, appetite | Fatigue, anorexia, weight loss, hypoglycaemia, poor stress tolerance, myalgias, arthalgias |
| Aldosterone | Sodium retention, potassium excretion, volume homeostasis | Hyponatraemia, hyperkalaemia, salt craving, postural hypotension, volume depletion |
| DHEA/DHEAS | Precursor for sex steroids | Reduced libido (females), decreased axillary/pubic hair, reduced well-being (females) |
Primary vs Secondary vs Tertiary Adrenal Insufficiency
| Feature | Primary (Addison's) | Secondary | Tertiary |
|---|---|---|---|
| Site of Pathology | Adrenal cortex | Pituitary | Hypothalamus |
| ACTH Level | ↑↑ High | ↓ Low | ↓ Low |
| Cortisol | ↓ Low | ↓ Low | ↓ Low |
| Aldosterone | ↓ Low | Normal (RAAS intact) | Normal |
| Hyperpigmentation | Present | Absent | Absent |
| Hyperkalaemia | Present | Absent | Absent |
| Hyponatraemia | Present (severe) | May be present (dilutional) | May be present |
| Common Causes | Autoimmune, TB | Pituitary tumour/surgery, Sheehan's | Steroid withdrawal (most common overall) |
Pathophysiology of Adrenal Crisis
Adrenal crisis represents acute decompensation in a patient with limited adrenal reserve. It is most commonly precipitated by:
- Intercurrent illness (infection, gastroenteritis) — increased cortisol demand
- Non-compliance with replacement therapy
- Inadequate sick-day dosing
- Surgery/trauma without stress-dose steroids
- Vomiting (unable to absorb oral medication)
Physiological cascade:
- Inadequate cortisol → impaired vascular tone → hypotension
- Inadequate cortisol → reduced gluconeogenesis → hypoglycaemia
- Inadequate aldosterone → sodium wasting, potassium retention → hyponatraemia, hyperkalaemia
- Volume depletion → cardiovascular collapse
4. Clinical Presentation
Symptoms
Clinical presentation is typically insidious, developing over weeks to months. A high index of suspicion is required as symptoms are non-specific.
Chronic Symptoms (Frequency Based on Case Series)
| Symptom | Frequency | Mechanism |
|---|---|---|
| Fatigue, weakness | 100% | Cortisol deficiency |
| Weight loss | 90-100% | Anorexia, cortisol deficiency |
| Anorexia | 80-90% | Cortisol deficiency |
| Nausea, vomiting | 75-85% | Cortisol deficiency, electrolyte disturbance |
| Postural dizziness | 85-90% | Hypotension, volume depletion |
| Salt craving | 60-65% | Aldosterone deficiency, sodium loss [9] |
| Abdominal pain | 30-35% | Unclear; can mimic acute abdomen |
| Diarrhoea or constipation | 20-25% | GI dysmotility |
| Muscle/joint pain | 40-50% | Cortisol deficiency |
| Reduced libido | 30-40% (esp. females) | DHEA deficiency |
| Depression, irritability | 40-60% | Cortisol deficiency, chronic illness |
| Poor concentration | 40-50% | Cortisol deficiency |
| Amenorrhoea | Variable | Often secondary to weight loss/stress |
Acute Presentation (Adrenal Crisis)
| Feature | Frequency | Notes |
|---|---|---|
| Profound weakness/collapse | > 95% | Unable to stand |
| Hypotension/shock | > 90% | Often refractory to fluids |
| Confusion/altered consciousness | 50-70% | May range to coma |
| Severe abdominal pain | 30-50% | May mimic surgical abdomen |
| Fever | 60-70% | Infection often trigger; cortisol deficiency also causes fever |
| Nausea, vomiting | > 80% | Compounds problem (can't absorb oral meds) |
Clinical Pearl: Adrenal Crisis Mimics Acute Abdomen: Severe abdominal pain with vomiting and hypotension can lead to unnecessary laparotomy. Always consider adrenal crisis in unexplained shock, especially with hyperpigmentation, hyponatraemia, or hyperkalaemia.
Signs
General Inspection
- Unwell, fatigued appearance
- Weight loss (may be profound)
- Dehydrated
- Postural instability
Characteristic Signs
| Sign | Location | Prevalence | Significance |
|---|---|---|---|
| Hyperpigmentation | Palmar creases, buccal mucosa, lips, scars, pressure points, nipples, axillae, perineum | 90-95% | Pathognomonic of primary AI; absent in secondary |
| Postural hypotension | Systolic drop > 20 mmHg | 85-90% | Reflects volume depletion and cortisol deficiency |
| Vitiligo | Patchy depigmentation | 10-20% | Marker of autoimmune diathesis |
| Loss of axillary/pubic hair | Axillae, pubic region | More prominent in females | DHEA deficiency |
| Pallor | Generalised | Variable | Normocytic anaemia |
| Auricular cartilage calcification | Ear cartilage | Rare | Long-standing AI |
Associated Autoimmune Stigmata
Examine for features of associated conditions:
- Thyroid: Goitre, thyroid eye signs, pretibial myxoedema
- Vitiligo: Depigmented patches
- Diabetes: Acanthosis (if associated with insulin resistance in treatment)
- Alopecia: Patchy or total hair loss
Red Flags — Adrenal Crisis
[!CAUTION] Life-Threatening Emergency — Immediate Action Required:
- Hypotension (SBP less than 90 mmHg) not responding to IV fluids
- Shock, cardiovascular collapse
- Severe hyperkalaemia (K⁺ > 6.5 mmol/L)
- Hypoglycaemia (glucose less than 3.0 mmol/L)
- Altered consciousness, confusion, coma
- Severe hyponatraemia (less than 120 mmol/L)
- Severe abdominal pain with hypotension (may mimic surgical abdomen)
Immediate Treatment:
- Hydrocortisone 100 mg IV/IM STAT (do not wait for results)
- IV 0.9% saline 1L in first hour (adjust to clinical response)
- Monitor glucose — give IV dextrose if hypoglycaemic
- Identify and treat precipitant (commonly infection)
- Admit to high-dependency/intensive care if severe
5. Clinical Examination
Structured Approach
1. General Observation (from end of bed):
- Skin: Overall pigmentation (compare to patient's baseline if possible)
- Vital signs: Tachycardia, postural hypotension
- Hydration: Dry mucous membranes, reduced skin turgor
2. Hands and Arms:
- Palmar crease hyperpigmentation (compare to dorsum of hand)
- Nail beds: May be pigmented
- Skin creases and scars: Darker than surrounding skin
- Hair: Reduced axillary hair (females)
3. Face and Mouth:
- Sun-exposed areas: Hyperpigmented
- Buccal mucosa: Dark patches on cheeks, gums, tongue
- Lips: Hyperpigmented
4. Neck:
- Thyroid: Assess for goitre (associated autoimmune thyroid disease)
- Scars: Thyroidectomy, adrenalectomy
5. Trunk:
- Nipple areolae: Hyperpigmented
- Old surgical scars: Hyperpigmented
- Vitiligo patches
6. Cardiovascular:
- Blood pressure: Lying and standing (assess for postural drop)
- Heart sounds: Usually normal
7. Abdomen:
- Tenderness (may be present in crisis)
- No specific organomegaly (unless associated condition)
Special Tests
| Test | Technique | Interpretation |
|---|---|---|
| Postural Blood Pressure | BP supine after 5 min rest → BP standing at 1 and 3 min | Drop > 20 mmHg systolic or > 10 mmHg diastolic = orthostatic hypotension |
| Palmar Crease Pigmentation | Compare crease pigmentation to surrounding palm | Creases darker than dorsum = suggestive of primary AI |
| Buccal Mucosa Inspection | Examine inner cheeks, gums, under tongue | Dark patches pathognomonic |
| Scar Inspection | Examine old surgical or traumatic scars | Scars darken after AI onset (new scars pigmented) |
OSCE Examination Checklist
ADDISON'S DISEASE EXAMINATION
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
□ General: Underweight, unwell, pigmented
□ Vital signs: Postural BP, heart rate
HANDS:
□ Palmar crease hyperpigmentation
□ Nail bed pigmentation
□ Axillary hair (females)
FACE:
□ Buccal mucosa pigmentation
□ Lip pigmentation
□ Sun-exposed skin
TRUNK:
□ Nipple areolae
□ Scar pigmentation
□ Vitiligo
CARDIOVASCULAR:
□ Postural hypotension
ASSOCIATED CONDITIONS:
□ Thyroid examination
□ Vitiligo
□ Alopecia areata
COMPLETE BY:
□ "I would like to check blood glucose"
□ "I would like to see recent U&E results"
□ "I would examine for signs of precipitating infection"
6. Investigations
First-Line (Screening) Investigations
| Test | Expected Finding | Interpretation | Notes |
|---|---|---|---|
| Urea & Electrolytes | Low Na⁺, High K⁺ | Hyponatraemia (typically 120-130 mmol/L), Hyperkalaemia (5.5-6.5 mmol/L) | Classic pattern; may be normal in mild/early disease |
| Glucose | Low or low-normal | Cortisol required for gluconeogenesis | Hypoglycaemia in crisis |
| FBC | Normocytic anaemia, eosinophilia, lymphocytosis | Cortisol normally suppresses eosinophils | Eosinophil count > 500/μL suggestive |
| Calcium | May be elevated | Cortisol normally promotes calcium excretion | Mild hypercalcaemia in ~10% |
| 9 AM Serum Cortisol | Low (less than 100 nmol/L highly suggestive) | Screening test (not diagnostic) | > 500 nmol/L effectively excludes AI |
| Plasma ACTH | High (> 100 pg/mL) | Distinguishes primary from secondary | Must be taken with/before 9am cortisol; requires specific handling |
Interpretation of 9 AM Cortisol
| 9 AM Cortisol | Interpretation | Action |
|---|---|---|
| less than 100 nmol/L | Strongly suggestive of AI | Proceed to SST (or treat if crisis) |
| 100-400 nmol/L | Indeterminate | SST required |
| > 500 nmol/L | AI effectively excluded | Consider alternative diagnoses |
Short Synacthen Test (SST) — Gold Standard
The short Synacthen test (also called ACTH stimulation test or cosyntropin test) is the gold standard for diagnosing adrenal insufficiency. [4,12]
Protocol:
| Time | Action |
|---|---|
| 0 min | Take baseline blood for cortisol and ACTH |
| Administer Synacthen (tetracosactide) 250 μg IM or IV | |
| 30 min | Measure serum cortisol |
| (60 min) | Optional — measure cortisol (rarely needed) |
Interpretation:
| 30-min Cortisol | Interpretation |
|---|---|
| ≥450-550 nmol/L | Normal response — AI excluded |
| less than 450 nmol/L | Abnormal — confirms adrenal insufficiency |
Note: Different assays may use slightly different cut-offs (450-550 nmol/L). Check local laboratory reference ranges.
Exam Detail: SST Interpretation Pearls:
-
Primary vs Secondary AI: SST confirms AI but does not distinguish primary from secondary. Use concurrent ACTH level:
- ACTH elevated (> 2× ULN) = Primary AI
- ACTH low/normal = Secondary AI
-
Low-Dose SST (1 μg): Some centres use 1 μg Synacthen for greater sensitivity in detecting partial AI. Not universally adopted.
-
Timing Considerations:
- Best performed in morning (8-9 AM) when cortisol is at peak
- Can be performed at any time in emergencies
-
False Negatives in Secondary AI: In recent-onset secondary AI (e.g., pituitary surgery), the adrenals may still respond normally to exogenous ACTH. Insulin tolerance test (ITT) may be needed.
-
In Crisis: Do NOT delay treatment to perform SST. Take a random cortisol and ACTH, then treat immediately. SST can be performed later during recovery.
Further Investigations
To Confirm Aetiology
| Test | Purpose | Expected in Autoimmune PAI |
|---|---|---|
| 21-Hydroxylase Antibodies (21-OH Ab) | Confirm autoimmune aetiology | Positive in 86-90% of autoimmune AI [6] |
| Adrenal Cortex Antibodies (ACA) | Alternative autoantibody test | Less specific than 21-OH Ab |
| CT Adrenals | Exclude structural causes | Small, atrophic adrenals (autoimmune); calcified (TB); enlarged (haemorrhage, metastases, infection) |
| Very Long Chain Fatty Acids (VLCFA) | Screen for adrenoleukodystrophy | Elevated C26:0 and C26:0/C22:0 ratio in ALD [11] |
| Chest X-ray / CT Chest | TB screening | Pulmonary TB features |
CT Adrenal Findings by Aetiology
| Aetiology | CT Appearance |
|---|---|
| Autoimmune | Small, atrophic adrenals bilaterally |
| Tuberculosis (early) | Bilateral adrenal enlargement |
| Tuberculosis (late) | Adrenal calcification, atrophy |
| Adrenal haemorrhage | Enlarged, hyperdense (acute); atrophy (chronic) |
| Metastatic disease | Bilateral masses, irregular |
| Adrenoleukodystrophy | May be normal or show brain white matter changes |
Screening for Associated Autoimmune Conditions
| Test | Condition Screened | Frequency of Association |
|---|---|---|
| TSH, Free T4 | Autoimmune thyroid disease | 40-50% |
| HbA1c, Fasting glucose | Type 1 diabetes | 10-20% |
| Tissue transglutaminase IgA | Coeliac disease | 5-10% |
| Vitamin B12, Intrinsic factor Ab | Pernicious anaemia | 5-10% |
| FSH, LH, Oestradiol (females) | Premature ovarian insufficiency | 10-20% |
| Anti-TPO, Anti-thyroglobulin | Hashimoto's thyroiditis | 40-50% |
Recommendation: Screen all patients with autoimmune PAI annually for thyroid dysfunction (TSH) and periodically for other autoimmune conditions. [4]
Investigation Algorithm
SUSPECTED ADDISON'S DISEASE
↓
┌─────────────────────────────────────┐
│ Initial Investigations: │
│ • U&E, glucose, FBC, calcium │
│ • 9 AM cortisol + ACTH (paired) │
└─────────────────────────────────────┘
↓
┌────────────────────────────────┐
│ 9 AM Cortisol Result: │
├────────────────────────────────┤
│ less than 100 nmol/L → Highly suggestive│
│ 100-400 nmol/L → Indeterminate │
│ > 500 nmol/L → AI excluded │
└────────────────────────────────┘
↓ (if less than 500)
┌─────────────────────────────────────┐
│ SHORT SYNACTHEN TEST (SST) │
│ 250 μg Synacthen IM/IV │
│ Measure cortisol at 30 min │
│ │
│ • ≥450-550 nmol/L = Normal │
│ • less than 450 nmol/L = Adrenal insufficiency│
└─────────────────────────────────────┘
↓
┌────────────────────────────────┐
│ ACTH Level: │
├────────────────────────────────┤
│ Elevated → PRIMARY AI (Addison's)│
│ Low/Normal → SECONDARY AI │
└────────────────────────────────┘
↓
┌─────────────────────────────────────┐
│ AETIOLOGY WORKUP: │
│ • 21-Hydroxylase antibodies │
│ • CT adrenals │
│ • VLCFA (young males) │
│ • Autoimmune screen (TSH, HbA1c, │
│ coeliac serology, B12) │
└─────────────────────────────────────┘
7. Differential Diagnosis
Conditions Mimicking Addison's Disease
| Condition | Similarities | Distinguishing Features |
|---|---|---|
| Secondary Adrenal Insufficiency | Fatigue, weight loss, hypoglycaemia, low cortisol | Low ACTH, no hyperpigmentation, no hyperkalaemia, mineralocorticoid axis intact |
| Chronic Fatigue Syndrome | Fatigue, myalgias | Normal cortisol response to SST, normal electrolytes |
| Depression | Fatigue, weight change, low mood | Weight gain more common; normal investigations |
| Anorexia Nervosa | Weight loss, fatigue | Normal or elevated cortisol; different psychological profile |
| Malignancy | Weight loss, fatigue, anorexia | Tumour markers, imaging findings |
| Hyperthyroidism | Weight loss, fatigue, tremor | Elevated T4, suppressed TSH; different symptom complex |
| Diabetes Mellitus | Weight loss, fatigue | Hyperglycaemia (not hypoglycaemia) |
| GI Disorders | Abdominal pain, nausea, weight loss | Normal electrolytes, different investigations |
Key Differentiating Points
Primary vs Secondary Adrenal Insufficiency:
| Feature | Primary (Addison's) | Secondary |
|---|---|---|
| ACTH | ↑↑ High | ↓ Low |
| Aldosterone | ↓ Low | Normal |
| Hyperpigmentation | Present | Absent |
| Hyperkalaemia | Present | Absent |
| Cause | Adrenal pathology | Pituitary/hypothalamic |
| Associated features | Other autoimmune conditions | Visual field defects, headache, other pituitary hormone deficiencies |
8. Classification
Autoimmune Polyglandular Syndromes (APS)
Autoimmune adrenalitis often occurs as part of autoimmune polyglandular syndromes:
| Type | Genetics | Key Features | Adrenal Component |
|---|---|---|---|
| APS-1 (APECED) | AIRE gene mutation (autosomal recessive) | Chronic mucocutaneous candidiasis, hypoparathyroidism, Addison's | Present in 60-70% |
| APS-2 (Schmidt Syndrome) | Polygenic (HLA-associated) | Addison's + autoimmune thyroid disease ± Type 1 DM | Defining feature |
| APS-4 | Polygenic | Addison's + other autoimmune (not APS-2) | With ≥1 non-APS-2 condition |
Causes of Primary Adrenal Insufficiency — Classification
1. Autoimmune (80-90% in developed countries)
- Isolated autoimmune adrenalitis
- APS-1 (APECED)
- APS-2 (Schmidt syndrome)
2. Infectious
- Tuberculosis (most common globally)
- Fungal (histoplasmosis, coccidioidomycosis)
- CMV adrenalitis (HIV/AIDS)
- MAC (HIV/AIDS)
3. Infiltrative/Metastatic
- Metastatic carcinoma (lung, breast, melanoma)
- Lymphoma
- Amyloidosis
- Haemochromatosis
- Sarcoidosis
4. Haemorrhagic
- Waterhouse-Friderichsen syndrome (meningococcal sepsis)
- Anticoagulant therapy
- Trauma
- Post-surgical
5. Genetic
- Adrenoleukodystrophy (X-linked)
- Congenital adrenal hyperplasia
- Adrenal hypoplasia congenita (DAX1 mutation)
- Triple A syndrome (Allgrove)
6. Iatrogenic
- Bilateral adrenalectomy
- Drug-induced (ketoconazole, etomidate, mitotane)
9. Management
Management Algorithm
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
ADDISON'S DISEASE MANAGEMENT
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
┌─────────────────────────────────────────────────────────────────┐
│ ACUTE: ADRENAL CRISIS — LIFE-THREATENING EMERGENCY │
├─────────────────────────────────────────────────────────────────┤
│ │
│ IMMEDIATE (within minutes): │
│ 1. IV access — take bloods: cortisol, ACTH, U&E, glucose, FBC │
│ 2. HYDROCORTISONE 100 mg IV/IM STAT │
│ (Do NOT delay for investigations) │
│ 3. IV 0.9% SALINE — 1 litre in first hour │
│ (Then guided by clinical response) │
│ 4. IV DEXTROSE if hypoglycaemic │
│ │
│ ONGOING: │
│ • Hydrocortisone 50-100 mg IV every 6-8 hours │
│ • Continue IV fluids (may need 2-4L in first 24 hours) │
│ • Cardiac monitoring (hyperkalaemia risk) │
│ • Treat precipitant (commonly infection) │
│ • ITU/HDU if haemodynamically unstable │
│ │
│ Note: Fludrocortisone NOT needed acutely │
│ (High-dose HC has mineralocorticoid activity) │
│ │
│ TRANSITION TO ORAL: │
│ • When stable and eating: convert to oral HC │
│ • Taper over 3-4 days to maintenance dose │
│ • Add fludrocortisone when HC less than 50 mg/day │
└─────────────────────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────────────┐
│ CHRONIC: LIFELONG REPLACEMENT THERAPY │
├─────────────────────────────────────────────────────────────────┤
│ │
│ GLUCOCORTICOID REPLACEMENT: │
│ │
│ HYDROCORTISONE (First-line) [4,13] │
│ • Total daily dose: 15-25 mg/day (typically 15-20 mg) │
│ • Divided into 2-3 doses to mimic circadian rhythm: │
│ │
│ ┌──────────────────────────────────────────────────────┐ │
│ │ REGIMEN A (3 doses): │ │
│ │ • 10 mg on waking (6-8 AM) │ │
│ │ • 5 mg at midday (12-1 PM) │ │
│ │ • 5 mg late afternoon (4-6 PM) │ │
│ │ Total: 20 mg/day │ │
│ ├──────────────────────────────────────────────────────┤ │
│ │ REGIMEN B (3 doses, lower): │ │
│ │ • 10 mg on waking │ │
│ │ • 5 mg at midday │ │
│ │ • 2.5 mg late afternoon │ │
│ │ Total: 17.5 mg/day │ │
│ ├──────────────────────────────────────────────────────┤ │
│ │ REGIMEN C (2 doses): │ │
│ │ • 15 mg on waking │ │
│ │ • 5 mg early afternoon │ │
│ │ Total: 20 mg/day │ │
│ └──────────────────────────────────────────────────────┘ │
│ │
│ • Give largest dose on waking (mimics cortisol peak) │
│ • Avoid evening doses (interferes with sleep) │
│ • Do NOT give with grapefruit juice (CYP3A4) │
│ │
│ ALTERNATIVES: │
│ • Modified-release hydrocortisone (Plenadren): 20-25 mg OD │
│ - Better cortisol profile; improves QoL in some [14] │
│ - More expensive; not universally available │
│ • Prednisolone: 3-5 mg daily (rarely used; less physiological) │
│ │
├─────────────────────────────────────────────────────────────────┤
│ MINERALOCORTICOID REPLACEMENT: │
│ │
│ FLUDROCORTISONE [4] │
│ • Dose: 50-200 micrograms once daily (typically 100 mcg) │
│ • Give in the morning with hydrocortisone │
│ • Titrate to: │
│ - Blood pressure (avoid hypertension) │
│ - Serum potassium (aim normal range) │
│ - Plasma renin activity (aim upper normal) │
│ • Most patients need 100 mcg; range 50-200 mcg │
│ │
├─────────────────────────────────────────────────────────────────┤
│ DHEA REPLACEMENT (Optional): │
│ │
│ • Consider DHEA 25-50 mg daily in FEMALES if: │
│ - Persistent fatigue despite optimised HC/FC │
│ - Reduced libido │
│ - Impaired well-being │
│ • Evidence is mixed; 2016 guideline: trial for 6 months [4,15] │
│ • Not available on NHS prescription (patient purchase) │
│ • Monitor for androgenic side effects (acne, hirsutism) │
│ │
└─────────────────────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────────────┐
│ SICK DAY RULES — CRITICAL PATIENT EDUCATION │
├─────────────────────────────────────────────────────────────────┤
│ │
│ ⚠️ SICK DAY RULES PREVENT ADRENAL CRISIS [7,16] │
│ │
│ ┌────────────────────────────────────────────────────────────┐ │
│ │ SITUATION │ HYDROCORTISONE ACTION │ │
│ ├────────────────────────────────┼───────────────────────────┤ │
│ │ Minor illness (cold, mild │ DOUBLE total daily dose │ │
│ │ infection without fever) │ until recovered │ │
│ ├────────────────────────────────┼───────────────────────────┤ │
│ │ Moderate illness (fever > 38°C, │ TRIPLE total daily dose │ │
│ │ significant infection) │ until recovered │ │
│ ├────────────────────────────────┼───────────────────────────┤ │
│ │ Vomiting/diarrhoea (cannot │ IM HYDROCORTISONE 100 mg │ │
│ │ keep tablets down) │ STAT → seek medical help │ │
│ ├────────────────────────────────┼───────────────────────────┤ │
│ │ Major stress (trauma, severe │ IM/IV HYDROCORTISONE │ │
│ │ illness, surgery) │ 100 mg → hospital │ │
│ └────────────────────────────────┴───────────────────────────┘ │
│ │
│ KEY MESSAGES: │
│ • NEVER stop hydrocortisone suddenly │
│ • If vomiting, switch to IM injection — do not wait │
│ • Return to normal dose when fully recovered │
│ • If unsure, take MORE not less │
│ │
└─────────────────────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────────────────┐
│ ESSENTIAL PATIENT EQUIPMENT & IDENTIFICATION │
├─────────────────────────────────────────────────────────────────┤
│ │
│ MANDATORY: │
│ □ Steroid emergency card (carry at ALL times) │
│ □ MedicAlert bracelet/necklace or equivalent │
│ □ Emergency hydrocortisone injection kit: │
│ • Hydrocortisone 100 mg powder + Water for Injection │
│ • Patient and family/carer trained in administration │
│ │
│ DOCUMENTATION: │
│ □ Written sick-day rules │
│ □ Emergency contact numbers │
│ □ GP and endocrinologist contact details │
│ │
└─────────────────────────────────────────────────────────────────┘
Surgical/Procedural Steroid Cover
Patients with Addison's disease require stress-dose glucocorticoids for surgery and invasive procedures:
| Procedure Category | Hydrocortisone Cover |
|---|---|
| Minor (dental, local anaesthetic, minor skin) | Double morning dose or 20 mg extra |
| Moderate (inguinal hernia, laparoscopic cholecystectomy) | Hydrocortisone 25 mg IV at induction, then 25 mg 8-hourly for 24-48 hours, then taper |
| Major (cardiac surgery, bowel resection, major orthopaedic) | Hydrocortisone 100 mg IV at induction, then 50-100 mg IV every 6-8 hours for 48-72 hours, then taper to oral |
Key Principle: Always give hydrocortisone cover; withhold usual fludrocortisone until oral intake and lower HC doses resume (HC has mineralocorticoid activity at high doses). [17]
Special Populations
Pregnancy [18]
| Aspect | Management |
|---|---|
| Glucocorticoid | Continue hydrocortisone; may need to increase dose by 20-40% in third trimester |
| Mineralocorticoid | May need to increase fludrocortisone (physiological anti-mineralocorticoid effect of progesterone) |
| Delivery | Stress-dose hydrocortisone: 100 mg IV at onset of active labour, then 50 mg 6-8 hourly until oral intake |
| Monitoring | Monitor for nausea/vomiting (may need IV HC); monitor BP |
| Postpartum | Return to pre-pregnancy dose; monitor for postpartum adrenal crisis |
Elderly
- May require lower hydrocortisone doses (reduced clearance)
- Higher risk of osteoporosis with over-replacement
- Be vigilant for atypical crisis presentations
Children
- Weight-based dosing: Hydrocortisone 8-10 mg/m²/day in 3 divided doses
- Growth monitoring (over-replacement suppresses growth)
- School and carer education essential
Monitoring
| Parameter | Frequency | Target/Notes |
|---|---|---|
| Clinical assessment | Every visit | Weight, BP (supine and standing), symptoms |
| Electrolytes (U&E) | 3-6 monthly initially, then annually | Normal sodium and potassium |
| Plasma renin activity | Annually | Aim upper normal (guides fludrocortisone dosing) |
| Bone density (DEXA) | Every 2-3 years | Monitor for osteoporosis from over-replacement |
| Thyroid function (TSH) | Annually | Screen for associated thyroid disease |
| HbA1c / Fasting glucose | Annually | Screen for Type 1 diabetes |
| Patient education | Every visit | Reinforce sick-day rules |
10. Complications
Adrenal Crisis
Adrenal crisis is the most serious complication and is a medical emergency. [7]
| Feature | Details |
|---|---|
| Incidence | 6-8 crises per 100 patient-years [7] |
| Mortality | 0.5% per crisis episode |
| Common Triggers | Gastroenteritis, febrile illness, surgery, trauma, non-compliance |
| Presentation | Hypotension, shock, confusion, abdominal pain, vomiting |
| Biochemistry | Hyponatraemia, hyperkalaemia, hypoglycaemia |
| Immediate Treatment | Hydrocortisone 100 mg IV + IV 0.9% saline |
Long-Term Complications
| Complication | Mechanism | Prevention/Management |
|---|---|---|
| Cardiovascular disease | Glucocorticoid effects; altered lipid metabolism | Avoid over-replacement; cardiovascular risk assessment |
| Osteoporosis | Glucocorticoid excess (over-replacement) | Use lowest effective HC dose; DEXA monitoring; calcium/vitamin D |
| Reduced bone mineral density | Over-replacement; disease effect | Optimise dosing; lifestyle measures |
| Impaired quality of life | Fatigue despite treatment | Optimise replacement; consider DHEA in females; address psychological impact |
| Infections | May be at increased risk | Vaccinations; prompt sick-day dosing |
| Associated autoimmune conditions | Shared autoimmune predisposition | Annual screening (TSH, glucose) |
Treatment-Related Complications
| Problem | Cause | Signs | Management |
|---|---|---|---|
| Over-replacement (Cushingoid) | Excess hydrocortisone | Weight gain, moon face, striae, hypertension, osteoporosis, hyperglycaemia | Reduce hydrocortisone dose |
| Under-replacement | Inadequate hydrocortisone | Fatigue, weight loss, hypotension, crisis risk | Increase hydrocortisone dose |
| Fludrocortisone excess | Too much mineralocorticoid | Hypertension, oedema, hypokalaemia | Reduce fludrocortisone dose |
| Fludrocortisone deficiency | Inadequate mineralocorticoid | Hypotension, salt craving, hyperkalaemia, elevated renin | Increase fludrocortisone dose |
11. Prognosis & Outcomes
Natural History
Untreated Addison's disease is invariably fatal, typically from adrenal crisis during intercurrent illness or stress. Thomas Addison's original patients all died within months to years of diagnosis. [1]
Outcomes with Modern Treatment
| Variable | Outcome | Evidence |
|---|---|---|
| Life expectancy | Near-normal with optimal management | Slight excess mortality (SMR 1.5-2.1) mainly from adrenal crisis and cardiovascular disease [19] |
| Quality of life | Generally good; ~30% report persistent fatigue | May be improved with modified-release HC or DHEA [14,15] |
| Adrenal crisis rate | ~6-8 per 100 patient-years | Reduced with good patient education [7] |
| Mortality from crisis | ~0.5% per episode | Higher in elderly and those with delayed treatment |
| Cardiovascular risk | Possibly increased | Under investigation; multifactorial |
Prognostic Factors
Favourable Prognosis:
- Early diagnosis before first crisis
- Excellent patient education and understanding
- Regular follow-up and monitoring
- Access to emergency hydrocortisone
- Carries identification (steroid card, MedicAlert)
- Supportive family/social network
Poorer Prognosis:
- Delayed diagnosis with crisis presentation
- Poor understanding of sick-day rules
- Non-compliance with medication
- Living alone without support
- Concurrent serious illness
- Elderly patients
- Limited healthcare access
12. Evidence & Guidelines
Key Guidelines
| Guideline | Organisation | Year | Key Recommendations |
|---|---|---|---|
| Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline [4] | Endocrine Society | 2016 | Comprehensive diagnosis, replacement therapy, crisis prevention |
| Emergency Management of Adrenal Insufficiency | Society for Endocrinology | 2020 | UK emergency protocols |
| European Expert Consensus Statement on Adrenal Insufficiency [20] | European Society of Endocrinology | 2014 | Diagnosis and long-term management |
Landmark Studies
Arlt & Allolio (2003) — Lancet Review [2]
- Comprehensive review establishing modern understanding of adrenal insufficiency
- Defined approach to diagnosis, replacement, and complications
- Clinical Impact: Foundational reference for current management paradigms
Hahner et al. (2015) — JCEM [7]
- Prospective study of adrenal crisis frequency and outcomes
- Crisis rate: 6-8 per 100 patient-years
- Clinical Impact: Demonstrated importance of patient education and prevention strategies
Johannsson et al. (2012) — JCEM [14]
- RCT of modified-release hydrocortisone (Plenadren) vs conventional HC
- Improved metabolic profile and quality of life
- Clinical Impact: Established role for modified-release preparations
Evidence Strength Summary
| Intervention | Level of Evidence | Key Evidence |
|---|---|---|
| Short Synacthen Test | 1b | Established diagnostic gold standard |
| Hydrocortisone replacement | 1a | Meta-analyses, RCTs, guidelines [4] |
| Fludrocortisone | 2a | Cohort studies, guidelines |
| DHEA supplementation | 1b | RCTs with mixed results [15] |
| Sick-day rules | 2b | Observational studies, crisis reduction [7] |
| Modified-release HC | 1b | RCTs showing benefit [14] |
13. Exam-Focused Sections
Common Exam Questions (MRCP, PLAB)
- "What are the causes of primary adrenal insufficiency?"
- "How would you investigate a patient with suspected Addison's disease?"
- "How would you differentiate primary from secondary adrenal insufficiency?"
- "What is your emergency management of adrenal crisis?"
- "What are the sick-day rules for patients with Addison's disease?"
- "How would you manage a patient with Addison's disease undergoing surgery?"
- "What biochemical abnormalities would you expect in Addison's disease?"
Viva Points
Viva Point: Opening Statement: "Addison's disease is primary adrenal insufficiency characterised by destruction of the adrenal cortex, leading to deficiency of cortisol, aldosterone, and adrenal androgens. In developed countries, autoimmune adrenalitis accounts for 80-90% of cases. [2,4]"
Key Facts to Quote:
- Prevalence: ~140 per million; incidence 4-6 per million per year [5]
- Autoantibody: 21-hydroxylase antibodies in 90% of autoimmune cases [6]
- Diagnostic test: Short Synacthen test — cortisol should rise to > 450-500 nmol/L at 30 minutes
- Treatment: Hydrocortisone 15-25 mg/day in divided doses + fludrocortisone 50-200 mcg OD [4]
- Crisis rate: 6-8 per 100 patient-years, reduced with education [7]
Structured Approach to Diagnosis: "I would approach this systematically. First, I would take a detailed history focusing on fatigue, weight loss, salt craving, postural symptoms, and associated autoimmune conditions. On examination, I would look for hyperpigmentation of palmar creases and buccal mucosa, postural hypotension, and features of associated conditions. Investigations would include U&E showing hyponatraemia and hyperkalaemia, 9 AM cortisol and ACTH, and a Short Synacthen test. If confirmed, I would investigate the aetiology with 21-hydroxylase antibodies and CT adrenals."
Model Answers
Q: How do you distinguish primary from secondary adrenal insufficiency?
"The key distinguishing features are:
-
ACTH level: Elevated in primary AI (loss of negative feedback from low cortisol), low in secondary AI (pituitary failure)
-
Hyperpigmentation: Present in primary AI (elevated ACTH/MSH from POMC), absent in secondary AI
-
Mineralocorticoid deficiency: Present in primary AI (aldosterone deficiency), preserved in secondary AI (RAAS system intact, independent of ACTH)
-
Hyperkalaemia: Present in primary AI (aldosterone deficiency), absent in secondary AI
-
Aetiology: Primary AI is due to adrenal pathology (autoimmune, TB, etc.); secondary AI is due to pituitary or hypothalamic pathology (tumour, surgery, Sheehan's, etc.)
A paired cortisol and ACTH at 9 AM is the key initial investigation to distinguish these."
Q: What is your emergency management of adrenal crisis?
"Adrenal crisis is a medical emergency requiring immediate treatment. My approach would be:
-
Do not delay treatment for investigations — if clinically suspected, treat immediately
-
Immediate actions:
- IV access and take bloods (cortisol, ACTH, U&E, glucose, FBC)
- Hydrocortisone 100 mg IV or IM STAT
- IV 0.9% saline — 1 litre in the first hour, then guided by response
- IV dextrose if hypoglycaemic
-
Ongoing management:
- Hydrocortisone 50-100 mg IV every 6-8 hours
- Continue IV fluids (may need 2-4L in first 24 hours)
- Cardiac monitoring for hyperkalaemia
- Identify and treat the precipitant (most commonly infection)
- Consider ITU/HDU if haemodynamically unstable
-
Fludrocortisone is NOT needed acutely — high-dose hydrocortisone has adequate mineralocorticoid activity
-
Transition to oral when stable and eating, with gradual taper to maintenance doses."
Common Mistakes (What Fails Candidates)
❌ Mistakes that lose marks:
- Forgetting that hyperpigmentation is absent in secondary AI
- Not knowing the SST protocol (250 μg Synacthen, measure at 30 min)
- Stating wrong cortisol cut-off (should be 450-500 nmol/L, not 550)
- Forgetting to mention fludrocortisone in chronic management
- Not knowing sick-day rules
- Missing the need for steroid card and emergency injection kit
- Waiting for investigation results before treating crisis
❌ Dangerous errors:
- Delaying hydrocortisone in crisis to wait for results
- Forgetting stress-dose steroids for surgery
- Allowing patients to stop steroids abruptly
MCQ-Style Questions
Q1. A 35-year-old woman presents with fatigue, weight loss, and hyperpigmentation of her palmar creases. Blood tests show: Na⁺ 128, K⁺ 5.8, cortisol 85 nmol/L at 9 AM. What is the next best investigation?
A) MRI pituitary B) CT adrenal glands C) Short Synacthen test D) 24-hour urinary free cortisol E) Insulin tolerance test
Answer: C) Short Synacthen test
Explanation: The clinical picture and 9 AM cortisol less than 100 nmol/L are highly suggestive of adrenal insufficiency. The Short Synacthen test is the gold standard diagnostic test. ACTH should also be measured to distinguish primary from secondary. CT adrenals would be appropriate once diagnosis is confirmed to investigate aetiology.
Q2. A patient with known Addison's disease develops gastroenteritis with vomiting. She takes hydrocortisone 20 mg/day and fludrocortisone 100 mcg/day. What advice should she be given?
A) Continue usual doses and drink fluids B) Double the hydrocortisone dose C) Triple the hydrocortisone dose D) Take IM hydrocortisone 100 mg and attend hospital E) Stop fludrocortisone until better
Answer: D) Take IM hydrocortisone 100 mg and attend hospital
Explanation: Vomiting means oral medication cannot be reliably absorbed. She should use her emergency hydrocortisone injection (IM 100 mg) and seek medical attention. This is a core sick-day rule. [7,16]
14. Patient/Layperson Explanation
What is Addison's Disease?
Addison's disease is a condition where your adrenal glands (small glands that sit on top of your kidneys) don't make enough of certain vital hormones. The main hormones affected are:
- Cortisol — helps your body respond to stress, control blood sugar, and fight infection
- Aldosterone — helps control your blood pressure and balance of salt and water in your body
Without these hormones, you can become very unwell, especially during times of stress like illness, injury, or surgery.
What Causes It?
In most cases (about 8 out of 10 people in the UK), the body's own immune system mistakenly attacks the adrenal glands. This is called "autoimmune" disease. Other causes include tuberculosis (more common in other parts of the world), infections, or rarely, cancer spreading to the adrenal glands.
What Are the Symptoms?
Symptoms often develop gradually over weeks to months and include:
- Extreme tiredness and weakness
- Weight loss and loss of appetite
- Feeling sick or being sick
- Dizziness when standing up
- Craving salty foods
- Darkening of the skin, especially in skin creases, inside the mouth, and on scars
- Muscle aches and pains
How Is It Diagnosed?
Your doctor will do blood tests to check your cortisol levels and other hormones. The main test is called the "Short Synacthen Test" — this involves giving you an injection that should make your adrenal glands produce cortisol. If your glands are damaged, they won't respond properly.
How Is It Treated?
You will need to take replacement hormones every day for the rest of your life:
1. Hydrocortisone tablets (replaces cortisol)
- Usually 2-3 times a day
- The largest dose is taken in the morning to copy your body's natural pattern
2. Fludrocortisone tablets (replaces aldosterone)
- Usually once daily in the morning
Sick-Day Rules — Very Important!
When you're unwell, your body needs more cortisol. You MUST increase your hydrocortisone dose:
| Situation | What to Do |
|---|---|
| Cold, mild illness without fever | Double your daily hydrocortisone dose |
| Fever (> 38°C), significant illness | Triple your daily hydrocortisone dose |
| Vomiting or can't keep tablets down | Give yourself the emergency injection (100 mg hydrocortisone) and go to hospital |
Never stop your hydrocortisone suddenly — this could make you very unwell.
What You Should Always Have
- Steroid emergency card — carry it with you at all times
- MedicAlert bracelet or necklace — so medical staff know about your condition if you can't tell them
- Emergency hydrocortisone injection kit — you and your family/friends should know how to use this
When to Seek Emergency Help
Go to A&E immediately if you:
- Feel very weak or faint
- Are vomiting and can't keep tablets down
- Collapse or feel you might collapse
- Have severe abdominal pain with feeling very unwell
- Have confusion or drowsiness
Tell them you have Addison's disease and may need emergency hydrocortisone.
Living with Addison's Disease
- With proper treatment, you can live a full, normal, and active life
- You'll need regular check-ups (usually every 6-12 months)
- Most people do well and have normal life expectancy
- Learning about your condition and the sick-day rules is very important
15. References
Primary Guidelines
-
Addison T. On the constitutional and local effects of disease of the suprarenal capsules. London: Samuel Highley. 1855. [Historical text]
-
Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003;361(9372):1881-1893. doi:10.1016/S0140-6736(03)13492-7 PMID: 12788587
-
Betterle C, Dal Pra C, Mantero F, Zanchetta R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr Rev. 2002;23(3):327-364. doi:10.1210/edrv.23.3.0466 PMID: 12050123
-
Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710 PMID: 26760044
-
Erichsen MM, Løvås K, Skinningsrud B, et al. Clinical, immunological, and genetic features of autoimmune primary adrenal insufficiency: observations from a Norwegian registry. J Clin Endocrinol Metab. 2009;94(12):4882-4890. doi:10.1210/jc.2009-1368 PMID: 19858318
-
Winqvist O, Karlsson FA, Kämpe O. 21-Hydroxylase, a major autoantigen in idiopathic Addison's disease. Lancet. 1992;339(8809):1559-1562. doi:10.1016/0140-6736(92)91829-w PMID: 1351548
-
Hahner S, Spinnler C, Gasperi M, et al. High incidence of adrenal crisis in educated patients with chronic adrenal insufficiency: a prospective study. J Clin Endocrinol Metab. 2015;100(2):407-416. doi:10.1210/jc.2014-3191 PMID: 25419882
-
Findling JW, Raff H. Clinical review: Cushing's syndrome--important issues in diagnosis and management. J Clin Endocrinol Metab. 2006;91(10):3746-3753. doi:10.1210/jc.2006-0997 PMID: 16868050
-
Neary N, Nieman L. Adrenal insufficiency: etiology, diagnosis and treatment. Curr Opin Endocrinol Diabetes Obes. 2010;17(3):217-223. doi:10.1097/MED.0b013e328338f608 PMID: 20375886
-
Olafsson AS, Sigurjonsdottir HA. Increasing Prevalence of Addison Disease: Results from a Nationwide Study. Endocr Pract. 2016;22(1):30-35. doi:10.4158/EP15754.OR PMID: 26401579
-
Moser HW, Raymond GV, Dubey P. Adrenoleukodystrophy: new approaches to a neurodegenerative disease. JAMA. 2005;294(24):3131-3134. doi:10.1001/jama.294.24.3131 PMID: 16380592
-
Kazlauskaite R, Evans AT, Villabona CV, et al. Corticotropin tests for hypothalamic-pituitary-adrenal insufficiency: a metaanalysis. J Clin Endocrinol Metab. 2008;93(11):4245-4253. doi:10.1210/jc.2008-0710 PMID: 18697863
-
Mah PM, Jenkins RC, Rostami-Hodjegan A, et al. Weight-related dosing, timing and monitoring hydrocortisone replacement therapy in patients with adrenal insufficiency. Clin Endocrinol (Oxf). 2004;61(3):367-375. doi:10.1111/j.1365-2265.2004.02106.x PMID: 15355454
-
Johannsson G, Nilsson AG, Bergthorsdottir R, et al. Improved cortisol exposure-time profile and outcome in patients with adrenal insufficiency: a prospective randomized trial of a novel hydrocortisone dual-release formulation. J Clin Endocrinol Metab. 2012;97(2):473-481. doi:10.1210/jc.2011-1926 PMID: 22112807
-
Alkatib AA, Cosma M, Elamin MB, et al. A systematic review and meta-analysis of randomized placebo-controlled trials of DHEA treatment effects on quality of life in women with adrenal insufficiency. J Clin Endocrinol Metab. 2009;94(10):3676-3681. doi:10.1210/jc.2009-0672 PMID: 19773400
-
Woodcock T, Barker P, Daniel S, et al. Guidelines for the management of glucocorticoids during the peri-operative period for patients with adrenal insufficiency. Anaesthesia. 2020;75(5):654-663. doi:10.1111/anae.14963 PMID: 32017015
-
Jung C, Inder WJ. Management of adrenal insufficiency during the stress of medical illness and surgery. Med J Aust. 2008;188(7):409-413. doi:10.5694/j.1326-5377.2008.tb01686.x PMID: 18393745
-
Lebbe M, Arlt W. What is the best diagnostic and therapeutic management strategy for an Addison patient during pregnancy? Clin Endocrinol (Oxf). 2013;78(4):497-502. doi:10.1111/cen.12097 PMID: 23173890
-
Bergthorsdottir R, Leonsson-Zachrisson M, Odén A, Johannsson G. Premature mortality in patients with Addison's disease: a population-based study. J Clin Endocrinol Metab. 2006;91(12):4849-4853. doi:10.1210/jc.2006-0076 PMID: 16968806
-
Husebye ES, Allolio B, Arlt W, et al. Consensus statement on the diagnosis, treatment and follow-up of patients with primary adrenal insufficiency. J Intern Med. 2014;275(2):104-115. doi:10.1111/joim.12162 PMID: 24330030
Further Resources
- Addison's Disease Self-Help Group (UK): addisons.org.uk
- Society for Endocrinology: endocrinology.org
- Patient.info Addison's Disease: patient.info/hormones/addisons-disease
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Clinical decisions should account for individual patient circumstances. Always consult appropriate guidelines and specialists for patient care.
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for addison?
Seek immediate emergency care if you experience any of the following warning signs: Adrenal crisis (hypotension, collapse, confusion), Severe hyperkalaemia (less than 6.5 mmol/L), Hypoglycaemia (less than 3.0 mmol/L), Unexplained shock refractory to fluids, Abdominal pain with hypotension, Severe hyponatraemia (less than 120 mmol/L), Altered consciousness in known Addisonian.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Hypothalamic-Pituitary-Adrenal Axis Physiology
- Steroid Hormone Biochemistry
Differentials
Competing diagnoses and look-alikes to compare.
- Secondary Adrenal Insufficiency
- Chronic Fatigue Syndrome
Consequences
Complications and downstream problems to keep in mind.