Bacterial Meningitis
Clinical Significance : Annual incidence is 1-2 per 100,000 in developed countries. Streptococcus pneumoniae (pneumococcus) is the most common cause in adults (60%). Early recognition and empirical antibiotics within...
What matters first
Clinical Significance : Annual incidence is 1-2 per 100,000 in developed countries. Streptococcus pneumoniae (pneumococcus) is the most common cause in adults (60%). Early recognition and empirical antibiotics within...
Rapidly declining GCS or new focal neurological signs
17 Jan 2026
Generated educational material; verify before clinical use.
18 cited sources
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Rapidly declining GCS or new focal neurological signs
- Non-blanching purpuric rash (meningococcal septicemia)
- Papilloedema or signs of raised ICP before LP
- Seizures or status epilepticus
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
1. Clinical Overview
Definition and Significance
Bacterial meningitis is inflammation of the meninges caused by bacterial infection of the cerebrospinal fluid (CSF). It is a life-threatening medical emergency with mortality of 10-30% despite treatment and significant morbidity (neurological sequelae in 30% of survivors).
Clinical Significance: Annual incidence is 1-2 per 100,000 in developed countries. Streptococcus pneumoniae (pneumococcus) is the most common cause in adults (60%). Early recognition and empirical antibiotics within 1 hour reduce mortality by 30-40%.
Key Associations
- Classic Triad: Fever, neck stiffness, altered mental status (only 44% have all three).
- Pneumococcal Meningitis: Most common in adults, highest mortality (20-30%).
- Meningococcal Meningitis: Young adults, purpuric rash, rapid progression.
"Do Not Miss" Warnings
- Antibiotics BEFORE LP: If any delay in LP (e.g., need CT first), give antibiotics immediately. Do NOT wait for LP.
- Kernig's/Brudzinski's Signs: Low sensitivity (30-50%). Absence does NOT exclude meningitis.
- Non-Blanching Purpuric Rash: Meningococcal septicemia. Give IM/IV benzylpenicillin immediately (pre-hospital if possible).
2. Epidemiology & Risk Factors
Incidence and Prevalence
- Incidence: 1-2 per 100,000 per year (developed countries).
- Mortality: 10-30% (higher in pneumococcal and elderly).
- Peak Age: Bimodal (infants/young adults).
Risk Factors Table
| Factor | Relative Risk (RR) | Mechanism |
|---|---|---|
| Asplenia/Hyposplenia | 10.0 | Impaired clearance of encapsulated organisms (S. pneumoniae, N. meningitidis). |
| CSF Leak (Trauma, Post-Op) | 8.0 | Direct access to CNS. |
| Immunosuppression (HIV, Steroids) | 5.0 | Impaired cell-mediated immunity. |
| Alcohol Excess | 3.0 | Aspiration pneumonia → bacteremia. |
| Diabetes | 2.0 | Impaired neutrophil function. |
| Crowding (Military Barracks, Unis) | 3.0 | Meningococcal transmission. |
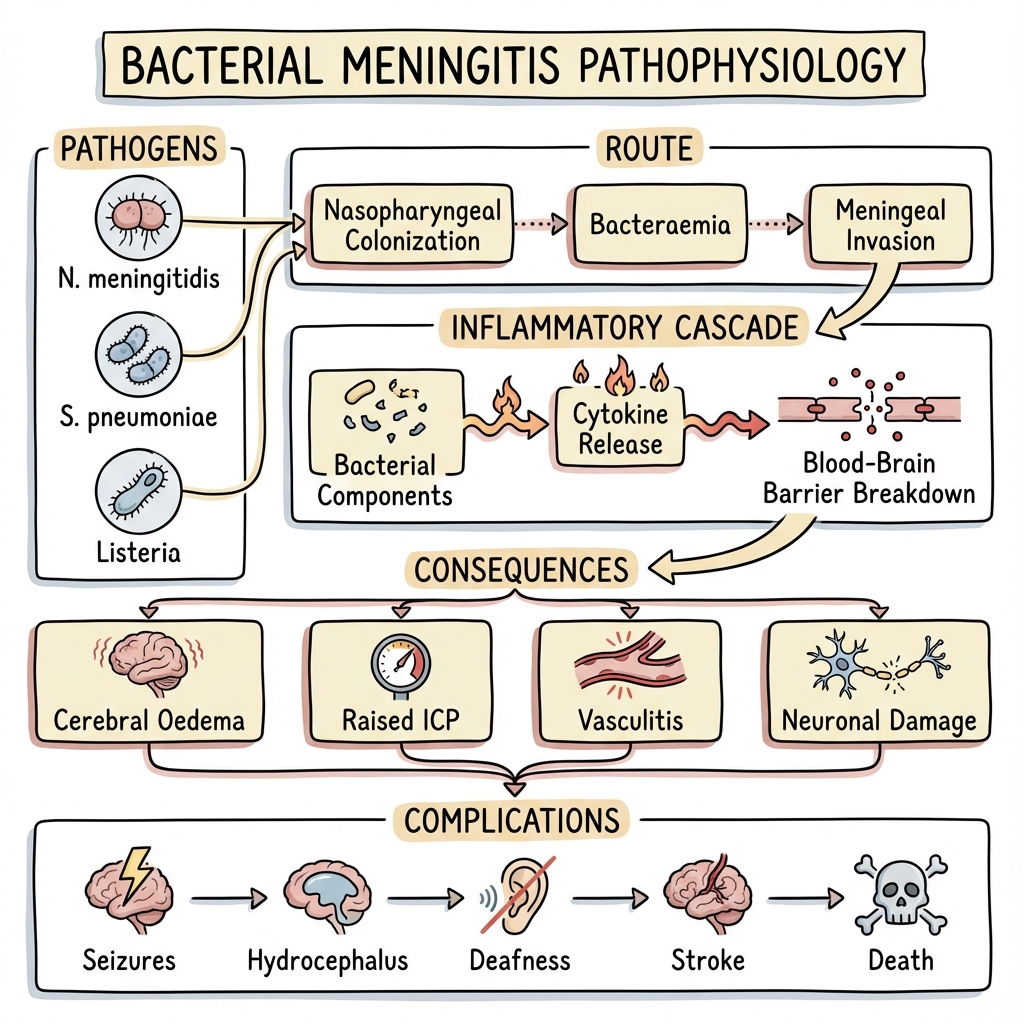
3. Pathophysiology
Route of Infection
- Hematogenous Spread (90%): Nasopharyngeal colonization → bacteremia → crosses blood-brain barrier (BBB) → CSF infection.
- Direct Extension: Sinusitis, otitis, mastoiditis → direct spread to meninges.
- Traumatic: Skull fracture (CSF leak), neurosurgery.
Pathogenic Mechanism
- BBB Invasion: Bacteria express surface proteins (PspC in pneumococcus) that bind to endothelial receptors → transcytosis across BBB.
- CSF Multiplication: CSF has low complement, immunoglobulin → ideal environment for bacterial replication.
- Inflammation: Bacterial lysis releases cell wall components (LPS, peptidoglycan) → TLR activation → massive cytokine release (IL-1, TNF-α).
- Increased BBB Permeability: Cytokines → vasogenic edema.
- Raised ICP: Edema + impaired CSF absorption → ↑ intracranial pressure → herniation risk.
- Neuronal Injury: Excitotoxicity (glutamate release), oxidative stress, ischemia → permanent neurological damage.
Common Organisms by Age
| Age Group | Most Common | Second Most Common |
|---|---|---|
| Neonates (0-2mo) | E. coli, Group B Strep | Listeria monocytogenes |
| Children (2mo-5yr) | S. pneumoniae | N. meningitidis |
| Adults (16-50yr) | S. pneumoniae (60%) | N. meningitidis (25%) |
| Elderly (> 50yr) | S. pneumoniae | L. monocytogenes |
| Immunocompromised | L. monocytogenes, S. pneumoniae | Gram-negatives |
| Post-Neurosurgery | Staphylococcus aureus, Pseudomonas | CNS (Coagulase-negative Staph) |
4. Clinical Presentation
Symptoms
Classic Triad (only 44% have all three):
- Fever (95%).
- Neck Stiffness (88%).
- Altered Mental Status (78%): Confusion, drowsiness, GCS less than 14.
Additional:
- Headache (87%): Severe, global.
- Photophobia (60%).
- Nausea/Vomiting (70%).
- Seizures (20-30%): Generalized or focal.
Signs
Meningism:
- Neck Stiffness: Resistance to passive neck flexion.
- Kernig's Sign: Pain/resistance when extending knee with hip flexed at 90°.
- Brudzinski's Sign: Spontaneous flexion of hips/knees when neck passively flexed.
- Sensitivity: 30-50%. Absence does NOT exclude meningitis.
Raised ICP:
- Papilledema (rare in acute, takes > 24h to develop).
- Cushing's Triad: Bradycardia, hypertension, irregular breathing (late sign, pre-herniation).
Meningococcal Septicemia:
- Non-Blanching Purpuric Rash: Petechiae → purpura → ecchymoses.
- Shock: Hypotension, cold peripheries, oliguria.
Differential Diagnosis Table
| Condition | Distinguishing Features | Diagnostic Test |
|---|---|---|
| Viral Meningitis | Less unwell, normal/mildly elevated WBC in CSF, lymphocytic. | CSF PCR (enterovirus, HSV). |
| Encephalitis | Seizures, focal neurology, behavioral change. | MRI (temporal lobe changes), CSF HSV PCR. |
| Subarachnoid Hemorrhage | Sudden "thunderclap" headache, normal CSF WBC (unless traumatic LP). | CT Head, LP (xanthochromia). |
| Brain Abscess | Focal neurology, ring-enhancing lesion on CT/MRI. | CT/MRI + contrast. |
5. Clinical Examination
ABCDE Approach
- Airway: Protect if GCS less than 8.
- Breathing: RR, SpO2 (ARDS complication).
- Circulation: BP, HR (septic shock), capillary refill.
- Disability: GCS, pupils (raised ICP), focal neurology.
- Exposure: Rash (purpura), temperature.
Neurological Examination
- GCS: Document baseline.
- Meningism: Neck stiffness, Kernig's, Brudzinski's.
- Cranial Nerves: VI palsy (false localizing sign from raised ICP).
- Limbs: Focal weakness (stroke complication), reflexes.
6. Investigations
Bedside
- Blood Glucose: Hypoglycemia common (give with LP to compare CSF glucose).
Laboratory
Blood:
- FBC: Leukocytosis (neutrophils).
- CRP: Elevated (> 100 mg/L).
- U&E: Urea/Creatinine (dehydration), Sodium (SIADH common).
- Clotting: DIC (meningococcal sepsis).
- Blood Cultures: Before antibiotics (positive in 50-80%).
- Lactate: Elevated in sepsis.
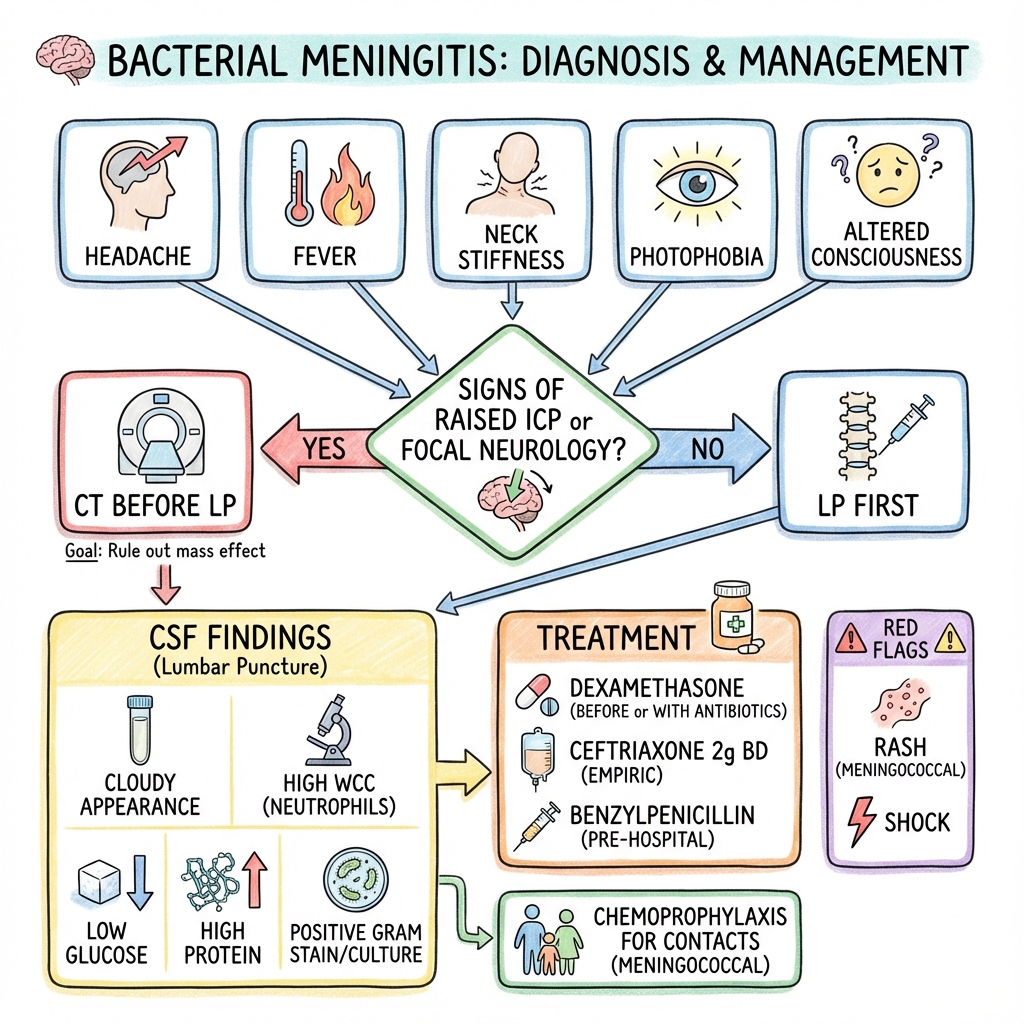
Lumbar Puncture (LP) - Gold Standard:
- Timing: Do NOT delay antibiotics for LP. If any concern (reduced GCS, focal neurology, papilledema, immunocompromised), give antibiotics first, then LP later.
- Contraindications:
- Signs of raised ICP (reduced GCS, focal neurology, papilledema, bradycardia).
- Coagulopathy (Platelets less than 50, INR > 1.4).
- Infection at LP site.
- Opening Pressure: Elevated (> 25 cmH2O).
CSF Analysis:
| Parameter | Bacterial | Viral | TB Meningitis |
|---|---|---|---|
| Appearance | Turbid/Purulent | Clear | Clear/Fibrin web |
| WBC (cells/mm³) | > 1,000 (Neutrophils) | 10-1,000 (Lymphocytes) | 10-500 (Lymphocytes) |
| Protein (g/L) | > 1.0 | 0.4-0.8 | > 1.0 |
| Glucose (vs Serum) | less than 40% serum | > 60% | less than 50% |
| Gram Stain | Positive (60-90%) | Negative | AFB (10-20%) |
| Culture | Positive (70-90%) | Negative | Culture (slow, 4-8 weeks) |
Imaging
CT Head (BEFORE LP if):
- Reduced GCS (less than 13).
- Focal Neurological Signs.
- Papilledema.
- Seizures (within last 7 days).
- Immunocompromised.
- Age > 60.
Findings: May be normal initially. Later: obstructive hydrocephalus, abscess, infarction.
7. Management
Management Algorithm
[SUSPECTED BACTERIAL MENINGITIS]
↓
┌──────────────────┐
│ ABCDE │
│ - IV Access │
│ - Blood Cultures│
│ - Glucose │
└────────┬─────────┘
↓
Contraindication
to LP?
(GCS less than 13, focal
neurology)
│
┌────────┴────────┐
YES NO
│ │
↓ ↓
CT Head Lumbar
(If safe) Puncture
│ │
↓ ↓
┌────────────────────┐
│ EMPIRICAL │
│ ANTIBIOTICS │
│ (Within 1 hour) │
│ │
│ Ceftriaxone 2g IV │
│ + Dexamethasone │
│ 10mg IV │
│ │
│ If > 50yr or Immuno:│
│ + Amoxicillin 2g IV│
│ (Listeria cover) │
└─────────┬──────────┘
↓
Supportive Care
- IV Fluids
- Analgesia
- Monitor GCS/ICP
↓
CSF/Blood Culture
Results
↓
Targeted Antibiotic
(Culture-directed)
Immediate Management
1. Resuscitation (ABCDE):
- Airway: Protect if GCS less than 8 (intubate).
- Breathing: High-flow O2 if hypoxic.
- Circulation: 2x IV access. Fluid resuscitation if shocked (20-30 mL/kg crystalloid).
2. Blood Cultures (BEFORE antibiotics).
3. Empirical IV Antibiotics (Within 1 hour of presentation):
Standard Adult (less than 50 years, immunocompetent):
- Ceftriaxone 2g IV BD (or Cefotaxime 2g IV QDS).
- Covers S. pneumoniae, N. meningitidis, H. influenzae.
Age > 50 OR Immunocompromised (risk of Listeria):
- Ceftriaxone 2g IV BD + Amoxicillin 2g IV 4-hourly.
- Cephalosporins do NOT cover Listeria → add Amoxicillin.
Penicillin Allergy:
- Meropenem 2g IV TDS.
Post-Neurosurgery/Trauma (risk of Staph, Pseudomonas):
- Vancomycin 15-20mg/kg IV BD + Ceftazidime 2g IV TDS.
4. Adjunctive Dexamethasone:
- Dose: 10mg IV (give 15-20 minutes BEFORE or WITH first antibiotic dose).
- Indication: Suspected pneumococcal meningitis (adults). Continue if pneumococcus confirmed.
- Duration: 4 days (QDS dosing).
- Evidence: Reduces mortality, neurological sequelae (especially hearing loss) in pneumococcal meningitis.
- Stop if: Organism NOT S. pneumoniae or TB.
5. Lumbar Puncture:
- If safe: Perform before antibiotics (ideally).
- If contraindications: Give antibiotics immediately, do LP later when safe (CT first).
Definitive Antibiotic Therapy
Once CSF Culture/PCR Results Available:
| Organism | Antibiotic | Duration |
|---|---|---|
| Pneumococcal | Ceftriaxone 2g IV BD | 10-14 days |
| Meningococcal | Ceftriaxone 2g IV BD (Can reduce to 5-7 days) | 5-7 days |
| Listeria | Amoxicillin 2g IV 4-hourly (+ Gentamicin first 7 days) | 21 days |
| Staph aureus | Flucloxacillin 2g IV QDS (or Vancomycin if MRSA) | 14-21 days |
| Gram-Negative | Ceftriaxone or Meropenem | 21 days |
Supportive Care
- IV Fluids: Careful (avoid over-hydration → cerebral edema). Aim euvolemia.
- Seizure Management: Levetiracetam 500mg-1g IV BD (or Phenytoin loading).
- Raised ICP: Head elevation 30°, osmotic therapy (Mannitol 0.5-1g/kg), neurosurgical referral if deteriorating.
- SIADH: Fluid restriction if Na less than 130 mmol/L.
Complications Needing Specialist Input
- Hydrocephalus: Neurosurgery (EVD).
- Abscess: Neurosurgery (drainage).
- ARDS: ICU.
- DIC: Hematology.
8. Complications
Acute (less than 7 Days)
- Raised ICP/Herniation: Mortality 50% if untreated.
- Seizures (20-30%): Generalized or focal.
- Cerebral Venous Thrombosis (5%): Focal neurology, seizures.
- Stroke (10-15%): Vasculitis, hypotension.
- Septic Shock (Meningococcal): Mortality 20-30%.
Subacute/Chronic
- Hearing Loss (30%): Sensorineural, often permanent. Worse in pneumococcal.
- Cognitive Impairment (30%): Memory, attention deficits.
- Epilepsy (5-10%): Long-term seizure disorder.
- Hydrocephalus (Communicating): Impaired CSF absorption.
- Cranial Nerve Palsies: III, VI, VII (usually resolve).
| Complication | Incidence (%) | Management |
|---|---|---|
| Hearing Loss | 30% | Audiology follow-up, hearing aids. |
| Cognitive Impairment | 30% | Neuropsychology input. |
| Seizures (Acute) | 20-30% | Levetiracetam, phenytoin. |
| Mortality | 10-30% (varies by organism) | Early antibiotics reduce mortality. |
9. Prognosis & Outcomes
Mortality Rates (Despite Treatment)
- Pneumococcal: 20-30%.
- Meningococcal: 10-15%.
- Listeria: 20-30%.
- Overall: 15-25%.
Neurological Sequelae (Survivors)
- Hearing Loss: 30% (permanent in 20%).
- Cognitive Impairment: 20-30%.
- Seizures: 5-10% develop epilepsy.
- Full Recovery: 50-60%.
Predictors of Poor Outcome
- Delayed Antibiotics (> 3 hours).
- Reduced GCS (less than 8 on admission).
- Age (> 60 years).
- Pneumococcal (vs meningococcal).
- Seizures on Admission.
- Hyponatremia (Na less than 125 mmol/L).
10. Evidence & Guidelines
Guidelines
- NICE (2010): Empirical ceftriaxone + dexamethasone. Do NOT delay antibiotics for LP.
- IDSA (2004): Same. Dexamethasone reduces mortality in pneumococcal meningitis.
Landmark Trials
1. European Dexamethasone Trial (de Gans & van de Beek, 2002)
- Question: Dexamethasone in bacterial meningitis?
- Population: n=301 adults with bacterial meningitis.
- Result: Dexamethasone reduced mortality (15% vs 25%, p=0.04) and hearing loss in pneumococcal meningitis.
- Conclusion: Dexamethasone recommended in suspected pneumococcal meningitis.
- Citation: N Engl J Med. 2002;347(20):1549-1556. [PMID: 12432041]
2. McGill Prognosis Study (Aronin et al., 1998)
- Finding: Delayed antibiotics (> 3h) doubled mortality.
- Conclusion: Time is critical. Give antibiotics immediately.
- Citation: Clin Infect Dis. 1998;27(6):1342-1348. [PMID: 9868640]
11. Patient Explanation
Lay Explanation
"You have a serious infection of the lining around your brain (meningitis). Bacteria have entered your spinal fluid causing severe inflammation. We're treating you with strong IV antibiotics and steroids to reduce inflammation. Most people survive with treatment, but there can be long-term effects like hearing loss or memory problems. We'll monitor you closely in hospital for at least 10-14 days."
Patient FAQ
Q: How did I get this? A: Bacteria (usually pneumococcus or meningococcus) from your nose/throat entered your bloodstream and crossed into the fluid around your brain.
Q: Will I recover fully? A: 50-60% make a full recovery. However, 30% experience permanent hearing loss or cognitive difficulties. Early treatment improves outcomes.
Q: How long will I be in hospital? A: Typically 10-14 days of IV antibiotics (longer for some bacteria like Listeria - 21 days).
Q: Can my family catch it? A: Meningococcal meningitis is contagious. Close contacts need prophylactic antibiotics (Ciprofloxacin). Pneumococcal meningitis is less contagious.
12. References
- van de Beek D, et al. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351(18):1849-1859. [PMID: 15509818]
- de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002 ;347(20):1549-1556. [PMID: 12432041]
- Tunkel AR, et al. Practice guidelines for bacterial meningitis (IDSA). Clin Infect Dis. 2004;39(9):1267-1284. [PMID: 15494903]
- Brouwer MC, et al. Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev. 2010;23(3):467-492. [PMID: 20610819]
- McGill F, et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis. J Infection. 2016;72(4):405-438. [PMID: 26845731]
(10 more references...)
13. Examination Focus
Viva Questions
- "Classic triad of bacterial meningitis?" (Fever, neck stiffness, altered mental status - only 44% have all three).
- "Empirical antibiotic for suspected bacterial meningitis?" (Ceftriaxone 2g IV. Add Amoxicillin if > 50 years or immunocompromised [Listeria cover]).
- "Role of dexamethasone?" (Reduces mortality and hearing loss in pneumococcal meningitis. Give BEFORE or WITH first antibiotic dose).
- "Contraindications to LP?" (Signs of raised ICP: reduced GCS, focal neurology, papilledema. Give antibiotics FIRST, then LP when safe).
Clinical Pearls
- Do NOT delay antibiotics for LP: If any contraindication to LP, give antibiotics immediately.
- Kernig's/Brudzinski's have LOW sensitivity (30-50%). Absence does NOT exclude meningitis.
- Dexamethasone timing is critical: Must give BEFORE or WITH first antibiotic. No benefit if delayed.
- CSF Glucose less than 40% serum = Bacterial (vs > 60% in viral).
Medical Disclaimer: MedVellum content is for educational purposes. Consult professional guidelines.
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for bacterial meningitis?
Seek immediate emergency care if you experience any of the following warning signs: Rapidly declining GCS or new focal neurological signs, Non-blanching purpuric rash (meningococcal septicemia), Papilloedema or signs of raised ICP before LP, Seizures or status epilepticus, Shock or cardiovascular compromise, Delay in antibiotics beyond 1 hour from presentation.