Anxiety Disorders in Adults: Comprehensive Clinical Management
Anxiety disorders represent the most prevalent class of mental disorders worldwide, characterized by excessive fear, anx... MRCP, MRCPsych exam preparation.
What matters first
Anxiety disorders represent the most prevalent class of mental disorders worldwide, characterized by excessive fear, anx... MRCP, MRCPsych exam preparation.
Active suicidal ideation with intent or plan requiring immediate psychiatric evaluation
9 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Active suicidal ideation with intent or plan requiring immediate psychiatric evaluation
- Severe self-neglect due to avoidance behaviors compromising basic needs
- Acute panic symptoms mimicking myocardial infarction or pulmonary embolism
- Signs of serotonin syndrome in patients on serotonergic medications
Exam focus
Current exam surfaces linked to this topic.
- MRCP
- MRCPsych
- AMC
Linked comparisons
Differentials and adjacent topics worth opening next.
- Hyperthyroidism
- Pheochromocytoma
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
SECTION 1: Clinical Overview
1.1 Summary
Anxiety disorders represent the most prevalent class of mental disorders worldwide, characterized by excessive fear, anxiety, and associated behavioral disturbances that cause clinically significant distress or functional impairment. [1] According to the Global Burden of Disease Study 2019, anxiety disorders affect approximately 301 million individuals globally, making them one of the leading causes of disability-adjusted life years (DALYs) in the mental health domain. [2] The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) classifies anxiety disorders as a distinct nosological category comprising generalized anxiety disorder (GAD), panic disorder (PD), social anxiety disorder (SAD), specific phobias, and agoraphobia, each with unique diagnostic criteria but sharing core features of excessive and persistent fear and anxiety. [3]
The clinical significance of anxiety disorders extends far beyond subjective distress. These conditions are associated with substantial functional impairment, healthcare utilization, reduced work productivity, and diminished quality of life. [4] The lifetime prevalence of any anxiety disorder ranges from 15% to 33.7% in high-income countries, with 12-month prevalence estimates of approximately 18.1% in the United States adult population. [5] Anxiety disorders demonstrate high comorbidity with major depressive disorder (MDD), with approximately 60% of individuals with anxiety disorders experiencing a comorbid mood disorder during their lifetime. [6] This comorbidity is associated with greater severity, poorer treatment response, and higher suicide risk.
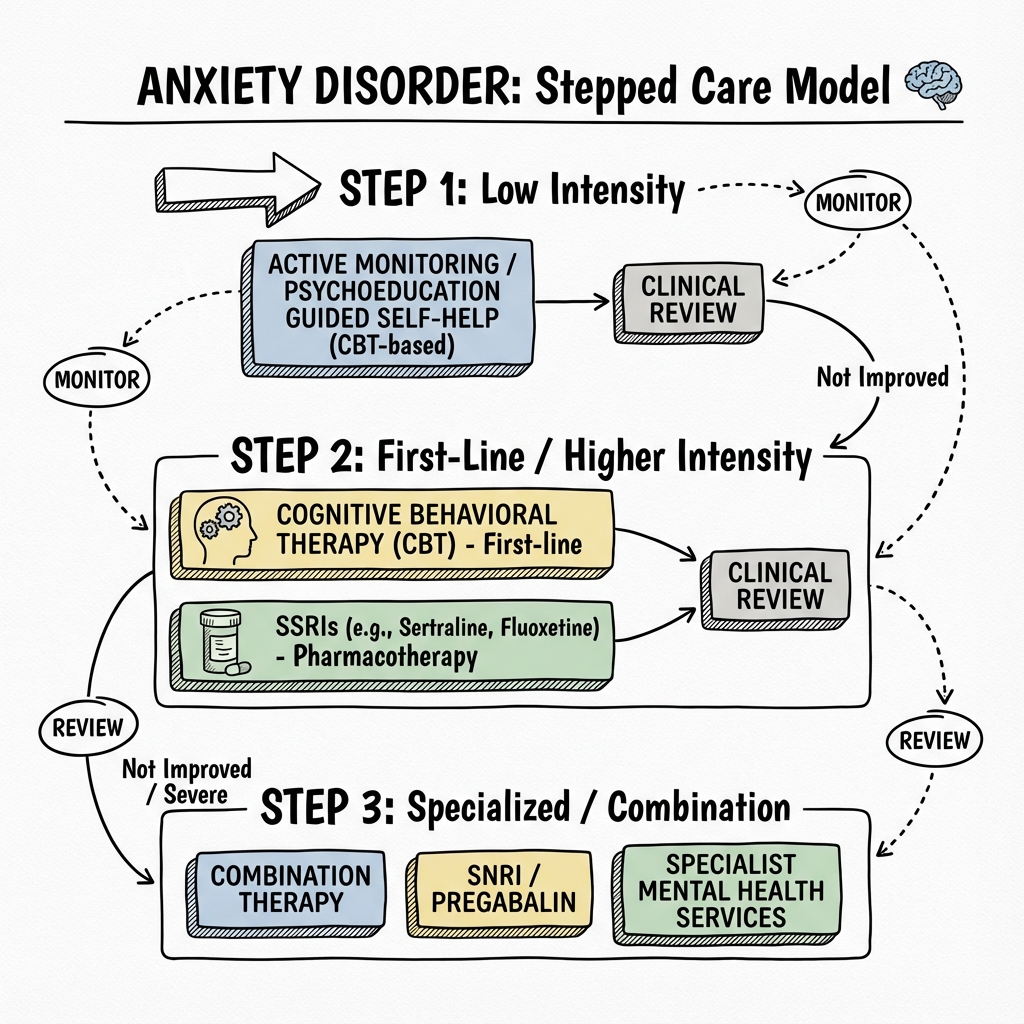
Contemporary management follows an evidence-based stepped-care approach integrating psychological therapies—predominantly cognitive behavioral therapy (CBT)—with pharmacological interventions including selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and adjunctive agents. [7] The National Institute for Health and Care Excellence (NICE) guidelines recommend low-intensity psychological interventions for mild anxiety, progressing to high-intensity CBT and/or pharmacotherapy for moderate-to-severe presentations. [8] Prognosis is generally favorable with evidence-based interventions, though chronic trajectories are common without treatment, emphasizing the importance of early identification and intervention.
1.2 Key Facts
- Definition: Anxiety disorders are characterized by excessive fear (emotional response to perceived or real imminent threat) and anxiety (anticipation of future threat) that are out of proportion to actual risk and persist beyond developmentally appropriate periods. [3]
- Global Prevalence: Approximately 4.05% (301 million individuals) globally; 7.3% in high-income countries, representing the most common mental disorder category. [2]
- Lifetime Prevalence: 33.7% for any anxiety disorder in the United States adult population, with women having approximately 2-fold higher rates than men. [5]
- 12-Month Prevalence: 18.1% in US adults; GAD affects 3.1%, panic disorder 2.7%, social anxiety disorder 7.1%, specific phobias 8.7%, and agoraphobia 0.8%. [5]
- Age of Onset: Median age of onset is 11 years for specific phobias, 13 years for social anxiety disorder, 20 years for panic disorder, and 31 years for generalized anxiety disorder. [9]
- Sex Distribution: Female-to-male ratio approximately 2:1 across most anxiety subtypes; this difference emerges at puberty and persists throughout the lifespan. [10]
- Mortality Risk: Indirectly increased via suicide (10-fold higher risk in severe cases), cardiovascular disease association (26-48% increased risk), and substance use disorders. [11]
- Disability Burden: Anxiety disorders rank as the sixth leading cause of disability globally (measured in years lived with disability). [2]
- Comorbidity: 60% lifetime comorbidity with major depression; 30% comorbidity with substance use disorders. [6]
- Gold Standard Assessment: Structured Clinical Interview for DSM-5 (SCID-5) or validated screening tools including GAD-7 (sensitivity 89%, specificity 82% at cutoff ≥10). [12]
- First-line Treatment: Cognitive behavioral therapy (CBT) and SSRIs (sertraline, escitalopram, paroxetine) demonstrate Level I evidence. [7]
- Treatment Response: Approximately 50-60% of patients achieve remission with first-line treatment; combined CBT plus pharmacotherapy demonstrates superior outcomes. [13]
1.3 Clinical Pearls
Diagnostic Pearl: "The Somatic Presentation" Approximately 40% of patients with anxiety disorders present primarily with physical symptoms to primary care settings—palpitations, dyspnea, gastrointestinal disturbance, or chronic pain—rather than reporting psychological distress. [14] Always screen for anxiety disorders in patients with medically unexplained symptoms, irritable bowel syndrome, chronic fatigue, or frequent emergency department presentations for chest pain with negative cardiac workup.
Examination Pearl: "The Panic-Cardiac Mimicry" Panic attacks closely mimic acute coronary syndrome and pulmonary embolism, with chest pain, dyspnea, and autonomic symptoms. Before diagnosing panic disorder, complete cardiac and pulmonary evaluation is mandatory. However, remember that panic disorder and coronary artery disease can coexist—treat both conditions when present. [15]
Treatment Pearl: "Start Low, Go Slow" When initiating SSRIs for anxiety disorders, begin at half the standard antidepressant dose (e.g., sertraline 25mg, escitalopram 5mg). Anxiety patients exhibit heightened sensitivity to the initial activating effects of serotonergic agents—transient increases in jitteriness, insomnia, and anxiety during the first 7-14 days frequently lead to premature discontinuation. [7] Warn patients about this paradoxical worsening and provide reassurance that it typically resolves within 2 weeks.
Pitfall Warning: "The Benzodiazepine Trap" Avoid prescribing benzodiazepines as monotherapy or for long-term use in anxiety disorders. While providing immediate symptomatic relief, benzodiazepines interfere with extinction learning essential for CBT efficacy and carry substantial risks of physiological dependence, cognitive impairment, and increased fall risk. [16] NICE guidelines recommend benzodiazepines only for short-term crisis management (maximum 2-4 weeks).
Mnemonic: "WATCHERS" for GAD Diagnostic Criteria Worry excessive (most days for ≥6 months), Anxiety difficult to control, Tension in muscles, Concentration difficulty, Hyperarousal (irritability), Energy loss (fatigue easily), Restlessness, Sleep disturbance. DSM-5 requires ≥3 of the 6 associated symptoms (excluding worry) for adults. [3]
Emergency Pearl: "Agitation Equals Risk" Psychomotor agitation in the context of anxiety—pacing, inability to sit still, wringing hands—represents a high-risk state for impulsive suicidal behavior. This agitated anxiety state warrants immediate escalation of care, one-to-one observation, and formal suicide risk assessment. [17] Never dismiss severe agitation as "just anxiety."
Exam Pearl: "Social Anxiety vs. Agoraphobia" Examiners frequently test this distinction: Social anxiety disorder involves fear of scrutiny and negative evaluation by others in social or performance situations. Agoraphobia involves fear of situations where escape may be difficult or help unavailable during panic-like symptoms—public transport, open spaces, enclosed spaces, crowds, or being outside home alone. [3] The cognitive focus differs: embarrassment vs. entrapment.
Evidence Pearl: "CBT Durability" Meta-analytic evidence demonstrates that the treatment gains from CBT for anxiety disorders are maintained at 12-24 month follow-up and may confer protection against relapse superior to pharmacotherapy alone. [18] This durability reflects the acquisition of active coping skills and corrective learning that persist after treatment termination.
1.4 Why This Matters Clinically
Patient Outcomes: Untreated anxiety disorders follow chronic trajectories with progressive functional decline. Longitudinal studies demonstrate that early-onset anxiety predicts subsequent development of major depression, substance use disorders, and cardiovascular disease. [11] The chronic hypercortisolemic state associated with untreated anxiety contributes to endothelial dysfunction, accelerated atherosclerosis, and increased risk of myocardial infarction and stroke—with hazard ratios of 1.26-1.48 for cardiovascular events. [19] Early treatment can interrupt this pathophysiological cascade.
Healthcare Burden: Anxiety disorders generate enormous healthcare costs—estimated at $42-47 billion annually in the United States—with over half attributed to non-psychiatric medical utilization as patients seek evaluation for somatic symptoms. [4] Patients with undiagnosed anxiety disorders are high utilizers of emergency departments, specialist consultations, and diagnostic testing, creating significant inefficiency in healthcare delivery.
Quality of Life: Anxiety disorders substantially impair quality of life across social, occupational, and physical domains. Social anxiety disorder leads to educational underachievement, occupational underperformance, and impaired intimate relationships. Agoraphobia can cause complete housebound status. Panic disorder generates anticipatory anxiety that restricts daily activities. [4]
Medico-legal Considerations: Failure to screen for suicidality in anxiety disorder presentations is a recognized source of litigation. Clinicians must document formal risk assessment, safety planning, and appropriate referral pathways. Additionally, prescribing benzodiazepines without discussing addiction risk or for prolonged periods creates liability exposure.
Training Relevance: Anxiety disorders are the most common psychiatric presentations in primary care and emergency medicine settings. Mastery of evidence-based assessment and management is a core competency for all medical practitioners, not exclusively psychiatrists. Examinations (MRCPsych, MRCP, USMLE) consistently test anxiety disorder knowledge.
SECTION 2: Classification and DSM-5-TR Diagnostic Criteria
2.1 Overview of Anxiety Disorder Spectrum
The DSM-5-TR classifies anxiety disorders as a distinct category characterized by features of excessive fear and anxiety with related behavioral disturbances. [3] The disorders differ primarily in the types of objects or situations that induce fear, anxiety, or avoidance behavior, and the associated cognitive ideation.
| Disorder | Core Fear/Anxiety Focus | Key Distinguishing Feature |
|---|---|---|
| Generalized Anxiety Disorder | Diffuse worry about multiple life domains | Chronic, excessive worry for ≥6 months |
| Panic Disorder | Recurrent unexpected panic attacks | Fear of future attacks and maladaptive behavior change |
| Agoraphobia | Situations where escape difficult | Fear of being trapped or unable to get help |
| Social Anxiety Disorder | Social situations with scrutiny | Fear of negative evaluation by others |
| Specific Phobia | Circumscribed object or situation | Marked fear immediately provoked by specific stimulus |
2.2 Generalized Anxiety Disorder (GAD)
DSM-5-TR Diagnostic Criteria: [3]
A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (work, school performance, health).
B. Difficulty controlling the worry.
C. Associated with three or more of the following six symptoms (only one required in children):
- Restlessness or feeling keyed up or on edge
- Being easily fatigued
- Difficulty concentrating or mind going blank
- Irritability
- Muscle tension
- Sleep disturbance (difficulty falling/staying asleep, restless unsatisfying sleep)
D. Causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
E. Not attributable to the physiological effects of a substance or another medical condition.
F. Not better explained by another mental disorder.
Prevalence and Course: Lifetime prevalence is 5.7-6.2% with 12-month prevalence of 2.9-3.1%. [5] GAD demonstrates the latest median age of onset (31 years) among anxiety disorders and follows a chronic waxing-and-waning course. Full remission rates are low without treatment (approximately 20% at 2 years).
2.3 Panic Disorder
DSM-5-TR Diagnostic Criteria: [3]
A. Recurrent unexpected panic attacks—an abrupt surge of intense fear or discomfort reaching peak within minutes, with four or more of 13 symptoms:
- Palpitations, pounding heart, or accelerated heart rate
- Sweating
- Trembling or shaking
- Sensations of shortness of breath or smothering
- Feelings of choking
- Chest pain or discomfort
- Nausea or abdominal distress
- Dizziness, unsteadiness, light-headedness, or faintness
- Chills or heat sensations
- Paresthesias (numbness or tingling)
- Derealization or depersonalization
- Fear of losing control or "going crazy"
- Fear of dying
B. At least one attack followed by ≥1 month of:
- Persistent concern about additional attacks or their consequences
- Significant maladaptive behavioral change related to attacks (avoidance)
C-D. Not attributable to substances, medical conditions, or other mental disorders.
Prevalence and Course: Lifetime prevalence 4.7% with 12-month prevalence 2.7%. [5] Peak onset in late adolescence to mid-30s. Panic attacks are necessary but not sufficient for panic disorder—approximately 23% of the general population experience isolated panic attacks without developing the disorder.
2.4 Agoraphobia
DSM-5-TR Diagnostic Criteria: [3]
A. Marked fear or anxiety about two or more of five situations:
- Using public transportation
- Being in open spaces
- Being in enclosed spaces
- Standing in line or being in a crowd
- Being outside of the home alone
B. Fear relates to thoughts that escape might be difficult or help unavailable in the event of panic-like symptoms.
C. Agoraphobic situations almost always provoke fear or anxiety.
D. Situations actively avoided, require companion, or endured with intense fear.
E. Fear is out of proportion to actual danger.
F. Fear persists for ≥6 months.
G-H. Causes significant distress/impairment; not better explained by other conditions.
Key Change in DSM-5: Agoraphobia is now a separate diagnosis from panic disorder. Approximately one-third of individuals with agoraphobia have never experienced panic symptoms. [3]
2.5 Social Anxiety Disorder (Social Phobia)
DSM-5-TR Diagnostic Criteria: [3]
A. Marked fear or anxiety about one or more social situations with possible scrutiny by others (social interactions, being observed, performing in front of others).
B. Fear of negative evaluation—acting in a way that will be embarrassing, humiliating, or lead to rejection.
C. Social situations almost always provoke fear or anxiety.
D. Social situations avoided or endured with intense fear/anxiety.
E. Fear is out of proportion to actual threat.
F. Persists for ≥6 months.
G-H. Causes significant distress/impairment; not attributable to substances or other conditions.
Specifier: Performance only—if fear restricted to speaking or performing in public.
Prevalence and Course: Lifetime prevalence 12.1% with 12-month prevalence 7.1%. [5] Typically begins in mid-teens with high chronicity. Early onset predicts greater severity and comorbidity.
2.6 Specific Phobia
DSM-5-TR Diagnostic Criteria: [3]
A. Marked fear or anxiety about a specific object or situation (e.g., flying, heights, animals, injections, blood).
B. Phobic object or situation almost always provokes immediate fear/anxiety.
C. Object or situation actively avoided or endured with intense fear/anxiety.
D. Fear is out of proportion to actual danger.
E. Persists for ≥6 months.
F-G. Causes significant distress/impairment; not better explained by other conditions.
Specifiers (by type):
- Animal (spiders, insects, dogs)
- Natural environment (heights, storms, water)
- Blood-injection-injury (needles, invasive medical procedures)
- Situational (airplanes, elevators, enclosed spaces)
- Other (choking, vomiting, loud sounds)
Prevalence and Course: Lifetime prevalence 12.5% with 12-month prevalence 8.7%—the most common anxiety disorder. [5] Median onset in childhood (7-11 years). Blood-injection-injury phobia is unique in producing vasovagal syncope rather than sympathetic activation.
SECTION 3: Epidemiology
3.1 Prevalence and Incidence
| Measure | Value | Population | Source |
|---|---|---|---|
| Global Prevalence | 301 million (4.05%) | All ages, 2019 | GBD Study [2] |
| US Lifetime Prevalence (Any Anxiety) | 33.7% | Adults 18+ | NCS-R [5] |
| US 12-Month Prevalence (Any Anxiety) | 18.1% | Adults 18+ | NCS-R [5] |
| GAD Lifetime Prevalence | 5.7% | Adults 18+ | NCS-R [5] |
| Panic Disorder Lifetime Prevalence | 4.7% | Adults 18+ | NCS-R [5] |
| Social Anxiety Lifetime Prevalence | 12.1% | Adults 18+ | NCS-R [5] |
| Specific Phobia Lifetime Prevalence | 12.5% | Adults 18+ | NCS-R [5] |
| Agoraphobia Lifetime Prevalence | 1.4% | Adults 18+ | NCS-R [5] |
Temporal Trends: Anxiety disorder prevalence increased by approximately 26% globally during the COVID-19 pandemic (2020), with particular impacts on young adults and women. [2] Pre-pandemic trends showed gradual increases in high-income countries, attributed to changing social structures, digital connectivity, and economic uncertainty.
3.2 Demographics Table
| Factor | Details | Clinical Significance |
|---|---|---|
| Age | Peak onset: Specific phobias 7-11y, SAD 13y, PD 20-24y, GAD 31y | Earlier onset predicts chronicity and comorbidity |
| Sex | Female:Male ratio 1.5-2:1 across subtypes | Hormonal and psychosocial factors; women less likely to receive treatment |
| Ethnicity | Higher reported rates in White/European populations | Potential cultural differences in reporting and help-seeking |
| Geography | Urban > Rural prevalence | Increased social density, noise, and life pace |
| Socioeconomic | Inverse relationship with income and education | Financial stress is potent anxiety trigger |
| Marital Status | Single, divorced, widowed at higher risk | Social support protective; relationship stress detrimental |
| Occupation | Healthcare, legal, service industries at higher risk | Occupational stress and burnout contribute |
3.3 Risk Factors
Non-Modifiable Risk Factors:
| Factor | Relative Risk (95% CI) | Mechanism |
|---|---|---|
| Female Sex | RR 1.9 (1.7-2.2) | Estrogen/progesterone modulation of HPA axis and amygdala sensitivity; psychosocial factors |
| Family History of Anxiety | RR 4.0-6.0 | Heritability 30-50%; shared genetic polymorphisms (5-HTTLPR, COMT) |
| Childhood Trauma/Adversity | RR 2.7-3.5 | Epigenetic alterations in glucocorticoid receptor genes; HPA axis dysregulation |
| Behavioral Inhibition Temperament | RR 2.5-4.0 | Innate temperamental trait of withdrawal from novelty predicts anxiety |
| Genetic Variants (5-HTTLPR short allele) | RR 1.4-1.8 | Reduced serotonin transporter efficiency affecting stress reactivity |
| Parental Anxiety/Depression | RR 2.0-3.0 | Genetic transmission plus modeling of anxious behaviors |
Modifiable Risk Factors:
| Factor | Relative Risk (95% CI) | Evidence Level | Intervention Impact |
|---|---|---|---|
| Chronic Stress/Life Events | RR 2.5-3.5 | Level I | Stress management reduces symptoms by 40-50% |
| Substance Misuse (alcohol, cannabis) | RR 2.0-3.0 | Level I | Treatment reduces anxiety in 60-70% |
| Chronic Insomnia | RR 2.1-2.8 | Level I | CBT-I reduces GAD-7 scores by 30-40% |
| Sedentary Lifestyle | RR 1.5-1.8 | Level II | Regular exercise has effect sizes similar to SSRIs |
| Caffeine (> 400mg/day) | RR 1.6-2.0 | Level II | Dose-dependent; reduction decreases panic frequency |
| Social Isolation | RR 2.0-2.5 | Level I | Social support strongly protective |
| Chronic Medical Illness | RR 2.0-3.0 | Level I | Integrated care improves outcomes |
3.4 Protective Factors
| Factor | Relative Risk | Mechanism | Evidence Level |
|---|---|---|---|
| Regular Physical Activity | RR 0.5-0.7 | Modulates BDNF, reduces HPA reactivity, endorphin release | Level I |
| Strong Social Support | RR 0.4-0.6 | Buffers stress response, provides practical and emotional resources | Level I |
| Mindfulness/Meditation Practice | RR 0.6-0.8 | Strengthens prefrontal cortical inhibition of amygdala | Level I |
| Cognitive Flexibility | RR 0.6-0.7 | Enables adaptive reappraisal of threats | Level II |
| Secure Attachment Style | RR 0.5-0.7 | Develops healthy emotional regulation patterns | Level II |
| Higher Education | RR 0.7-0.8 | Health literacy, coping resources, socioeconomic stability | Level II |
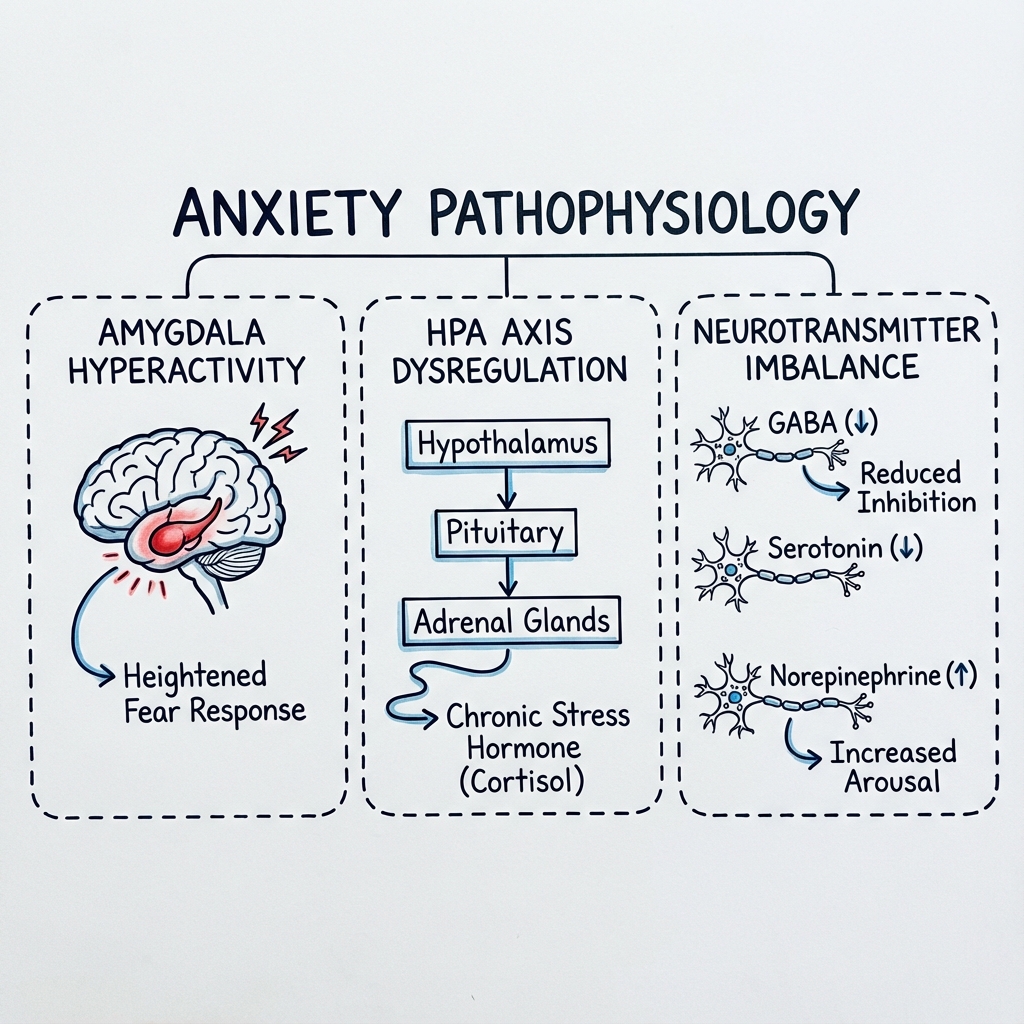
SECTION 4: Pathophysiology
4.1 Neurobiological Model of Anxiety
Anxiety disorders arise from dysregulation within interconnected neural circuits mediating threat detection, emotional processing, and fear extinction. The contemporary understanding integrates genetic vulnerability, environmental modifiers, and neuroplastic changes that create a self-perpetuating cycle of hypervigilance and maladaptive avoidance.
4.2 Neural Circuitry: The Fear Network
Core Structures:
| Structure | Normal Function | Dysfunction in Anxiety |
|---|---|---|
| Amygdala (Central Nucleus) | Rapid threat detection; initiates fear response | Hyperreactivity to neutral and ambiguous stimuli; lowered activation threshold |
| Prefrontal Cortex (vmPFC, mPFC) | Top-down inhibition of amygdala; cognitive reappraisal | Reduced activity; impaired regulatory control over fear response |
| Anterior Cingulate Cortex (ACC) | Error monitoring; conflict detection; emotional processing | Aberrant activation; impaired discrimination between threat and safety |
| Hippocampus | Contextual memory; safety learning; threat contextualization | Reduced volume (5-10%); impaired safety signal recognition |
| Insula | Interoceptive awareness; visceral sensation processing | Heightened interoceptive sensitivity; catastrophic interpretation of bodily sensations |
| Bed Nucleus of Stria Terminalis (BNST) | Sustained anxiety; anticipatory worry | Hyperactive in GAD; drives chronic apprehension rather than acute fear |
| Locus Coeruleus | Noradrenergic arousal system | Hyperactive; excessive norepinephrine release drives somatic symptoms |
Circuit Dysfunction: In anxiety disorders, the prefrontal cortex fails to provide adequate inhibitory control over amygdala activity. This results in "emotional hijacking"—threat-related stimuli trigger disproportionate fear responses without effective top-down modulation. [20] The hippocampus, which normally contextualizes threats and signals safety, shows reduced volume and impaired function in chronic anxiety, compromising the brain's ability to distinguish between genuinely dangerous and safe situations.
4.3 Neurotransmitter Systems
GABAergic System: Gamma-aminobutyric acid (GABA) is the primary inhibitory neurotransmitter in the central nervous system. Anxiety disorders are associated with reduced GABAergic tone, particularly decreased sensitivity or density of GABA-A receptors (alpha-2 and alpha-3 subunits) in limbic structures. [21] This reduction diminishes inhibitory control over excitatory circuits. Benzodiazepines exert their anxiolytic effect by enhancing GABA-A receptor function.
Serotonergic System: Serotonin (5-HT) modulates emotional responses through extensive projections from the raphe nuclei to limbic and prefrontal regions. The 5-HT1A receptor subtype is particularly implicated in anxiety—reduced 5-HT1A binding in the amygdala and raphe nuclei correlates with anxiety severity. [21] The 5-HTTLPR polymorphism affecting serotonin transporter expression influences stress reactivity and anxiety vulnerability. SSRIs enhance serotonergic transmission and are first-line pharmacotherapy.
Noradrenergic System: The locus coeruleus noradrenergic system drives the physiological arousal component of anxiety—tachycardia, tremor, sweating, and hypervigilance. Hyperactivity of this system underlies the somatic manifestations of panic attacks and generalized anxiety. [22] Beta-blockers (propranolol) target peripheral noradrenergic effects for performance anxiety.
HPA Axis Dysregulation: The hypothalamic-pituitary-adrenal (HPA) axis demonstrates altered function in anxiety disorders. Corticotropin-releasing hormone (CRH) hyperactivity in the hypothalamus drives sustained cortisol elevation. [20] While acute cortisol enhances survival responses, chronic hypercortisolemia is neurotoxic—particularly to hippocampal neurons—creating a feedback loop that perpetuates anxiety vulnerability.
Glutamatergic System: Glutamate, the primary excitatory neurotransmitter, contributes to anxiety through NMDA receptor-mediated hyperexcitability. Excessive glutamatergic activity in the amygdala contributes to fear conditioning and "kindling"—whereby repeated anxiety episodes progressively lower the threshold for future episodes. [21]
4.4 Genetics and Epigenetics
Heritability: Twin studies demonstrate 30-50% heritability for anxiety disorders, indicating substantial genetic contribution with significant environmental influence. [23]
Candidate Genes:
| Gene | Function | Anxiety Association |
|---|---|---|
| 5-HTTLPR | Serotonin transporter | Short allele associated with increased amygdala reactivity and anxiety |
| COMT Val158Met | Dopamine/catecholamine degradation | Met allele linked to reduced prefrontal dopamine and anxiety vulnerability |
| CRHR1 | Corticotropin-releasing hormone receptor | Polymorphisms affect HPA axis reactivity |
| FKBP5 | Glucocorticoid receptor sensitivity | Interacts with early trauma to predict anxiety |
| NPSR1 | Neuropeptide S receptor | Associated with panic disorder |
Epigenetic Modifications: Early life adversity induces DNA methylation changes, particularly in the NR3C1 gene (glucocorticoid receptor), permanently altering HPA axis set-point and stress reactivity. [23] These epigenetic marks can be partially reversed through environmental enrichment and psychotherapeutic intervention.
4.5 The Fear Conditioning Model
Anxiety disorders involve aberrant fear conditioning and failed extinction learning:
-
Acquisition: Neutral stimuli become associated with threat through classical conditioning (e.g., panic attack in supermarket → supermarket becomes conditioned stimulus)
-
Generalization: Fear spreads from original trigger to similar stimuli (supermarket → all stores → leaving home)
-
Avoidance: Behavioral escape from feared stimuli provides immediate relief (negative reinforcement) but prevents extinction learning
-
Failed Extinction: Unlike healthy individuals, those with anxiety disorders fail to extinguish conditioned fear responses. The vmPFC fails to signal safety, and hippocampal context-dependent memory is impaired
Therapeutic Implications: CBT with exposure therapy directly targets this circuit by repeatedly exposing patients to feared stimuli without negative outcome, promoting extinction learning and strengthening prefrontal inhibitory control over the amygdala. [18]
4.6 Interoceptive Sensitivity Model (Panic Disorder)
Panic disorder involves heightened interoceptive sensitivity—excessive attention to and catastrophic misinterpretation of normal bodily sensations. [15] Minor physiological fluctuations (heart rate variation, breathing irregularity) are detected, interpreted as dangerous, triggering further autonomic activation in a positive feedback loop culminating in full panic attack. The insula cortex, which processes visceral sensation, shows heightened reactivity in panic disorder.
SECTION 5: Clinical Presentation
5.1 Symptoms by Anxiety Disorder Subtype
Generalized Anxiety Disorder:
| Symptom | Frequency | Character | Clinical Significance |
|---|---|---|---|
| Excessive worry | 100% | Persistent "what if" thinking about multiple domains | Core diagnostic feature |
| Muscle tension | 60-80% | Chronic neck/shoulder tension, jaw clenching | Most specific physical symptom |
| Sleep disturbance | 70-80% | Difficulty falling asleep, restless sleep | Maintains anxiety cycle |
| Fatigue | 60-70% | Easily tired despite adequate sleep | Chronic arousal exhausts resources |
| Concentration difficulty | 50-60% | "Mind going blank," indecision | Functional impairment marker |
| Irritability | 50-60% | Low frustration tolerance | Often presents as interpersonal difficulty |
| Restlessness | 50-60% | "Keyed up," inability to relax | Observable agitation |
Panic Disorder:
| Symptom | Frequency | Character | Clinical Significance |
|---|---|---|---|
| Palpitations | 85-95% | Racing, pounding, irregular heartbeat | Most common symptom |
| Dyspnea | 80-90% | Feeling of suffocation, can't get enough air | Mimics respiratory emergency |
| Chest pain/discomfort | 60-70% | Tightness, pressure, sharp pain | Requires cardiac evaluation |
| Dizziness/lightheadedness | 60-70% | Unsteadiness, faintness | Hyperventilation-induced |
| Sweating | 60-70% | Profuse, generalized | Sympathetic activation |
| Trembling/shaking | 60-70% | Visible tremor | Noradrenergic surge |
| Paresthesias | 40-50% | Numbness, tingling (circumoral, extremities) | Hyperventilation-induced hypocalcemia |
| Depersonalization/derealization | 40-50% | "Unreal" feeling, detachment | Dissociative component |
| Fear of dying | 30-50% | Conviction of imminent death | Drives emergency presentations |
| Fear of losing control | 30-40% | "Going crazy" | Source of significant distress |
Anticipatory Anxiety: Between attacks, persistent worry about future attacks and their consequences (embarrassment, medical emergency, loss of control).
Agoraphobic Avoidance: Many patients develop avoidance of situations associated with panic attacks, which may progress to complete agoraphobia.
Social Anxiety Disorder:
| Symptom | Frequency | Context | Clinical Significance |
|---|---|---|---|
| Fear of negative evaluation | 100% | Core cognitive feature | Defines the disorder |
| Blushing | 60-80% | Social/performance situations | Highly distressing; visible |
| Trembling | 50-70% | Especially hands, voice | Interferes with performance |
| Sweating | 50-70% | Generalized or focal | Visible manifestation |
| Nausea/GI distress | 40-50% | Anticipatory or situational | May limit eating in public |
| Mind going blank | 40-50% | When "on the spot" | Cognitive disruption |
| Avoidance of social situations | 80-90% | From subtle to complete | Major functional impact |
| Safety behaviors | 90%+ | Avoiding eye contact, scripting speech | Maintain anxiety |
Specific Phobia:
Immediate, intense fear upon exposure to the specific phobic stimulus. Unlike other anxiety disorders, anxiety is circumscribed to the phobic object/situation. Blood-injection-injury phobia uniquely produces vasovagal syncope (biphasic response: initial tachycardia followed by bradycardia and hypotension).
5.2 Signs on Examination
General Observation:
- Appearance: Tense posture, furrowed brow, hypervigilance
- Behavior: Restlessness, fidgeting, frequent position shifts, poor eye contact (SAD)
- Speech: Rapid or hesitant, circumstantial when anxious
Vital Signs (during acute anxiety/panic):
- Tachycardia (HR 100-150 bpm)
- Tachypnea (RR 20-30/min)
- Mildly elevated blood pressure
- Normal oxygen saturation (distinguishes from medical emergency)
Physical Signs:
| Sign | Technique | Finding | Sensitivity/Specificity |
|---|---|---|---|
| Tremor | Outstretched hands | Fine postural tremor | 60-70% / 40-50% |
| Diaphoresis | Inspect palms, axillae | Moist, cool skin | 50-60% / 50-60% |
| Hyperreflexia | Deep tendon reflex testing | Brisk reflexes | 40-50% / 60-70% |
| Cold extremities | Palpation | Peripheral vasoconstriction | 50-60% / 50-60% |
| Mydriasis | Pupil examination | Dilated pupils | 30-40% / 70-80% |
| Sighing respirations | Observation | Frequent sighing, irregular breathing | 45-55% / 65-75% |
| Hyperventilation | Observation | Rapid, shallow breathing; tetany in severe cases | 40-50% / 70-80% |
Mental Status Examination:
- Mood: "Anxious," "on edge," "terrified"
- Affect: Anxious, apprehensive, constricted to anxious range; congruent with mood
- Thought process: Goal-directed but may be circumstantial; racing thoughts
- Thought content: Worry, catastrophizing; check for suicidal ideation
- Perception: Usually normal; may report depersonalization/derealization during panic
- Cognition: May show impaired concentration; otherwise intact
- Insight: Usually preserved—patients recognize worry is excessive
- Judgment: May be impaired by avoidance behaviors
5.3 Red Flags
[!CAUTION] RED FLAGS — Require Immediate Action:
- Suicidal Ideation/Intent: Express desire to die or "escape" the anxiety permanently; assess plan, means, intent
- Psychomotor Agitation: Severe restlessness, pacing, inability to sit still—high risk for impulsive self-harm
- Chest Pain with Risk Factors: New-onset, especially with cardiac risk factors—exclude ACS before attributing to panic
- Syncope: Loss of consciousness is unusual in panic (except blood-injury phobia)—evaluate for cardiac arrhythmia
- Focal Neurological Signs: New weakness, speech changes—consider stroke or neurological emergency
- First Panic Attack After Age 45: Higher likelihood of medical etiology (cardiac, pulmonary, endocrine)
- Acute Benzodiazepine Withdrawal: Seizure risk; requires medical management
- Severe Weight Loss: Indicates severe anxiety-related anorexia or occult medical condition
5.4 Screening and Assessment Tools
| Tool | Description | Scoring | Interpretation |
|---|---|---|---|
| GAD-7 | 7-item self-report for generalized anxiety | 0-21 | ≥5 mild, ≥10 moderate, ≥15 severe; ≥10 optimal screening threshold |
| PHQ-9 | 9-item depression screen (always co-administer) | 0-27 | Assesses comorbid depression |
| Panic Disorder Severity Scale (PDSS) | 7-item clinician-rated | 0-28 | Tracks panic frequency, severity, anticipatory anxiety, avoidance |
| Liebowitz Social Anxiety Scale (LSAS) | 24-item social anxiety severity | 0-144 | ≥30 probable SAD; ≥60 moderate; ≥90 severe |
| SPIN (Social Phobia Inventory) | 17-item self-report | 0-68 | ≥19 suggestive of SAD |
| Beck Anxiety Inventory (BAI) | 21-item somatic symptoms | 0-63 | ≥16 moderate; ≥26 severe anxiety |
| Columbia Suicide Severity Rating Scale (C-SSRS) | Structured suicide assessment | Categorical | Always assess if any suicidal ideation present |
GAD-7 Interpretation: [12]
- 0-4: Minimal anxiety
- 5-9: Mild anxiety
- 10-14: Moderate anxiety
- 15-21: Severe anxiety
Sensitivity 89%, specificity 82% at cutoff ≥10 for GAD diagnosis.
SECTION 6: Differential Diagnosis
6.1 Psychiatric Differential Diagnosis
| Condition | Key Distinguishing Features | Overlap with Anxiety Disorders |
|---|---|---|
| Major Depressive Disorder | Pervasive low mood, anhedonia, guilt, suicidality; anxiety is secondary | 60% comorbidity; treat both |
| Bipolar Disorder | History of manic/hypomanic episodes; anxiety during mood episodes | Screen before SSRI initiation |
| PTSD | Trauma history, re-experiencing, avoidance of trauma reminders, hyperarousal | Distinct etiology; overlapping symptoms |
| OCD | Intrusive, ego-dystonic obsessions; ritualistic compulsions | Classified separately in DSM-5 |
| Somatic Symptom Disorder | Excessive thoughts/behaviors about somatic symptoms | Anxiety about health prominent |
| Illness Anxiety Disorder | Preoccupation with having serious illness despite minimal symptoms | Health-focused anxiety |
| Adjustment Disorder with Anxiety | Identifiable stressor within 3 months; resolves within 6 months of stressor resolution | Time-limited; identifiable cause |
| Substance Use Disorder | Substance intoxication/withdrawal mimics or causes anxiety | Causal relationship assessment |
6.2 Medical Differential Diagnosis
Critical Rule: Always exclude medical causes of anxiety before establishing a primary anxiety disorder diagnosis, particularly in new-onset anxiety, atypical presentations, treatment-resistant cases, or anxiety with onset after age 45.
| System | Condition | Key Distinguishing Features | Investigations |
|---|---|---|---|
| Endocrine | Hyperthyroidism | Weight loss, heat intolerance, tremor, tachycardia, goiter | TSH, Free T4 |
| Endocrine | Pheochromocytoma | Paroxysmal hypertension, headache, sweating episodes | Plasma/urine metanephrines |
| Endocrine | Hypoglycemia | Relationship to meals, relief with glucose | Capillary/serum glucose |
| Endocrine | Cushing syndrome | Weight gain, striae, moon facies, hypertension | 24h urinary cortisol, dexamethasone suppression |
| Cardiovascular | Arrhythmias (SVT, AFib) | Sudden onset/offset, irregular pulse | ECG, Holter monitor |
| Cardiovascular | Mitral valve prolapse | Systolic click, mid-systolic murmur | Echocardiogram |
| Cardiovascular | Heart failure | Orthopnea, PND, peripheral edema, S3 gallop | BNP, echocardiogram |
| Respiratory | Asthma/COPD | Wheeze, cough, dyspnea on exertion | Spirometry, peak flow |
| Respiratory | Pulmonary embolism | Sudden onset dyspnea, pleuritic chest pain, risk factors | D-dimer, CTPA |
| Neurological | Temporal lobe epilepsy | Aura, automatisms, post-ictal confusion | EEG, MRI brain |
| Neurological | Vestibular disorders | Vertigo, nystagmus, imbalance | Dix-Hallpike, audiometry |
| Other | Caffeine excess | > 400mg/day intake | Dietary history |
| Other | Medication-induced | Correlates with medication initiation | Medication review |
| Substance | Alcohol/benzodiazepine withdrawal | Timing relative to last use, autonomic instability | Toxicology screen |
| Substance | Stimulant intoxication | Recent use, dilated pupils, agitation | Toxicology screen |
6.3 Investigations to Exclude Medical Causes
First-Line (All Patients):
- Full blood count (anemia, infection)
- Thyroid function tests (TSH, Free T4)
- Blood glucose
- Basic metabolic panel (electrolytes, calcium)
- ECG (arrhythmia)
Second-Line (Based on Clinical Suspicion):
- Liver function tests (hepatic encephalopathy, alcohol)
- Urine drug screen (substance-induced)
- Vitamin B12, folate, vitamin D
- Cortisol (if Cushing's suspected)
- Plasma/urine metanephrines (if pheochromocytoma suspected)
- Chest X-ray (pulmonary pathology)
- Echocardiogram (if murmur or cardiac symptoms)
- EEG (if seizure suspected)
- Brain MRI (if focal neurological signs)
SECTION 7: Investigations
7.1 Bedside Investigations
| Test | Expected Finding | Purpose | Urgency |
|---|---|---|---|
| Vital signs | Tachycardia, tachypnea; normal SpO2 | Distinguish from medical emergency | Immediate |
| Blood glucose | Normal (4-7 mmol/L) | Exclude hypoglycemia | Immediate |
| Pulse oximetry | Normal (> 95%) | Exclude hypoxia | Immediate |
| ECG | Sinus tachycardia; no ischemic changes or arrhythmia | Exclude cardiac cause | Immediate in acute presentations |
| Urinalysis | Normal | Exclude UTI (can cause delirium in elderly) | Routine |
7.2 Laboratory Investigations
| Test | Expected Finding | Purpose | Clinical Action |
|---|---|---|---|
| TSH | Normal (0.4-4.0 mIU/L) | Exclude hyperthyroidism | If low, check Free T4 and T3 |
| Free T4 | Normal | Confirm thyroid status | Treat thyroid disease if abnormal |
| FBC | Normal | Exclude anemia, infection | Investigate abnormalities |
| U&E/Creatinine | Normal | Baseline for medications; exclude electrolyte disturbance | Required before SSRI/SNRI |
| LFTs | Normal | Baseline for medications; alcohol misuse | Required for some medications |
| Calcium | Normal | Exclude hypercalcemia | Can cause anxiety symptoms |
| Urine toxicology | Negative | Exclude substance-induced anxiety | Screen if history suggests |
| Vitamin B12/Folate | Normal | Nutritional deficiencies can cause psychiatric symptoms | Supplement if deficient |
7.3 Specialized Investigations (Selected Cases)
| Investigation | Indication | Expected Finding |
|---|---|---|
| Plasma metanephrines | Paroxysmal hypertension, treatment-resistant "panic" | Elevated in pheochromocytoma |
| 24-hour urinary cortisol | Cushingoid features | Elevated in Cushing syndrome |
| Holter monitor | Palpitations, suspected arrhythmia | Arrhythmia detection |
| Echocardiogram | Murmur, heart failure symptoms | MVP, structural heart disease |
| EEG | Altered consciousness, automatisms, aura | Epileptiform activity |
| MRI brain | Focal neurological signs, late-onset anxiety | Structural lesions |
| CTPA | Sudden dyspnea, pleuritic pain, DVT risk | Pulmonary embolism |
7.4 Psychological Assessment
| Assessment | Purpose | Administrator |
|---|---|---|
| GAD-7 | Screen and monitor generalized anxiety | Self-report |
| PHQ-9 | Screen comorbid depression | Self-report |
| PDSS | Assess panic disorder severity | Clinician |
| LSAS | Assess social anxiety severity | Clinician or self-report |
| SCID-5 | Definitive diagnostic interview | Trained clinician |
| Columbia-Suicide Severity Rating Scale | Suicide risk assessment | Clinician |
| Functional assessment (work, social, ADLs) | Impairment severity | Clinical interview |
SECTION 8: Management
8.1 Management Algorithm
┌─────────────────────────────────────────────────────────────────────────┐
│ ANXIETY DISORDER MANAGEMENT ALGORITHM │
│ (NICE Stepped Care Model) │
└─────────────────────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ INITIAL ASSESSMENT │
│ • Screen with GAD-7, PHQ-9 │
│ • Exclude medical causes (TSH, ECG) │
│ • Assess suicide risk │
│ • Identify disorder subtype │
│ • Evaluate severity and impairment │
└─────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ SEVERITY STRATIFICATION │
│ • Mild: GAD-7 5-9, minimal impairment │
│ • Moderate: GAD-7 10-14 │
│ • Severe: GAD-7 ≥15, significant │
│ impairment or suicidality │
└─────────────────────────────────────────┘
│
┌───────────────────────────┼───────────────────────────┐
▼ ▼ ▼
┌───────────────┐ ┌───────────────┐ ┌───────────────┐
│ STEP 1-2 │ │ STEP 3 │ │ STEP 4 │
│ MILD │ │ MODERATE │ │ SEVERE │
│ │ │ │ │ │
│ Psychoeducation│ │ High-intensity│ │ Specialist │
│ Self-help │ │ CBT (12-15 │ │ referral │
│ (guided or │ │ sessions) │ │ │
│ unguided) │ │ AND/OR │ │ Combined CBT │
│ Lifestyle │ │ SSRI/SNRI │ │ + Pharmacol. │
│ modifications │ │ │ │ │
│ Active │ │ Applied │ │ Consider │
│ monitoring │ │ relaxation │ │ augmentation │
└───────────────┘ │ for GAD │ │ strategies │
│ └───────────────┘ │ │
│ │ │ Crisis team │
│ │ │ if needed │
▼ ▼ └───────────────┘
┌───────────────┐ ┌───────────────┐ │
│ 4-6 WEEK │ │ 8-12 WEEK │ ▼
│ REVIEW │ │ REVIEW │ ┌───────────────┐
│ │ │ │ │ TREATMENT- │
│ If improved: │ │ Response? │ │ RESISTANT │
│ Continue │ │ (≥50% ↓ GAD-7)│ │ │
│ │ └───────┬───────┘ │ • Combine Rx │
│ If no change: │ Yes │ No │ • Switch │
│ → Step up │ ▼ │ medication │
└───────────────┘ ┌───────────────┐ │ • Augment │
│ CONTINUE │ │ (pregabalin,│
│ 6-12 months │ │ buspirone, │
│ │ │ quetiapine) │
│ Then gradual │ │ • Intensive │
│ taper with │ │ CBT program │
│ relapse plan │ └───────────────┘
└───────────────┘
8.2 Acute/Emergency Management
For Acute Panic Attack (Emergency Department):
- Reassurance and Environment: Move to quiet room; calm, supportive approach
- Breathing Control: Guide slow diaphragmatic breathing (4 seconds in, hold 4 seconds, 4 seconds out)
- Exclude Medical Emergency: Brief cardiac and pulmonary assessment; ECG if indicated
- Pharmacological (if severe/prolonged):
- Lorazepam 0.5-1mg PO/SL/IM (single dose)
- Avoid routine benzodiazepine prescriptions
- Psychoeducation: Explain panic physiology; reassure about non-dangerous nature
- Safety Planning: Assess suicide risk; provide crisis contacts
- Follow-up: Arrange primary care or mental health follow-up within 1-2 weeks
For Severe Anxiety with Suicidal Ideation:
- Immediate psychiatric consultation
- One-to-one observation
- Remove access to means
- Formal risk assessment (C-SSRS)
- Consider psychiatric admission if high risk
8.3 Psychological Therapies
Cognitive Behavioral Therapy (CBT) — FIRST-LINE for all anxiety disorders [7,8]
| Component | Description | Mechanism |
|---|---|---|
| Psychoeducation | Understanding anxiety physiology and cycle | Demystifies symptoms; reduces catastrophizing |
| Cognitive restructuring | Identifying and challenging anxious thoughts | Modifies threat appraisal |
| Behavioral experiments | Testing anxious predictions | Disconfirms feared outcomes |
| Exposure therapy | Graduated, systematic exposure to feared stimuli | Promotes extinction learning |
| Relaxation training | Diaphragmatic breathing, progressive muscle relaxation | Reduces physiological arousal |
| Relapse prevention | Maintaining gains; managing setbacks | Long-term efficacy |
Evidence: Meta-analyses demonstrate effect sizes of 0.8-1.3 for CBT vs. waitlist controls across anxiety disorders. [18] Treatment gains maintained at 12-24 month follow-up.
Format: Individual or group; typically 12-16 sessions; protocol-based manualized treatment
Disorder-Specific CBT Emphases:
- GAD: Worry exposure; intolerance of uncertainty modification; problem-solving
- Panic Disorder: Interoceptive exposure; behavioral experiments; cognitive restructuring of catastrophic misinterpretation
- Social Anxiety: Behavioral experiments in social situations; attention training; video feedback
- Specific Phobia: Graduated exposure hierarchy; in-vivo exposure; single-session treatment effective for simple phobias
- Agoraphobia: Graduated exposure to avoided situations; with or without therapist-accompanied exposure
Applied Relaxation — Alternative first-line for GAD [8] Technique involving progressive muscle relaxation and rapid relaxation skills applied in anxiety-provoking situations. Non-inferior to CBT for GAD in NICE evidence review.
Acceptance and Commitment Therapy (ACT) Third-wave CBT approach emphasizing acceptance of anxious thoughts rather than challenging content; focus on values-directed action despite anxiety. Growing evidence base; may be helpful for treatment-resistant cases.
8.4 Pharmacological Management
First-Line Medications: SSRIs and SNRIs [7,8]
| Medication | Class | Starting Dose | Target Dose | Key Considerations |
|---|---|---|---|---|
| Sertraline | SSRI | 25mg daily | 50-200mg daily | First-choice; good efficacy and tolerability |
| Escitalopram | SSRI | 5mg daily | 10-20mg daily | Well-tolerated; QTc prolongation at higher doses |
| Paroxetine | SSRI | 10mg daily | 20-50mg daily | Effective but more weight gain; difficult discontinuation |
| Fluoxetine | SSRI | 10mg daily | 20-60mg daily | Long half-life reduces discontinuation symptoms |
| Venlafaxine XR | SNRI | 37.5mg daily | 75-225mg daily | May be more effective for severe anxiety; monitor BP |
| Duloxetine | SNRI | 30mg daily | 60-120mg daily | Also effective for pain; less hypertension than venlafaxine |
Key Prescribing Principles:
- Start low, go slow: Begin at half standard antidepressant dose due to initial activation/jitteriness
- Warn about delayed onset: Therapeutic effects emerge at 2-4 weeks; full effect by 8-12 weeks
- Warn about initial worsening: Anxiety may transiently increase in first 1-2 weeks
- Duration: Continue for minimum 12 months after remission; longer if recurrent episodes
- Discontinuation: Gradual taper over 4+ weeks to minimize discontinuation syndrome
Second-Line and Adjunctive Medications:
| Medication | Class | Dose Range | Indication | Key Considerations |
|---|---|---|---|---|
| Pregabalin | Gabapentinoid | 150-600mg/day divided | GAD (licensed UK/EU) | Rapid onset; sedation; Schedule V controlled substance |
| Buspirone | 5-HT1A partial agonist | 15-60mg/day divided | GAD adjunct | No sedation; delayed onset (2-4 weeks); no dependence |
| Mirtazapine | NaSSA | 15-45mg at night | Anxiety with insomnia | Sedating; weight gain; useful if sleep prominent |
| Propranolol | Beta-blocker | 10-40mg PRN | Performance anxiety | Targets peripheral symptoms only; not for generalized use |
| Hydroxyzine | Antihistamine | 25-100mg/day | Short-term anxiolysis | Sedating; anticholinergic; avoid in elderly |
Treatment-Resistant Anxiety (After 2 adequate SSRI/SNRI trials):
| Strategy | Evidence Level | Considerations |
|---|---|---|
| Combine CBT with pharmacotherapy | Level I | Superior to either alone |
| Switch within class (SSRI to different SSRI) | Level II | Often helpful |
| Switch across class (SSRI to SNRI or vice versa) | Level II | Consider if class-specific side effects |
| Augment with pregabalin | Level I | Licensed for GAD in UK/EU |
| Augment with buspirone | Level II | Well-tolerated; modest effect size |
| Augment with quetiapine XR (25-150mg) | Level II | Metabolic monitoring required; off-label |
| Augment with aripiprazole (2-10mg) | Level III | Limited evidence; metabolic side effects |
Medications to Use with Caution or Avoid:
| Medication | Concern | Recommendation |
|---|---|---|
| Benzodiazepines | Dependence; impairs extinction learning; cognitive impairment; falls | Short-term crisis use only (2-4 weeks maximum); not for maintenance |
| Tricyclic antidepressants | Cardiac toxicity; anticholinergic effects; lethal in overdose | Avoid as first-line; imipramine has evidence but safety concerns |
| Antipsychotics (high-dose) | Metabolic syndrome; EPS; QTc prolongation | Low-dose augmentation only; not monotherapy |
8.5 Benzodiazepine Prescribing Guidelines
If Benzodiazepines Must Be Used:
- Reserve for short-term crisis management only (maximum 2-4 weeks)
- Use lowest effective dose
- Document clear rationale and time-limited plan
- Provide psychoeducation about dependence risk
- Schedule definite review date
- Avoid in patients with substance use history
- Do not prescribe on repeat/ongoing basis
Benzodiazepine Selection (if indicated for short-term use):
| Agent | Half-life | Onset | Dose | Notes |
|---|---|---|---|---|
| Lorazepam | Intermediate (10-20h) | Moderate | 0.5-1mg PRN, max 4mg/day | Less accumulation; fewer drug interactions |
| Diazepam | Long (20-100h) | Fast | 2-10mg PRN, max 30mg/day | Longer-acting; smoother effect; accumulates |
| Clonazepam | Long (18-50h) | Slow | 0.25-0.5mg BD | Less euphoria; longer duration |
8.6 Lifestyle and Complementary Interventions
| Intervention | Evidence Level | Recommendation | Effect Size |
|---|---|---|---|
| Aerobic exercise | Level I | 150 min/week moderate intensity | Equivalent to pharmacotherapy (d=0.5-0.8) |
| Caffeine reduction | Level II | less than 200mg/day (2 coffees); gradual reduction | Reduces panic frequency |
| Alcohol reduction | Level I | Minimize or abstain | Reduces anxiety; prevents "rebound" anxiety |
| Sleep hygiene | Level II | Regular schedule; limit screens | Bidirectional relationship with anxiety |
| Mindfulness meditation | Level I | 10-20 min daily | Effect size d=0.5 for anxiety reduction |
| Yoga | Level II | Regular practice | Modest effect; may enhance CBT |
8.7 Special Populations
Pregnancy and Breastfeeding:
- CBT is first-line (no fetal exposure)
- If pharmacotherapy required: sertraline preferred (most safety data)
- Avoid paroxetine in first trimester (cardiac malformation risk)
- Benzodiazepines: avoid if possible; floppy infant syndrome risk
- Discuss risks vs. benefits; untreated severe anxiety also carries fetal risks
Elderly:
- Start at lower doses; slower titration
- Avoid benzodiazepines (falls, cognitive impairment)
- SSRIs preferred; monitor for hyponatremia (SIADH)
- Shorter CBT protocols may be needed
Comorbid Substance Use Disorder:
- Treat both conditions concurrently
- Avoid benzodiazepines (high misuse potential)
- SSRIs safe and effective
- Integrated treatment programs optimal
Cardiovascular Disease:
- SSRIs are safe post-MI
- Sertraline has best evidence in cardiac population
- Avoid TCAs (cardiac toxicity)
- Treat anxiety to reduce cardiac risk
8.8 Treatment Duration and Discontinuation
Acute Phase: 8-12 weeks to achieve response Continuation Phase: 6-12 months post-remission for first episode; longer for recurrent Maintenance: Consider indefinite treatment for recurrent episodes (≥3) or severe residual symptoms
Discontinuation Protocol:
- Achieve sustained remission (≥6 months symptom-free)
- Taper gradually over minimum 4 weeks (longer if prolonged treatment)
- Reduce by 25% every 2-4 weeks
- Warn about discontinuation symptoms vs. relapse
- Provide relapse prevention plan
- Close follow-up during taper
Discontinuation Syndrome (especially with paroxetine, venlafaxine):
- Dizziness, nausea, headache, flu-like symptoms
- Electric shock sensations ("brain zaps")
- Irritability, insomnia
- Onset 2-4 days after stopping; typically resolves in 1-2 weeks
- Management: slower taper; temporarily increase dose if severe
SECTION 9: Complications
9.1 Psychiatric Complications
| Complication | Frequency | Risk Factors | Prevention/Management |
|---|---|---|---|
| Major Depressive Disorder | 50-60% lifetime | Chronicity, severity, avoidance | Early treatment; monitor mood |
| Substance Use Disorder | 20-30% lifetime | Self-medication, family history | Screen for substances; integrated treatment |
| Suicide | 10% attempt lifetime; elevated completed | Comorbid depression, hopelessness | Regular risk assessment; safety planning |
| Other anxiety disorders | 30-50% | Shared vulnerability | Comprehensive assessment |
| Personality disorder comorbidity | 25-30% | Early onset, trauma history | Longer-term psychotherapy |
9.2 Medical Complications
| Complication | Mechanism | Relative Risk | Prevention |
|---|---|---|---|
| Cardiovascular disease | Chronic HPA activation, endothelial dysfunction | RR 1.26-1.48 | Treat anxiety; cardiovascular risk factor management |
| Hypertension | Chronic sympathetic activation | RR 1.2-1.5 | Monitor BP; treat both conditions |
| Irritable bowel syndrome | Gut-brain axis dysfunction | RR 2.0-3.0 | Integrated management |
| Chronic pain syndromes | Central sensitization | RR 1.5-2.5 | Address anxiety component |
| Migraine | Shared neurobiology | RR 2.0-3.0 | Treat both conditions |
9.3 Treatment-Related Complications
| Complication | Incidence | Presentation | Management |
|---|---|---|---|
| SSRI activation syndrome | 15-20% initially | Increased anxiety, jitteriness, insomnia | Start low dose; warn patient; temporary |
| Sexual dysfunction | 30-60% | Decreased libido, anorgasmia, erectile dysfunction | Dose reduction; switch (bupropion); add buspirone |
| Weight gain | Variable | Paroxetine, mirtazapine highest risk | Monitor weight; choose alternatives |
| Serotonin syndrome | Rare | Agitation, hyperthermia, tremor, rigidity | Avoid drug combinations; stop serotonergic agents |
| Bleeding | Increased risk | Especially with NSAIDs or anticoagulants | Use gastroprotection if indicated |
| Benzodiazepine dependence | 30-50% with prolonged use | Tolerance, withdrawal, dose escalation | Limit to short-term use |
| Hyponatremia | 1-5% (elderly) | Confusion, falls, seizures | Monitor sodium, especially elderly |
SECTION 10: Prognosis and Outcomes
10.1 Natural History (Untreated)
| Disorder | Course | Spontaneous Remission | Key Prognostic Features |
|---|---|---|---|
| GAD | Chronic, waxing-waning | 20% at 2 years | Most chronic trajectory |
| Panic Disorder | Variable; 30-40% chronic | 30-40% at 5 years | Agoraphobia worsens prognosis |
| Social Anxiety | Chronic; low remission | 20-30% at 5 years | Early onset predicts chronicity |
| Specific Phobia | Stable without treatment | 10-20% | Often persists decades |
| Agoraphobia | Progressive without treatment | 10-20% | May lead to complete housebound status |
10.2 Outcomes with Treatment
| Outcome Measure | CBT | Pharmacotherapy | Combined |
|---|---|---|---|
| Response rate (≥50% improvement) | 50-60% | 50-60% | 60-70% |
| Remission rate | 40-50% | 40-50% | 50-60% |
| Relapse at 12 months (after stopping) | 15-25% | 30-50% | 20-30% |
| Sustained remission at 2 years | 50-60% | 40-50% | 55-65% |
Predictors of Good Outcome:
- Early treatment initiation
- Good treatment adherence
- Absence of avoidance behaviors
- Lower baseline severity
- Absence of comorbid personality disorder
- Strong social support
- Completion of full CBT course
Predictors of Poor Outcome:
- Delayed treatment (> 2 years from onset)
- Severe avoidance/agoraphobia
- Comorbid depression or substance use
- Personality disorder comorbidity
- Early onset
- History of childhood trauma
- Treatment non-adherence
10.3 Long-Term Functional Outcomes
- Occupational: 30-50% report significant work impairment; higher unemployment rates
- Social: Impaired relationships, social isolation (especially SAD)
- Quality of life: Significantly reduced across all domains
- Healthcare utilization: High service use continues even after diagnosis
SECTION 11: Prevention and Screening
11.1 Primary Prevention
| Strategy | Target Population | Evidence Level | Implementation |
|---|---|---|---|
| School-based anxiety prevention programs | Children 8-15 years | Level I | Universal or targeted programs |
| Parenting interventions | Parents of behaviorally inhibited children | Level II | Reduce overprotection; encourage exposure |
| Early intervention for at-risk youth | High anxiety symptoms, family history | Level I | Brief CBT-based interventions |
| Stress management in high-risk occupations | Healthcare, emergency services | Level II | Workplace wellness programs |
11.2 Screening Recommendations
| Setting | Recommendation | Tool | Frequency |
|---|---|---|---|
| Primary Care | Screen adults with unexplained somatic symptoms | GAD-7 + PHQ-9 | Opportunistic |
| Emergency Department | Screen frequent attenders for panic | Brief screening | At presentation |
| Chronic Disease Clinics | Screen patients with chronic illness | GAD-7 | Annual |
| Perinatal | Screen pregnant/postpartum women | GAD-7 + PHQ-9 | Each trimester; postpartum |
| Mental Health | Routine assessment | Comprehensive | Each visit |
SECTION 12: Key Guidelines and Evidence
12.1 Major Clinical Guidelines
NICE Guideline NG116: Generalized Anxiety Disorder and Panic Disorder in Adults (2019, updated 2020) [8]
- Organization: National Institute for Health and Care Excellence (UK)
- Key Recommendations:
- Stepped care model for anxiety management
- CBT is first-line psychological therapy
- SSRIs (sertraline) first-line pharmacotherapy
- Benzodiazepines only for short-term crisis use (2-4 weeks maximum)
- Do not use antipsychotics for GAD/panic
- Link: https://www.nice.org.uk/guidance/ng116
APA Practice Guideline for Treatment of Panic Disorder (2010, reaffirmed 2020) [7]
- Organization: American Psychiatric Association
- Key Recommendations:
- CBT and SSRIs/SNRIs are Level I recommendations
- Combined treatment may be superior
- Benzodiazepines effective but not first-line due to dependence
WFSBP Guidelines for Anxiety Disorders (2023) [24]
- Organization: World Federation of Societies of Biological Psychiatry
- Key Recommendations:
- SSRIs/SNRIs first-line for all anxiety disorders
- Pregabalin alternative for GAD
- CBT should be offered to all patients
12.2 Landmark Trials
CALM Trial (2010) [13]
- Design: Randomized controlled trial, n=1004
- Intervention: Coordinated Anxiety Learning and Management (CALM) vs. usual care
- Outcome: CALM achieved 60.7% response vs. 39.5% usual care (pless than 0.001)
- Impact: Demonstrated superiority of collaborative care integrating CBT and pharmacotherapy
- PMID: 20483971
STAR*D Anxiety Analysis (2008) [25]
- Design: Secondary analysis of STAR*D depression trial
- Key Finding: Patients with anxious depression have lower remission rates, more side effects, and require longer treatment
- Impact: Highlighted importance of addressing comorbid anxiety
- PMID: 18190331
Meta-analysis of CBT for Anxiety (Cuijpers et al., 2016) [18]
- Design: Meta-analysis of 144 studies
- Key Finding: Effect size d=0.84 vs. control; effects maintained at 12-month follow-up
- Impact: Established CBT as evidence-based first-line treatment
- PMID: 24607174
BALANCE Trial - Pregabalin for GAD (2010) [26]
- Design: RCT, n=454
- Intervention: Pregabalin vs. placebo vs. lorazepam
- Outcome: Pregabalin effective with anxiolytic effects within first week
- PMID: 16026622
SECTION 13: Patient Explanation
13.1 What Are Anxiety Disorders?
Anxiety is a normal human emotion that helps protect us from danger. However, in anxiety disorders, this protective system becomes overactive—like a smoke alarm that goes off for burnt toast rather than a real fire. Your brain is signaling "danger" even when there is no actual threat, causing your body to react with a racing heart, rapid breathing, and muscle tension.
13.2 What Causes Anxiety Disorders?
Anxiety disorders develop from a combination of factors:
- Genetics: Anxiety tends to run in families
- Brain chemistry: Imbalances in brain chemicals like serotonin
- Life experiences: Stressful events, especially in childhood
- Learned patterns: Habits of worry and avoidance
13.3 How Are They Treated?
Two main approaches work well, often best when combined:
Talking therapy (CBT): You'll learn to identify anxious thoughts, challenge them, and gradually face feared situations. This rewires the brain's anxiety response.
Medication: Antidepressant medications (SSRIs) help rebalance brain chemistry. They take 2-4 weeks to work and are not addictive.
13.4 What Can I Do to Help Myself?
- Regular exercise (30 minutes, 5 times weekly)
- Reduce caffeine and alcohol
- Practice relaxation or mindfulness
- Maintain regular sleep patterns
- Stay connected with supportive people
- Face fears gradually rather than avoiding them
13.5 What Is the Outlook?
Most people with anxiety disorders improve significantly with treatment. About 50-60% achieve full remission. The skills you learn in therapy stay with you and help prevent future episodes. Early treatment leads to better outcomes.
SECTION 14: Examination Focus
14.1 Common Examination Questions
-
"What are the DSM-5 criteria for generalized anxiety disorder?"
- Excessive worry more days than not for ≥6 months
- Difficulty controlling worry
- ≥3 associated symptoms (restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance)
- Significant distress/impairment
- Not due to substance or medical condition
-
"A 28-year-old woman presents with palpitations, dyspnea, and fear of dying during episodes lasting 10-30 minutes. What is your differential and management?"
- Differential: Panic disorder, cardiac arrhythmia, hyperthyroidism, pheochromocytoma
- Immediate: ECG, pulse oximetry, glucose, reassurance
- Investigations: TSH, 12-lead ECG, consider Holter if paroxysmal
- If panic disorder confirmed: CBT first-line, SSRI (sertraline 25mg increasing to 50-100mg)
-
"Describe the mechanism of action and evidence for SSRIs in anxiety disorders."
- SSRIs inhibit serotonin reuptake, increasing synaptic 5-HT
- Downstream effects include 5-HT1A receptor desensitization and neuroplastic changes
- NNT approximately 5-7 for response vs. placebo
- Effect size d=0.3-0.5 in meta-analyses
- Time course: 2-4 weeks initial effect, 8-12 weeks full effect
-
"Differentiate social anxiety disorder from agoraphobia."
- Social anxiety: Fear of scrutiny and negative evaluation by others
- Agoraphobia: Fear of situations where escape difficult or help unavailable
- Cognitive focus: Embarrassment/judgment vs. entrapment/panic-like symptoms
14.2 Viva Opening Statement
"Anxiety disorders are a group of mental disorders characterized by excessive fear and anxiety with associated behavioral disturbances. They are the most common mental disorders globally, with a lifetime prevalence of approximately 33%. The disorders include generalized anxiety disorder, panic disorder, social anxiety disorder, specific phobias, and agoraphobia. Management follows evidence-based guidelines with cognitive behavioral therapy and SSRIs as first-line treatments, and prognosis is generally favorable with appropriate intervention."
14.3 Common Mistakes to Avoid
- Failure to exclude medical causes before diagnosing primary anxiety
- Prescribing benzodiazepines as first-line or for long-term use
- Starting SSRIs at full dose (causes activation; start at half dose)
- Not warning patients about initial worsening and delayed onset of effect
- Forgetting to assess suicide risk in anxiety presentations
- Confusing social anxiety with agoraphobia (scrutiny vs. entrapment)
- Missing comorbid depression (always co-screen with PHQ-9)
14.4 Key Evidence to Cite
- CALM trial: Integrated care superior to usual care (PMID: 20483971)
- Cuijpers meta-analysis: CBT effect size d=0.84 with maintained gains (PMID: 24607174)
- NCS-R epidemiology: 33.7% lifetime prevalence (PMID: 15939837)
- NICE NG116: Stepped care, CBT first-line, SSRIs first-line pharmacotherapy
SECTION 15: References
-
Stein MB, Sareen J. Clinical Practice. Generalized Anxiety Disorder. N Engl J Med. 2015;373(21):2059-2068. doi:10.1056/NEJMcp1502514 [PMID: 26580998]
-
GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019. Lancet Psychiatry. 2022;9(2):137-150. doi:10.1016/S2215-0366(21)00395-3 [PMID: 35026139]
-
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision. Washington, DC: American Psychiatric Publishing; 2022.
-
Craske MG, Stein MB. Anxiety. Lancet. 2016;388(10063):3048-3059. doi:10.1016/S0140-6736(16)30381-6 [PMID: 27349358]
-
Kessler RC, Petukhova M, Sampson NA, Zaslavsky AM, Wittchen HU. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012;21(3):169-184. doi:10.1002/mpr.1359 [PMID: 22865617]
-
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602. doi:10.1001/archpsyc.62.6.593 [PMID: 15939837]
-
Bandelow B, Michaelis S, Wedekind D. Treatment of anxiety disorders. Dialogues Clin Neurosci. 2017;19(2):93-107. doi:10.31887/DCNS.2017.19.2/bbandelow [PMID: 28867934]
-
National Institute for Health and Care Excellence. Generalised anxiety disorder and panic disorder in adults: management. NICE guideline [NG116]. 2019 (updated 2020). https://www.nice.org.uk/guidance/ng116
-
de Lijster JM, Dierckx B, Utens EM, et al. The Age of Onset of Anxiety Disorders. Can J Psychiatry. 2017;62(4):237-246. doi:10.1177/0706743716640757 [PMID: 27310233]
-
McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. 2011;45(8):1027-1035. doi:10.1016/j.jpsychires.2011.03.006 [PMID: 21439576]
-
Batelaan NM, Seldenrijk A, Bot M, van Balkom AJ, Penninx BW. Anxiety and new onset of cardiovascular disease: critical review and meta-analysis. Br J Psychiatry. 2016;208(3):223-231. doi:10.1192/bjp.bp.114.156554 [PMID: 26932485]
-
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097. doi:10.1001/archinte.166.10.1092 [PMID: 16717171]
-
Roy-Byrne P, Craske MG, Sullivan G, et al. Delivery of evidence-based treatment for multiple anxiety disorders in primary care: a randomized controlled trial. JAMA. 2010;303(19):1921-1928. doi:10.1001/jama.2010.608 [PMID: 20483971]
-
Tyrer P, Baldwin D. Generalised anxiety disorder. Lancet. 2006;368(9553):2156-2166. doi:10.1016/S0140-6736(06)69865-6 [PMID: 17174708]
-
Huffman JC, Pollack MH. Predicting panic disorder among patients with chest pain: an analysis of the literature. Psychosomatics. 2003;44(3):222-236. doi:10.1176/appi.psy.44.3.222 [PMID: 12724504]
-
Lader M. Benzodiazepines revisited—will we ever learn? Addiction. 2011;106(12):2086-2109. doi:10.1111/j.1360-0443.2011.03563.x [PMID: 21714826]
-
Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. 2018;212(5):279-286. doi:10.1192/bjp.2018.27 [PMID: 29587888]
-
Cuijpers P, Cristea IA, Karyotaki E, Reijnders M, Huibers MJ. How effective are cognitive behavior therapies for major depression and anxiety disorders? A meta-analytic update of the evidence. World Psychiatry. 2016;15(3):245-258. doi:10.1002/wps.20346 [PMID: 27717254]
-
Penninx BWJH. Anxiety disorders. Lancet. 2021;397(10277):914-927. doi:10.1016/S0140-6736(21)00359-7 [PMID: 33675836]
-
Shin LM, Liberzon I. The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology. 2010;35(1):169-191. doi:10.1038/npp.2009.83 [PMID: 19625997]
-
Nuss P. Anxiety disorders and GABA neurotransmission: a disturbance of modulation. Neuropsychiatr Dis Treat. 2015;11:165-175. doi:10.2147/NDT.S58841 [PMID: 25653526]
-
Charney DS. Neuroanatomical circuits modulating fear and anxiety behaviors. Acta Psychiatr Scand Suppl. 2003;(417):38-50. doi:10.1034/j.1600-0447.108.s417.3.x [PMID: 12950435]
Last Updated: 2026-01-09
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Always consult current guidelines and local protocols. This content does not replace clinical judgment or patient-specific assessment.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Basic Neuroanatomy and Neurotransmitter Systems
- Principles of Cognitive Behavioral Therapy
Differentials
Competing diagnoses and look-alikes to compare.
- Hyperthyroidism
- Pheochromocytoma
- Supraventricular Tachycardia
- Substance Withdrawal States
Consequences
Complications and downstream problems to keep in mind.
- Major Depressive Disorder
- Substance Use Disorders
- Cardiovascular Disease