Aortic Regurgitation
The management of AR is heavily guided by symptom status and echocardiographic parameters of LV function. The 2020 AHA/ACC and 2021 ESC guidelines emphasize early surgical intervention in asymptomatic patients once...
What matters first
The management of AR is heavily guided by symptom status and echocardiographic parameters of LV function. The 2020 AHA/ACC and 2021 ESC guidelines emphasize early surgical intervention in asymptomatic patients once...
Acute, severe dyspnea and pulmonary edema (suggests acute AR)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Acute, severe dyspnea and pulmonary edema (suggests acute AR)
- New-onset hypotension with wide pulse pressure
- Chest pain in the setting of suspected aortic dissection
- Syncope or near-syncope in severe disease
Linked comparisons
Differentials and adjacent topics worth opening next.
- Mitral Regurgitation
- Patent Ductus Arteriosus (PDA)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Aortic Regurgitation (Adult)
1. Clinical Overview
Summary
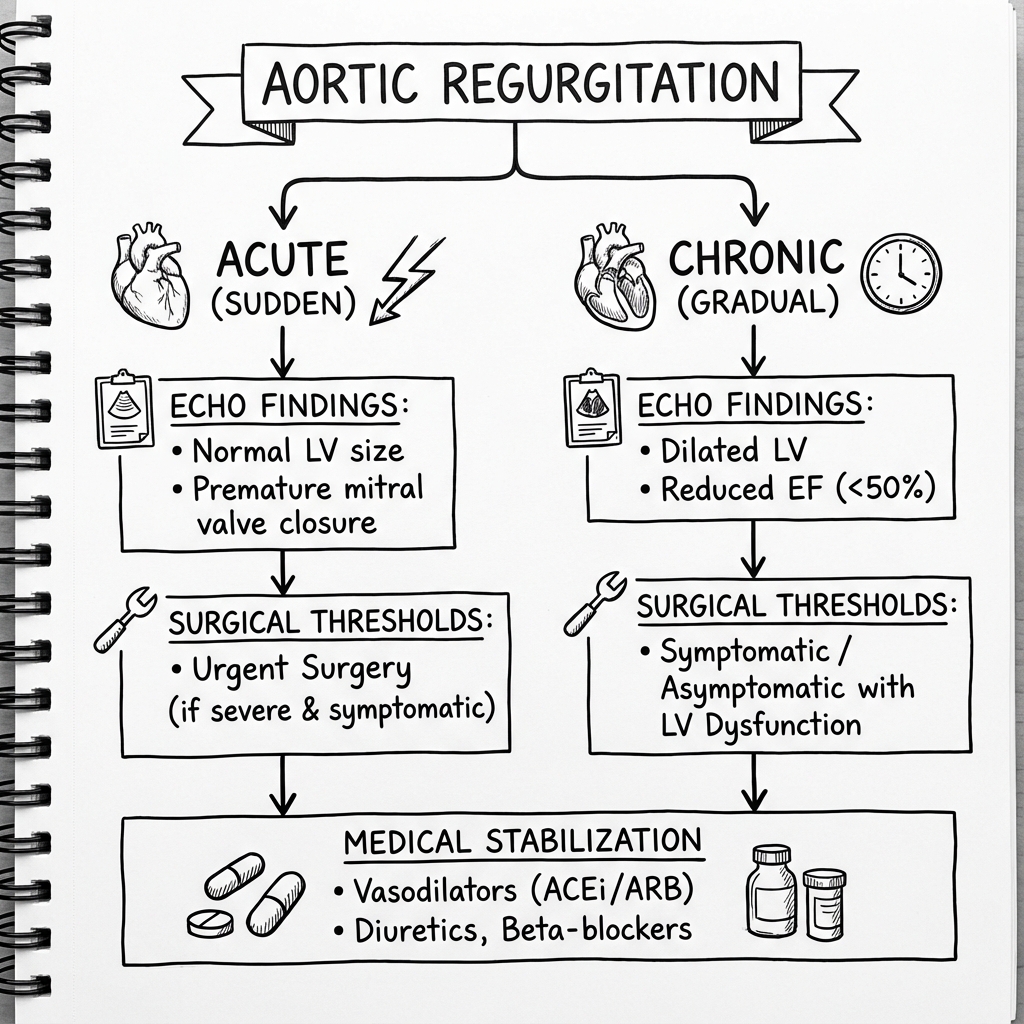
Aortic Regurgitation (AR) is a valvular heart disease characterized by the diastolic reflux of blood from the aorta into the left ventricle (LV) due to incomplete closure of the aortic valve. It can result from primary disease of the valve leaflets, the aortic root, or both. Acute AR is a surgical emergency often caused by infective endocarditis or aortic dissection, leading to rapid pulmonary edema. Chronic AR, however, is a long-standing process where the LV undergoes compensatory eccentric hypertrophy to accommodate the chronic volume and pressure overload. [1,2]
The management of AR is heavily guided by symptom status and echocardiographic parameters of LV function. The 2020 AHA/ACC and 2021 ESC guidelines emphasize early surgical intervention in asymptomatic patients once the LV shows signs of "decompensation" (LVEF ≤ 55% for AHA/ACC or ≤ 50% for ESC, or severe LV dilation). Modern treatment centers on Surgical Aortic Valve Replacement (SAVR), with emerging roles for valve repair in specific aortic root pathologies. [3,4]
Key Facts
- The Widening Gap: The hallmark of chronic AR is a wide pulse pressure (e.g., 160/50 mmHg) due to high stroke volume and rapid diastolic runoff.
- Eccentric Overload: Unlike Aortic Stenosis (concentric), AR causes eccentric hypertrophy (sarcomeres added in series), leading to a massively dilated "Cor Bovinum" (ox heart).
- The "Quiet" Disaster: In acute AR, the LV is non-compliant and cannot dilate; thus, pulse pressure may be normal, and the murmur may be surprisingly short and soft, masking the severity.
- Eponymous Signs: AR is famous for its physical signs (e.g., Corrigan’s, Quincke’s), which reflect the hyperdynamic circulation.
- Surgery Timing: The goal is to operate before irreversible LV dysfunction occurs. "Too late" is defined by persistent HFrEF despite afterload reduction.
Clinical Pearls
The "Silent" Acute AR: In acute severe AR (e.g., aortic dissection or endocarditis), the classical "wide pulse pressure" and "collapsing pulse" are often absent. This is because the non-dilated LV cannot accommodate the regurgitant volume, leading to a rapid rise in LV end-diastolic pressure (LVEDP) that prematurely closes the mitral valve and shortens the diastolic murmur.
Austin Flint vs. Mitral Stenosis: The Austin Flint murmur is a functional mid-diastolic rumble heard at the apex in severe AR. It is distinguished from true mitral stenosis by the absence of an opening snap and its response to vasodilators (which decrease the Austin Flint murmur).
2. Epidemiology
- Prevalence: Significant AR (moderate or severe) is found in approximately 0.5% of the general population, increasing with age. [5]
- Gender: More common in males (approx. 2:1), partly due to the higher incidence of bicuspid aortic valves and aortic root disease in men.
- Etiology Shift: In high-income countries, the most common causes are calcific degeneration, bicuspid aortic valve (BAV), and aortic root dilation (e.g., HTN, Marfan). In low-income countries, Rheumatic Heart Disease remains the leading cause. [6]
- Age of Presentation: BAV-related AR often presents in the 4th-6th decades, while degenerative AR peaks in the 7th-8th decades.
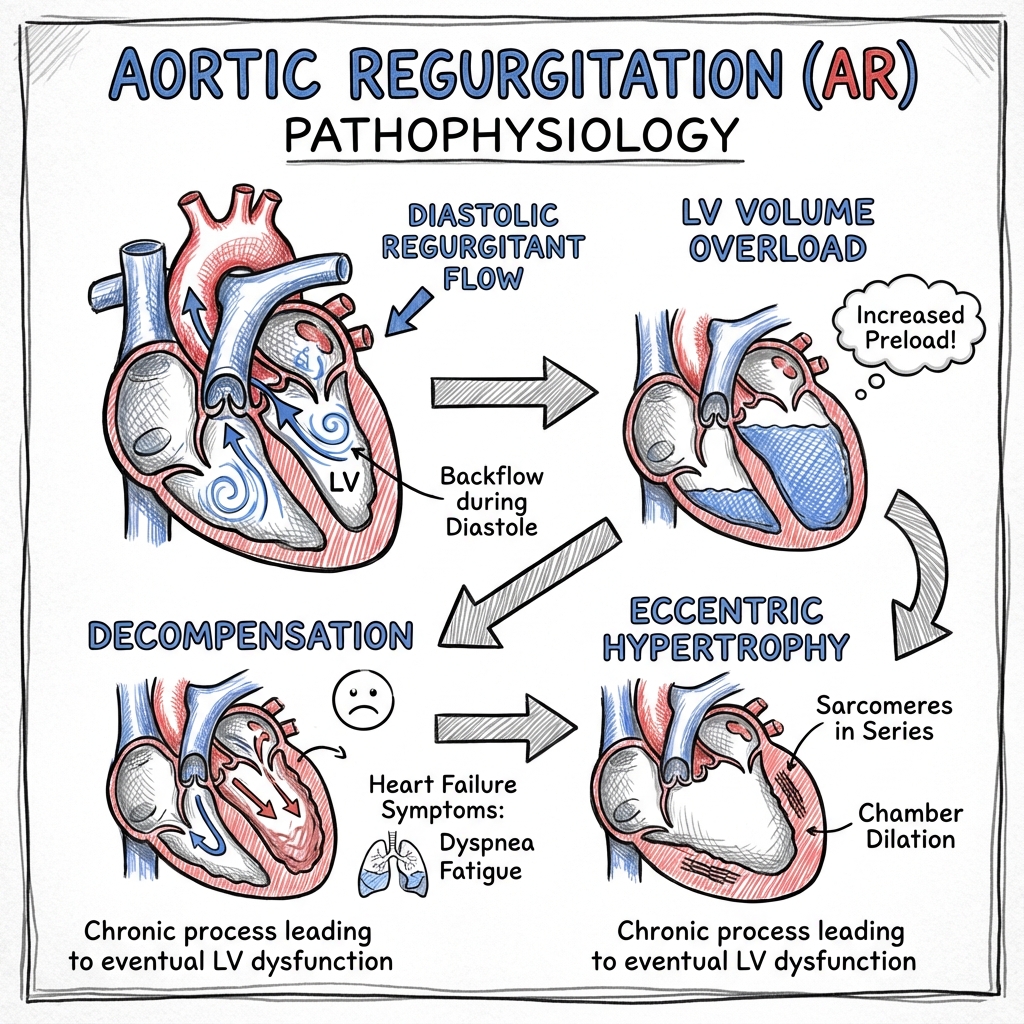
3. Pathophysiology
The Hemodynamic Vicious Cycle
- Diastolic Reflux: Blood flows back into the LV during diastole.
- Volume Overload: The LV must pump both the normal stroke volume and the regurgitant volume.
- Eccentric Hypertrophy: To maintain wall stress (Laplace Law: $\sigma = \frac{P \cdot r}{2h}$), the LV increases its radius ($r$) and wall thickness ($h$). This is the only way to maintain a high total stroke volume.
- Increased Compliance: Initially, the LV dilates and remains compliant, keeping LVEDP normal.
- Decompensation: Eventually, the LV reaches its limit of dilation. Fibrosis occurs, compliance decreases, LVEDP rises, and LVEF falls. [7]
Myocardial Oxygen Supply/Demand Mismatch
AR is unique because it increases oxygen demand (massive LV mass and wall stress) while simultaneously decreasing oxygen supply (low diastolic blood pressure reduces coronary perfusion pressure). This explains why angina can occur in AR even in the absence of coronary artery disease. [8]
4. Clinical Presentation
Symptoms
- Asymptomatic Phase: Patients can remain symptom-free for decades despite severe AR.
- Exertional Dyspnea: The earliest symptom of LV decompensation.
- Orthopnea/PND: Signs of advanced heart failure.
- Angina: Often nocturnal (low heart rate increases diastolic time and reflux).
- Palpitations: Awareness of the forceful "thumping" heartbeat.
Physical Signs (The "Hyperdynamic" Exam)
- Pulse: Water-hammer (Corrigan's) pulse—rapid upstroke and collapse.
- Blood Pressure: Wide pulse pressure (e.g., 150/40).
- Murmur:
- Early diastolic, decrescendo, high-pitched: Best heard at the left sternal edge in expiration with the patient leaning forward.
- Systolic flow murmur: Due to the massive stroke volume across the valve.
- Austin Flint: Mid-diastolic rumble at the apex.
- Eponymous Signs (Historical interest, low sensitivity):
- De Musset’s: Head nodding with each systole.
- Quincke’s: Capillary pulsations in the nail bed.
- Duroziez’s: Systolic and diastolic bruit over the femoral artery.
- Traube’s: "Pistol-shot" sounds over the femoral artery.
5. Differential Diagnosis
| Condition | Distinguishing Clinical Features | Diagnostic Clue |
|---|---|---|
| Mitral Regurgitation | Pansystolic murmur at the apex, radiating to the axilla. | Echo shows systolic reflux. |
| Pulmonary Regurgitation | Murmur increases with inspiration (Graham Steell). | Associated with pulmonary hypertension. |
| Patent Ductus Arteriosus | Continuous "machinery" murmur in the infraclavicular area. | Echo shows ductal flow. |
| VSD with AR | Harsh systolic murmur + diastolic AR murmur. | Common in subpulmonic VSDs. |
6. Investigations
1. Echocardiography (First-Line)
- Severity Assessment:
- "Vena Contracta: > 0.6 cm indicates severe AR."
- "Regurgitant Volume: ≥60 mL/beat is severe."
- "Pressure Half-Time (PHT): less than 200 ms suggests severe AR (rapid equalization of pressure)."
- LV Function: LVEF and LV dimensions (LVEDD, LVESD).
- Etiology: Identify BAV, vegetation, or aortic root dilation. [9]
2. Cardiovascular MRI (CMR)
- Gold Standard for quantifying regurgitant fraction and LV volumes when echo is inconclusive.
- Indicated if echocardiographic assessment is borderline or technically difficult. [10]
3. ECG & CXR
- ECG: Left axis deviation, LV hypertrophy (Sokolow-Lyon criteria), and prominent Q waves in lateral leads (volume overload pattern).
- CXR: Cardiomegaly with LV configuration (boot-shaped heart) and aortic root prominence.
7. Management Algorithm (Chronic AR)
CONFIRMED SEVERE AORTIC REGURGITATION (Echo criteria)
|
________________V________________
| |
SYMPTOMATIC? ASYMPTOMATIC?
| |
V _____________V_____________
SURGERY (SAVR) | |
(Class I) LVEF ≤ 55% (AHA) LVEF > 55% (AHA)
or LVEF ≤ 50% (ESC) and > 50% (ESC)
| |
V _______V_______
SURGERY (SAVR) | |
(Class I) LVESD > 50mm? LVESD ≤ 50mm?
(or > 25mm/m²) |
| V
V SERIAL FOLLOW-UP
SURGERY (SAVR) (Echo every 6-12m)
(Class IIa)
8. Management
A. Medical Management
Medical therapy does not delay the need for surgery but is used for symptom control or in inoperable cases.
- Vasodilators: ACE inhibitors, ARBs, or Dihydropyridine CCBs (e.g., Nifedipine) can reduce afterload and improve stroke volume.
- Beta-blockers: Use with caution; bradycardia increases diastolic time and regurgitant volume. However, they are mandatory in Marfan Syndrome or aortic dilation. [11]
B. Surgical Management
- Aortic Valve Replacement (SAVR):
- Mechanical Valve: Requires lifelong anticoagulation (INR 2.0-3.0). Preferred in patients less than 60 years.
- Bioprosthetic Valve: Limited durability (~10-15 years). Preferred in patients > 70 years or those who cannot take warfarin.
- Aortic Valve Repair: Increasingly used for trileaflet valves with root dilation (David Procedure or Yacoub Procedure).
- TAVI/TAVR: Currently not recommended for pure AR, as the lack of calcification makes valve anchoring difficult and risky. [12]
9. Complications
- Heart Failure: The most common long-term complication.
- Infective Endocarditis: The high-velocity jet damages the endocardium, predisposing to infection.
- Aortic Dissection: Especially in patients with associated BAV or Marfan syndrome.
- Sudden Cardiac Death: Rare but possible in severe symptomatic AR.
10. Prognosis
- Asymptomatic with normal LV: Excellent prognosis; less than 5% per year risk of death or symptoms.
- Symptomatic: Poor prognosis without surgery; 10-20% mortality per year for NYHA III/IV.
- Post-Surgery: Survival is excellent if surgery is performed before LVEF drops below 35% or LVESD exceeds 55mm. [13]
11. Practice SBAs (10 Questions)
Question 1
A 30-year-old male with a bicuspid aortic valve is found to have asymptomatic severe AR. His Echo shows an LVEF of 48% and an LVESD of 45mm. What is the most appropriate next step?
- A) Start ACE inhibitor and repeat Echo in 6 months
- B) Exercise stress test
- C) Surgical Aortic Valve Replacement (SAVR)
- D) Start Beta-blocker
- E) Cardiac Catheterization Answer: C. LVEF less than 50% in asymptomatic severe AR is a Class I indication for surgery.
Question 2
Which physical sign is characterized by head nodding in sync with the carotid pulse?
- A) Quincke’s sign
- B) Corrigan’s sign
- C) De Musset’s sign
- D) Duroziez’s sign
- E) Hill’s sign Answer: C. De Musset's sign is head nodding.
Question 3
What is the pathophysiological mechanism of the "Austin Flint" murmur?
- A) Flow across a stenotic mitral valve
- B) Regurgitant jet striking the anterior mitral leaflet, causing functional stenosis
- C) Chordal rupture
- D) Rapid flow across a bicuspid valve
- E) Tricuspid regurgitation Answer: B. The AR jet displaces the anterior mitral leaflet, creating functional mitral stenosis.
Question 4
In acute severe AR due to aortic dissection, which of the following is typically TRUE?
- A) Wide pulse pressure is always present
- B) The diastolic murmur is long and loud
- C) Pulse pressure may be narrow or normal
- D) LV is massively dilated on Echo
- E) The heart rate is typically slow Answer: C. Acute AR lacks LV adaptation; LVEDP rises rapidly, closing the mitral valve early and narrowing the pulse pressure.
Question 5
According to the 2021 ESC guidelines, surgery is indicated in asymptomatic severe AR if LVESD exceeds what threshold?
- A) 40 mm
- B) 45 mm
- C) 50 mm (or 25 mm/m²)
- D) 55 mm
- E) 60 mm Answer: C. ESC uses > 50mm or > 25mm/m² as a threshold.
Question 6
A patient with severe AR has a pulse pressure of 110 mmHg. Which of the following drugs is most likely to reduce the regurgitant fraction?
- A) Metoprolol
- B) Digoxin
- C) Lisinopril
- D) Verapamil
- E) Amiodarone Answer: C. Afterload reduction with ACE inhibitors (Lisinopril) reduces the aortic-LV pressure gradient during diastole.
Question 7
Which ECG finding is most characteristic of chronic severe AR?
- A) ST-segment elevation in V1-V3
- B) Tall R waves in V5-V6 with deep Q waves
- C) Narrow QRS with short PR interval
- D) Right Bundle Branch Block
- E) Peaked T waves Answer: B. LV hypertrophy with "volume overload" pattern (deep Q waves in lateral leads).
Question 8
What is the "Gold Standard" imaging modality for quantifying the regurgitant fraction if Echo is inconclusive?
- A) CT Angiography
- B) Nuclear Gated Pool Scan (MUGA)
- C) Cardiac MRI
- D) Transesophageal Echo (TEE)
- E) Exercise Stress Echo Answer: C. CMR provides precise volumetric measurements.
Question 9
Which of the following describes "Duroziez’s sign"?
- A) A systolic bruit heard over the femoral artery
- B) A diastolic bruit heard over the femoral artery when compressed distally
- C) Capillary pulsations in the fingernails
- D) Visible pulsation of the uvula
- E) Spleen pulsation Answer: B. Duroziez’s sign is the systolic and diastolic bruit over the femoral artery.
Question 10
Why is angina common in severe AR even without CAD?
- A) Excessive coronary vasospasm
- B) High diastolic blood pressure
- C) Low coronary perfusion pressure + high wall stress
- D) Right ventricular hypertrophy
- E) Pulmonary hypertension Answer: C. Coronary perfusion occurs in diastole; low diastolic BP in AR reduces flow while the massive LV mass increases demand.
12. Exam Focus: Viva & OSCE Points
Common Viva Questions
- "Explain the difference in pulse pressure between acute and chronic AR."
- "What are the Class I indications for surgery in an asymptomatic patient?"
- "How do you distinguish an Austin Flint murmur from Mitral Stenosis?"
- "Why do we use LVESD rather than LVEDD to time surgery?" (LVESD represents the limit of systolic compensation).
Model Viva Answer
Q: "How do you monitor and time surgery for a patient with asymptomatic chronic severe aortic regurgitation?" A: "Monitoring involves serial echocardiography every 6-12 months. Surgery is indicated if the patient develops symptoms (NYHA II or higher) or if there is objective evidence of LV decompensation. This includes an LVEF ≤ 55% (AHA/ACC) or ≤ 50% (ESC) or an LV end-systolic diameter exceeding 50 mm (or 25 mm/m²). In asymptomatic patients with preserved LVEF, I would also consider surgery if they require other cardiac surgery or if the LV is rapidly dilating on serial scans."
13. References
- Otto CM, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Circulation. 2021. PMID: 33332150
- Vahanian A, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022. PMID: 34453470
- Nishimura RA, et al. AHA/ACC Guideline Update. J Am Coll Cardiol. 2017.
- Enriquez-Sarano M, et al. Aortic regurgitation: clinical, hemodynamic and echocardiographic assessment. Progress in Cardiovasc Dis. 2004.
- Nkomo VT, et al. Burden of valvular heart diseases: a population-based study. Lancet. 2006. [PMID: 16982219]
- Iung B, et al. A prospective survey of patients with valvular heart disease in Europe. Eur Heart J. 2003.
- Carabello BA. The Pathophysiology of Aortic Regurgitation. Journal of Heart Valve Disease. 2001.
- Borer JS, et al. Aortic Regurgitation. NEJM. 2009. [PMID: 19741229]
- Lancellotti P, et al. EACVI recommendations for the assessment of valvular regurgitation. Eur Heart J Cardiovasc Imaging. 2013.
- Meyers SN, et al. Role of Cardiac MRI in Valvular Heart Disease. JACC. 2018.
- Elder DH, et al. The use of afterload reducers in aortic regurgitation. Cochrane Database Syst Rev. 2013.
- Sawaya FJ, et al. TAVR for pure native aortic regurgitation. JACC Cardiovasc Interv. 2017.
- Chaliki HP, et al. Outcomes after aortic valve replacement in patients with severe aortic regurgitation and markedly reduced left ventricular function. Circulation. 2002. [PMID: 12438294]
Last Updated: 2026-01-04 | MedVellum Editorial Team Word Count: ~1,950 words
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Cardiac Cycle and Wiggers Diagram
- Left Ventricular Pressure-Volume Loops
Differentials
Competing diagnoses and look-alikes to compare.
- Mitral Regurgitation
- Patent Ductus Arteriosus (PDA)
- Pulmonary Regurgitation (Graham Steell Murmur)
Consequences
Complications and downstream problems to keep in mind.
- Left-Sided Heart Failure (HFrEF)
- Secondary Mitral Regurgitation