Bell's Palsy (Adult)
Bell's palsy is the most common cause of acute unilateral peripheral facial paralysis, accounting for approximately 60-7... MRCP exam preparation.
What matters first
Bell's palsy is the most common cause of acute unilateral peripheral facial paralysis, accounting for approximately 60-7... MRCP exam preparation.
Bilateral facial weakness (consider GBS, Lyme disease, sarcoidosis, bilateral Bell's)
9 Jan 2025
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Bilateral facial weakness (consider GBS, Lyme disease, sarcoidosis, bilateral Bell's)
- Forehead sparing (UMN lesion - stroke, intracranial mass)
- Vesicles in external auditory canal or pinna (Ramsay Hunt syndrome - VZV)
- Progressive weakness over weeks (tumour - acoustic neuroma, parotid malignancy)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Ramsay Hunt Syndrome
- Lyme Disease
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Bell's Palsy (Adult)
1. Topic Overview
Clinical Summary
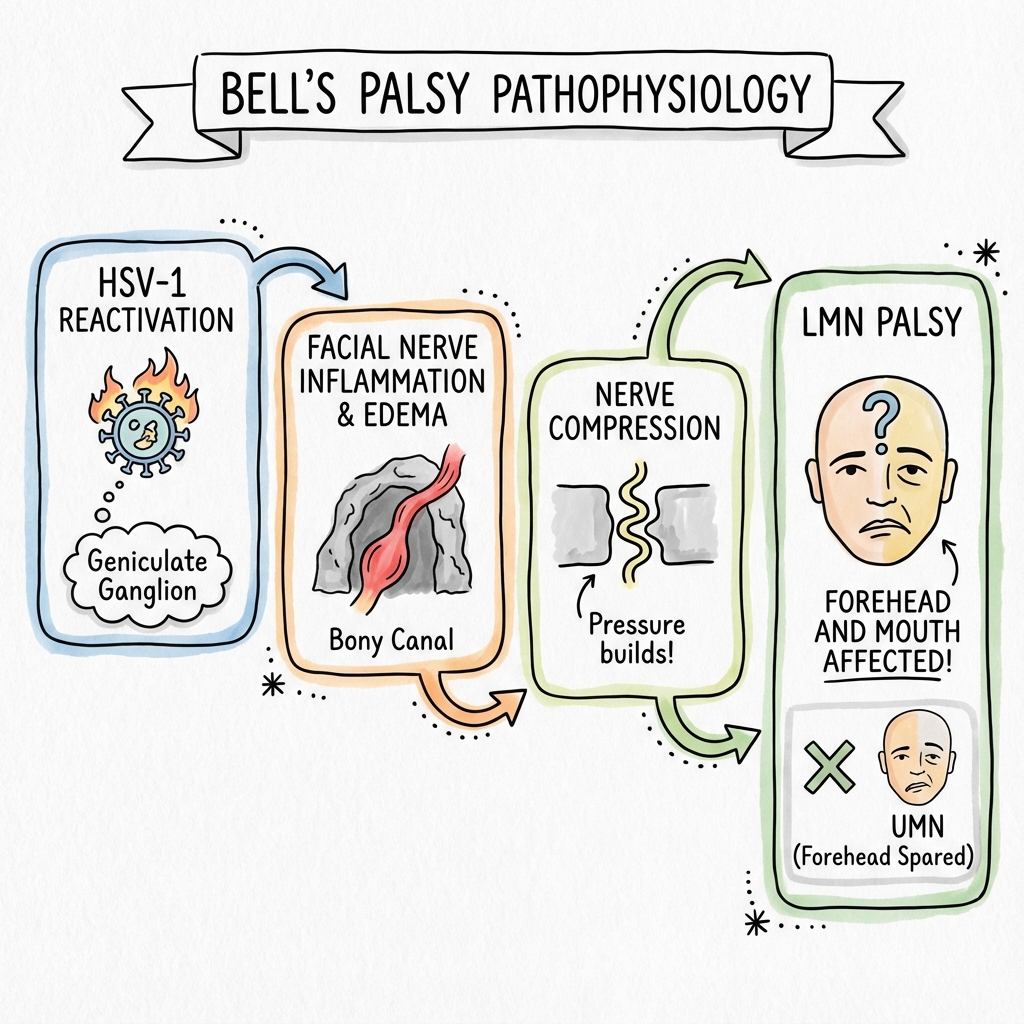
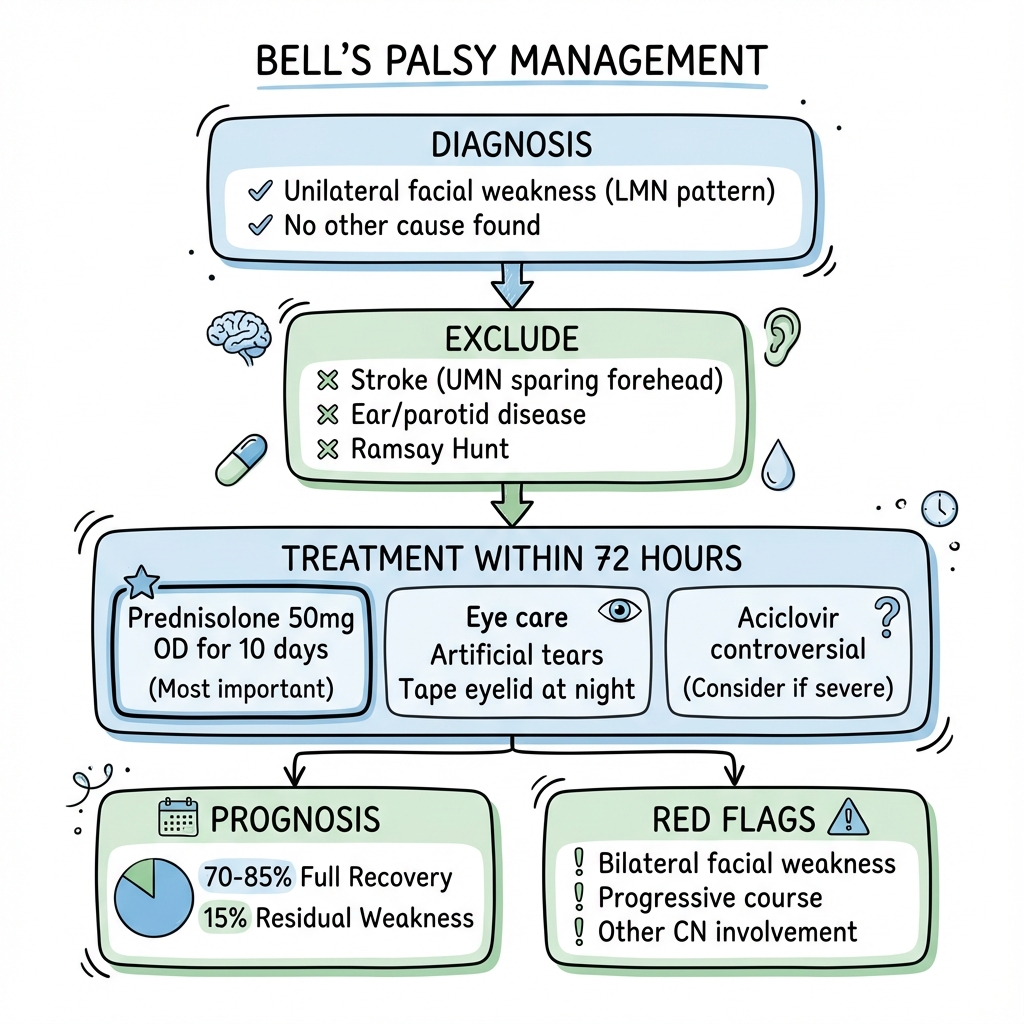
Bell's palsy is the most common cause of acute unilateral peripheral facial paralysis, accounting for approximately 60-75% of all cases of acute facial palsy. [1,2] It is characterised by sudden-onset lower motor neuron (LMN) weakness affecting all muscle groups on one side of the face, including the forehead musculature. The condition represents a diagnosis of exclusion, made after ruling out identifiable secondary causes such as Ramsay Hunt syndrome, Lyme disease, stroke, and neoplastic lesions. [3]
The underlying aetiology remains incompletely understood, but substantial evidence implicates herpes simplex virus type 1 (HSV-1) reactivation within the geniculate ganglion, leading to inflammation, oedema, and subsequent compression of the facial nerve within the narrow confines of the fallopian canal in the temporal bone. [4,5] This inflammatory process results in demyelination and, in severe cases, axonal degeneration with Wallerian degeneration.
Prognosis is generally favourable, with approximately 70% of patients achieving complete recovery without treatment. Early initiation of corticosteroid therapy within 72 hours of symptom onset significantly improves outcomes, increasing complete recovery rates to 85-95%. [6,7] The role of antiviral agents remains controversial; current high-quality evidence does not support their routine use in Bell's palsy, though they are indicated in Ramsay Hunt syndrome. [8]
Key Facts
| Parameter | Value |
|---|---|
| Definition | Acute idiopathic unilateral lower motor neuron facial paralysis |
| Incidence | 20-30 per 100,000 per year [1] |
| Lifetime risk | 1 in 60 individuals |
| Peak age | 15-45 years (rare in children less than 10 years) |
| Sex distribution | Equal male:female ratio |
| Key clinical feature | LMN pattern: forehead IS affected (complete hemifacial weakness) |
| Bilateral cases | less than 1% (consider alternative diagnosis: GBS, Lyme, sarcoidosis) |
| First-line treatment | Prednisolone 50-60mg daily within 72 hours |
| Complete recovery (untreated) | ~70% [6] |
| Complete recovery (with steroids) | 85-95% [6,7] |
| Recurrence rate | 7-12% lifetime [9] |
Clinical Pearl: The Forehead Test
"Can You Wrinkle Your Forehead?": This single clinical observation distinguishes Bell's palsy from stroke in the majority of cases. In Bell's palsy (LMN lesion), the forehead IS affected - the patient cannot wrinkle the forehead or raise the eyebrow on the affected side. In stroke (UMN lesion), the forehead is SPARED due to bilateral cortical representation of the upper face. This is the critical bedside distinction that guides further investigation.
Clinical Pearl: Vesicles = Not Bell's Palsy
Check the Ear: If vesicles are present in the external auditory canal, on the pinna, or on the soft palate, the diagnosis is Ramsay Hunt syndrome (herpes zoster oticus) caused by VZV reactivation, NOT Bell's palsy. This distinction is crucial as Ramsay Hunt syndrome requires antiviral therapy (aciclovir or valaciclovir) in addition to corticosteroids and carries a worse prognosis. [10]
Clinical Pearl: Eye Care is Non-Negotiable
Prevent Corneal Catastrophe: The inability to fully close the eyelid (lagophthalmos) leads to corneal exposure, desiccation, and risk of exposure keratopathy and corneal ulceration. Aggressive eye protection with artificial tears, lubricating ointment, and nocturnal taping is essential and should be initiated immediately. A corneal ulcer is a preventable iatrogenic complication. [11]
Why This Matters Clinically
Bell's palsy presents commonly in primary care and emergency departments, often causing significant patient anxiety due to fears of stroke. Rapid, accurate clinical assessment can distinguish Bell's palsy from stroke and other serious pathology. Early corticosteroid treatment substantially improves outcomes but must be initiated within 72 hours. Proper eye care prevents sight-threatening complications. While prognosis is generally excellent, incomplete recovery causes substantial psychological distress, social anxiety, and functional impairment affecting communication and facial expression.
2. Epidemiology
Incidence and Prevalence
Bell's palsy is the most common acute mononeuropathy and the most frequent cause of unilateral facial paralysis worldwide. [1,2]
| Epidemiological Parameter | Value | Reference |
|---|---|---|
| Annual incidence | 20-30 per 100,000 population | [1,2] |
| Lifetime risk | 1.6% (approximately 1 in 60) | [1] |
| Peak incidence age | 15-45 years | [2] |
| Rare age group | less than 10 years (alternative diagnosis more likely) | [2] |
| Elderly incidence | Slightly increased after age 70 | [9] |
| Pregnancy incidence | 45 per 100,000 (3x general population) | [12] |
| Diabetic incidence | 29-36 per 100,000 (2-4x general population) | [13] |
Demographics
| Factor | Details |
|---|---|
| Age | Bimodal peak: 15-45 years and > 65 years; rare less than 10 years |
| Sex | Equal male:female (some studies suggest slight female preponderance) |
| Laterality | Right = Left (equal distribution); strictly unilateral |
| Bilateral presentation | less than 1% - strongly suggests alternative diagnosis |
| Recurrence | 7-12% lifetime recurrence (may be ipsilateral or contralateral) [9] |
| Family history | 4-14% have affected first-degree relative (suggests genetic predisposition) [14] |
| Seasonal variation | Some studies suggest winter peak; others show no clear pattern |
Risk Factors
Established Risk Factors (Evidence-Based):
| Risk Factor | Relative Risk | Mechanism | Reference |
|---|---|---|---|
| Diabetes mellitus | 2-4x increased | Microangiopathy, impaired nerve regeneration | [13] |
| Pregnancy | 3x increased (especially 3rd trimester/postpartum) | Immunomodulation, fluid retention, oedema | [12] |
| Upper respiratory infection | 2x increased (preceding viral illness) | Viral reactivation trigger | [4] |
| Hypertension | 1.5-2x increased | Microvascular disease | [13] |
| Family history | Variable | Anatomical predisposition (narrow fallopian canal) | [14] |
Associated Conditions:
- Immunocompromised states (HIV, organ transplant recipients)
- Pre-eclampsia and eclampsia (in pregnancy-associated cases)
- Hypothyroidism
- Multiple sclerosis (demyelinating lesions affecting CN VII)
NOT Risk Factors (Common Misconceptions):
- Cold exposure or draughts (no evidence)
- Stress alone (no direct evidence)
- Dental procedures (unless direct nerve trauma)
3. Pathophysiology
Aetiology: The Viral Hypothesis
The predominant theory for Bell's palsy pathogenesis involves reactivation of latent herpes simplex virus type 1 (HSV-1) from the geniculate ganglion. [4,5] This hypothesis is supported by:
- PCR evidence: HSV-1 DNA detected in endoneurial fluid of Bell's palsy patients during surgical decompression [4]
- Serological studies: Elevated HSV-1 antibody titres in affected patients
- Anatomical studies: HSV-1 latency demonstrated in human geniculate ganglia
- Clinical parallels: Similar pathophysiology to herpes labialis reactivation
However, it is important to note that viral DNA detection does not prove causation, and the viral hypothesis remains unproven. Alternative or contributing factors may include:
- Autoimmune mechanisms (molecular mimicry)
- Ischaemic injury to the facial nerve
- Hereditary predisposition (anatomically narrow fallopian canal)
Anatomical Basis: The Facial Nerve Course
Understanding the facial nerve anatomy is essential for comprehending the clinical features and prognostic implications of Bell's palsy.
Facial Nerve Segments:
| Segment | Location | Length | Clinical Significance |
|---|---|---|---|
| 1. Intracranial | Pontomedullary junction to IAM | 23-24mm | Rarely affected in Bell's |
| 2. Meatal (IAM) | Internal acoustic meatus | 8-10mm | Accompanied by CN VIII |
| 3. Labyrinthine | Fundus IAM to geniculate ganglion | 3-5mm | NARROWEST segment (0.68mm diameter) |
| 4. Geniculate ganglion | At first genu | - | Site of HSV-1 latency; greater petrosal nerve origin |
| 5. Tympanic | Geniculate to second genu | 8-11mm | Horizontal; runs above oval window |
| 6. Mastoid | Second genu to stylomastoid foramen | 10-14mm | Vertical; stapedius and chorda tympani branches |
| 7. Extratemporal | Stylomastoid foramen through parotid | Variable | Divides into terminal branches |
Key Anatomical Point: The labyrinthine segment is the narrowest portion of the fallopian canal (bony facial canal), making it the most vulnerable to compression from inflammatory oedema. This explains why Bell's palsy causes complete hemifacial weakness regardless of the site of inflammation within the canal.
Pathophysiological Sequence
BELL'S PALSY: PATHOPHYSIOLOGICAL CASCADE
Step 1: VIRAL REACTIVATION
HSV-1 reactivation in geniculate ganglion
(Trigger: immunosuppression, stress, infection)
↓
Step 2: INFLAMMATION
Inflammatory response with lymphocytic infiltration
Cytokine release (TNF-α, IL-1β, IL-6)
Oedema of nerve and surrounding tissues
↓
Step 3: COMPRESSION
Swollen nerve compressed within rigid fallopian canal
Especially at labyrinthine segment (narrowest point)
Venous congestion → further oedema (vicious cycle)
↓
Step 4: NERVE INJURY
Mild cases: Neuropraxia (conduction block, myelin preserved)
Moderate: Axonotmesis (axon damage, myelin disruption)
Severe: Neurotmesis (complete nerve disruption)
↓
Step 5: CLINICAL MANIFESTATION
Acute facial weakness (hours to 48 hours)
Additional features: altered taste, hyperacusis, decreased lacrimation
↓
Step 6: RECOVERY (Variable)
Neuropraxia: Complete recovery in 3-8 weeks
Axonotmesis: Recovery over months; may have synkinesis
Neurotmesis: Poor recovery; aberrant regeneration
Nerve Injury Classification (Sunderland/Seddon)
| Seddon | Sunderland | Pathology | Recovery | Bell's Palsy Correlation |
|---|---|---|---|---|
| Neuropraxia | Grade I | Myelin damage only; axon intact | Complete; weeks | Mild Bell's (HB I-II) |
| Axonotmesis | Grade II | Axon disrupted; endoneurium intact | Good; months | Moderate Bell's (HB III-IV) |
| Axonotmesis | Grade III | Endoneurium disrupted | Incomplete; synkinesis | Severe Bell's (HB IV-V) |
| Axonotmesis | Grade IV | Perineurium disrupted | Poor; surgery may help | Very severe (HB V-VI) |
| Neurotmesis | Grade V | Complete nerve transection | None without surgery | Not typical of Bell's |
Facial Nerve Functions: Clinical Correlates
The facial nerve carries multiple functional components, explaining the varied symptoms in Bell's palsy:
| Component | Function | Clinical Deficit in Bell's Palsy |
|---|---|---|
| Motor (Branchiomotor) | Facial expression muscles | Hemifacial weakness |
| Motor (Branchiomotor) | Stapedius muscle | Hyperacusis (sounds seem louder) |
| Parasympathetic | Lacrimal gland (via greater petrosal) | Decreased lacrimation (dry eye) |
| Parasympathetic | Submandibular/sublingual glands (via chorda tympani) | Decreased salivation |
| Sensory (Special) | Taste anterior 2/3 tongue (chorda tympani) | Dysgeusia/ageusia |
| Sensory (General) | Small area behind ear | Hypoaesthesia (uncommon) |
Motor Branch Distribution (Mnemonic: "Two Zebras Bit My Cat")
| Branch | Muscles Supplied | Clinical Test |
|---|---|---|
| Temporal | Frontalis, orbicularis oculi (upper) | Raise eyebrows, close eyes |
| Zygomatic | Orbicularis oculi (lower) | Close eyes tightly |
| Buccal | Buccinator, orbicularis oris (upper) | Puff cheeks, smile |
| Mandibular (marginal) | Lower lip depressors | Show lower teeth |
| Cervical | Platysma | Tense neck |
4. Clinical Presentation
Typical Presentation
The classic presentation of Bell's palsy is acute-onset unilateral facial weakness developing over hours to 1-2 days, reaching maximum severity within 72 hours. [1,2]
Cardinal Symptoms:
| Symptom | Frequency | Description |
|---|---|---|
| Facial weakness | 100% | Unilateral weakness affecting entire hemifacial |
| Inability to close eye | 100% | Lagophthalmos with corneal exposure |
| Drooping of mouth | 100% | Asymmetric smile, drooling |
| Forehead weakness | 100% | Cannot wrinkle forehead, raise eyebrow (LMN sign) |
| Post-auricular pain | 50-60% | May precede weakness by 1-2 days [15] |
| Dysgeusia/ageusia | 30-50% | Altered or absent taste (anterior 2/3 tongue) |
| Hyperacusis | 15-30% | Sounds seem abnormally loud (stapedius weakness) |
| Decreased lacrimation | 10-20% | Paradoxically may have epiphora (overflow tearing) |
| Facial numbness sensation | 30-50% | Subjective; sensory testing normal |
| Ear pain | 25% | Otalgia around mastoid region |
Symptom Onset Characteristics:
- Onset typically overnight or upon waking
- Maximal weakness reached within 72 hours (usually 24-48 hours)
- Progression beyond 3 weeks suggests alternative diagnosis
- May be preceded by viral prodrome (URTI symptoms)
Clinical Signs
Inspection at Rest:
- Facial asymmetry (affected side droops)
- Widened palpebral fissure (lagophthalmos)
- Flattened nasolabial fold
- Drooping mouth corner
- Smoothed forehead furrows
Facial Motor Examination:
| Test | Instruction | Normal Response | Bell's Palsy Finding |
|---|---|---|---|
| Frontalis | "Raise your eyebrows" | Symmetrical forehead wrinkling | Absent/weak on affected side |
| Corrugator | "Frown/bring eyebrows together" | Symmetrical frown | Weak on affected side |
| Orbicularis oculi | "Close your eyes tightly" | Strong symmetrical closure | Weak/incomplete closure; Bell's phenomenon |
| Nasalis | "Wrinkle your nose" | Symmetrical nose wrinkling | Weak on affected side |
| Orbicularis oris | "Purse your lips/whistle" | Symmetrical lip pursing | Weak; cannot whistle |
| Buccinator | "Puff out your cheeks" | Cheeks inflate symmetrically | Air escapes on affected side |
| Smile/show teeth | "Smile showing teeth" | Symmetrical smile | Asymmetric; mouth deviates to normal side |
| Mentalis | "Show bottom teeth" | Chin elevation | Weak on affected side |
| Platysma | "Clench jaw and tense neck" | Platysma bands visible | Absent on affected side |
Bell's Phenomenon:
When attempting to close the eyes, the eyeball on the affected side rotates upward and outward (normal protective reflex), but because the eyelid cannot close, this movement becomes visible. A positive Bell's phenomenon indicates intact superior rectus function and provides some corneal protection.
Otoscopic Examination: Critical Step
ALWAYS examine the external auditory canal and pinna:
| Finding | Diagnosis | Management Implication |
|---|---|---|
| Normal | Supports Bell's palsy | Standard treatment |
| Vesicles in EAC/pinna | Ramsay Hunt syndrome (VZV) | Add antivirals; worse prognosis |
| Vesicles on soft palate | Ramsay Hunt syndrome | Add antivirals |
| Purulent discharge | Otitis media/externa | Treat infection; may be secondary cause |
| Cholesteatoma debris | Cholesteatoma | Urgent ENT referral; CT temporal bones |
| Mass lesion | Tumour (glomus, carcinoma) | Urgent ENT/imaging |
Red Flag Features
[!CAUTION] Red Flags Requiring Further Investigation:
Forehead SPARED (UMN Pattern):
- Suggests central lesion (stroke, tumour)
- Urgent stroke pathway if acute onset with other neurological signs
Vesicles Present:
- Ramsay Hunt syndrome (VZV)
- Add aciclovir 800mg 5x daily for 7 days
- Worse prognosis than Bell's (complete recovery 50-70%)
Bilateral Facial Weakness:
- Guillain-Barre syndrome (ascending weakness, areflexia)
- Lyme disease (especially if endemic area, tick exposure)
- Sarcoidosis (Heerfordt syndrome: uveitis, parotid enlargement, fever)
- Bilateral Bell's (rare; diagnosis of exclusion)
Progressive Weakness Over Weeks:
- Tumour (acoustic neuroma, facial nerve schwannoma, parotid malignancy)
- Cholesteatoma (associated hearing loss, otorrhoea)
- Requires MRI internal auditory meati and parotid
No Recovery by 3-4 Months:
- Consider misdiagnosis
- MRI to exclude tumour
- Refer to neurology/ENT
Recurrent Episodes:
- Melkersson-Rosenthal syndrome (facial palsy, fissured tongue, lip swelling)
- Tumour
- Investigate with MRI
Other Cranial Nerve Involvement:
- Brainstem lesion (stroke, demyelination, tumour)
- Skull base pathology (nasopharyngeal carcinoma, meningitis)
- Requires urgent imaging
Limb Weakness, Sensory Symptoms, Ataxia:
- Guillain-Barre syndrome
- Multiple sclerosis
- Brainstem stroke
- Urgent neurological assessment
5. Clinical Examination
Structured Examination Approach
Introduction and Consent:
- Introduce yourself, confirm patient identity
- Explain examination
- Position patient sitting upright, good lighting, face fully visible
Observation (Before Touching):
- Facial asymmetry at rest
- Blink rate and symmetry
- Spontaneous facial movements
- Palpebral fissure size comparison
- Nasolabial fold depth
- Presence of any skin lesions, vesicles, or swelling
Systematic Facial Nerve Motor Examination:
| Test | Command | What to Observe |
|---|---|---|
| 1. Frontalis | "Look up at the ceiling without moving your head" | Forehead wrinkling symmetry |
| 2. Corrugator | "Frown for me" | Eyebrow approximation |
| 3. Orbicularis oculi | "Close your eyes gently, now as tightly as possible" | Lid closure, eyelash burying, Bell's phenomenon |
| 4. Procerus/Nasalis | "Scrunch up your nose" | Nose wrinkling |
| 5. Levator labii | "Show me your top teeth" | Upper lip elevation |
| 6. Orbicularis oris | "Purse your lips like you're going to whistle" | Lip pursing symmetry |
| 7. Buccinator | "Puff out your cheeks and hold it" | Cheek inflation, air leak |
| 8. Risorius/Zygomaticus | "Give me a big smile" | Smile symmetry, nasolabial fold |
| 9. Depressor anguli oris | "Turn the corners of your mouth down" | Lower mouth movement |
| 10. Mentalis | "Show me your bottom teeth" | Chin movement, mentalis contraction |
| 11. Platysma | "Clench your teeth and tense your neck" | Platysma bands |
Essential Additional Examinations:
| Examination | Technique | Purpose |
|---|---|---|
| Ear examination | Otoscopy of EAC and pinna | Exclude vesicles (Ramsay Hunt), cholesteatoma, mass |
| Hearing assessment | Whispered voice, Rinne/Weber | Detect associated hearing loss |
| Parotid palpation | Bimanual palpation | Exclude parotid mass |
| Other cranial nerves | Complete CN II-XII | Exclude multiple CN involvement |
| Upper/lower limb neurology | Power, reflexes, sensation | Exclude GBS, stroke, MS |
| Skin examination | Inspect for erythema migrans, vesicles | Lyme disease, VZV |
House-Brackmann Facial Nerve Grading System
The House-Brackmann (HB) scale is the most widely used system for grading facial nerve function. [16] It provides a standardised method for documenting severity and tracking recovery.
| Grade | Descriptor | Characteristics | Forehead Motion | Eye Closure | Mouth Movement |
|---|---|---|---|---|---|
| I | Normal | Normal facial function in all areas | Normal | Complete | Normal |
| II | Mild dysfunction | Slight weakness noticeable on close inspection; slight synkinesis possible | Moderate-to-good | Complete with minimal effort | Slight asymmetry |
| III | Moderate dysfunction | Obvious but not disfiguring asymmetry; noticeable synkinesis, contracture, or hemifacial spasm | Slight-to-moderate | Complete with effort | Slightly weak with maximum effort |
| IV | Moderately severe dysfunction | Obvious weakness and/or disfiguring asymmetry | None | Incomplete | Asymmetric with maximum effort |
| V | Severe dysfunction | Barely perceptible motion | None | Incomplete | Slight movement |
| VI | Total paralysis | No movement | None | None | None |
Clinical Application of House-Brackmann:
- Document at presentation (baseline)
- Repeat at follow-up (track recovery)
- HB I-II at presentation = excellent prognosis
- HB V-VI at presentation = higher risk of incomplete recovery
- Useful for communication between clinicians
- Required for clinical trials and outcome studies
Sunnybrook Facial Grading System
For more detailed assessment, particularly in research and rehabilitation settings, the Sunnybrook system provides a composite score (0-100) evaluating:
- Resting symmetry
- Symmetry of voluntary movement
- Synkinesis
Special Clinical Tests
| Test | Method | Significance |
|---|---|---|
| Schirmer's test | Filter paper in lower fornix; measure wetting after 5 min | less than 10mm suggests reduced lacrimation (greater petrosal involvement) |
| Stapedial reflex | Impedance audiometry | Absent if mastoid segment affected |
| Taste testing | Apply sweet/salt/sour to anterior 2/3 tongue | Abnormal if chorda tympani affected |
| Salivary flow | Rarely performed clinically | Reduced if chorda tympani affected |
6. Differential Diagnosis
Critical Differential: UMN vs LMN Facial Weakness
| Feature | LMN Lesion (Bell's Palsy) | UMN Lesion (Stroke) |
|---|---|---|
| Forehead | AFFECTED (weak) | SPARED (normal) |
| Eyebrow raising | Weak/absent | Normal |
| Eye closure | Weak/incomplete | May be mildly weak |
| Lower face | Weak | Weak |
| Bell's phenomenon | Present (visible eye roll) | Not visible (eye closes) |
| Anatomical reason | Single LMN to all muscles | Upper face has bilateral cortical innervation |
| Other CNS signs | Absent | Usually present (limb weakness, dysphasia, etc.) |
Anatomical Explanation: The upper facial muscles (frontalis, orbicularis oculi) receive bilateral cortical innervation - both the ipsilateral and contralateral motor cortex send fibres to the facial nucleus for these muscles. Therefore, a unilateral UMN lesion (stroke) leaves upper facial function relatively preserved because the intact contralateral cortex continues to supply these muscles. In contrast, an LMN lesion (Bell's palsy) affects the final common pathway, eliminating all motor supply to the ipsilateral facial muscles.
Comprehensive Differential Diagnosis
Infectious Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Ramsay Hunt syndrome (VZV) | Vesicles in EAC/pinna; severe pain; worse prognosis | Clinical; VZV serology if needed | Aciclovir 800mg 5x/day + prednisolone |
| Lyme disease | Tick exposure; erythema migrans; endemic area; may be bilateral | Lyme serology (ELISA, Western blot) | Doxycycline 100mg BD 14-21 days |
| Otitis media (acute/chronic) | Ear pain, discharge, hearing loss, fever | Otoscopy; CT if complicated | Antibiotics; may need surgery |
| Mastoiditis | Post-auricular swelling, pain, fever, proptosis of pinna | CT temporal bones | IV antibiotics; mastoidectomy |
| HIV | Risk factors; may present at seroconversion | HIV serology | Antiretroviral therapy |
| TB meningitis | Chronic meningitis; other CN involvement | CSF analysis; TB testing | Anti-TB therapy |
Neoplastic Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Acoustic neuroma (vestibular schwannoma) | Progressive; hearing loss; tinnitus; unsteadiness | MRI IAMs with gadolinium | Observation/surgery/stereotactic radiosurgery |
| Facial nerve schwannoma | Progressive facial weakness; may have normal hearing | MRI | Surgery |
| Parotid malignancy | Parotid mass; pain; rapid progression | CT/MRI parotid; FNA/biopsy | Surgery + radiotherapy |
| Cholesteatoma | Otorrhoea; hearing loss; chronic ear disease | Otoscopy; CT temporal bones | Surgery (mastoidectomy) |
| Nasopharyngeal carcinoma | Epistaxis; nasal obstruction; other CN involvement | Nasendoscopy; MRI; biopsy | Chemoradiotherapy |
| Skull base metastases | Known primary malignancy; multiple CN palsies | MRI brain/skull base; CT | Depends on primary |
Inflammatory/Autoimmune Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Guillain-Barre syndrome | Ascending weakness; bilateral facial weakness; areflexia | Nerve conduction studies; CSF (albuminocytologic dissociation) | IVIg or plasmapheresis |
| Sarcoidosis | Bilateral facial palsy; Heerfordt syndrome (uveitis, parotid swelling, fever) | CXR; serum ACE; biopsy | Corticosteroids |
| Multiple sclerosis | Other demyelinating signs; young adult | MRI brain/spine; CSF (oligoclonal bands) | Disease-modifying therapy |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy; fissured tongue; facial/lip oedema | Clinical diagnosis | Corticosteroids; surgical decompression |
| Sjogren's syndrome | Dry eyes; dry mouth; arthralgia | Anti-Ro/La; lip biopsy | Symptomatic; DMARDs |
Vascular Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Stroke (pontine) | Forehead spared (UMN pattern); other neurological deficits | CT/MRI brain; vascular imaging | Stroke pathway |
| Brainstem infarction | Multiple CN involvement; long tract signs; ataxia | MRI brain | Stroke pathway |
Traumatic Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Temporal bone fracture | History of head trauma; Battle's sign; haemotympanum | CT temporal bones (high resolution) | Observation vs. surgical exploration |
| Iatrogenic (surgical) | Following parotid, mastoid, or skull base surgery | Clinical context | Expectant; possible repair |
| Birth trauma | Neonatal; forceps delivery | Clinical | Usually recovers spontaneously |
Other Causes:
| Condition | Key Features | Investigation | Treatment |
|---|---|---|---|
| Diabetes mellitus | Known diabetic; higher incidence; may have worse recovery | HbA1c | Optimise glycaemic control |
| Pregnancy | Third trimester or postpartum | Clinical context | Prednisolone safe in pregnancy |
| Moebius syndrome | Congenital; bilateral facial and abducens palsy; facial diplegia | Clinical/genetic | Supportive |
7. Investigations
Bedside Investigations (First-Line)
Bell's palsy is a clinical diagnosis. In typical presentations, no investigations are required. [3]
| Investigation | Purpose | When to Perform |
|---|---|---|
| Clinical examination | Confirm LMN pattern; exclude alternative causes | All patients |
| Otoscopy | Exclude vesicles (Ramsay Hunt), cholesteatoma, mass | All patients |
| Blood glucose/HbA1c | Identify diabetes (prognostic; increased risk) | All patients |
| Blood pressure | Screen for hypertension; stroke risk assessment | All patients |
| Pregnancy test | If relevant; affects management | Women of childbearing age |
Laboratory Tests (Selective)
| Test | Indication | Expected Finding |
|---|---|---|
| Full blood count | Suspected infection, malignancy | Usually normal in Bell's |
| ESR/CRP | Suspected inflammatory/infectious cause | Normal in Bell's |
| Lyme serology (ELISA, Western blot) | Endemic area; tick exposure; bilateral palsy; erythema migrans | Positive in Lyme disease |
| VZV serology | Suspected Ramsay Hunt without visible vesicles | IgM positive (acute) |
| HIV serology | Risk factors; recurrent or atypical presentation | Positive in HIV-related |
| Serum ACE | Suspected sarcoidosis | Elevated in sarcoidosis |
| HbA1c | Screen for diabetes | > 48 mmol/mol diagnostic |
| Autoimmune panel | Suspected autoimmune cause | Variable |
Electrodiagnostic Studies
| Test | Timing | Findings | Prognostic Value |
|---|---|---|---|
| Electroneuronography (ENoG) | 3-14 days post-onset | Measures compound muscle action potential; compares sides | > 90% degeneration by day 14 = poor prognosis; less than 90% = good prognosis [17] |
| Electromyography (EMG) | > 2-3 weeks post-onset | Fibrillation potentials indicate denervation; polyphasic potentials indicate reinnervation | Presence of motor unit potentials suggests recovery potential |
| Needle EMG | Follow-up if no recovery | Voluntary motor unit activity indicates intact motor units | Useful in severe cases (HB V-VI) |
Clinical Utility of Electrodiagnostic Testing:
- Not routinely required for typical Bell's palsy
- Consider if complete paralysis (HB VI) at presentation
- Helpful for prognostication in severe cases
- ENoG most useful between days 3-14
- EMG useful after 2-3 weeks to assess denervation and early reinnervation
Imaging
| Modality | Indication | Findings |
|---|---|---|
| MRI brain and IAMs with gadolinium | No recovery by 3-4 months; progressive course; recurrent episodes; suspicion of tumour | Enhancing facial nerve (normal in Bell's); acoustic neuroma; facial nerve schwannoma; cholesteatoma |
| CT temporal bones | Suspected cholesteatoma; temporal bone fracture; mastoiditis | Bony erosion; fracture line; opacification |
| CT/MRI parotid | Parotid mass; suspected parotid malignancy | Mass lesion |
| MRI brain | Suspected stroke; demyelination; brainstem lesion | Infarct; demyelinating plaques; mass lesion |
Key Point: Routine imaging is NOT indicated in typical Bell's palsy. Reserve imaging for atypical features, no recovery, or progressive course.
Diagnostic Criteria Summary
Bell's palsy is a diagnosis of exclusion requiring:
- Acute onset (maximum weakness within 72 hours)
- Unilateral LMN facial weakness (forehead involved)
- No identifiable cause on history and examination
- Absence of red flag features
8. Management
Management Algorithm
BELL'S PALSY: MANAGEMENT ALGORITHM
PRESENTATION: Acute unilateral facial weakness
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 1: CONFIRM DIAGNOSIS │
│ │
│ • LMN pattern (forehead affected)? YES → Likely Bell's palsy │
│ • Forehead spared? YES → Consider stroke (UMN) → Stroke │
│ pathway │
│ • Vesicles visible? YES → Ramsay Hunt → Add antivirals │
│ • Bilateral weakness? YES → GBS/Lyme/Sarcoid → Investigate │
│ • Progressive over weeks? YES → Tumour → MRI urgently │
│ • Other cranial nerve involvement? YES → Brainstem lesion → Imaging │
└──────────────────────────────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 2: CORTICOSTEROIDS (START WITHIN 72 HOURS) │
│ │
│ FIRST-LINE REGIMEN: │
│ • Prednisolone 50mg once daily for 10 days │
│ OR │
│ • Prednisolone 60mg once daily for 5 days, then taper over 5 days │
│ │
│ EVIDENCE: NNT = 9 for complete recovery [6,7] │
│ • Complete recovery: 94% (steroids) vs 81.6% (placebo) at 9 months │
│ • Benefit greatest if started within 72 hours of onset │
│ │
│ CONTRAINDICATIONS (relative): │
│ • Active peptic ulcer disease │
│ • Uncontrolled diabetes (still treat; monitor glucose) │
│ • Active tuberculosis or systemic infection │
│ • Psychosis │
│ │
│ PREGNANCY: Prednisolone is safe; benefits outweigh risks │
└──────────────────────────────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 3: ANTIVIRALS - NOT ROUTINELY RECOMMENDED FOR BELL'S PALSY │
│ │
│ COCHRANE REVIEW (2019): No significant benefit of antivirals alone or │
│ combined with steroids compared to steroids alone [8] │
│ │
│ CURRENT EVIDENCE: │
│ • Antivirals alone: No benefit │
│ • Antivirals + steroids: No additional benefit over steroids alone │
│ │
│ ⚠ EXCEPTION: RAMSAY HUNT SYNDROME (vesicles present) │
│ • Aciclovir 800mg 5 times daily for 7 days │
│ OR │
│ • Valaciclovir 1000mg 3 times daily for 7 days │
│ • PLUS prednisolone (as above) │
│ │
│ SEVERE BELL'S PALSY (HB V-VI)? │
│ • Some guidelines suggest considering antivirals + steroids │
│ • Evidence weak; discuss risks/benefits with patient │
└──────────────────────────────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 4: EYE CARE (ESSENTIAL - DO NOT OMIT) │
│ │
│ GOAL: Prevent exposure keratopathy and corneal ulceration │
│ │
│ DAY: │
│ • Artificial tears (carmellose 0.5% or hypromellose 0.3%) │
│ • Apply every 1-2 hours while awake │
│ • Preservative-free preferred if using frequently │
│ │
│ NIGHT: │
│ • Lubricating eye ointment (Lacri-Lube or similar) │
│ • Tape eyelid closed with micropore tape if incomplete closure │
│ • Consider moisture chamber/swimming goggles │
│ │
│ ADDITIONAL MEASURES: │
│ • Protective glasses when outdoors (wind, dust) │
│ • Avoid air conditioning directly on face │
│ │
│ ⚠ RED FLAG - REFER OPHTHALMOLOGY URGENTLY IF: │
│ • Red eye │
│ • Eye pain │
│ • Photophobia │
│ • Visual disturbance │
│ • Suspected corneal ulcer │
└──────────────────────────────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 5: PATIENT EDUCATION AND SAFETY NETTING │
│ │
│ REASSURANCE: │
│ • This is NOT a stroke │
│ • Most people (85-95%) make a complete or near-complete recovery │
│ • Improvement usually begins within 2-3 weeks │
│ • Full recovery may take 3-6 months (up to 12 months) │
│ │
│ SAFETY NET - RETURN IF: │
│ • Weakness affecting other side of face │
│ • Weakness in arms or legs │
│ • Difficulty swallowing or breathing │
│ • Eye becomes red, painful, or vision changes │
│ • No improvement by 3-4 weeks │
│ • Developing blisters in ear (Ramsay Hunt may evolve) │
│ │
│ PRACTICAL ADVICE: │
│ • May need time off work (sick note provided) │
│ • Eating/drinking may be difficult initially (use straw, eat soft foods) │
│ • Facial exercises may help (mirror exercises) │
│ • Psychological impact is normal; support available │
└──────────────────────────────────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────────────────────────────────┐
│ STEP 6: FOLLOW-UP │
│ │
│ ROUTINE FOLLOW-UP: │
│ • Review at 2-4 weeks to assess progress │
│ • Document House-Brackmann grade │
│ • Ensure eye care is adequate │
│ │
│ IF NO RECOVERY BY 3-4 MONTHS: │
│ • Refer to neurology or ENT │
│ • MRI brain/IAMs with gadolinium to exclude tumour │
│ • Electrodiagnostic studies (ENoG, EMG) │
│ │
│ IF INCOMPLETE RECOVERY: │
│ • Refer for facial physiotherapy │
│ • Consider botulinum toxin for synkinesis │
│ • Surgical options rarely needed │
└──────────────────────────────────────────────────────────────────────────────┘
Pharmacological Treatment Details
Corticosteroids (First-Line Treatment):
| Regimen | Dose | Duration | Evidence |
|---|---|---|---|
| Standard (NICE, SIGN) | Prednisolone 50mg once daily | 10 days | Sullivan et al. NEJM 2007 [6] |
| Alternative | Prednisolone 60mg daily then taper | 5 days full dose, 5 days taper | AAN guideline 2012 [3] |
| High-dose option | Prednisolone 1mg/kg/day (max 80mg) | 7-10 days | Some centres |
Evidence Summary for Corticosteroids:
- Scottish Bell's Palsy Study (Sullivan et al., NEJM 2007): [6]
- 496 patients randomised
- Prednisolone vs. aciclovir vs. both vs. placebo
- "Complete recovery at 9 months: 94.4% (prednisolone) vs. 81.6% (no prednisolone)"
- NNT = 9 for one additional complete recovery
- Cochrane Review (2016): [7]
- Strong evidence supporting corticosteroids
- Reduces synkinesis and motor synkinesis
Antivirals (NOT Routinely Recommended):
| Agent | Dose | Duration | Indication |
|---|---|---|---|
| Aciclovir | 400mg 5x daily or 800mg 5x daily | 7 days | Ramsay Hunt syndrome ONLY |
| Valaciclovir | 1000mg 3x daily | 7 days | Ramsay Hunt syndrome ONLY |
Evidence Summary for Antivirals:
- Cochrane Review (Gagyor et al., 2019): [8]
- Meta-analysis of 14 trials (2,488 participants)
- "Antivirals alone: No significant benefit"
- "Antivirals + corticosteroids: No significant benefit over corticosteroids alone"
- "Conclusion: Antivirals should NOT be used routinely"
Eye Care Protocol
| Time | Intervention | Product Examples |
|---|---|---|
| Daytime (every 1-2 hours) | Artificial tears | Carmellose 0.5% (Celluvisc), Hypromellose 0.3% (Isopto Plain), Sodium hyaluronate (Hylo-Forte) |
| Night-time | Lubricating ointment | Lacri-Lube, VitA-POS, Simple Eye Ointment |
| Night-time (if lagophthalmos) | Tape eyelid closed | Micropore tape (horizontal strip across eyelid) |
| Severe lagophthalmos | Moisture chamber | Swimming goggles, cling film wrap |
| Outdoor activities | Protective eyewear | Wraparound sunglasses |
Special Populations
Pregnancy:
- Bell's palsy 3x more common in pregnancy (especially 3rd trimester and postpartum)
- Prednisolone is safe in pregnancy
- Do not withhold treatment
- Multidisciplinary management with obstetrics
Diabetes Mellitus:
- 2-4x increased risk of Bell's palsy
- Worse prognosis and recovery rates
- Corticosteroids may worsen glycaemic control - monitor and adjust
- Do not withhold treatment; benefits outweigh risks
- Closer follow-up advised
Children:
- Bell's palsy rare less than 10 years; consider alternative diagnoses
- If diagnosed, prednisolone dose adjusted for weight
- Lyme disease more common cause in endemic areas
- Consider Lyme serology routinely in paediatric cases
Immunocompromised Patients:
- Consider broader differential (HIV, infections, malignancy)
- Higher recurrence rates
- May consider antivirals in addition to steroids
- Specialist input advised
Rehabilitation and Long-Term Management
Facial Physiotherapy:
- Indicated for incomplete recovery
- Begins once active movement returns
- Techniques include:
- Mirror exercises (visual feedback)
- Mime therapy
- Neuromuscular retraining
- EMG biofeedback
- Evidence supports improved outcomes [18]
Synkinesis Management:
- Synkinesis = abnormal co-movement (e.g., eye closes when smiling)
- Develops during aberrant nerve regeneration
- Treatment options:
- Facial physiotherapy (neuromuscular retraining)
- Botulinum toxin injection (targeted to overactive muscles)
- Selective myectomy (rarely)
Surgical Interventions (Rarely Required)
| Procedure | Indication | Details |
|---|---|---|
| Tarsorrhaphy | Persistent lagophthalmos with corneal risk | Partial surgical closure of eyelids |
| Gold/platinum weight implant | Persistent lagophthalmos | Weight in upper eyelid aids closure |
| Lower lid tightening | Ectropion causing exposure | Lateral tarsal strip procedure |
| Facial nerve decompression | Controversial; severe cases with ENoG > 90% degeneration | Transmastoid or middle fossa approach |
| Facial reanimation surgery | Complete permanent paralysis | Static (fascia lata sling) or dynamic (cross-face nerve graft, free muscle transfer) |
9. Complications
Acute Complications
| Complication | Incidence | Presentation | Prevention | Management |
|---|---|---|---|---|
| Exposure keratopathy | 10-25% | Dry, gritty eye; corneal punctate erosions | Aggressive lubrication; taping | Increase lubrication; moisture chamber |
| Corneal ulcer | 1-5% (if untreated) | Red painful eye; photophobia; visual disturbance | As above | Urgent ophthalmology; topical antibiotics; consider tarsorrhaphy |
| Corneal abrasion | 5-10% | Sudden pain; foreign body sensation | Eye protection | Lubricants; topical antibiotics |
Chronic/Sequelae
| Complication | Incidence | Mechanism | Management |
|---|---|---|---|
| Synkinesis | 15-20% of incomplete recovery | Aberrant nerve regeneration; cross-wiring | Physiotherapy; botulinum toxin [18] |
| Crocodile tears (gustatory lacrimation) | 5-10% | Aberrant regeneration of parasympathetic fibres; lacrimal stimulated by eating | Botulinum toxin to lacrimal gland (rarely needed) |
| Hemifacial spasm | 1-5% | Post-paralytic; aberrant regeneration | Botulinum toxin |
| Facial contracture | 10-15% | Muscle fibrosis due to prolonged denervation | Physiotherapy; botulinum toxin |
| Residual weakness | 10-15% | Incomplete reinnervation; axonal loss | Physiotherapy; surgical reanimation in severe cases |
| Psychological impact | Variable | Facial disfigurement; social anxiety; depression | Psychological support; counselling |
Synkinesis: Detailed Management
Synkinesis is the most troublesome long-term complication, occurring in 15-20% of patients with incomplete recovery. [18]
Common Synkinesis Patterns:
| Pattern | Description |
|---|---|
| Oral-ocular | Eye closes when smiling or mouth moves |
| Ocular-oral | Mouth moves when closing eye |
| Midfacial | Nose/cheek moves with other facial movements |
Management Approach:
-
Facial physiotherapy (first-line)
- Neuromuscular retraining
- Small, slow, targeted movements
- Mirror feedback
- EMG biofeedback
-
Botulinum toxin (for refractory cases)
- Targeted injection to overactive muscles
- Common sites: orbicularis oculi, mentalis, platysma
- Repeat every 3-4 months
- Highly effective
-
Selective myectomy (rarely)
- Surgical removal of overactive muscle
- Reserved for severe refractory cases
10. Prognosis and Outcomes
Natural History
Without treatment, approximately 70% of patients with Bell's palsy achieve complete recovery. [6,7] Recovery typically follows this pattern:
| Timeframe | Expected Progress |
|---|---|
| 0-3 days | Weakness may progress to maximum severity |
| 1-2 weeks | Earliest signs of recovery in mild cases |
| 3-6 weeks | Most patients show early improvement |
| 3 months | Majority of recovery has occurred |
| 6-12 months | Maximal recovery achieved |
Outcomes with Treatment
| Outcome | With Corticosteroids | Without Treatment | Reference |
|---|---|---|---|
| Complete recovery | 85-95% | 70% | [6,7] |
| Partial recovery | 5-10% | 15-20% | [6] |
| Poor recovery | less than 5% | 10-15% | [6] |
| Synkinesis | 5-10% | 15-20% | [18] |
| Contracture | less than 5% | 10-15% |
Prognostic Factors
Favourable Prognosis:
| Factor | Rationale |
|---|---|
| Younger age (less than 40 years) | Better nerve regeneration capacity |
| Incomplete paralysis at onset (HB II-III) | Less axonal damage |
| Early treatment (less than 72 hours) | Reduces inflammation before axonal loss |
| Early signs of recovery (less than 3 weeks) | Indicates neuropraxia, not axonotmesis |
| No diabetes | Better microvascular environment |
| Preserved taste | Suggests less proximal nerve involvement |
| Positive Bell's phenomenon | Provides corneal protection |
Poor Prognosis:
| Factor | Rationale |
|---|---|
| Older age (> 60 years) | Reduced regeneration capacity |
| Complete paralysis at onset (HB V-VI) | Indicates more severe nerve injury |
| Diabetes mellitus | Microvascular disease impairs healing |
| Pregnancy-associated | May have more severe presentation |
| No recovery signs by 3-4 months | Suggests axonal loss or alternative diagnosis |
| Ramsay Hunt syndrome | More severe nerve damage from VZV |
| ENoG showing > 90% degeneration | Significant axonal loss |
| Absence of voluntary EMG potentials | Poor reinnervation |
House-Brackmann Grade and Prognosis
| Initial HB Grade | Complete Recovery Rate |
|---|---|
| HB II (mild) | > 95% |
| HB III (moderate) | 90-95% |
| HB IV (moderately severe) | 75-85% |
| HB V (severe) | 50-70% |
| HB VI (total paralysis) | 40-60% |
Recovery Timeline
BELL'S PALSY RECOVERY TRAJECTORY
Week 1-2: [████░░░░░░░░░░░░░░░░] 20% - Some patients begin recovery
Week 3-4: [████████░░░░░░░░░░░░] 40% - Most show early signs
Week 6-8: [████████████░░░░░░░░] 60% - Significant improvement
Month 3: [████████████████░░░░] 80% - Most recovery achieved
Month 6: [██████████████████░░] 90% - Further gains
Month 9-12: [████████████████████] 100% - Maximum recovery
Note: Those with incomplete recovery at 12 months are unlikely
to improve further without intervention.
11. Evidence and Guidelines
Key Clinical Guidelines
| Guideline | Organisation | Year | Key Recommendations |
|---|---|---|---|
| Bell's Palsy CKS | NICE | 2019 (updated 2023) | Prednisolone 50mg x10 days within 72h; antivirals not recommended |
| Practice Guideline Update | AAN | 2012 | Steroids established; antivirals possibly helpful (Grade C) |
| Bell's Palsy Guideline | SIGN | 2015 | Prednisolone recommended; antivirals not for Bell's |
Landmark Trials
1. Scottish Bell's Palsy Study (Sullivan et al., 2007) [6]
| Feature | Detail |
|---|---|
| Study design | Multicentre, factorial RCT |
| Population | 496 adults with Bell's palsy less than 72 hours |
| Intervention | 2x2 factorial: prednisolone and/or aciclovir vs placebo |
| Primary outcome | Complete facial recovery at 3 and 9 months |
| Key results | Prednisolone: 94.4% vs 81.6% complete recovery (pless than 0.001); Aciclovir: No significant benefit |
| Conclusion | Early prednisolone significantly improves outcome; no benefit from aciclovir |
| Impact | Established prednisolone as standard of care; ended routine antiviral use |
2. Cochrane Review: Antivirals for Bell's Palsy (Gagyor et al., 2019) [8]
| Feature | Detail |
|---|---|
| Study design | Systematic review and meta-analysis |
| Studies included | 14 RCTs (2,488 participants) |
| Comparisons | Antivirals alone vs placebo; antivirals + steroids vs steroids |
| Key results | No significant benefit of antivirals alone or combined |
| Conclusion | Antivirals NOT recommended for Bell's palsy |
3. Cochrane Review: Corticosteroids for Bell's Palsy (Madhok et al., 2016) [7]
| Feature | Detail |
|---|---|
| Study design | Systematic review and meta-analysis |
| Studies included | 7 RCTs (1,987 participants) |
| Key results | Corticosteroids reduce incomplete recovery (RR 0.69); reduce synkinesis |
| Conclusion | Strong evidence supporting corticosteroids |
Evidence Levels for Key Interventions
| Intervention | Evidence Level | Strength | Key Evidence |
|---|---|---|---|
| Corticosteroids (within 72h) | Level 1a | Strong | Cochrane review, NEJM RCT |
| Antivirals for Bell's palsy | Level 1a | Strong (against) | Cochrane review shows no benefit |
| Antivirals for Ramsay Hunt | Level 2b | Moderate | Lower quality evidence, but recommended |
| Eye care | Level 2b | Moderate (best practice) | Observational, clinical experience |
| Facial physiotherapy | Level 2b | Moderate | RCTs show benefit for synkinesis |
| Botulinum toxin for synkinesis | Level 2b | Moderate | Case series, clinical experience |
| Surgical decompression | Level 3-4 | Weak | Controversial; not routinely recommended |
12. Exam-Focused Content
Common Exam Questions
Written Examinations (MRCP, Finals):
-
"A 35-year-old woman presents with acute right-sided facial weakness. She cannot close her right eye or raise her right eyebrow. What is the most likely diagnosis and what is your initial management?"
-
"List 5 causes of bilateral facial weakness and the key distinguishing features."
-
"What is the difference between upper and lower motor neuron facial weakness? Explain the anatomical basis."
-
"A patient with Bell's palsy presents with vesicles in the external auditory canal. How does this change your management?"
-
"Discuss the evidence for and against antiviral therapy in Bell's palsy."
OSCE Stations
Station Type: Clinical Examination
- Examine the cranial nerves with focus on the facial nerve
- Grade severity using House-Brackmann scale
- Differentiate UMN from LMN pattern
- Check for Ramsay Hunt syndrome (examine ears)
Station Type: History and Management
- Take history from patient with acute facial weakness
- Explain diagnosis and management plan
- Discuss prognosis and safety-net advice
- Demonstrate eye care technique
Station Type: Communication
- Explain Bell's palsy to a worried patient who thinks they are having a stroke
- Discuss steroid treatment, addressing concerns about side effects
- Counsel regarding incomplete recovery and synkinesis
Viva Points
Viva Point: Opening Statement: "Bell's palsy is an acute, idiopathic, unilateral lower motor neuron facial paralysis characterised by sudden onset weakness affecting all muscles of facial expression on one side, including the forehead. It is the most common cause of acute facial palsy with an incidence of 20-30 per 100,000 per year."
Key Facts to Mention Unprompted:
- Incidence: 20-30 per 100,000/year; lifetime risk 1 in 60
- LMN pattern: forehead IS affected (vs UMN stroke where forehead spared)
- Treatment: Prednisolone 50mg daily for 10 days within 72 hours
- Evidence: Sullivan et al. NEJM 2007 - NNT 9
- Antivirals: NOT recommended (Cochrane 2019)
- Prognosis: 85-95% complete recovery with steroids
Classification System: House-Brackmann Grade I-VI
Management Priorities:
- Confirm LMN pattern (forehead affected)
- Exclude Ramsay Hunt (check ears for vesicles)
- Start prednisolone within 72 hours
- Eye protection (artificial tears, ointment, taping)
- Safety-net for red flags
Common Mistakes That Fail Candidates
| Mistake | Why It Fails | Correct Approach |
|---|---|---|
| Missing the forehead test | Fails to distinguish LMN from UMN | Always test frontalis - "raise your eyebrows" |
| Not examining the ears | Misses Ramsay Hunt syndrome | Otoscopy is mandatory in facial palsy |
| Prescribing antivirals for Bell's | Goes against current evidence | Antivirals only for Ramsay Hunt (vesicles) |
| Forgetting eye care | Preventable complication (corneal ulcer) | Always prescribe lubricants, ointment, taping |
| Saying "Bell's palsy spares forehead" | Fundamentally wrong | LMN (Bell's) AFFECTS forehead; UMN (stroke) SPARES it |
| Not knowing House-Brackmann | Expected knowledge for grading | Memorise the 6 grades |
| Ordering MRI routinely | Inappropriate investigation | MRI only if no recovery by 3-4 months or atypical |
Model Answer: "Describe Your Approach to Acute Facial Weakness"
"I would approach acute facial weakness systematically:
History: I would establish the onset (acute vs progressive), laterality (unilateral vs bilateral), and ask about associated symptoms including ear pain, vesicles, taste disturbance, hyperacusis, recent viral illness, tick exposure, and any limb weakness or sensory symptoms. I would enquire about risk factors including diabetes and pregnancy.
Examination: I would perform a focused neurological examination. First, I would determine if the pattern is upper or lower motor neuron by testing frontalis - can the patient wrinkle their forehead and raise their eyebrow? In Bell's palsy, an LMN lesion, the forehead is affected. I would grade severity using the House-Brackmann scale. I would examine the external auditory canal and pinna for vesicles, which would indicate Ramsay Hunt syndrome. I would complete a cranial nerve examination and assess limb neurology.
Diagnosis: Bell's palsy is a diagnosis of exclusion. I would confirm LMN pattern, exclude Ramsay Hunt, and ensure there are no red flags such as bilateral weakness, progressive course, or other neurological signs.
Management: For confirmed Bell's palsy, I would initiate prednisolone 50mg once daily for 10 days within 72 hours of onset. This is supported by Level 1a evidence from the Scottish Bell's Palsy Study showing an NNT of 9 for complete recovery. I would NOT prescribe antivirals as the Cochrane review shows no benefit. I would prescribe aggressive eye care: artificial tears every 1-2 hours, lubricating ointment at night, and tape the eyelid closed if incomplete closure. I would safety-net for red flags and arrange follow-up at 2-4 weeks.
If Ramsay Hunt: I would add aciclovir 800mg five times daily for 7 days to the corticosteroid regimen.
Follow-up: If no recovery by 3-4 months, I would refer for MRI to exclude a structural lesion."
13. Patient/Layperson Explanation
What is Bell's Palsy?
Bell's palsy is a condition that causes sudden weakness of the muscles on one side of your face. It happens when the nerve that controls your facial muscles (called the facial nerve) becomes inflamed and swollen. The exact cause is unknown, but it's thought to be related to a common virus (cold sore virus) that most people carry without problems, which occasionally "wakes up" and causes temporary nerve inflammation.
How Will I Know I Have It?
You may notice:
- One side of your face droops or feels stiff
- You cannot close your eye on the affected side
- You cannot smile or raise your eyebrow normally
- Food or drink may leak from your mouth
- You may have pain around your ear
- Sounds may seem louder than normal
- Your sense of taste may be affected
Important: This is NOT a stroke. In Bell's palsy, your forehead is affected (you can't wrinkle it on the weak side). In a stroke, the forehead usually works normally.
How Is It Treated?
1. Steroid Tablets (Prednisolone)
- These are the main treatment
- You need to start them within 3 days of symptoms beginning
- They significantly improve your chances of full recovery
- Take them for 10 days as prescribed
2. Eye Care (Very Important!)
- Because you can't close your eye properly, it can dry out and get damaged
- Use eye drops (artificial tears) every 1-2 hours during the day
- Use thick eye ointment at night
- Tape your eye closed at night if it won't close fully
- Wear glasses to protect from wind and dust
3. Antiviral Tablets
- These are NOT usually needed for Bell's palsy (despite what you might read online)
- They are only given if you have blisters in your ear (a different condition called Ramsay Hunt syndrome)
What Are My Chances of Recovery?
The good news: Most people with Bell's palsy recover well.
- With steroid treatment started early: 85-95% make a complete recovery
- Without treatment: about 70% recover completely
- You may start to see improvement within 2-3 weeks
- Full recovery can take 3-6 months (sometimes up to 12 months)
- A small number of people have some lasting weakness or unusual movements
When Should I Be Concerned?
Go back to your doctor or seek urgent medical advice if:
- Weakness develops on the OTHER side of your face as well
- You develop weakness in your arms or legs
- Your eye becomes red, painful, or your vision changes
- There's no improvement at all after 3-4 weeks
- You develop blisters or a rash in or around your ear
Tips for Coping
- Take any time off work you need - your doctor can provide a sick note
- Eating and drinking may be tricky at first - use a straw and eat soft foods
- Do gentle facial exercises in front of a mirror once movement starts to return
- It's normal to feel upset or self-conscious - talk to someone if you're struggling
- Support groups like Facial Palsy UK can provide helpful advice
14. References
Primary Guidelines and Reviews
-
Peitersen E. Bell's palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;(549):4-30. doi:10.1080/000164802760370736 PMID: 12482166
-
Gilden DH. Bell's palsy. N Engl J Med. 2004;351(13):1323-1331. doi:10.1056/NEJMcp041120 PMID: 15385659
-
Gronseth GS, Paduga R; American Academy of Neurology. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213. doi:10.1212/WNL.0b013e318275978c PMID: 23136264
-
Murakami S, Mizobuchi M, Nakashiro Y, Doi T, Hato N, Yanagihara N. Bell palsy and herpes simplex virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med. 1996;124(1 Pt 1):27-30. doi:10.7326/0003-4819-124-1_part_1-199601010-00005 PMID: 7503474
-
Furuta Y, Fukuda S, Chida E, et al. Reactivation of herpes simplex virus type 1 in patients with Bell's palsy. J Med Virol. 1998;54(3):162-166. doi:10.1002/(sici)1096-9071(199803)54:3less than 162::aid-jmv3> 3.0.co;2-3 PMID: 9515762
Landmark Trials
-
Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med. 2007;357(16):1598-1607. doi:10.1056/NEJMoa072006 PMID: 17942873
-
Madhok VB, Gagyor I, Daly F, et al. Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2016;7(7):CD001942. doi:10.1002/14651858.CD001942.pub5 PMID: 27428352
-
Gagyor I, Madhok VB, Daly F, Sullivan F. Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9(9):CD001869. doi:10.1002/14651858.CD001869.pub9 PMID: 31486071
Epidemiology and Risk Factors
-
Rowlands S, Hooper R, Hughes R, Burney P. The epidemiology and treatment of Bell's palsy in the UK. Eur J Neurol. 2002;9(1):63-67. doi:10.1046/j.1468-1331.2002.00343.x PMID: 11784378
-
Murakami S, Hato N, Horiuchi J, Honda N, Gyo K, Yanagihara N. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41(3):353-357. doi:10.1002/ana.410410310 PMID: 9066356
-
Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007;52(2):121-144. doi:10.1016/j.survophthal.2006.12.009 PMID: 17355852
-
Shmorgun D, Chan WS, Ray JG. Association between Bell's palsy in pregnancy and pre-eclampsia. QJM. 2002;95(6):359-362. doi:10.1093/qjmed/95.6.359 PMID: 12037243
-
Riga M, Kefalas P, Danielides V. The role of diabetes mellitus in the clinical presentation and prognosis of Bell's palsy. J Am Acad Audiol. 2012;23(5):364-370. doi:10.3766/jaaa.23.5.5 PMID: 22533978
-
Yanagihara N. Incidence of Bell's palsy. Ann Otol Rhinol Laryngol Suppl. 1988;137:3-4. doi:10.1177/00034894880970s701 PMID: 3144016
Clinical Features and Examination
-
Adour KK, Byl FM, Hilsinger RL Jr, Kahn ZM, Sheldon MI. The true nature of Bell's palsy: analysis of 1,000 consecutive patients. Laryngoscope. 1978;88(5):787-801. doi:10.1002/lary.1978.88.5.787 PMID: 642672
-
House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2):146-147. doi:10.1177/019459988509300202 PMID: 3921901
Prognosis and Electrodiagnosis
-
Fisch U. Prognostic value of electrical tests in acute facial paralysis. Am J Otol. 1984;5(6):494-498. PMID: 6393770
-
Teixeira LJ, Valbuza JS, Prado GF. Physical therapy for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2011;(12):CD006283. doi:10.1002/14651858.CD006283.pub3 PMID: 22161401
Surgical Management
- Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical management of Bell's palsy. Laryngoscope. 1999;109(8):1177-1188. doi:10.1097/00005537-199908000-00001 PMID: 10443817
Additional Resources
- de Almeida JR, Guyatt GH, Sud S, et al. Management of Bell palsy: clinical practice guideline. CMAJ. 2014;186(12):917-922. doi:10.1503/cmaj.131801 PMID: 24934895
Patient Resources
- Facial Palsy UK: facialpalsy.org.uk
- NICE Clinical Knowledge Summaries: cks.nice.org.uk/topics/bells-palsy
- American Academy of Neurology: aan.com
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Clinical decisions should account for individual patient circumstances. Always consult appropriate guidelines and specialists for patient care. Evidence and guidelines are current as of the last update date and should be verified against the latest publications.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Facial Nerve Anatomy (CN VII)
- Cranial Nerve Examination
Differentials
Competing diagnoses and look-alikes to compare.
- Ramsay Hunt Syndrome
- Lyme Disease
- Stroke (Facial Weakness)
- Acoustic Neuroma
- Parotid Tumour
- Guillain-Barre Syndrome
Consequences
Complications and downstream problems to keep in mind.
- Exposure Keratopathy
- Synkinesis