Stable Angina
Comprehensive evidence-based guide to stable angina diagnosis and management including CCS classification, investigations, medical therapy, and revascularization
What matters first
Comprehensive evidence-based guide to stable angina diagnosis and management including CCS classification, investigations, medical therapy, and revascularization
Check the red flags, emergency triggers, and escalation points before using the deep-dive material.
9 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Stable Angina
Quick Reference
Critical Alerts
- Distinguish stable from unstable angina: Unstable angina (rest pain, crescendo pattern, new-onset severe) is an ACS emergency requiring immediate admission
- CTCA is first-line investigation for suspected stable angina per NICE guidelines (not exercise stress test)
- All patients require secondary prevention: Aspirin, high-intensity statin, ACE inhibitor consideration regardless of symptom control
- GTN non-response after 3 doses (15 minutes) = call 999: Potential ACS, patient should not delay seeking emergency care
- COURAGE and ISCHEMIA trials: Revascularization in stable CAD does not reduce mortality vs optimal medical therapy; reserve for refractory symptoms or high-risk anatomy
- Beta-blockers are first-line anti-anginal therapy: Reduce heart rate and myocardial oxygen demand
- SYNTAX score guides PCI vs CABG decision: High SYNTAX score (> 32) favors CABG in multivessel disease
- FFR/iFR guides revascularization: Functional significance of stenosis matters more than angiographic appearance
Classic Presentation
| Feature | Description |
|---|---|
| Location | Retrosternal, may radiate to jaw, neck, left arm, back |
| Quality | Tight, heavy, constricting, pressure, "elephant on chest" |
| Intensity | Moderate to severe (4-8/10) |
| Duration | 2-10 minutes (typically less than 20 minutes) |
| Triggers | Exertion, cold weather, emotional stress, heavy meals |
| Relief | Rest or sublingual GTN within 5-10 minutes |
| Pattern | Predictable, stable pattern over time |
Emergency Treatments
| Scenario | Immediate Action | Notes |
|---|---|---|
| Acute angina episode | GTN spray 400 mcg SL (1-2 sprays) | May repeat every 5 min x 3 doses |
| No relief after 3 GTN doses | Call 999, give aspirin 300 mg | Suspect ACS |
| Unstable features | Emergency admission | Rest pain, crescendo, new-onset severe |
Definition
Overview
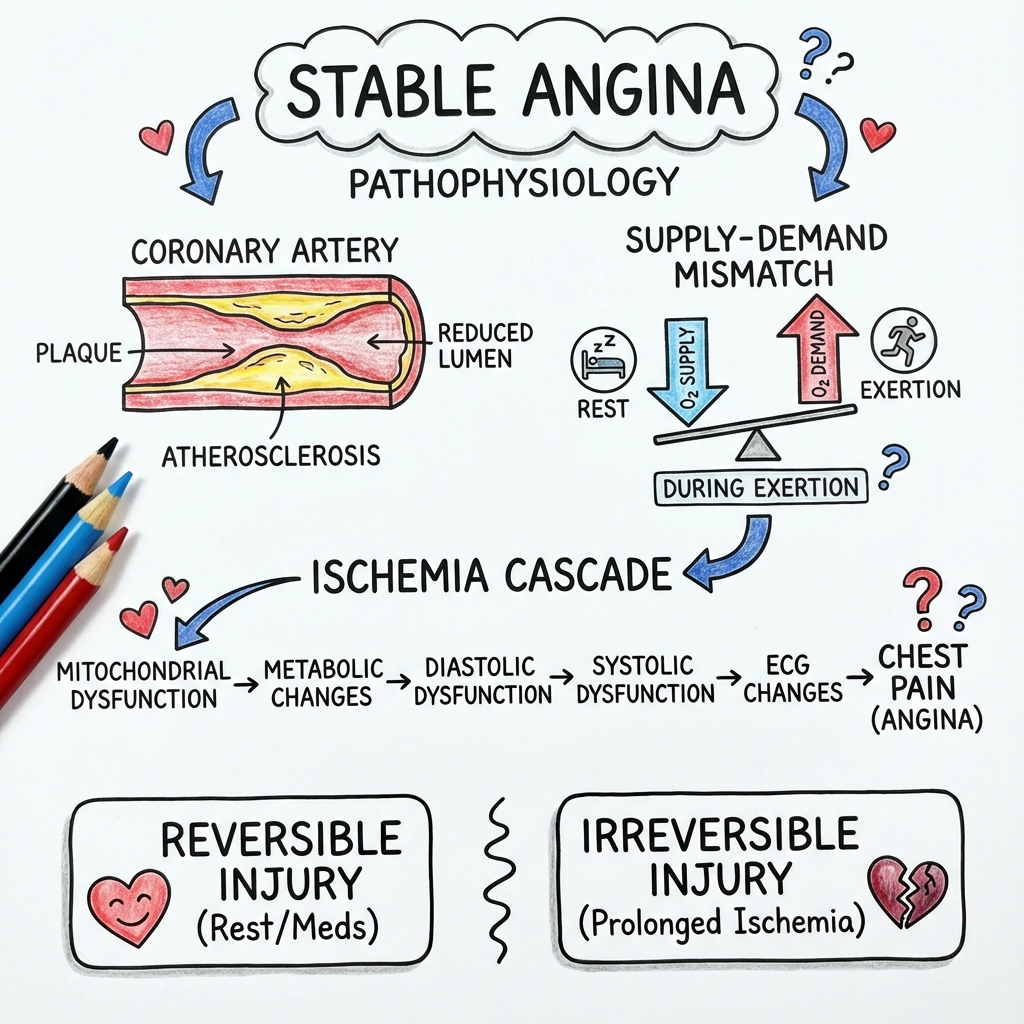
Stable angina, now classified as Chronic Coronary Syndrome (CCS) in contemporary guidelines, is chest pain or discomfort caused by myocardial ischemia resulting from fixed obstructive coronary artery disease (typically > 70% stenosis of an epicardial coronary artery, or > 50% left main stem). [1,2] The condition is characterized by predictable, reproducible symptoms occurring with physical exertion, emotional stress, cold exposure, or after heavy meals, and is relieved by rest or sublingual nitrates within 5-10 minutes. [3]
Stable angina represents the most common initial presentation of coronary artery disease (CAD), affecting 2-4% of the adult population in developed countries. [4] It serves as a critical marker of underlying atherosclerotic cardiovascular disease, carrying a 2-3% annual risk of myocardial infarction or cardiovascular death without appropriate treatment. [5] Early diagnosis and optimal management can reduce this risk by 50% through secondary prevention and, where indicated, revascularization. [6]
The pathophysiology involves a supply-demand mismatch: during exertion, myocardial oxygen demand increases (due to increased heart rate, contractility, and wall tension), but coronary blood flow cannot increase adequately past the fixed stenosis, resulting in relative ischemia, anaerobic metabolism, lactate accumulation, and pain. [7]
Classification
Canadian Cardiovascular Society (CCS) Functional Classification [8]:
| Grade | Limitation | Description | Examples |
|---|---|---|---|
| I | None | Ordinary physical activity does not cause angina | Angina with strenuous, rapid, or prolonged exertion |
| II | Slight | Angina with walking > 2 blocks on level ground or climbing > 1 flight of stairs at normal pace | Walking uphill, cold weather, emotional stress, after meals |
| III | Marked | Angina with walking 1-2 blocks on level ground or climbing 1 flight of stairs | Significantly limited ordinary physical activity |
| IV | Severe | Inability to carry out any physical activity without angina; angina may be present at rest | Angina at rest or with minimal exertion |
Clinical Significance of CCS Classification:
- CCS I-II: Generally managed medically with good quality of life
- CCS III-IV: Consider invasive investigation and revascularization if anatomy suitable
- CCS IV with rest angina: Overlaps with unstable angina/ACS spectrum - requires careful evaluation
By Syndrome Type (ESC 2019 Chronic Coronary Syndrome Classification) [1]:
- Patients with suspected CAD and stable anginal symptoms and/or dyspnea
- Patients with new-onset heart failure or LV dysfunction and suspected CAD
- Asymptomatic and symptomatic patients with stabilized symptoms less than 1 year after ACS or revascularization
- Asymptomatic and symptomatic patients > 1 year after initial diagnosis or revascularization
- Patients with angina and suspected vasospastic or microvascular disease
- Asymptomatic subjects with CAD detected at screening
Microvascular Angina (Cardiac Syndrome X) [74]
Definition: Angina pectoris with normal or near-normal coronary arteries on angiography, due to coronary microvascular dysfunction.
Characteristics:
- More common in women (female:male ratio 3:1)
- Typical exertional angina but normal epicardial coronaries (less than 50% stenosis)
- Positive stress testing (ischemic ECG changes, perfusion defects)
- Impaired coronary flow reserve (CFR less than 2.0 on PET or CMR)
- Prognosis: Generally favorable for survival but significant quality of life impact [75]
Diagnosis:
- Requires exclusion of obstructive CAD (CTCA or ICA)
- Demonstration of ischemia on functional testing
- CFR assessment via PET, CMR stress perfusion, or invasive coronary flow measurements
- Endothelial dysfunction testing (acetylcholine provocation - specialist centers)
Treatment [76]:
- Risk factor modification (as per obstructive CAD)
- Anti-anginal therapy: CCBs (amlodipine), beta-blockers, ranolazine effective
- ACE inhibitors (improve endothelial function)
- Consider statins (pleiotropic endothelial benefits)
- Avoid revascularization (ineffective; no obstructive lesions)
- Cardiac rehabilitation and psychological support
Epidemiology
Prevalence and Incidence:
- Prevalence (UK): 2-4% of adult population; 10-15% in > 65 years age group [4,9]
- Incidence (UK): 20,000-40,000 new cases per year [10]
- Global burden: Ischemic heart disease remains the leading cause of death worldwide [11]
- Healthcare impact: Significant contributor to hospital admissions, medication costs, and disability
Demographics:
- Age: Peak onset 55-75 years; risk increases exponentially with age
- Sex: Male predominance in younger ages (3:1 in less than 65 years), equalizes post-menopause [12]
- Women present later (mean age 70 vs 66 years in men)
- Women more likely to have atypical presentations
- Microvascular angina more common in women
- Ethnicity: South Asian populations have 1.5-2 fold higher risk of CAD [13]
- Higher rates of diabetes, insulin resistance, and adverse lipid profiles
- Earlier age of onset
Risk Factors and Relative Risks [14,15]:
| Risk Factor | Relative Risk (RR) | Population Attributable Risk | Modifiable |
|---|---|---|---|
| Smoking (current) | 2.0-3.0 | 36% | Yes |
| Diabetes Mellitus | 2.5-3.5 | 10% | Partially |
| Hypertension | 2.0-2.5 | 18% | Yes |
| Dyslipidemia (LDL > 4 mmol/L) | 2.5-3.0 | 49% | Yes |
| Family Hx (1st degree less than 55M/less than 65F) | 1.5-2.0 | 14% | No |
| Obesity (BMI > 30) | 1.5-2.0 | 20% | Yes |
| Chronic Kidney Disease | 2.0-3.0 | Variable | Partially |
| Physical Inactivity | 1.5-2.0 | 12% | Yes |
| Psychosocial Factors | 2.0-2.5 | 33% | Partially |
INTERHEART Study: Nine modifiable risk factors account for > 90% of population-attributable risk for MI globally [16]:
- Smoking, dyslipidemia, hypertension, diabetes, abdominal obesity, psychosocial factors, insufficient fruits/vegetables, regular alcohol, physical inactivity
Pathophysiology
Atherosclerosis and Plaque Development
Stages of Atherogenesis [17,18]:
-
Endothelial Dysfunction and Injury
- Causes: Shear stress, hypertension, smoking, hyperglycemia, hyperlipidemia
- Results in increased permeability to LDL and monocytes
- Reduced nitric oxide bioavailability
-
LDL Accumulation and Oxidation
- LDL particles enter intima and undergo oxidation
- Oxidized LDL is pro-inflammatory and cytotoxic
- Triggers inflammatory cascade
-
Foam Cell Formation (Fatty Streak)
- Monocytes differentiate into macrophages in intima
- Macrophages engulf oxidized LDL via scavenger receptors
- Lipid-laden macrophages become "foam cells"
- Earliest visible lesion in atherosclerosis
-
Fibrous Plaque Formation
- Smooth muscle cell migration from media to intima
- Smooth muscle cells produce extracellular matrix (collagen, elastin)
- Formation of fibrous cap overlying lipid core
- Progressive luminal narrowing
-
Plaque Maturation
- Stable plaque: Thick fibrous cap, small lipid core, minimal inflammation
- Vulnerable plaque: Thin fibrous cap (less than 65 μm), large lipid-rich necrotic core, high inflammatory cell content
- Stable plaques cause stable angina; vulnerable plaques cause ACS
Mechanism of Angina (Supply-Demand Mismatch) [7,19]
Determinants of Myocardial Oxygen DEMAND:
| Factor | Mechanism | Clinical Implication |
|---|---|---|
| Heart rate | Increased with exercise, stress | Target with beta-blockers |
| Contractility | Increased with exercise, sympathetic activation | Target with beta-blockers |
| Wall tension (preload) | Increased with volume loading | Target with nitrates, diuretics |
| Afterload | Increased with hypertension | Target with antihypertensives |
Determinants of Myocardial Oxygen SUPPLY:
| Factor | Mechanism | Clinical Implication |
|---|---|---|
| Coronary blood flow | Diastolic duration, coronary perfusion pressure | Heart rate control improves diastolic filling |
| Coronary artery patency | Stenosis limits flow reserve | Revascularization |
| Oxygen content | Hemoglobin, saturation | Treat anemia, hypoxia |
| Coronary vasodilation | Epicardial and microvascular | Nitrates, CCBs |
Ischemic Cascade [20]:
- Reduced coronary blood flow → Subendocardial ischemia (most vulnerable)
- Metabolic changes → Lactate accumulation, ATP depletion
- Diastolic dysfunction → Impaired relaxation
- Systolic dysfunction → Wall motion abnormality
- ECG changes → ST depression, T-wave inversion
- Angina → Pain perception (last to occur)
Clinical Correlation: Patients may have silent ischemia (especially diabetics) with wall motion abnormalities and ECG changes but no pain.
Coronary Anatomy [21]
Left Coronary System:
- Left Main Stem (LMS): 1-2 cm length; supplies 75% of LV in left-dominant, 60% in right-dominant circulation
- Stenosis > 50% is significant (critical)
- "Left main equivalent" = proximal LAD + proximal Circumflex disease
- Left Anterior Descending (LAD): Supplies anterior wall, anterior septum, apex
- Most commonly diseased coronary artery
- Proximal LAD disease is high-risk (large territory at jeopardy)
- Gives off septal perforators and diagonal branches
- Left Circumflex (LCx): Supplies lateral wall, posterior wall in left-dominant systems
- Gives off obtuse marginal branches
Right Coronary System:
- Right Coronary Artery (RCA): Supplies RV, inferior wall, posterior wall in right-dominant systems
- Supplies SA node in 60% and AV node in 90% of patients
- Gives off posterior descending artery (PDA) in right-dominant circulation (85%)
Coronary Dominance:
- Right dominant (85%): RCA gives rise to PDA
- Left dominant (8%): LCx gives rise to PDA
- Co-dominant (7%): Both contribute
Collateral Circulation
- Develops in response to chronic ischemia
- Pre-existing anastomoses enlarge (arteriogenesis)
- Can provide significant blood flow to ischemic territory
- Explains why some patients with severe stenosis have limited symptoms
- Collateral-dependent myocardium may be at risk during revascularization
Clinical Presentation
Symptoms
Typical Angina (Definite Angina) - Must have ALL THREE features [3,22]:
- Constricting discomfort in chest, neck, jaw, shoulder, or arm
- Precipitated by physical exertion
- Relieved by rest or GTN within 5 minutes
Atypical Angina (Probable Angina): Two of the above three features
Non-Anginal Chest Pain: One or none of the above features
Characteristics of Angina:
| Feature | Description | Diagnostic Notes |
|---|---|---|
| Location | Retrosternal, diffuse (hand over chest - Levine's sign) | Pointing with one finger suggests non-cardiac |
| Quality | Pressure, tightness, heaviness, squeezing, constricting | Sharp, stabbing, pleuritic suggests other causes |
| Radiation | Jaw, neck, left arm (inner aspect), between shoulder blades, epigastrium | Radiation increases likelihood of cardiac origin |
| Duration | 2-10 minutes (usually less than 20 minutes) | > 20 min suggests ACS; seconds suggests MSK/neuropathic |
| Triggers | Exertion, cold weather, emotional stress, heavy meals, sexual activity | Predictable triggers support stable angina |
| Relief | Rest (2-5 min), sublingual GTN (1-5 min) | Immediate relief (seconds) suggests non-cardiac; no relief suggests ACS |
Angina Equivalents (Common in elderly, diabetics, women) [23]:
- Exertional dyspnea (most common equivalent)
- Fatigue
- Nausea, indigestion (especially with inferior ischemia)
- Lightheadedness, presyncope
- Diaphoresis
Atypical Presentations More Common In:
- Women (50% present atypically)
- Elderly (> 75 years)
- Diabetics (autonomic neuropathy)
- Post-transplant patients
- Chronic kidney disease
"Do Not Miss"
- Unstable Features (ACS Spectrum) [24]
RED FLAGS - Urgent admission required:
| Feature | Definition | Action |
|---|---|---|
| Rest angina | Angina at rest, usually prolonged > 20 min | Emergency admission for ACS pathway |
| Crescendo angina | Increasing frequency, severity, or duration | Emergency admission |
| New-onset severe angina | CCS III-IV symptoms within past 2 months | Urgent assessment within 72 hours |
| Post-MI angina | Angina occurring within 2 weeks of MI | Emergency admission |
| No response to GTN | Pain not relieved after 3 doses (15 min) | Call 999, give aspirin 300 mg |
Distinguishing Stable from Unstable Angina:
| Feature | Stable Angina | Unstable Angina (ACS) |
|---|---|---|
| Pattern | Predictable, unchanged for weeks/months | New, worsening, or unpredictable |
| Triggers | Consistent exertional threshold | Lower threshold or occurs at rest |
| Duration | less than 20 minutes | Often > 20 minutes |
| Relief | Rest or GTN within 5-10 min | Incomplete or delayed relief |
| Frequency | Stable over time | Increasing frequency |
| Risk | 2-3% annual MACE | 5-15% 30-day MACE |
Variant (Prinzmetal) Angina [25]
Definition: Angina caused by coronary artery vasospasm, occurring at rest (often nocturnal), with transient ST elevation during episodes.
Characteristics:
- Occurs at rest, often between midnight and early morning
- ST elevation during pain (resolves with pain resolution)
- May occur in normal coronaries or superimposed on fixed stenosis
- Associated with smoking, cocaine, hyperventilation
- Episodes may be cyclical
Key Points:
- Avoid beta-blockers (may worsen vasospasm via unopposed alpha-vasoconstriction)
- Treat with calcium channel blockers (first-line) and nitrates
- Risk of arrhythmias during spasm (VT/VF)
History Taking
Essential Questions:
-
Pain Characteristics:
- Where exactly is the pain/discomfort? Point to it.
- What does it feel like? (Quality: pressure, tightness, heaviness)
- How severe is it on a scale of 0-10?
- How long does each episode last?
- Does it spread anywhere? (Radiation)
-
Triggers and Relief:
- What brings it on? (Exertion, cold, meals, stress)
- How much activity triggers it? (Walking distance, stairs - for CCS grading)
- What makes it go away? (Rest, GTN - and how quickly?)
- Does it come on at rest? (RED FLAG)
-
Pattern and Progression:
- How long have you had these symptoms?
- Is the pattern stable or getting worse? (RED FLAG if worsening)
- How often do you get episodes?
-
Associated Symptoms:
- Breathlessness, nausea, sweating, palpitations, lightheadedness?
-
Risk Factor Assessment:
- Smoking history (pack-years, current status)
- Diabetes, hypertension, cholesterol history
- Family history of premature CAD (less than 55 male, less than 65 female first-degree relative)
- Previous vascular disease (stroke, TIA, PVD)
-
GTN Use:
- Do you use GTN spray/tablets?
- How often? How many doses needed?
- Does it work within 5 minutes?
- Any side effects? (Headache common)
-
Functional Status:
- How is this affecting your daily life?
- What activities can you no longer do?
- Work impact?
Physical Examination
During Angina Episode (rarely witnessed):
- Diaphoresis, pallor
- Tachycardia, hypertension (sympathetic activation)
- S4 gallop (LV stiffness)
- Transient mitral regurgitation murmur (papillary muscle ischemia)
Between Episodes:
| Finding | Significance |
|---|---|
| General | |
| Xanthelasma | Hyperlipidemia marker |
| Corneal arcus (less than 50 years) | Hyperlipidemia |
| Tendon xanthomas | Familial hypercholesterolemia |
| Cardiovascular | |
| Blood pressure (both arms) | Hypertension; difference > 20 mmHg suggests aortic dissection/subclavian stenosis |
| Carotid bruits | Systemic atherosclerosis |
| JVP elevation | Heart failure |
| Displaced apex beat | LV dilatation (previous MI, cardiomyopathy) |
| S3 gallop | Heart failure |
| S4 gallop | LVH, diastolic dysfunction |
| Ejection systolic murmur | Aortic stenosis (may cause angina) |
| Peripheral | |
| Absent peripheral pulses | Peripheral vascular disease |
| Femoral bruits | Aortoiliac disease |
| Ankle-brachial index less than 0.9 | Peripheral arterial disease |
| Respiratory | |
| Basal crackles | Pulmonary edema (LV dysfunction) |
Key Point: Examination is often completely normal in stable angina between episodes.
Differential Diagnosis
Cardiac Causes of Chest Pain
| Diagnosis | Features | Differentiators |
|---|---|---|
| Acute Coronary Syndrome | Prolonged (> 20 min), rest pain, crescendo pattern | Emergency; troponin elevation, dynamic ECG changes |
| Aortic Stenosis | Exertional angina, syncope, dyspnea; ejection systolic murmur, slow rising pulse | Can coexist with CAD; echo shows valve pathology |
| Hypertrophic Cardiomyopathy | Exertional symptoms; family history; systolic murmur (increases with Valsalva) | Echo shows asymmetric septal hypertrophy |
| Pericarditis | Sharp, pleuritic, positional (worse lying, better sitting forward); pericardial rub | Diffuse ST elevation, PR depression on ECG |
| Aortic Dissection | Sudden, severe, "tearing" pain radiating to back; BP asymmetry | Emergency CT aorta; hypertensive emergency |
Non-Cardiac Causes of Chest Pain
| Diagnosis | Features | Differentiators |
|---|---|---|
| GERD/Esophageal Spasm | Burning, retrosternal, related to meals, lying flat; may respond to GTN | Esophageal-cardiac reflex; PPI trial; pH study |
| Musculoskeletal | Sharp, localized, reproducible on palpation/movement | Tenderness on examination; movement-related |
| Costochondritis | Anterior chest wall tenderness at costochondral junctions | Reproducible tenderness; no radiation |
| Pulmonary Embolism | Sudden onset, pleuritic, dyspnea; risk factors (immobility, surgery, malignancy) | D-dimer, CTPA |
| Pneumothorax | Sudden onset, pleuritic, dyspnea; reduced breath sounds, hyperresonance | CXR shows pneumothorax |
| Pleuritis/Pneumonia | Pleuritic, cough, fever, productive sputum | CXR consolidation; inflammatory markers |
| Herpes Zoster | Dermatomal distribution; pain precedes rash by days | Vesicular rash in dermatome |
| Anxiety/Panic | Situational, associated with hyperventilation, palpitations, paresthesias | Often atypical features; diagnosis of exclusion |
Esophageal-Cardiac Differentiation Challenge
Both conditions can cause:
- Retrosternal discomfort
- Response to nitrates (esophageal spasm may respond)
- Radiation
Key Differentiators for Cardiac Origin:
- Exertional relationship (strongly suggests cardiac)
- Associated diaphoresis
- Response to rest
- Cardiovascular risk factors
- ECG changes during pain
Diagnostic Approach
Clinical Probability Assessment
Pre-Test Probability (PTP) of obstructive CAD is based on age, sex, and symptom type. [3,26]
Updated ESC 2019 Pre-Test Probabilities (lower than historical Framingham-derived estimates):
| Age (years) | Men - Typical | Men - Atypical | Women - Typical | Women - Atypical |
|---|---|---|---|---|
| 30-39 | 3% | 3% | 2% | 2% |
| 40-49 | 22% | 10% | 6% | 3% |
| 50-59 | 32% | 17% | 10% | 6% |
| 60-69 | 44% | 26% | 13% | 11% |
| 70+ | 52% | 34% | 16% | 13% |
Clinical Likelihood Modifiers (increase probability):
- Known CAD
- Diabetes
- Dyslipidemia
- Hypertension
- Smoking
- Family history
- ST-T changes on resting ECG
- Positive exercise test previously
- Coronary calcification on prior imaging
Probability Categories and Actions [1]:
- Very low PTP (less than 5%): Consider other diagnoses; non-invasive testing rarely indicated
- Low PTP (5-15%): Consider calcium scoring or CTCA
- Intermediate PTP (15-85%): Non-invasive testing indicated (CTCA preferred)
- High PTP (> 85%): Invasive coronary angiography may be appropriate
Investigations
Bedside Tests
12-Lead ECG [27]:
| Finding | Significance |
|---|---|
| Normal (50% of stable angina) | Does not exclude CAD |
| Q waves | Prior MI |
| ST depression | Ischemia (if during pain) or strain pattern |
| T-wave inversion | Ischemia or previous ischemic insult |
| LVH pattern | Suggests hypertensive heart disease |
| LBBB | May indicate prior MI; limits stress test interpretation |
| Atrial fibrillation | Common comorbidity; increases stroke risk |
During Angina Episode:
- ST depression ≥1 mm (horizontal or downsloping) = significant ischemia
- ST elevation = severe transmural ischemia or vasospasm
Laboratory Investigations
| Test | Purpose | Notes |
|---|---|---|
| Full Blood Count | Anemia (reduces O2 delivery) | Treat if Hb less than 100 g/L |
| Lipid Profile | Cardiovascular risk; treatment target | Total cholesterol, LDL, HDL, triglycerides; LDL target less than 1.4-1.8 mmol/L |
| HbA1c / Fasting glucose | Diabetes screening | Diabetes is CAD equivalent |
| U&E | Baseline for ACEi, contrast agents | eGFR for contrast risk stratification |
| Liver Function Tests | Baseline for statin therapy | Check pre-statin and 3 months after |
| Thyroid Function | Hyperthyroidism can worsen/cause angina | Hypothyroidism affects lipids |
| hsTroponin | Rule out ACS if clinical concern | Should be negative in stable angina |
| BNP/NT-proBNP | Heart failure assessment | Elevated if LV dysfunction |
Coronary Artery Calcium Score (CACS) [28]
When to Use:
- Low to intermediate PTP (5-15%)
- Uncertainty about need for further testing
- Asymptomatic individuals for risk stratification
Interpretation:
| Score | Interpretation | Implications |
|---|---|---|
| 0 | No identite | Very low probability of obstructive CAD; consider alternative diagnosis |
| 1-99 | Mild calcification | Low-moderate risk; consider further testing if symptoms typical |
| 100-399 | Moderate calcification | Indicates significant CAD; further testing warranted |
| ≥400 | Extensive calcification | High probability of obstructive CAD; proceed to CTCA or ICA |
Limitations: Does not detect non-calcified ("soft") plaque; may be falsely low in younger patients or acute presentations.
CT Coronary Angiography (CTCA) [29,30]
NICE Recommendation (NG95): CTCA is first-line anatomical test for patients with chest pain of recent onset where CAD cannot be excluded by clinical assessment alone.
| Parameter | Details |
|---|---|
| Indications | Suspected stable angina, intermediate PTP (15-85%) |
| Sensitivity | 95-99% for > 50% stenosis |
| Specificity | 85-90% |
| NPV | 99% (excellent for ruling out significant CAD) |
| PPV | 60-70% (may overestimate stenosis severity) |
Advantages:
- Non-invasive
- Excellent negative predictive value (rules out CAD effectively)
- Visualizes plaque morphology and coronary anatomy
- Fast acquisition (~5 seconds)
- Can identify non-coronary causes of chest pain
Limitations:
- Requires heart rate control (beta-blocker often given if HR > 60)
- Contrast exposure
- Radiation exposure (3-5 mSv with modern scanners)
- Reduced accuracy with extensive calcification, arrhythmias, high BMI
- Cannot assess functional significance of intermediate stenoses (50-70%)
Post-CTCA Decision:
- No/mild CAD (less than 50%): Reassure, secondary prevention
- Moderate stenosis (50-70%): Functional testing (stress imaging) or FFR-CT
- Severe stenosis (> 70%): Invasive angiography for revascularization planning
FFR-CT (CT-Derived Fractional Flow Reserve) [77,78]:
- Non-invasive functional assessment derived from CTCA datasets using computational fluid dynamics
- FFR-CT ≤0.80: Hemodynamically significant stenosis
- FFR-CT > 0.80: Non-significant stenosis; optimal medical therapy
- Advantages: No additional imaging, no adenosine, no radiation beyond CTCA
- Evidence: PLATFORM, ADVANCE trials show reduced unnecessary ICA, cost-effective
- Increasingly integrated into CTCA reporting workflows
Functional (Stress) Testing
Principles: Detect myocardial ischemia by increasing myocardial oxygen demand (exercise or pharmacological stress) and detecting ischemia via ECG, imaging (perfusion or wall motion), or symptoms. [31]
Exercise Tolerance Test (ETT) / Exercise ECG [32]:
| Parameter | Details |
|---|---|
| Protocol | Bruce protocol (most common); incrementing speed and gradient every 3 min |
| Positive test | ≥1 mm horizontal/downsloping ST depression, angina, arrhythmias, fall in BP |
| Sensitivity | 45-68% (lower than imaging modalities) |
| Specificity | 70-77% |
Indications:
- Assessment of exercise capacity
- Symptom-exercise correlation
- Post-revascularization assessment
Contraindications:
- Recent MI (less than 48 hours)
- Unstable angina
- Severe symptomatic aortic stenosis
- Acute myocarditis/pericarditis
- Acute PE or aortic dissection
- Uncontrolled arrhythmias
- Inability to exercise
Duke Treadmill Score (DTS) [33]:
- Formula: Exercise time (min) - (5 × ST deviation in mm) - (4 × angina index)
- "Angina index: 0 = no angina; 1 = non-limiting angina; 2 = exercise-limiting angina"
- Low risk (≥5): 0.25% annual mortality
- Moderate risk (-10 to +4): 1.25% annual mortality
- High risk (≤-11): 5.25% annual mortality
Stress Echocardiography [34]:
| Parameter | Details |
|---|---|
| Stress methods | Exercise (treadmill, bicycle) or pharmacological (dobutamine) |
| Interpretation | Inducible regional wall motion abnormality = ischemia |
| Sensitivity | 80-85% |
| Specificity | 85-90% |
Advantages: No radiation, assesses LV function, valvular disease
Myocardial Perfusion Imaging (MPI / SPECT) [35]:
| Parameter | Details |
|---|---|
| Tracers | Technetium-99m (sestamibi/tetrofosmin) or Thallium-201 |
| Stress methods | Exercise or pharmacological (adenosine, regadenoson, dipyridamole, dobutamine) |
| Interpretation | Reversible perfusion defect = ischemia; fixed defect = infarction/scar |
| Sensitivity | 85-90% |
| Specificity | 70-80% |
Advantages: High sensitivity, semi-quantitative ischemia assessment, viability assessment
Cardiac MRI (CMR) Stress Perfusion [36]:
| Parameter | Details |
|---|---|
| Stress agent | Adenosine or regadenoson |
| Interpretation | Inducible perfusion defect on first-pass imaging = ischemia |
| Sensitivity | 89-91% |
| Specificity | 80-85% |
Advantages: No radiation, excellent spatial resolution, assesses viability (late gadolinium enhancement)
PET Perfusion Imaging [37]:
- Highest diagnostic accuracy among functional tests
- Allows absolute myocardial blood flow quantification
- Limited availability, expensive
- Used for microvascular disease assessment
Invasive Coronary Angiography (ICA) [38]
Gold Standard for coronary anatomy assessment and definitive diagnosis.
Indications:
- High clinical probability of CAD with refractory symptoms
- High-risk features on non-invasive testing
- Inconclusive non-invasive testing
- Consideration of revascularization
- Severe stenosis on CTCA
- Post-STEMI/NSTEMI
Key Outputs:
- Number and location of diseased vessels
- Severity of stenoses (% diameter stenosis)
- LV function (LV gram)
- Planning for revascularization (PCI vs CABG)
Limitations:
- Invasive procedure (vascular access, contrast, radiation)
- Angiographic severity does not always correlate with functional significance
- Complications: Bleeding, vascular injury, stroke, MI, death (overall major complication rate less than 1%)
Fractional Flow Reserve (FFR) and Instantaneous Wave-Free Ratio (iFR) [39,40]
Purpose: Assess functional significance of intermediate coronary stenoses (40-70% on angiography).
FFR:
- Measured during maximum hyperemia (adenosine infusion)
- Ratio of distal coronary pressure to aortic pressure
- FFR ≤0.80: Functionally significant → benefits from revascularization
- FFR > 0.80: Not significant → optimal medical therapy
iFR:
- Measured during the wave-free period of diastole (no adenosine needed)
- iFR ≤0.89: Functionally significant
- iFR > 0.89: Not significant
Evidence (FAME, FAME 2, iFR-SWEDEHEART, DEFINE-FLAIR):
- FFR/iFR-guided PCI improves outcomes compared to angiography-guided PCI
- FAME 2: FFR-guided PCI reduced urgent revascularization compared to medical therapy alone
Treatment
Principles of Management
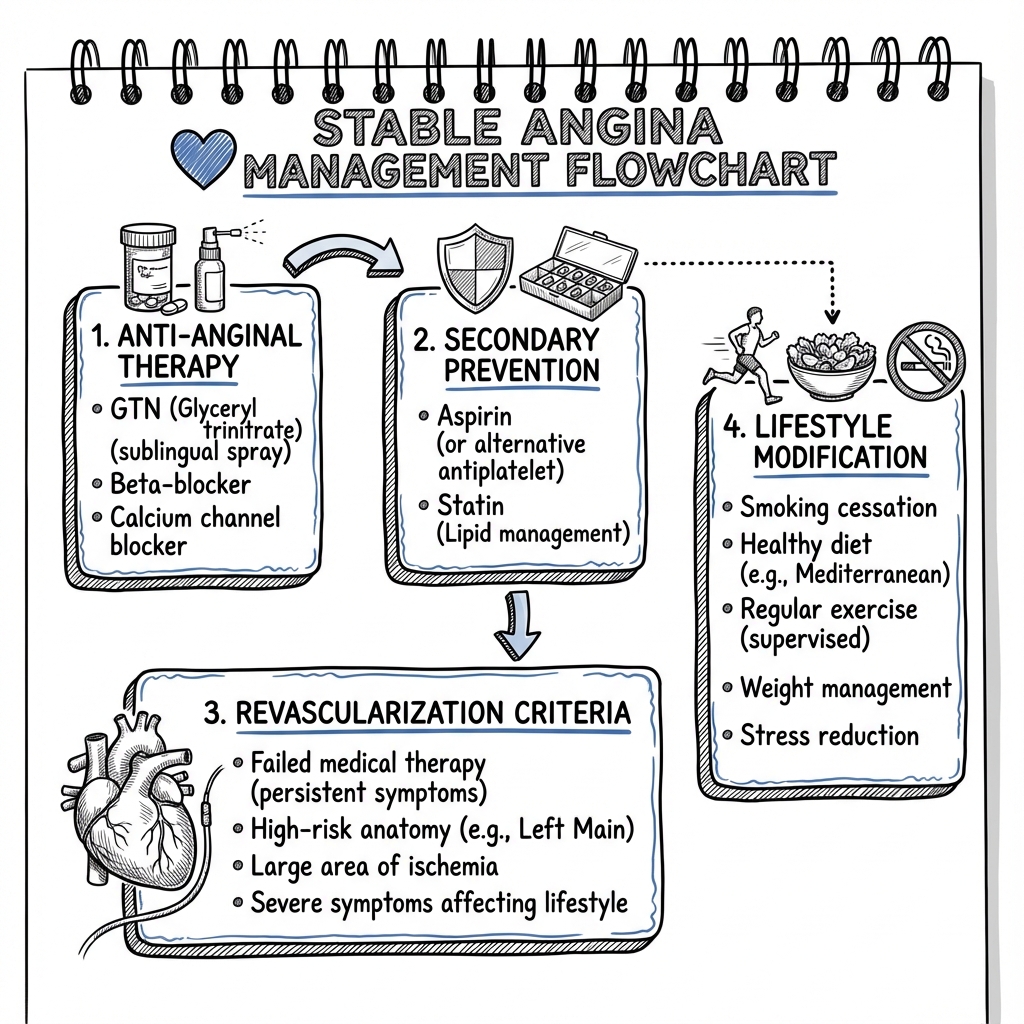
Stable angina management is multimodal, targeting: [1,41]
- Symptom Relief: Anti-anginal therapy to reduce angina frequency and improve quality of life
- Secondary Prevention: Disease-modifying therapy to reduce cardiovascular events (MI, stroke, death)
- Lifestyle Modification: Risk factor control through behavioral changes
- Revascularization: When indicated for refractory symptoms or high-risk anatomy
Treatment Goals:
- Abolish or reduce angina to CCS I-II
- Reduce frequency of GTN use
- Improve exercise capacity and quality of life
- Reduce cardiovascular morbidity and mortality
- Prevent progression to ACS
Medical Management
Anti-Anginal Therapy (Symptom Relief) [42,43]
First-Line Agents (Choose ONE):
1. Beta-Blockers (First-Line Preferred) [44,45]:
| Drug | Starting Dose | Titrate To | Notes |
|---|---|---|---|
| Bisoprolol | 2.5-5 mg OD | 10 mg OD | Cardioselective, once daily |
| Metoprolol | 25-50 mg BD | 100 mg BD | Cardioselective |
| Atenolol | 25-50 mg OD | 100 mg OD | Cardioselective, once daily |
| Carvedilol | 3.125 mg BD | 25 mg BD | Non-selective, alpha-blocking; preferred in HF |
| Nebivolol | 2.5 mg OD | 10 mg OD | Cardioselective, vasodilatory |
Mechanism: Reduce heart rate (negative chronotropy), contractility (negative inotropy), and blood pressure → decreased myocardial oxygen demand.
Target: Resting HR 55-60 bpm.
Contraindications: Asthma (severe/uncontrolled), acute decompensated heart failure, severe bradycardia (less than 50 bpm), second/third-degree AV block, sick sinus syndrome (without pacemaker), severe hypotension.
Side Effects: Bradycardia, fatigue, cold extremities, erectile dysfunction, depression, bronchospasm, masking of hypoglycemia.
2. Calcium Channel Blockers (Alternative First-Line) [46]:
Rate-Limiting CCBs (Non-Dihydropyridines) - use if beta-blocker contraindicated:
| Drug | Starting Dose | Titrate To | Notes |
|---|---|---|---|
| Diltiazem MR | 120 mg OD | 360 mg OD | Rate-limiting |
| Verapamil | 80 mg TDS | 120 mg TDS | Rate-limiting; avoid in HF |
Contraindications: Heart failure with reduced EF (negative inotropy), second/third-degree AV block, severe bradycardia, hypotension. Do NOT combine with beta-blockers (risk of severe bradycardia/heart block).
Dihydropyridine CCBs - use in combination with beta-blockers:
| Drug | Starting Dose | Titrate To | Notes |
|---|---|---|---|
| Amlodipine | 5 mg OD | 10 mg OD | Vasodilatory; can combine with BB |
| Nifedipine MR | 30 mg OD | 90 mg OD | Vasodilatory; avoid short-acting |
| Felodipine | 5 mg OD | 10 mg OD | Vasodilatory |
Mechanism: Coronary and peripheral vasodilation (DHP); reduce heart rate and contractility (non-DHP).
Side Effects: Peripheral edema (ankle swelling, especially amlodipine), flushing, headache, constipation (verapamil), bradycardia (non-DHP).
Add-On/Second-Line Anti-Anginals (if monotherapy insufficient):
3. Long-Acting Nitrates [47]:
| Drug | Dose | Notes |
|---|---|---|
| Isosorbide mononitrate | 30-120 mg OD (extended-release) | Once daily, preferably morning |
| Isosorbide dinitrate | 20-40 mg BD-TDS | Need nitrate-free interval |
Mechanism: Venodilation → reduced preload → reduced LV wall tension and O2 demand; some coronary vasodilation.
CRITICAL: Nitrate-free interval (10-14 hours) essential to prevent tolerance (typically overnight).
Side Effects: Headache (common initially, often improves), flushing, hypotension, dizziness, tolerance.
Contraindication: Concurrent use of PDE5 inhibitors (sildenafil, tadalafil, vardenafil) - severe hypotension risk; severe aortic stenosis.
4. Nicorandil [48]:
| Dose | Mechanism | Notes |
|---|---|---|
| 10-30 mg BD | K-ATP channel opener + nitrate-like action | Arterial AND venous dilation |
Evidence: IONA trial showed reduced cardiovascular events in stable angina.
Side Effects: Headache, flushing, GI ulceration (rare but serious - oral, GI, anal ulcers), dizziness.
Contraindication: Concurrent PDE5 inhibitors.
5. Ivabradine [49]:
| Dose | Mechanism | Notes |
|---|---|---|
| 5 mg BD → 7.5 mg BD | Selective If channel inhibitor (sinus node) | Pure HR reduction without negative inotropy |
Indications:
- Beta-blocker intolerant/contraindicated AND sinus rhythm AND HR > 70 bpm
- Add-on to beta-blocker if HR remains > 70 bpm
Contraindications: Atrial fibrillation (only works in sinus rhythm), severe bradycardia (less than 60 bpm pre-treatment), sick sinus syndrome, SA/AV block, acute MI, cardiogenic shock, concurrent strong CYP3A4 inhibitors.
Side Effects: Visual disturbances (phosphenes - transient brightness), bradycardia, AF, headache.
6. Ranolazine [50]:
| Dose | Mechanism | Notes |
|---|---|---|
| 375-750 mg BD | Inhibits late sodium current → improves diastolic relaxation | No hemodynamic effects (HR, BP) |
Indications: Refractory angina as add-on therapy when other agents inadequate or contraindicated.
Contraindications: Severe hepatic impairment, concurrent potent CYP3A4 inhibitors, QT prolongation.
Side Effects: Dizziness, nausea, constipation, QT prolongation.
GTN (Glyceryl Trinitrate) - Acute Symptom Reliever [51]:
| Formulation | Dose | Onset | Duration |
|---|---|---|---|
| Sublingual spray | 400 mcg (1-2 sprays) | 1-2 min | 20-30 min |
| Sublingual tablets | 300-600 mcg | 1-2 min | 20-30 min |
Instructions:
- Use at first sign of angina OR prophylactically before exertion
- Sit down before using (hypotension risk)
- One spray/tablet, wait 5 minutes; repeat up to 3 times
- If no relief after 3 doses (15 minutes) → CALL 999 (ambulance) - suspect ACS
- Common side effects: Headache, flushing, dizziness
Practical Points:
- Replace spray/tablets every 8 weeks (GTN degrades)
- Avoid within 24 hours of sildenafil/vardenafil; 48 hours of tadalafil
Secondary Prevention (Disease-Modifying Therapy) [52,53]
ALL patients with stable angina/CAD require:
1. Antiplatelet Therapy:
| Drug | Dose | Evidence | Notes |
|---|---|---|---|
| Aspirin | 75 mg OD (lifelong) | 22% relative risk reduction in vascular events | First-line; irreversible COX-1 inhibition |
| Clopidogrel | 75 mg OD | Alternative if aspirin intolerant | ADP receptor inhibitor |
Post-PCI: DAPT (Aspirin + P2Y12 inhibitor) for 6-12 months typically [54].
2. High-Intensity Statin Therapy [55]:
| Drug | Dose | LDL Target | Notes |
|---|---|---|---|
| Atorvastatin | 80 mg ON | less than 1.4 mmol/L (or > 50% reduction) | High-intensity statin |
| Rosuvastatin | 20-40 mg ON | less than 1.4 mmol/L (or > 50% reduction) | High-intensity statin |
Evidence: 4S, LIPID, HPS, PROVE-IT TIMI 22 trials - statins reduce MI, stroke, cardiovascular death by 30-40% [56].
ESC 2019 Target: LDL less than 1.4 mmol/L AND ≥50% reduction from baseline for very high-risk patients (established CAD).
Monitoring: Check lipids at 8-12 weeks after starting/changing dose; LFTs at baseline, 8-12 weeks, then annually.
3. ACE Inhibitors [57]:
| Drug | Starting Dose | Target Dose | Notes |
|---|---|---|---|
| Ramipril | 2.5 mg OD | 10 mg OD | HOPE trial evidence |
| Perindopril | 2 mg OD | 8 mg OD | EUROPA trial evidence |
| Lisinopril | 5 mg OD | 20 mg OD | Alternative |
Indications (consider for all CAD patients; mandatory if):
- Diabetes mellitus
- Chronic kidney disease (albuminuria)
- LV systolic dysfunction (EF less than 40%)
- Hypertension
- Post-MI
Evidence: HOPE trial (ramipril) and EUROPA trial (perindopril) showed 20-25% relative risk reduction in cardiovascular events in CAD patients [58,59].
ARBs: Use if ACE inhibitor intolerant (cough, angioedema).
4. Blood Pressure Control:
- Target: less than 130/80 mmHg (if tolerated) for most patients with CAD [60]
- First-line: ACE inhibitor/ARB + CCB (amlodipine) ± thiazide
5. Glycemic Control (Diabetics):
- Target HbA1 c: less than 53 mmol/mol (7%) for most; individualize
- Consider SGLT2 inhibitors or GLP-1 agonists (cardiovascular benefit) [61]
Lifestyle Modification [62]
Critical for all patients - address at every consultation:
| Intervention | Recommendation | Evidence |
|---|---|---|
| Smoking cessation | Complete cessation; offer pharmacotherapy (NRT, varenicline, bupropion) | Single most effective intervention; 50% risk reduction within 1 year |
| Diet | Mediterranean diet: Olive oil, fish, vegetables, whole grains, nuts | PREDIMED trial: 30% CV event reduction |
| Physical activity | 150 min/week moderate or 75 min/week vigorous aerobic exercise | Cardiac rehabilitation referral |
| Weight management | BMI target 20-25 kg/m² | Reduces BP, lipids, diabetes risk |
| Alcohol | Limit to ≤14 units/week, spread across week | Avoid binge drinking |
| Cardiac rehabilitation | Structured exercise program; education; psychological support | 20-25% mortality reduction |
Cardiac Rehabilitation:
- All stable angina patients should be offered cardiac rehabilitation
- Components: Supervised exercise, education, dietary advice, psychological support, smoking cessation
- Mortality benefit: 20-25% reduction [63]
Revascularization [64,65]
Indications for Invasive Angiography and Revascularization:
- Refractory symptoms (CCS III-IV) despite optimal medical therapy
- High-risk anatomy identified on non-invasive testing
- Large area of ischemia (> 10% of LV myocardium) on functional testing
- LV systolic dysfunction attributable to ischemia
- Prognostic benefit (specific anatomical subsets)
PCI (Percutaneous Coronary Intervention) [66]
Technique: Balloon angioplasty + drug-eluting stent (DES) deployment via catheter.
Indications:
- 1-2 vessel disease without proximal LAD involvement
- Low-intermediate SYNTAX score (≤22)
- Patient preference for less invasive approach
- High surgical risk
Outcomes:
- Procedural success: > 95%
- In-hospital mortality: less than 1%
- Target lesion revascularization (DES): 5-10% at 5 years
Post-PCI Antiplatelet Therapy [54]:
| Duration | Regimen | Notes |
|---|---|---|
| Standard (12 months) | Aspirin 75 mg + Clopidogrel 75 mg OR Ticagrelor 90 mg BD | Chronic coronary syndrome after elective PCI |
| Short DAPT (1-3 months) | Consider if high bleeding risk | STOPDAPT-2, TWILIGHT trials |
| Extended (> 12 months) | Consider if high ischemic risk, low bleeding risk | PEGASUS-TIMI 54 |
CABG (Coronary Artery Bypass Grafting) [67]
Technique: Surgical bypass using arterial (LIMA, RIMA, radial) or venous (SVG) conduits.
Indications for CABG over PCI:
- Left main stem disease (> 50% stenosis)
- Three-vessel disease, especially with:
- Diabetes mellitus
- Reduced LV function (EF less than 50%)
- High SYNTAX score (> 32)
- Complex lesions (bifurcation, calcification, chronic total occlusion)
- Two-vessel disease with proximal LAD involvement
SYNTAX Score [68]:
- Anatomical complexity scoring system based on angiographic features
- Low (0-22): PCI or CABG similar outcomes
- Intermediate (23-32): Case-by-case; Heart Team discussion
- High (> 32): CABG preferred
Evidence (SYNTAX, FREEDOM, EXCEL, NOBLE trials):
- 3-vessel/left main disease: CABG superior long-term outcomes (lower MACE, repeat revascularization)
- FREEDOM trial: CABG superior to PCI in diabetics with multivessel disease [69]
Conduit Patency:
- LIMA to LAD: 95% patency at 10 years
- SVG: 50-60% patency at 10 years
Perioperative Risks:
- Mortality: 1-3%
- Stroke: 1-2%
- MI: 2-5%
- Atrial fibrillation: 25-30%
- Wound infection: 2-5%
COURAGE and ISCHEMIA Trials - Key Evidence [70,71]
COURAGE Trial (2007):
- Question: PCI + OMT vs OMT alone in stable CAD?
- Result: No difference in death or MI at 4.6 years
- Conclusion: PCI provides symptom relief but does not reduce mortality/MI over OMT in stable CAD
ISCHEMIA Trial (2020):
- Question: Invasive strategy (angiography ± revascularization) vs conservative (OMT alone) in stable ischemic heart disease with moderate-severe ischemia?
- Result: No difference in CV death, MI, hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest at 3.2 years
- Conclusion: Initial conservative strategy reasonable; revascularization reserved for refractory symptoms or high-risk anatomy
Clinical Implications:
- Revascularization in stable CAD is primarily for symptom relief
- All patients require optimal medical therapy regardless of revascularization status
- Reserve revascularization for refractory symptoms or prognostic indications (left main, severe 3VD)
Complications
Progression of Disease
| Complication | Annual Risk (Untreated) | Mechanism |
|---|---|---|
| Myocardial Infarction | 2-3% | Plaque rupture, thrombosis |
| Progression to Unstable Angina | 5-10% | Plaque instability |
| Heart Failure | Variable | Chronic ischemia → hibernating myocardium → LV dysfunction |
| Arrhythmias | Variable | Ischemia-induced VT/VF, AF |
| Sudden Cardiac Death | 0.5-1% | Malignant arrhythmias |
Treatment-Related Complications
Medication Side Effects:
| Drug Class | Common Side Effects | Serious Adverse Effects |
|---|---|---|
| Beta-blockers | Fatigue, cold extremities, ED | Severe bradycardia, bronchospasm, heart block |
| CCBs | Ankle edema, flushing | Heart block (non-DHP), worsening HF |
| Nitrates | Headache, hypotension | Tolerance, severe hypotension with PDE5i |
| Aspirin | Dyspepsia, bruising | GI bleeding, hypersensitivity |
| Statins | Myalgia | Rhabdomyolysis (rare), hepatotoxicity |
| ACE inhibitors | Dry cough, hyperkalemia | Angioedema, acute kidney injury |
PCI Complications:
| Complication | Incidence | Management |
|---|---|---|
| Access site bleeding | 2-5% | Compression, transfusion if severe |
| Contrast nephropathy | 5-10% (high risk) | Hydration, limit contrast volume |
| Stent thrombosis | 1-2% (with DAPT) | Emergency PCI; ensure DAPT compliance |
| Coronary dissection | less than 1% | May require additional stenting or CABG |
| Stroke | 0.1-0.2% | Supportive care |
CABG Complications:
| Complication | Incidence | Notes |
|---|---|---|
| Atrial fibrillation | 25-30% | Usually transient; anticoagulation if persistent |
| Stroke | 1-2% | Risk increases with age, aortic atherosclerosis |
| Sternal wound infection | 2-5% | Higher with diabetes, obesity |
| Graft occlusion | Variable | LIMA superior patency vs SVG |
| Cognitive decline | Common | Often temporary ("pump head") |
Prognosis
Natural History and Outcomes [72,73]
Stable Angina (All-Comers):
- Annual mortality: 1-2%
- Annual MI rate: 2-3%
- 5-year survival: 85-90%
By Anatomical Severity:
| Disease Extent | Annual Mortality (Medical Rx) |
|---|---|
| 1-vessel disease | 1.5% |
| 2-vessel disease | 2.5% |
| 3-vessel disease | 3-5% |
| Left main disease | 7-10% |
Prognostic Factors (Poor Prognosis):
- Left main stem disease
- Proximal LAD disease
- Three-vessel disease
- LV systolic dysfunction (EF less than 40%)
- Large area of ischemia (> 10% LV)
- Diabetes mellitus
- Advanced age (> 75 years)
- CKD
- Prior MI
- Poor exercise tolerance (Duke score ≤-11)
Response to Treatment
Symptom Control:
- Optimal medical therapy: 70-80% achieve CCS I-II
- PCI: 85-90% symptom improvement at 1 year
- CABG: 90-95% symptom-free at 1-5 years
Secondary Prevention Impact:
- Statins: 30-40% reduction in cardiovascular events
- Aspirin: 22% reduction in vascular events
- ACE inhibitors: 20-25% reduction (HOPE, EUROPA)
- Smoking cessation: 50% risk reduction
Contemporary Outcomes (2020-2024 Data) [79,80]:
- Modern OMT (aspirin, high-intensity statin, ACEi, beta-blocker) reduces 5-year MACE by 45-50%
- Drug-eluting stent technology: Target lesion failure less than 5% at 5 years
- Contemporary CABG (LIMA + arterial grafts): 10-year survival 85-90% in low-risk patients
- All-cause mortality stable angina (OMT era): 0.8-1.2% per year in contemporary cohorts
Patient Education
Condition Explanation
"You have angina, which is chest pain caused by narrowed arteries to your heart. The narrowing is due to a buildup of fatty deposits (atherosclerosis). When you exercise or exert yourself, your heart needs more oxygen, but the narrowed arteries can't deliver enough blood flow to meet that demand. This causes the chest pain or discomfort you experience."
"Angina is a warning sign that your heart arteries are narrowed, but the good news is that we can treat it effectively with medications that both relieve your symptoms and reduce your risk of having a heart attack in the future."
Medication Guidance
"We treat angina with two types of medication:
- Symptom relief (like beta-blockers or calcium channel blockers to prevent pain, and GTN spray for immediate relief)
- Heart protection (aspirin to thin your blood, statins to lower cholesterol, and sometimes blood pressure tablets) - these reduce your risk of heart attacks and strokes by 30-40%"
"It's very important to take your heart protection medications every day, even when you feel well. These are the medications that save lives."
GTN Spray Instructions
"Keep your GTN spray with you at all times. Use it at the first sign of chest pain:
- Sit down before using it (it can make you feel lightheaded)
- Spray once or twice under your tongue
- Wait 5 minutes - the pain should improve
- If not better, spray again (up to 3 times total, 5 minutes apart)
- If pain persists after 3 doses (15 minutes), call 999 immediately - this could be a heart attack"
"You can also use GTN spray before activities you know cause angina (like climbing stairs or walking uphill)."
When to Seek Emergency Care
Call 999 immediately if:
- Chest pain lasting more than 15 minutes
- Chest pain not relieved by 3 doses of GTN
- Chest pain occurring at rest (not during activity)
- Pain more severe than usual
- Feeling very unwell - sweaty, nauseous, breathless
- Pain spreading to jaw, arm, or back
Lifestyle Advice
"There are important changes you can make that will significantly reduce your risk:
- Stop smoking - this is the single most important thing you can do
- Eat a Mediterranean diet - more fish, olive oil, vegetables, less processed food
- Stay active - aim for 30 minutes of moderate activity most days; we'll refer you to cardiac rehabilitation
- Maintain a healthy weight
- Limit alcohol - no more than 14 units per week"
Quality Metrics
Performance Indicators
| Metric | Target | Rationale |
|---|---|---|
| Documentation of CCS class | 100% | Standardized severity assessment |
| Aspirin prescribed (or documented contraindication) | > 95% | Evidence-based secondary prevention |
| Statin prescribed (high-intensity) | > 95% | Evidence-based secondary prevention |
| ACE inhibitor considered | > 90% | Cardioprotection in eligible patients |
| Smoking status documented | 100% | Enables cessation intervention |
| Smoking cessation advice given | 100% (smokers) | Most effective lifestyle intervention |
| Cardiac rehabilitation referral | > 80% | Proven mortality benefit |
| GTN prescribed with instructions | 100% | Acute symptom management |
| Red flags/unstable features assessed | 100% | Safety: exclude ACS |
Key Clinical Pearls
Diagnostic Pearls
- Typical angina has 3 features: Retrosternal constricting discomfort + exertion-related + relieved by rest/GTN within 5 min
- 50% of stable angina patients have normal resting ECG: Do not rely on ECG to diagnose or exclude angina
- CTCA is first-line investigation (NICE NG95): Not exercise stress testing
- Functional significance matters more than angiographic appearance: Use FFR/iFR for intermediate stenoses (40-70%)
- Atypical presentations are common in women, diabetics, elderly: Maintain high clinical suspicion
Treatment Pearls
- Beta-blockers are first-line anti-anginal: Target HR 55-60 bpm
- Nitrate-free interval essential: Prevents tolerance (10-14 hours overnight)
- Don't combine verapamil/diltiazem with beta-blockers: Risk of severe bradycardia/heart block
- All patients need secondary prevention: Aspirin + statin + consider ACEi - even if asymptomatic on anti-anginals
- COURAGE and ISCHEMIA trials: Revascularization doesn't reduce mortality in stable CAD vs OMT; reserve for symptoms or high-risk anatomy
Revascularization Pearls
- SYNTAX score guides PCI vs CABG: High score (> 32) favors CABG
- CABG superior in diabetics with multivessel disease: FREEDOM trial
- LIMA to LAD is gold standard conduit: 95% patency at 10 years
- Post-PCI DAPT typically 6-12 months: Balance ischemic and bleeding risk
Red Flag Pearls
- Rest pain, crescendo pattern, new-onset severe = unstable angina (ACS): Emergency admission
- No response to 3 GTN doses = call 999: Suspect MI
- Angina with syncope suggests aortic stenosis: Listen for murmur; arrange echo
- Sudden severe "tearing" chest pain = aortic dissection: CT aorta
Viva Questions
Common Viva Questions
-
"Differentiate stable angina from unstable angina."
- Stable: Predictable, exertional, consistent pattern, relieved by rest/GTN in 5-10 min
- Unstable: Rest pain, crescendo, new-onset severe (less than 2 months), prolonged (> 20 min), incomplete relief = ACS spectrum requiring emergency admission
-
"What is the first-line investigation for suspected stable angina?"
- CTCA per NICE NG95 guidelines
- High sensitivity (95-99%) and excellent NPV (99%) for ruling out significant CAD
-
"Describe the medical management of stable angina."
- Anti-anginal (symptom relief): BB (first-line) or CCB; add long-acting nitrate, nicorandil, ivabradine if needed; GTN PRN
- Secondary prevention: Aspirin 75 mg, high-intensity statin (atorvastatin 80 mg), ACEi (ramipril 10 mg) if indicated
-
"What are the indications for CABG over PCI?"
- Left main stem disease (> 50% stenosis)
- Three-vessel disease, especially with diabetes, reduced EF, high SYNTAX score (> 32)
- Two-vessel disease with proximal LAD involvement
- Complex lesions not suitable for PCI
-
"What did the COURAGE and ISCHEMIA trials show?"
- PCI + OMT does not reduce death or MI compared to OMT alone in stable CAD
- Revascularization provides symptom relief but not prognostic benefit in stable disease
- Initial conservative strategy is reasonable; reserve revascularization for refractory symptoms or high-risk anatomy
-
"What is the CCS classification of angina?"
- CCS I: Angina only with strenuous exertion
- CCS II: Angina with walking > 2 blocks or > 1 flight stairs
- CCS III: Angina with walking 1-2 blocks or 1 flight stairs
- CCS IV: Angina at rest or with any activity
-
"What is FFR and when is it used?"
- Fractional Flow Reserve: Ratio of distal coronary pressure to aortic pressure during maximal hyperemia
- Used to assess functional significance of intermediate stenoses (40-70%)
- FFR ≤0.80 indicates hemodynamically significant stenosis warranting revascularization
Future Directions
- Coronary Computed Tomography Angiography-derived FFR (FFR-CT): Non-invasive functional assessment
- Novel Anti-Anginal Agents: New targets for refractory angina
- CGRP Antagonists: Exploring cardiovascular applications
- Gene Therapy and Regenerative Medicine: Therapeutic angiogenesis for refractory angina
- Precision Medicine: Genetic risk scoring and personalized therapy
- AI-Assisted Diagnosis: Machine learning for CAD prediction and risk stratification
- Bioresorbable Vascular Scaffolds: Future of coronary intervention (currently limited)
References
-
Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. doi:10.1093/eurheartj/ehz425
-
Task Force Members, Montalescot G, Sechtem U, et al. 2013 ESC guidelines on the management of stable coronary artery disease. Eur Heart J. 2013;34(38):2949-3003. doi:10.1093/eurheartj/eht296
-
National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis (NG95). London: NICE; 2016 (updated 2024). Available from: https://www.nice.org.uk/guidance/ng95
-
Hemingway H, Langenberg C, Damant J, Frost C, Pyorala K, Barrett-Connor E. Prevalence of angina in women versus men: a systematic review and meta-analysis. Circulation. 2008;117(12):1526-1536. doi:10.1161/CIRCULATIONAHA.107.720953
-
Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease. J Am Coll Cardiol. 2012;60(24):e44-e164. doi:10.1016/j.jacc.2012.07.013
-
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study). Lancet. 2004;364(9438):937-952. doi:10.1016/S0140-6736(04)17018-9
-
Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481-3488. doi:10.1161/CIRCULATIONAHA.105.537878
-
Campeau L. Letter: Grading of angina pectoris. Circulation. 1976;54(3):522-523. doi:10.1161/circ.54.3.947585
-
Beltrame JF, Weekes AJ, Morgan C, Tavella R, Spertus JA. The prevalence of weekly angina among patients with chronic stable angina in primary care practices. Arch Intern Med. 2009;169(16):1491-1499. doi:10.1001/archinternmed.2009.295
-
British Heart Foundation. Heart and circulatory disease statistics 2023. Available from: https://www.bhf.org.uk/
-
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019. Lancet. 2020;396(10258):1204-1222. doi:10.1016/S0140-6736(20)30925-9
-
Shaw LJ, Bugiardini R, Merz CN. Women and ischemic heart disease: evolving knowledge. J Am Coll Cardiol. 2009;54(17):1561-1575. doi:10.1016/j.jacc.2009.04.098
-
Gupta M, Singh N, Verma S. South Asians and cardiovascular risk: what clinicians should know. Circulation. 2006;113(25):e924-e929. doi:10.1161/CIRCULATIONAHA.105.583815
-
Greenland P, Knoll MD, Stamler J, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA. 2003;290(7):891-897. doi:10.1001/jama.290.7.891
-
Khot UN, Khot MB, Bajzer CT, et al. Prevalence of conventional risk factors in patients with coronary heart disease. JAMA. 2003;290(7):898-904. doi:10.1001/jama.290.7.898
-
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937-952. doi:10.1016/S0140-6736(04)17018-9
-
Libby P. The vascular biology of atherosclerosis. In: Braunwald's Heart Disease. 12th ed. Elsevier; 2022.
-
Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852-1866. doi:10.1161/CIRCRESAHA.114.302721
-
Duncker DJ, Bache RJ. Regulation of coronary blood flow during exercise. Physiol Rev. 2008;88(3):1009-1086. doi:10.1152/physrev.00045.2006
-
Nesto RW, Kowalchuk GJ. The ischemic cascade: temporal sequence of hemodynamic, electrocardiographic and symptomatic expressions of ischemia. Am J Cardiol. 1987;59(7):23C-30C. doi:10.1016/0002-9149(87)90192-5
-
Scanlon PJ, Faxon DP, Audet AM, et al. ACC/AHA guidelines for coronary angiography. J Am Coll Cardiol. 1999;33(6):1756-1824. doi:10.1016/s0735-1097(99)00126-6
-
Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol. 1983;1(2 Pt 1):574-575. doi:10.1016/s0735-1097(83)80093-x
-
Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA. 2000;283(24):3223-3229. doi:10.1001/jama.283.24.3223
-
Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction. Circulation. 2002;106(14):1893-1900. doi:10.1161/circ.106.14.1893
-
Beltrame JF, Crea F, Kaski JC, et al. International standardization of diagnostic criteria for vasospastic angina. Eur Heart J. 2017;38(33):2565-2568. doi:10.1093/eurheartj/ehv351
-
Genders TS, Steyerberg EW, Hunink MG, et al. Prediction model to estimate presence of coronary artery disease: retrospective pooled analysis of existing cohorts. BMJ. 2012;344:e3485. doi:10.1136/bmj.e3485
-
Wagner GS, Macfarlane P, Wellens H, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. J Am Coll Cardiol. 2009;53(11):1003-1011. doi:10.1016/j.jacc.2008.12.014
-
Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease. J Am Coll Cardiol. 2008;52(21):1724-1732. doi:10.1016/j.jacc.2008.07.031
-
Miller JM, Rochitte CE, Dewey M, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359(22):2324-2336. doi:10.1056/NEJMoa0806576
-
SCOT-HEART Investigators. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N Engl J Med. 2018;379(10):924-933. doi:10.1056/NEJMoa1805971
-
Wolk MJ, Bailey SR, Doherty JU, et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease. J Am Coll Cardiol. 2014;63(4):380-406. doi:10.1016/j.jacc.2013.11.009
-
Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing. Circulation. 2002;106(14):1883-1892. doi:10.1161/circ.106.14.1883
-
Mark DB, Shaw L, Harrell FE Jr, et al. Prognostic value of a treadmill exercise score in outpatients with suspected coronary artery disease. N Engl J Med. 1991;325(12):849-853. doi:10.1056/NEJM199109193251204
-
Pellikka PA, Arruda-Olson A, Chaudhry FA, et al. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease. J Am Soc Echocardiogr. 2020;33(1):1-41.e8. doi:10.1016/j.echo.2019.07.001
-
Underwood SR, Anagnostopoulos C, Cerqueira M, et al. Myocardial perfusion scintigraphy: the evidence. Eur J Nucl Med Mol Imaging. 2004;31(2):261-291. doi:10.1007/s00259-003-1344-5
-
Nagel E, Greenwood JP, McCann GP, et al. Magnetic Resonance Perfusion or Fractional Flow Reserve in Coronary Disease. N Engl J Med. 2019;380(25):2418-2428. doi:10.1056/NEJMoa1816263
-
Bateman TM, Dilsizian V, Beanlands RS, et al. American Society of Nuclear Cardiology and Society of Nuclear Medicine and Molecular Imaging Joint Position Statement on the Clinical Indications for Myocardial Perfusion PET. J Nucl Cardiol. 2016;23(5):1227-1231. doi:10.1007/s12350-016-0626-9
-
Scanlon PJ, Faxon DP, Audet AM, et al. ACC/AHA guidelines for coronary angiography. J Am Coll Cardiol. 1999;33(6):1756-1824. doi:10.1016/s0735-1097(99)00126-6
-
Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213-224. doi:10.1056/NEJMoa0807611
-
Gotberg M, Christiansen EH, Gudmundsdottir IJ, et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N Engl J Med. 2017;376(19):1813-1823. doi:10.1056/NEJMoa1616540
-
Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477. doi:10.1093/eurheartj/ehz425
-
Jespersen L, Hvelplund A, Abildstrom SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33(6):734-744. doi:10.1093/eurheartj/ehr331
-
Tardif JC, Ford I, Tendera M, Bourassa MG, Fox K; INITIATIVE Investigators. Efficacy of ivabradine, a new selective I(f) inhibitor, compared with atenolol in patients with chronic stable angina. Eur Heart J. 2005;26(23):2529-2536. doi:10.1093/eurheartj/ehi586
-
Bangalore S, Steg G, Deedwania P, et al. β-Blocker use and clinical outcomes in stable outpatients with and without coronary artery disease. JAMA. 2012;308(13):1340-1349. doi:10.1001/jama.2012.12559
-
Frishman WH. Beta-adrenergic blockers in the treatment of coronary artery disease. Drugs. 2003;63(20):2117-2136. doi:10.2165/00003495-200363200-00001
-
Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281(20):1927-1936. doi:10.1001/jama.281.20.1927
-
Thadani U, Lipicky RJ. Short and long-acting oral nitrates for stable angina pectoris. Cardiovasc Drugs Ther. 1994;8(4):611-623. doi:10.1007/BF00877416
-
IONA Study Group. Effect of nicorandil on coronary events in patients with stable angina: the Impact Of Nicorandil in Angina (IONA) randomised trial. Lancet. 2002;359(9314):1269-1275. doi:10.1016/S0140-6736(02)08265-X
-
Fox K, Ford I, Steg PG, et al. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372(9641):807-816. doi:10.1016/S0140-6736(08)61170-8
-
Chaitman BR, Pepine CJ, Parker JO, et al. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina. JAMA. 2004;291(3):309-316. doi:10.1001/jama.291.3.309
-
Cheitlin MD, Hutter AM Jr, Brindis RG, et al. ACC/AHA expert consensus document. Use of sildenafil (Viagra) in patients with cardiovascular disease. J Am Coll Cardiol. 1999;33(1):273-282. doi:10.1016/s0735-1097(98)00656-1
-
Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71-86. doi:10.1136/bmj.324.7329.71
-
Cholesterol Treatment Trialists' (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5
-
Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease. Eur Heart J. 2018;39(3):213-260. doi:10.1093/eurheartj/ehx419
-
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111-188. doi:10.1093/eurheartj/ehz455
-
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344(8934):1383-1389.
-
Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000;342(3):145-153. doi:10.1056/NEJM200001203420301
-
Yusuf S, Sleight P, Pogue J, et al. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients (HOPE). N Engl J Med. 2000;342(3):145-153. doi:10.1056/NEJM200001203420301
-
Fox KM; EURopean trial On reduction of cardiac events with Perindopril in stable coronary Artery disease Investigators. Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet. 2003;362(9386):782-788. doi:10.1016/s0140-6736(03)14286-9
-
Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021-3104. doi:10.1093/eurheartj/ehy339
-
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373(22):2117-2128. doi:10.1056/NEJMoa1504720
-
Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016;37(29):2315-2381. doi:10.1093/eurheartj/ehw106
-
Anderson L, Oldridge N, Thompson DR, et al. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J Am Coll Cardiol. 2016;67(1):1-12. doi:10.1016/j.jacc.2015.10.044
-
Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394
-
Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J Am Coll Cardiol. 2022;79(2):e21-e129. doi:10.1016/j.jacc.2021.09.006
-
Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-1780. doi:10.1056/NEJMoa012843
-
Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med. 1986;314(1):1-6. doi:10.1056/NEJM198601023140101
-
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961-972. doi:10.1056/NEJMoa0804626
-
Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367(25):2375-2384. doi:10.1056/NEJMoa1211585
-
Boden WE, O'Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516. doi:10.1056/NEJMoa070829
-
Maron DJ, Hochman JS, Reynolds HR, et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N Engl J Med. 2020;382(15):1395-1407. doi:10.1056/NEJMoa1915922
-
Daly CA, De Stavola B, Sendon JL, et al. Predicting prognosis in stable angina--results from the Euro heart survey of stable angina: prospective observational study. BMJ. 2006;332(7536):262-267. doi:10.1136/bmj.38695.605440.AE
-
Emond M, Mock MB, Davis KB, et al. Long-term survival of medically treated patients in the Coronary Artery Surgery Study (CASS) Registry. Circulation. 1994;90(6):2645-2657. doi:10.1161/01.cir.90.6.2645
-
Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356(8):830-840. doi:10.1056/NEJMra061889
-
Jespersen L, Abildstrom SZ, Hvelplund A, Prescott E. Persistent angina: highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin Res Cardiol. 2013;102(8):571-581. doi:10.1007/s00392-013-0568-z
-
Ong P, Camici PG, Beltrame JF, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 2018;250:16-20. doi:10.1016/j.ijcard.2017.08.068
-
Nørgaard BL, Leipsic J, Gaur S, et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J Am Coll Cardiol. 2014;63(12):1145-1155. doi:10.1016/j.jacc.2013.11.043
-
Douglas PS, Pontone G, Hlatky MA, et al. Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT): outcome and resource impacts study. Eur Heart J. 2015;36(47):3359-3367. doi:10.1093/eurheartj/ehv444
-
Doenst T, Haverich A, Serruys P, et al. PCI and CABG for Treating Stable Coronary Artery Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2019;73(8):964-976. doi:10.1016/j.jacc.2018.11.053
-
Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364(3):226-235. doi:10.1056/NEJMoa1002358
Medical Disclaimer: MedVellum content is for educational purposes only. Always consult professional guidelines and local protocols for clinical decision-making.