Biliary Colic & Acute Cholecystitis
Biliary colic and acute cholecystitis represent a clinical spectrum of gallstone-related disease affecting the gallbladder. Biliary colic is transient right upper quadrant (RUQ) pain caused by temporary cystic duct...
What matters first
Biliary colic and acute cholecystitis represent a clinical spectrum of gallstone-related disease affecting the gallbladder. Biliary colic is transient right upper quadrant (RUQ) pain caused by temporary cystic duct...
RUQ pain with fever
8 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- RUQ pain with fever
- Positive Murphy's sign
- Jaundice (suggests CBD stone)
- Pancreatitis features
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Biliary Colic & Acute Cholecystitis
Topic Overview
Summary
Biliary colic and acute cholecystitis represent a clinical spectrum of gallstone-related disease affecting the gallbladder. Biliary colic is transient right upper quadrant (RUQ) pain caused by temporary cystic duct obstruction by a gallstone, typically resolving within 6 hours as the stone dislodges. [1] Acute cholecystitis is sustained gallbladder inflammation resulting from persistent cystic duct obstruction, leading to gallbladder distension, mucosal ischaemia, and secondary bacterial infection. [2]
The distinction between these entities is critical for management: biliary colic is self-limiting and managed conservatively with elective cholecystectomy, while acute cholecystitis requires antibiotics and early surgical intervention (within 7 days). [3] Murphy's sign—inspiratory arrest on deep palpation of the RUQ—is a highly specific clinical finding for acute cholecystitis. [4] Ultrasonography is the first-line imaging modality, demonstrating gallstones, gallbladder wall thickening, and pericholecystic fluid. [5]
Early laparoscopic cholecystectomy within one week of symptom onset has become the standard of care for acute cholecystitis, reducing total hospital stay and complications compared to delayed surgery. [3]
Key Facts
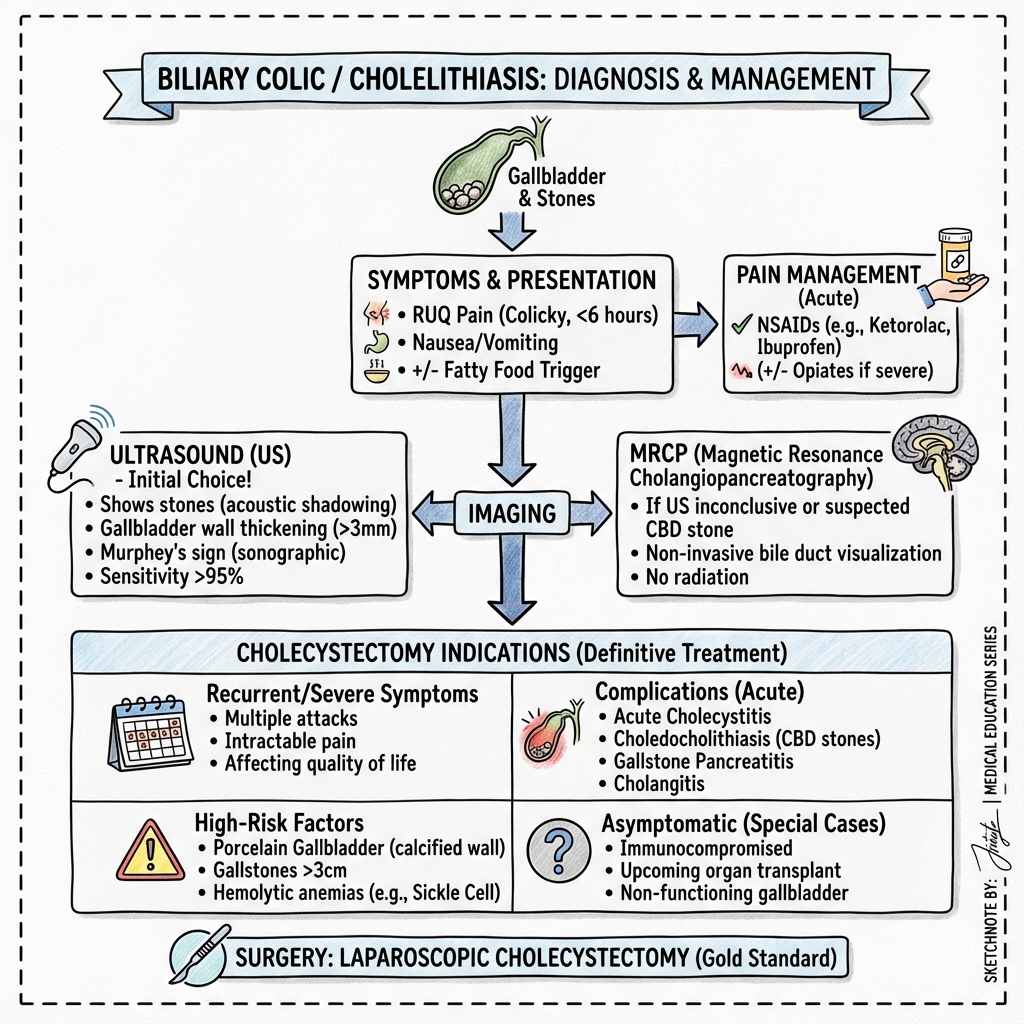
- Biliary colic: Episodic RUQ pain lasting 30 minutes to 6 hours, typically without fever or peritoneal signs
- Acute cholecystitis: Persistent RUQ pain exceeding 6 hours, fever, positive Murphy's sign, elevated inflammatory markers (WCC, CRP)
- Imaging: Ultrasound first-line (sensitivity 88%, specificity 80% for acute cholecystitis) [5]
- Treatment: Conservative management for biliary colic; antibiotics plus early cholecystectomy for acute cholecystitis
- Tokyo Guidelines 2018: Internationally validated severity grading system (Grade I-III) guiding management [2]
Clinical Pearls
Pain duration is key: Pain persisting beyond 6 hours should raise suspicion for acute cholecystitis rather than uncomplicated biliary colic
Murphy's sign specificity: When properly elicited (inspiratory arrest during deep RUQ palpation), Murphy's sign has specificity of 79-96% for acute cholecystitis [4,5]
Ultrasound limitations: 5-10% of gallstones may not be visualized on ultrasound; normal ultrasound does not exclude gallstone disease [5]
Early surgery wins: Cholecystectomy within 72 hours of presentation reduces hospital stay by 4 days and complication rates by 30% compared to delayed surgery [3]
Why This Matters Clinically
Gallstone disease affects 10-15% of Western adults, making it one of the most prevalent gastrointestinal conditions. [6] Cholecystectomy ranks among the most frequently performed elective surgical procedures worldwide. Accurate differentiation between biliary colic and acute cholecystitis determines urgency of intervention, antibiotic use, and surgical timing—directly impacting patient outcomes, complication rates, and healthcare resource utilization.
Visual Summary
Visual assets to be added:
- Biliary anatomy diagram showing gallbladder, cystic duct, common bile duct, and pancreatic duct
- Ultrasound imaging: gallstones with posterior acoustic shadowing
- Murphy's sign technique demonstration
- Tokyo Guidelines 2018 severity stratification flowchart
- Laparoscopic cholecystectomy port placement diagram
- Calot's triangle anatomy for surgical reference
Epidemiology
Prevalence
Gallstone disease demonstrates high prevalence with significant geographic and demographic variation:
- Western populations: 10-15% prevalence in adults [6]
- Asymptomatic gallstones: 80% remain asymptomatic throughout lifetime
- Symptomatic progression: 1-4% of asymptomatic gallstone carriers develop symptoms annually [6]
- Acute cholecystitis: Develops in approximately 10% of patients with symptomatic gallstones [1]
- Cholecystectomy: Approximately 750,000 procedures performed annually in the United States alone
Demographics
Sex Disparity
- Female-to-male ratio: 2-3:1 [6]
- Sex differences diminish after age 60
Age Distribution
- Prevalence increases progressively with age
- Under 40 years: ~5% prevalence
- Over 60 years: ~25% prevalence
- Peak incidence of acute cholecystitis: 50-60 years [1]
Ethnic Variation
- Highest rates: Native Americans (Pima Indians up to 70% by age 30)
- High prevalence: Hispanic populations, Northern Europeans
- Lower prevalence: Sub-Saharan African populations, Asian populations
Risk Factors
Non-Modifiable Risk Factors
| Factor | Relative Risk | Mechanism |
|---|---|---|
| Female sex | 2-3× | Estrogen increases cholesterol secretion, reduces bile acid synthesis |
| Age | 1.5-2× per decade | Decreased bile acid synthesis, gallbladder hypomotility |
| Ethnicity | Variable | Genetic factors affecting bile composition |
| Family history | 2-4× | Genetic variants in cholesterol transporters (ABCG8) |
| Pregnancy | 2-5× per pregnancy | Progesterone-induced gallbladder stasis, estrogen effects [6] |
Modifiable Risk Factors
| Factor | Relative Risk | Notes |
|---|---|---|
| Obesity | 2-7× (BMI-dependent) | Major modifiable risk; linear relationship with BMI [6] |
| Rapid weight loss | 3-5× | Especially > 1.5 kg/week; cholesterol supersaturation |
| Metabolic syndrome | 1.5-3× | Insulin resistance, dyslipidemia components |
| Type 2 diabetes | 1.3-2× | Gallbladder dysmotility, autonomic dysfunction |
| Prolonged fasting | 2-3× | Gallbladder stasis |
| Total parenteral nutrition | High | Lack of CCK stimulation, biliary stasis |
Disease-Associated Risk Factors
| Condition | Stone Type | Pathophysiology |
|---|---|---|
| Crohn's disease | Cholesterol | Reduced ileal bile acid reabsorption (especially terminal ileal disease) [6] |
| Ileal resection | Cholesterol | Bile acid depletion, cholesterol supersaturation |
| Haemolytic disorders | Pigment | Increased unconjugated bilirubin (sickle cell, hereditary spherocytosis) |
| Cirrhosis | Pigment | Hypersplenism, increased bilirubin production |
| Cystic fibrosis | Mixed | Biliary sludge, altered bile composition |
Medications
| Drug Class | Risk | Mechanism |
|---|---|---|
| Estrogen therapy | 2-3× | HRT, oral contraceptives; increased cholesterol secretion |
| Fibrates | 1.5-2× | Increased biliary cholesterol saturation |
| Somatostatin analogues | 2-4× | Reduced gallbladder motility |
| Ceftriaxone | Variable | Biliary precipitation (especially high doses) |
Mnemonic Revisited: The "5 Fs"
The traditional "5 Fs" (Female, Forty, Fertile, Fat, Family history) oversimplifies risk but captures key demographic patterns. Modern understanding recognizes metabolic syndrome, rapid weight loss, and specific disease states as equally or more significant risk factors. [6]
Pathophysiology
Bile Physiology Overview
Understanding gallstone pathophysiology requires knowledge of normal bile composition and secretion:
Bile Components
- Bile salts (67%): Micelle formation, cholesterol solubilization
- Phospholipids (22%): Primarily phosphatidylcholine
- Cholesterol (4%): Normally solubilized in micelles
- Bilirubin (0.3%): Conjugated bilirubin glucuronide
- Electrolytes, proteins (remainder)
Enterohepatic Circulation
- 95% bile acid reabsorption in terminal ileum
- Total bile acid pool: 2-4 g
- Recirculates 6-8 times daily
- Disruption (Crohn's, resection) → cholesterol supersaturation
Gallstone Formation
Cholesterol Stones (80% of cases)
Stage 1: Cholesterol Supersaturation
- Imbalance in bile composition
- Cholesterol exceeds micelle-forming capacity
- Lithogenic index > 1.0 (cholesterol/bile salt ratio)
Stage 2: Nucleation
- Cholesterol monohydrate crystal precipitation
- Nucleation factors: mucin glycoproteins, immunoglobulins
- Anti-nucleation factors: apolipoproteins, lecithin
Stage 3: Crystal Growth and Stone Formation
- Mucin gel trapping of crystals
- Progressive crystal aggregation
- Biliary sludge → microliths → macroscopic stones
Contributing Factors
- Gallbladder hypomotility (prolonged CCK resistance)
- Increased cholesterol synthesis (obesity, genetics)
- Decreased bile acid synthesis (age, estrogen)
- Mucin hypersecretion [6]
Pigment Stones (20% of cases)
Black Pigment Stones
- Composition: Calcium bilirubinate, calcium carbonate, mucin glycoproteins
- Associated with: Chronic haemolysis, cirrhosis, age > 70
- Mechanism: Unconjugated bilirubin precipitation [6]
Brown Pigment Stones
- Composition: Calcium bilirubinate, calcium palmitate, cholesterol
- Associated with: Biliary infection, stasis (bacterial deconjugation of bilirubin)
- Location: Often form in bile ducts (intra- or extrahepatic)
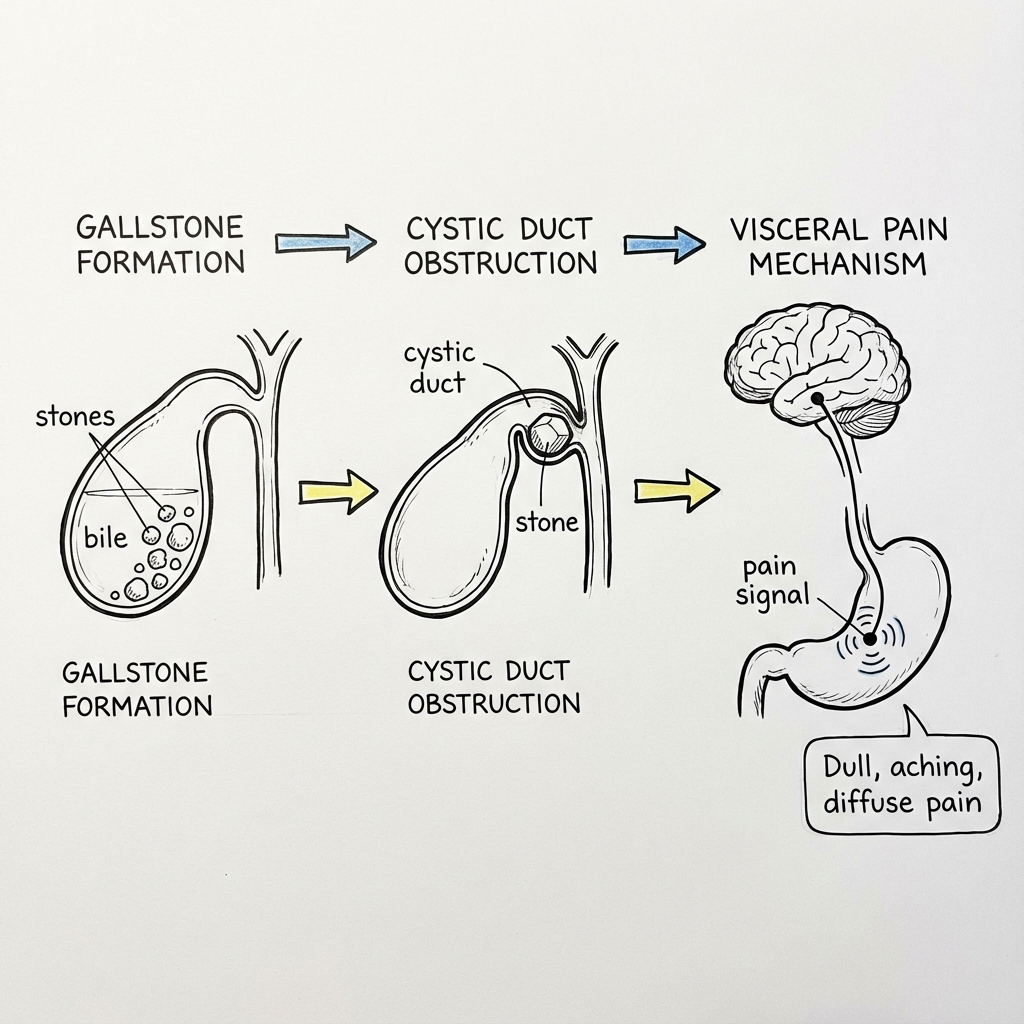
Biliary Colic Pathophysiology
Mechanism
- Gallstone migration from gallbladder body to neck/infundibulum
- Transient impaction in cystic duct (Hartmann's pouch)
- Gallbladder contraction against obstruction (CCK-mediated post-prandial)
- Increased intraluminal pressure → visceral pain (sympathetic afferents T7-T9)
- Stone dislodges → pressure normalizes → pain resolves
Pain Characteristics
- Visceral pain: Poorly localized, constant (despite name "colic")
- Duration: Typically 30 minutes to 6 hours [1]
- Radiation: Epigastrium to right scapula (T7-T9 dermatomes)
- No inflammation: Normal inflammatory markers
Resolution
- Stone returns to gallbladder body (gravitational)
- Stone passes into common bile duct (may cause choledocholithiasis)
- Spontaneous resolution within hours
Acute Cholecystitis Pathophysiology
Stage 1: Mechanical Obstruction (0-24 hours)
- Persistent cystic duct obstruction by impacted stone (90-95% of cases)
- Continued gallbladder bile secretion
- Progressive distension (from 30 mL to > 100 mL)
- Increased intraluminal pressure (> 25 mmHg)
Stage 2: Mucosal Injury and Inflammation (24-72 hours)
- Venous and lymphatic obstruction
- Mucosal ischaemia and necrosis
- Release of inflammatory mediators (prostaglandins, leukotrienes)
- Phospholipase activation → lysolecithin (direct mucosal toxicity)
- Transmural inflammation [1,2]
Stage 3: Secondary Bacterial Infection (48-96 hours)
- Bacterial translocation from compromised mucosa
- Common organisms: E. coli (40%), Klebsiella (20%), Enterococcus (15%) [7]
- Anaerobes in severe/gangrenous cases: Bacteroides, Clostridium
- Biofilm formation on stones
Stage 4: Complications (Variable Timing)
- Empyema: Pus-filled gallbladder (5-10% of cases)
- Gangrenous cholecystitis: Transmural necrosis (2-30%, higher in elderly) [2]
- Perforation: Localized (pericholecystic abscess) or free (peritonitis) (2-3%)
- Emphysematous cholecystitis: Gas-forming organisms (1%, diabetics, males)
Acalculous Cholecystitis (5-10% of acute cholecystitis)
Mechanism
- Gallbladder ischaemia without stone obstruction
- Associated with critical illness, major surgery, burns, sepsis
- Bile stasis + ischaemia + infection
Risk Factors
- ICU admission, mechanical ventilation
- Major trauma, burns (> 30% BSA)
- Total parenteral nutrition
- Vasopressor use (splanchnic vasoconstriction)
- Immunosuppression (higher perforation risk)
Prognosis
- Higher morbidity and mortality than calculous (30% vs. 1%)
- More rapid progression to gangrene and perforation [8]
Clinical Presentation
Biliary Colic: Clinical Features
Pain Characteristics
| Feature | Description | Frequency |
|---|---|---|
| Location | RUQ or epigastric | 70-80% RUQ; 20-30% epigastric [1] |
| Character | Constant, "boring" (not truly colicky) | Typical |
| Duration | 30 minutes to 6 hours (typically 2-4 hours) | Diagnostic criterion |
| Radiation | Right scapula, right shoulder, interscapular | 50-60% |
| Onset | Often post-prandial (especially fatty meals) | 60-70% |
| Severity | Moderate to severe (requiring analgesia) | Variable |
Associated Symptoms
- Nausea and vomiting: 70-80% of patients
- Diaphoresis: Common during peak pain
- Restlessness: Patient cannot find comfortable position
- Bloating and dyspepsia: May precede or follow attack
What Biliary Colic Does NOT Feature
- ❌ Fever (suggests cholecystitis or cholangitis)
- ❌ Rigors (suggests ascending infection)
- ❌ Jaundice (suggests CBD stone)
- ❌ Peritoneal signs (suggests perforation or other acute abdomen)
- ❌ Prolonged pain > 6 hours (suggests cholecystitis) [1]
Differential Diagnosis Hints
In biliary colic, pain is:
- Less sudden than perforated viscus
- More sustained than intestinal colic
- Not positional (unlike MSK pain)
- Not relieved by antacids (unlike peptic ulcer)
Acute Cholecystitis: Clinical Features
Cardinal Features (Tokyo Guidelines 2018 Diagnostic Criteria) [2]
A. Local Signs of Inflammation
- Murphy's sign (positive)
- RUQ mass/pain/tenderness
B. Systemic Signs of Inflammation
- Fever (> 37.5°C)
- Elevated CRP (> 3 mg/dL)
- Elevated WCC (> 10,000/μL)
C. Imaging Findings
- Characteristic findings on ultrasound, CT, or MRI
Diagnosis: A + B + C = Definite acute cholecystitis
Murphy's Sign: Detailed Examination Technique
Proper Elicitation
- Patient positioned supine, relaxed
- Examiner's hand placed below right costal margin (RCM)
- Patient asked to take deep inspiration
- Positive sign: Inspiratory arrest due to pain at point of maximum RUQ tenderness
Test Characteristics [4,5]
- Sensitivity: 50-65% (many false negatives in obese, elderly)
- Specificity: 79-96% (highly specific when positive)
- Negative predictive value: Low (negative does not exclude)
Sonographic Murphy's Sign
- Tenderness directly over gallbladder on ultrasound probe pressure
- Sensitivity 63%, specificity 93% [5]
- Particularly useful in obese patients
Pain Evolution
Unlike biliary colic:
- Duration: > 6 hours (often 24-48 hours before presentation) [1]
- Progression: Worsening rather than resolving
- Character: May become sharper with peritoneal involvement
Systemic Features
| Feature | Frequency | Severity Correlation |
|---|---|---|
| Fever | 50-70% | Grade II-III more likely |
| Tachycardia | 40-60% | Correlates with systemic inflammation |
| Anorexia | 70-80% | Non-specific |
| Malaise | Variable | Suggests systemic inflammatory response |
Examination Findings
Abdominal Examination
- RUQ tenderness: Universal (if absent, reconsider diagnosis)
- Guarding: Local RUQ (suggests transmural inflammation)
- Rebound tenderness: Peritoneal involvement
- Palpable gallbladder: 15-30% (more common in acalculous)
- Boas' sign: Hyperesthesia below right scapula (historical, rarely used)
Systemic Examination
- Jaundice: Absent in uncomplicated cholecystitis (if present, consider Mirizzi syndrome, choledocholithiasis)
- Hemodynamic instability: Grade III cholecystitis
Red Flags: When to Escalate Urgency
| Finding | Concern | Action |
|---|---|---|
| Jaundice | CBD stone (choledocholithiasis) | Urgent LFTs, imaging (MRCP), consider ERCP |
| Rigors + fever | Ascending cholangitis | Blood cultures, IV antibiotics, ERCP consideration |
| Severe RUQ pain + elevated amylase | Gallstone pancreatitis | Amylase/lipase, manage as pancreatitis, plan early cholecystectomy |
| Sepsis/shock | Gangrenous/perforated cholecystitis | Resuscitation, broad-spectrum antibiotics, surgical consultation |
| Elderly (> 70) or immunocompromised | Higher perforation/gangrene risk | Lower threshold for imaging, admission, early surgery [2] |
| Diabetes mellitus | Emphysematous cholecystitis risk | CT if USS equivocal, aggressive management |
Clinical Examination
Systematic Approach
General Inspection
- Patient position: Restless during biliary colic; still during peritonitis
- Signs of chronic liver disease: Stigmata suggest cirrhosis (pigment stones)
- Jaundice: Inspect sclera, skin (suggests biliary obstruction)
- Hydration status: Prolonged vomiting may cause dehydration
Vital Signs
| Parameter | Biliary Colic | Acute Cholecystitis | Severe/Complicated |
|---|---|---|---|
| Temperature | Afebrile | Low-grade (37.5-38.5°C) | High fever > 38.5°C |
| Heart rate | Normal/mildly elevated | Tachycardia (90-110) | > 110 bpm (sepsis) |
| Blood pressure | Normal | Normal | Hypotension (Grade III) |
| Respiratory rate | Normal | May be elevated | Elevated if septic |
Abdominal Examination
Inspection
- Scars: Previous upper abdominal surgery
- Distension: Generalized (ileus) or localized (mass)
- Movement with respiration: Reduced in peritonism
Palpation
- Begin away from pain: Start in left lower quadrant
- Superficial palpation: Assess for guarding (involuntary muscle spasm)
- Deep palpation:
- RUQ tenderness localization
- Murphy's sign elicitation (see above)
- "Mass: Palpable gallbladder (distended/empyema) or phlegmon"
Percussion
- Localized tenderness
- Rule out hepatomegaly (lower edge of dullness)
Auscultation
- Bowel sounds: Present in uncomplicated cases; absent suggests ileus or peritonitis
Special Signs
Murphy's Sign (see detailed technique above)
- Most important clinical sign
- Specificity 79-96% for acute cholecystitis [4,5]
Courvoisier's Law
- Painless jaundice + palpable gallbladder = unlikely to be gallstones (suggests malignancy)
- Rationale: Chronic stone disease → fibrotic, non-distensible gallbladder
Boas' Sign
- Hyperesthesia below right scapula
- Historical; low sensitivity/specificity
- Rarely used in modern practice
Severity Assessment
Use Tokyo Guidelines 2018 criteria at bedside: [2]
Grade I (Mild)
- Local inflammation only
- No organ dysfunction
- Systemically well
Grade II (Moderate)
- Elevated WCC > 18,000
- Palpable tender RUQ mass
- Symptoms > 72 hours
- Marked local inflammation (imaging)
Grade III (Severe)
- Evidence of organ dysfunction:
- "Cardiovascular: Hypotension requiring pressors"
- "Neurological: Altered consciousness"
- "Respiratory: PaO2/FiO2 less than 300"
- "Renal: Creatinine > 177 μmol/L"
- "Hepatic: INR > 1.5"
- "Hematological: Platelets less than 100,000"
Investigations
Initial Blood Tests
Full Blood Count (FBC)
| Parameter | Biliary Colic | Acute Cholecystitis | Interpretation |
|---|---|---|---|
| WCC | Normal (4-11 × 10⁹/L) | Elevated (12-20 × 10⁹/L) | > 18 suggests severe (Tokyo Grade II) [2] |
| Neutrophils | Normal | Neutrophilia | Left shift suggests bacterial infection |
| Haemoglobin | Normal | Normal (unless haemolysis) | Low if bleeding/haemolytic disorder |
| Platelets | Normal | Normal/elevated (reactive) | Thrombocytopenia suggests sepsis/DIC |
Inflammatory Markers
-
CRP:
- "Biliary colic: less than 10 mg/L"
- "Acute cholecystitis: 50-150 mg/L (typically > 30 mg/L) [2]"
- "Rising CRP: Worsening inflammation"
-
Procalcitonin:
- May be elevated in bacterial cholecystitis
- Not routinely measured; reserved for sepsis evaluation
Liver Function Tests (LFTs)
| Test | Normal Cholecystitis | Abnormal: Suggests |
|---|---|---|
| Bilirubin | Normal (less than 21 μmol/L) | CBD stone, Mirizzi syndrome, cholangitis |
| ALT | Normal or mildly ↑ | CBD stone (ALT > 100), hepatitis |
| ALP | Normal or mildly ↑ | Biliary obstruction (ALP > 200) [1] |
| GGT | Normal or mildly ↑ | Cholestasis (follows ALP pattern) |
| Albumin | Normal | Chronic liver disease if low |
LFT Interpretation
- Normal LFTs: Cholecystitis confined to gallbladder
- Cholestatic pattern (ALP/GGT > 2× ALT): Suspect CBD stone → proceed to MRCP
- Transaminitis (ALT > 100): Gallstone pancreatitis, passed CBD stone, hepatitis
Pancreatic Enzymes
- Amylase/Lipase:
- Order if epigastric pain, vomiting prominent
- "Elevation > 3× ULN: Gallstone pancreatitis [9]"
- "Mild elevation (1-2× ULN): Can occur in cholecystitis alone"
Renal Function and Electrolytes
- Urea/Creatinine: Assess dehydration, baseline renal function
- Electrolytes: Vomiting-induced hypokalemia, hypochloremia (metabolic alkalosis)
Coagulation
- PT/INR: Baseline if considering surgery; elevated suggests liver dysfunction or sepsis
Imaging Investigations
Ultrasound (First-Line)
Indications
- All patients with suspected biliary pathology
- Non-invasive, no radiation, high availability [5]
Technique
- Patient preparation: 6-8 hours fasting (distends gallbladder)
- Transabdominal approach: Right subcostal, intercostal views
- Operator-dependent: Quality varies with body habitus, experience
Ultrasound Findings in Gallstone Disease
| Finding | Description | Sensitivity/Specificity |
|---|---|---|
| Gallstones | Echogenic foci with posterior acoustic shadowing | 89%/99% for stones > 2mm [5] |
| Biliary sludge | Layering echogenic material (no shadowing) | Variable |
| CBD dilatation | CBD > 6mm (> 7mm if post-cholecystectomy) | 55%/85% for CBD stone [5] |
Ultrasound Findings in Acute Cholecystitis [5]
| Finding | Sensitivity | Specificity | Description |
|---|---|---|---|
| Gallstones | 90% | N/A | Usually visualized (acalculous in 5-10%) |
| Wall thickening | 50-75% | 85-95% | > 3mm (> 4mm more specific); measure at fundus |
| Pericholecystic fluid | 25-50% | 90-95% | Surrounds gallbladder; suggests severe inflammation |
| Sonographic Murphy's sign | 63% | 93% | Tenderness directly over gallbladder with probe pressure |
Additional Features (Complicated Cholecystitis)
- Wall irregularity/striated appearance: Gangrenous cholecystitis
- Intramural gas: Emphysematous cholecystitis (requires CT confirmation)
- Pericholecystic abscess: Loculated fluid collection
Limitations of Ultrasound
- Operator-dependent
- Limited by obesity (BMI > 35), bowel gas
- Poor sensitivity for CBD stones (55%) [5]
- Cannot definitively exclude cholecystitis if normal
Computed Tomography (CT)
Indications
- Equivocal ultrasound findings
- Suspected complications (perforation, abscess, emphysematous cholecystitis)
- Differential diagnosis (appendicitis, pancreatitis, renal colic)
- Acalculous cholecystitis in critically ill
CT Findings
- Wall thickening > 3mm
- Pericholecystic fat stranding
- Subserosal edema ("halo sign")
- Gallstones (if calcified; pure cholesterol stones may be radiolucent)
- Complications: Abscess, perforation, gas in wall
Advantages over Ultrasound
- Better visualization in obese patients
- Detects complications more reliably
- Evaluates entire abdomen (alternative diagnoses)
Disadvantages
- Radiation exposure
- Contrast allergy/nephrotoxicity
- More expensive
- Lower specificity than ultrasound for simple cholecystitis
Magnetic Resonance Cholangiopancreatography (MRCP)
Indications
- Suspected CBD stone (cholestatic LFTs, jaundice, dilated CBD on USS)
- Pre-operative planning if ERCP consideration
- Failed or equivocal ERCP
- Mirizzi syndrome evaluation
MRCP Advantages
- Non-invasive (unlike ERCP)
- Excellent visualization of biliary tree and pancreatic duct
- Sensitivity 85-92% for CBD stones [10]
- No radiation
Findings
- CBD stones (filling defects)
- Biliary dilatation
- Mirizzi syndrome (extrinsic compression of common hepatic duct)
- Bile duct anomalies
Hepatobiliary Iminodiacetic Acid (HIDA) Scan
Indications
- Suspected acute cholecystitis with normal ultrasound
- Acalculous cholecystitis
- Chronic cholecystitis (gallbladder ejection fraction)
- Post-operative bile leak assessment
Technique
- IV Tc-99m HIDA (taken up by hepatocytes, excreted in bile)
- Imaging at intervals: Normal gallbladder fills within 60 minutes
- Non-visualization of gallbladder at 4 hours = cystic duct obstruction
Interpretation
- Positive (cholecystitis): Non-filling of gallbladder (cystic duct obstruction)
- Negative: Normal gallbladder filling (excludes cholecystitis)
- Sensitivity 90-95%, specificity 90-95% [11]
Limitations
- Time-consuming (4 hours)
- False positives: Prolonged fasting, TPN, chronic liver disease, critically ill
- Not widely available
Endoscopic Retrograde Cholangiopancreatography (ERCP)
Not a Diagnostic Tool
- ERCP is therapeutic, not diagnostic (use MRCP for diagnosis)
- Reserved for confirmed or highly suspected CBD stones
Indications for ERCP
- CBD stone confirmed on MRCP
- Acute cholangitis (therapeutic urgency)
- Persistent cholestatic LFTs post-cholecystectomy
Classification & Staging
Tokyo Guidelines 2018: Severity Grading [2]
The Tokyo Guidelines provide internationally validated criteria for diagnosing and grading acute cholecystitis severity, guiding management decisions.
Diagnostic Criteria
Suspected Diagnosis: A + B (1 item each)
A. Local Signs
- Murphy's sign
- RUQ mass/pain/tenderness
B. Systemic Signs
- Fever
- Elevated CRP
- Elevated WCC
Definite Diagnosis: A + B + C
C. Imaging Findings
- Findings characteristic of acute cholecystitis on USS/CT/MRI
Severity Grading
Grade I (Mild Acute Cholecystitis)
Criteria:
- Does not meet criteria for Grade II or III
- Otherwise healthy patient
- Mild inflammatory changes on imaging
Management:
- Early laparoscopic cholecystectomy (within 7 days, ideally less than 72 hours)
- Excellent outcomes with low conversion rate
Grade II (Moderate Acute Cholecystitis)
Criteria (any one of):
- Elevated WCC (> 18,000/μL)
- Palpable tender mass in RUQ
- Duration of symptoms > 72 hours
- Marked local inflammation (gangrenous cholecystitis, pericholecystic abscess, hepatic abscess, biliary peritonitis, emphysematous cholecystitis)
Management:
- Early cholecystectomy in stable patients
- Percutaneous drainage if high surgical risk or unfit
- Higher conversion to open rate
Grade III (Severe Acute Cholecystitis)
Criteria: Organ dysfunction (any one of)
| System | Dysfunction Criterion |
|---|---|
| Cardiovascular | Hypotension requiring dopamine ≥5 μg/kg/min or any dose noradrenaline |
| Neurological | Decreased level of consciousness |
| Respiratory | PaO2/FiO2 ratio less than 300 |
| Renal | Oliguria, creatinine > 177 μmol/L (> 2.0 mg/dL) |
| Hepatic | PT-INR > 1.5 |
| Hematological | Platelet count less than 100,000/μL |
Management:
- Urgent supportive care and resuscitation
- Percutaneous cholecystostomy drainage
- Antibiotics for sepsis
- Delay cholecystectomy until stabilized (interval cholecystectomy after 6-8 weeks)
Outcomes by Grade [2]
- Grade I: Mortality less than 0.5%
- Grade II: Mortality 1-3%
- Grade III: Mortality 5-10% (up to 30% if untreated)
Alternative Classification Systems
Acalculous vs. Calculous
- Calculous (90-95%): Stone-related cystic duct obstruction
- Acalculous (5-10%): Ischemic, critically ill, higher mortality [8]
Histopathological Classification
- Acute: Neutrophilic infiltration, edema, congestion
- Chronic: Fibrosis, Rokitansky-Aschoff sinuses, chronic inflammatory infiltrate
- Acute-on-chronic: Mixed features (most common surgical specimen)
Management
Initial Management (All Patients)
Resuscitation and Supportive Care
| Intervention | Rationale |
|---|---|
| Nil by mouth | Reduces CCK-mediated gallbladder contraction, prepares for potential surgery |
| IV fluids | Correct dehydration from vomiting; typically 1-2 L crystalloid (normal saline/Hartmann's) |
| Analgesia | NSAIDs first-line (diclofenac, ketorolac); opioids if inadequate (morphine, oxycodone) [1] |
| Antiemetics | Metoclopramide, ondansetron, cyclizine |
| VTE prophylaxis | LMWH (enoxaparin) if admitted and mobile, TED stockings |
Analgesia Notes
- NSAIDs: Effective for visceral pain; avoid if renal impairment or bleeding risk
- Opioids: May cause sphincter of Oddi spasm theoretically (clinical significance debated); do not withhold
- Avoid intramuscular diclofenac (risk of necrotizing fasciitis)
Management of Biliary Colic (Uncomplicated)
Immediate Management
- Analgesia and antiemetics as above
- Assess for features of cholecystitis (see diagnostic criteria)
- Blood tests: FBC, CRP, LFTs (exclude cholecystitis, CBD stone)
- Ultrasound if first presentation (confirm stones, exclude cholecystitis)
Disposition
- Discharge criteria: Pain resolving, tolerating oral intake, afebrile, normal inflammatory markers
- Admission criteria: Persistent pain, unable to tolerate oral, diagnostic uncertainty
Outpatient Follow-Up
- Elective cholecystectomy referral (prevents recurrence and complications) [1]
- Dietary advice: Low-fat diet (reduces CCK release)
- Return advice: Fever, persistent pain > 6 hours, jaundice
Cholecystectomy Timing
- Recommended within 6 months of first episode
- 20% risk of recurrent biliary symptoms within 1 year without surgery
- 1-3% annual risk of acute cholecystitis
Management of Acute Cholecystitis
Antibiotic Therapy [7]
Indications
- All cases of acute cholecystitis (cystic duct obstruction → bacterial superinfection in 50-70%)
Spectrum
- Gram-negative: E. coli, Klebsiella, Enterobacter
- Gram-positive: Enterococcus species
- Anaerobes: Bacteroides, Clostridium (gangrenous, severe cases)
Antibiotic Regimens
| Severity | First-Line | Alternative | Duration |
|---|---|---|---|
| Grade I (Mild) | Co-amoxiclav 1.2g IV TDS | Cefuroxime 1.5g IV TDS + metronidazole 500mg IV TDS | Until surgery (typically 24-72 hours) |
| Grade II-III (Moderate-Severe) | Piperacillin-tazobactam 4.5g IV TDS | Meropenem 1g IV TDS | 5-7 days total (including post-op) |
| Penicillin Allergy | Ciprofloxacin 400mg IV BD + metronidazole 500mg IV TDS | Gentamicin 5-7 mg/kg IV OD + metronidazole 500mg IV TDS | As above |
Notes
- Switch to oral antibiotics when afebrile and tolerating diet (e.g., co-amoxiclav 625mg TDS)
- Duration: Continue antibiotics for 24-48 hours post-surgery if uncomplicated
- Prolonged course: Gangrenous, perforated, or empyema (7-14 days)
Surgical Management: Early Cholecystectomy
Evidence for Early Surgery
Landmark trials (ACDC,CHCHAL) demonstrate: [3]
- Early cholecystectomy (within 7 days) reduces total hospital stay by 4 days
- Lower complication rates (5% vs. 17% for delayed)
- Lower readmission rates (7% vs. 23%)
- No increase in conversion to open (12% vs. 14%)
- Cost-effective
Timing Recommendations
- Optimal window: Within 72 hours of symptom onset (lower conversion rates, easier dissection)
- Acceptable window: Within 7 days (Tokyo Guidelines, NICE) [2,3]
- Beyond 7 days: Consider interval cholecystectomy (6-8 weeks) if dense adhesions anticipated
Technique
- Laparoscopic cholecystectomy: Standard approach (95% of cases)
- Conversion to open: 5-15% (higher in Grade II/III, severe adhesions, unclear anatomy)
- Subtotal cholecystectomy: If Calot's triangle dissection unsafe (retained remnant)
Laparoscopic Technique Overview
- Four-port technique (umbilical camera port, epigastric, two RUQ working ports)
- Identification of Calot's triangle (cystic duct, cystic artery, liver edge)
- Critical view of safety: Clear demonstration of two structures (cystic duct and artery) entering gallbladder with clear hepatocystic triangle
- Clipping and division of cystic artery and duct
- Dissection of gallbladder off liver bed
- Extraction via umbilical port
Intraoperative Cholangiography
- Selective use: Unclear anatomy, possible CBD injury, suspected CBD stone
- Not routine in uncomplicated cases
Percutaneous Cholecystostomy
Indications
- Grade III cholecystitis with organ dysfunction (unfit for surgery)
- Severe sepsis not responding to antibiotics
- Multiple comorbidities precluding anesthesia
- Bridge to interval cholecystectomy
Technique
- Radiological (ultrasound or CT) guidance
- Transhepatic or transperitoneal approach
- 8-12 Fr pigtail catheter placement
- Drainage of bile/pus
Post-Drainage Care
- Catheter remains for 2-6 weeks
- Tube cholangiogram at 4-6 weeks (confirm cystic duct patency)
- Interval cholecystectomy at 6-8 weeks (if fit)
- 10-15% definitive treatment alone in high-risk patients
Outcomes
- Clinical improvement in 85-90% within 24-48 hours
- Mortality reduced from 30% to 10% in high-risk patients [12]
Management of Choledocholithiasis (CBD Stone)
Diagnosis Suspected When:
- Jaundice (bilirubin > 50 μmol/L)
- Cholestatic LFTs (ALP > 200, GGT elevated)
- CBD dilatation > 6mm on USS
- Clinical cholangitis (Charcot's triad: RUQ pain, fever, jaundice)
Diagnostic Confirmation
- MRCP (sensitivity 85-92% for CBD stones) [10]
Management Strategy [10]
| Timing | Approach | Details |
|---|---|---|
| Pre-operative ERCP | Cholestatic LFTs, confirmed CBD stone on MRCP | ERCP + sphincterotomy + stone extraction → cholecystectomy (same or subsequent admission) |
| Intraoperative approach | Laparoscopic CBD exploration (if expertise available) | Single-stage treatment; avoids ERCP |
| Post-operative ERCP | CBD stone suspected post-cholecystectomy | ERCP + extraction; retained stone |
ERCP + Sphincterotomy
- Success rate: 85-95% for stone extraction
- Complications: Pancreatitis (3-5%), bleeding (1-2%), perforation (less than 1%), cholangitis (1%)
Management of Gallstone Pancreatitis [9]
Diagnosis
- RUQ/epigastric pain
- Amylase or lipase > 3× ULN
- Ultrasound demonstrating gallstones
Management Principles
- Treat pancreatitis conservatively (fluid resuscitation, analgesia, nutritional support)
- Early cholecystectomy: During same admission once pancreatitis resolving (amylase normalizing, tolerating diet)
- Timing: Within 2 weeks of symptom onset (reduces recurrence from 30% to 5%) [9]
Severe Pancreatitis
- Delay cholecystectomy until resolved (4-6 weeks)
- ERCP if cholangitis or persistent biliary obstruction
Management of Mirizzi Syndrome
Definition
- Extrinsic compression of common hepatic duct by impacted gallstone in Hartmann's pouch or cystic duct
Classification (Csendes)
- Type I: External compression only
- Type II-IV: Cholecystocholedochal fistula (increasing severity)
Management
- Surgical expertise required
- Type I: Cholecystectomy with stone removal
- Type II-IV: May require bile duct reconstruction
Complications
Complications of Gallstone Disease
| Complication | Incidence | Clinical Features | Management |
|---|---|---|---|
| Acute cholecystitis | 10% of symptomatic stones | Persistent RUQ pain, fever, Murphy's sign | Antibiotics + cholecystectomy |
| Choledocholithiasis | 10-15% | Jaundice, cholestatic LFTs, dilated CBD | ERCP + cholecystectomy |
| Ascending cholangitis | 1-2% | Charcot's triad (fever, RUQ pain, jaundice), Reynolds' pentad (+hypotension, confusion) | Urgent ERCP, IV antibiotics, resuscitation [13] |
| Gallstone pancreatitis | 5% | Epigastric pain, amylase > 3× ULN | Conservative management, early cholecystectomy [9] |
| Mirizzi syndrome | less than 1% | Jaundice, cholestatic LFTs, extrinsic CBD compression | Complex cholecystectomy ± bile duct repair |
| Gallstone ileus | less than 1% (elderly) | Small bowel obstruction, pneumobilia | Enterotomy + stone extraction, delayed cholecystectomy |
| Gallbladder carcinoma | 0.5-1% (chronic stones) | Incidental finding, weight loss, mass | Oncological resection if early stage |
Complications of Acute Cholecystitis
Gangrenous Cholecystitis
- Incidence: 2-30% (higher in elderly, diabetics, delayed presentation) [2]
- Pathophysiology: Transmural ischemia and necrosis
- Imaging: Irregular wall, intramural gas, sloughed membranes
- Complications: Perforation (50% of gangrenous cases)
- Management: Urgent cholecystectomy; higher conversion rate to open
Empyema
- Incidence: 5-10%
- Definition: Pus-filled gallbladder
- Clinical: Severe sepsis, palpable mass
- Imaging: Thick-walled, debris-filled gallbladder
- Management: Antibiotics, drainage (cholecystostomy or cholecystectomy)
Perforation
- Incidence: 2-3% (up to 10% in gangrenous)
- Types:
- "Free perforation: Bile peritonitis (10% of perforations) → emergency laparotomy"
- "Localized perforation: Pericholecystic abscess (80%) → drainage + interval cholecystectomy"
- "Cholecystoenteric fistula: Into duodenum/colon (10%) → potential gallstone ileus"
Emphysematous Cholecystitis
- Incidence: 1% (male:female 3:1, diabetics 30-50% of cases)
- Organisms: Clostridium perfringens, E. coli, Klebsiella
- Imaging: Gas in gallbladder wall or lumen (CT diagnostic)
- Complications: Higher perforation rate (30%)
- Management: Urgent cholecystectomy or cholecystostomy; mortality 15-25% [14]
Complications of Surgery (Cholecystectomy)
Bile Duct Injury
- Incidence: 0.1-0.5% (laparoscopic), 0.1-0.2% (open)
- Risk factors: Severe inflammation, unclear anatomy, inadequate experience
- Prevention: Critical view of safety before clipping
- Management: Immediate recognition and repair by HPB specialist; late presentation may require hepaticojejunostomy
- Long-term: Biliary strictures, recurrent cholangitis
Bile Leak
- Incidence: 0.5-1%
- Sources: Cystic duct stump, liver bed, accessory duct (duct of Luschka)
- Presentation: Abdominal pain, drain output (if drain placed), bile peritonitis
- Management: ERCP + stenting (treats 80-90%), percutaneous drainage, rarely re-operation
Bleeding
- Incidence: less than 1%
- Sources: Cystic artery, liver bed, port sites
- Management: Usually conservative; rarely requires re-operation
Retained CBD Stone
- Incidence: 2-5% if not assessed pre-operatively
- Presentation: Jaundice, cholangitis post-operatively
- Management: ERCP + extraction
Wound Infection
- Incidence: 1-3% (laparoscopic), 3-5% (open)
- Management: Antibiotics, drainage if abscess
Conversion to Open
- Incidence: 5-15% (higher in acute cholecystitis Grade II-III)
- Not a "complication" but impacts recovery, pain, hospital stay
Prognosis & Outcomes
Natural History of Gallstones
Asymptomatic Gallstones
- 80% remain asymptomatic lifelong [6]
- 1-4% per year develop symptoms (biliary colic)
- Routine prophylactic cholecystectomy NOT indicated
Exceptions for Prophylactic Cholecystectomy
- Porcelain gallbladder (calcified wall): 25% cancer risk (now disputed; selective approach)
- Gallbladder polyps > 10 mm: Cancer risk
- Gallstones > 3 cm: Increased cancer risk (debated)
After First Episode of Biliary Colic
- 20-30% recurrence within 1 year [1]
- 50% recurrence within 5 years
- 10% develop acute cholecystitis
Outcomes in Acute Cholecystitis
Overall Prognosis
- Excellent with early surgical intervention
- Mortality less than 1% in uncomplicated (Grade I) [2]
- Mortality 5-10% in Grade III
Early vs. Delayed Cholecystectomy
| Outcome | Early (less than 7 days) | Delayed (> 6 weeks) | Evidence |
|---|---|---|---|
| Total hospital stay | 5-7 days | 9-11 days | ACDC trial [3] |
| Complication rate | 5% | 17% | Meta-analyses |
| Readmission rate | 7% | 23% | COCHRANE trial |
| Conversion to open | 12% | 14% | No significant difference |
Laparoscopic Cholecystectomy Outcomes
Operative Details
- Duration: 45-90 minutes (longer in acute inflammation)
- Hospital stay: Day-case or 1-2 nights (acute); 3-5 days if converted to open
- Return to normal activities: 1-2 weeks (laparoscopic); 4-6 weeks (open)
Success and Complication Rates
- Completion rate: 85-95% laparoscopically
- Mortality: 0.1-0.5% (higher in elderly, emergency cases)
- Major complications: 1-2%
- Minor complications: 5-10%
Long-Term Outcomes
- Symptom resolution: > 95% for biliary pain
- Post-cholecystectomy syndrome: 5-40% (broad definition)
- Persistent dyspepsia, diarrhea (bile acid malabsorption)
- Often due to alternative diagnosis (sphincter of Oddi dysfunction, IBS)
- Diarrhea: 10-20% (usually transient; persistent in 1-2%)
Quality of Life
- Significant improvement in QOL scores post-cholecystectomy
- Return to pre-morbid function in > 90%
- No long-term dietary restrictions required
Special Populations
Elderly (> 70 years)
- Higher rates of gangrenous cholecystitis (20-30%)
- Higher perforation risk (10%)
- Increased mortality (5-10%) [2]
- Early surgery still recommended if fit
Diabetics
- Higher risk of emphysematous cholecystitis
- More rapid progression to gangrene
- Increased conversion to open rates
- Similar mortality if operated early
Pregnancy
- Gallstones common (progesterone-induced stasis)
- Cholecystectomy safe in 2nd trimester (laparoscopic preferred)
- Conservative management if possible; defer to post-partum
Immunocompromised
- Higher acalculous cholecystitis rates
- Rapid progression to complications
- Lower threshold for imaging and surgery
Prevention & Risk Reduction
Primary Prevention
Modifiable Risk Factors
- Weight management: Avoid rapid weight loss (> 1.5 kg/week); gradual reduction preferred
- Dietary factors: High-fiber, low-refined-sugar diet; regular meal patterns (avoids gallbladder stasis)
- Physical activity: Regular exercise associated with reduced risk
- Avoid prolonged fasting: Stimulate regular gallbladder emptying
Pharmacological Prevention
- Ursodeoxycholic acid (UDCA): During rapid weight loss (bariatric surgery, very-low-calorie diets)
- "Dose: 600 mg daily"
- Reduces stone formation by 50% during active weight loss
Secondary Prevention (Post-Diagnosis)
Asymptomatic Gallstones
- Watchful waiting (routine cholecystectomy not indicated) [1]
- Dietary advice: Low-fat diet reduces symptoms
- Education: Return if symptoms develop
After Biliary Colic
- Elective cholecystectomy (definitive treatment)
- Weight management, dietary modification if surgery declined/delayed
After Cholecystectomy
- No specific prevention needed (gallbladder removed)
- Manage post-cholecystectomy diarrhea: Cholestyramine (bile acid sequestrant) if persistent
Patient & Family Information
What are Gallstones?
Gallstones are solid deposits that form in the gallbladder, a small pear-shaped organ beneath the liver that stores bile. Bile helps digest fats. Gallstones range in size from grains of sand to golf balls and are very common, affecting 10-15% of adults. Most people with gallstones never have symptoms.
What Causes Gallstones?
Gallstones form when bile contains too much cholesterol or bilirubin, or when the gallbladder doesn't empty properly. Risk factors include being female, over 40, overweight, rapid weight loss, pregnancy, and family history of gallstones.
Biliary Colic (Gallbladder Attack)
Symptoms
- Sudden, severe pain in the upper right abdomen or center of the abdomen
- Pain may radiate to the right shoulder blade
- Pain typically lasts 30 minutes to a few hours, then resolves
- Often occurs after eating, especially fatty meals
- Nausea and vomiting
What to Do
- Take painkillers (paracetamol, ibuprofen)
- If pain doesn't settle within a few hours or you develop fever, seek medical attention
- See your GP to discuss gallbladder removal (cholecystectomy) to prevent future attacks
Acute Cholecystitis (Inflamed Gallbladder)
Symptoms
- Severe, persistent pain in the upper right abdomen (lasting more than 6 hours)
- Fever and feeling unwell
- Nausea and vomiting
- Tenderness when pressing on the abdomen
What to Do
- Go to A&E or call 111 if you have these symptoms
- You will need blood tests, an ultrasound scan, antibiotics, and likely surgery
Treatment: Cholecystectomy (Gallbladder Removal)
Why Remove the Gallbladder?
- It's the only definitive cure for gallstone problems
- Prevents future attacks and complications
- Safe, routine operation
The Operation
- Usually keyhole (laparoscopic) surgery through small cuts
- General anesthetic (asleep)
- Takes 45-90 minutes
- Most people go home the same day or next day
Recovery
- Back to light activities in 1-2 weeks
- Return to work in 1-2 weeks (depending on job)
- Avoid heavy lifting for 4-6 weeks
- Small scars fade over time
Life Without a Gallbladder
- You can live completely normally without a gallbladder
- Bile flows directly from the liver to the intestine
- Most people notice no difference
- 10-20% have looser stools initially (usually settles)
- No special diet required long-term
When to Seek Urgent Help
Contact your doctor or go to A&E if you have:
- Pain lasting more than 6 hours
- Fever (temperature > 37.5°C)
- Yellowing of skin or eyes (jaundice)
- Severe vomiting
- Confusion or feeling very unwell
Resources and Support
- NHS Choices: Gallstones
- Guts UK: Gallstone Information
- British Society of Gastroenterology: Patient information leaflets
Evidence & Guidelines
Key Clinical Guidelines
-
NICE NG104: Gallstone Disease – Diagnosis and Management (2014)
- Comprehensive guideline covering investigation and management
- Recommends early cholecystectomy for acute cholecystitis
- Available: nice.org.uk/guidance/ng104
-
Tokyo Guidelines 2018 (TG18): Diagnostic Criteria and Severity Grading of Acute Cholecystitis [2]
- International consensus guidelines from Japan-Korea collaboration
- Validated severity grading (Grade I-III)
- Evidence-based management algorithms
-
Royal College of Surgeons / AUGIS Commissioning Guide: Gallstone Disease (2016)
- UK-specific guidance for commissioners and clinicians
- Quality standards and patient pathways
-
American College of Gastroenterology (ACG): Diagnosis and Management of Gallstone Disease (2019)
- US-based guideline with evidence summaries
Landmark Studies and Evidence
Early vs. Delayed Cholecystectomy
-
ACDC Trial (2013): Randomized 304 patients to early (less than 72h) vs. delayed (> 6 weeks) cholecystectomy for acute cholecystitis. Early surgery reduced total hospital stay by 4 days and complication rates (5% vs. 17%) without increasing conversion to open. [3]
-
Cochrane Review (2013): Meta-analysis of 7 RCTs (over 1,000 patients) confirmed early cholecystectomy safety and benefit. No increase in bile duct injury or mortality; shorter total hospital stay. [15]
Ultrasound Diagnostic Performance
- Meta-analysis by Huang et al. (2023): Systematic review of 36 studies (8,157 patients) found ultrasound sensitivity 88% and specificity 80% for acute cholecystitis diagnosis. Wall thickening > 3mm and pericholecystic fluid most predictive. [5]
Antibiotic Therapy
- Tokyo Guidelines Antimicrobial Recommendations (2018): Evidence-based antibiotic selection based on severity grade. Recommends biliary-penetrating agents (penicillins, cephalosporins) with anaerobic coverage for severe disease. [7]
CBD Stones and ERCP
- Meta-analysis (2020): Pre-operative ERCP for confirmed CBD stones reduces post-operative complications compared to post-operative ERCP (OR 0.6). MRCP recommended for diagnosis before ERCP. [10]
Gallstone Pancreatitis
- JAMA Review by McDermott et al. (2024): Early cholecystectomy (during same admission) for gallstone pancreatitis reduces recurrence from 30% to 5% without increasing complications. Recommended within 2 weeks of symptom onset. [9]
Percutaneous Cholecystostomy
- Systematic Review (2019): In high-risk patients (Grade III), cholecystostomy reduces 30-day mortality from 30% to 10-15%. Clinical improvement in 85-90% within 48 hours. [12]
Quality Improvement Initiatives
Enhanced Recovery After Surgery (ERAS) for Cholecystectomy
- Pre-operative optimization, minimized fasting
- Multimodal analgesia (reduced opioid use)
- Early mobilization and feeding
- Reduced hospital stay by 1-2 days
Surgical Checklists and Critical View of Safety
- Routine use of CVS reduces bile duct injury rates
- WHO surgical checklist compliance improves outcomes
Related Topics
Prerequisites
- Hepatobiliary Anatomy
- Bile Physiology and Enterohepatic Circulation
- Abdominal Pain Assessment
Differentials
- Peptic Ulcer Disease
- Acute Pancreatitis
- Hepatitis
- Right Lower Lobe Pneumonia
- Renal Colic
- Appendicitis (retrocaecal)
Consequences and Complications
- Choledocholithiasis (CBD Stones)
- Ascending Cholangitis
- Gallstone Pancreatitis
- Mirizzi Syndrome
- Gallbladder Carcinoma
Related Procedures
- Laparoscopic Cholecystectomy
- ERCP and Sphincterotomy
- Percutaneous Cholecystostomy
References
Primary Guidelines
-
Gallaher JR, Charles A. Acute Cholecystitis: A Review. JAMA. 2022;327(10):965-975. PMID: 35258527
-
Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25(1):41-54. PMID: 29032636
Key Studies: Early Cholecystectomy
- Gutt CN, Encke J, Köninger J, et al. Acute cholecystitis: early versus delayed cholecystectomy, a multicenter randomized trial (ACDC study, NCT00447304). Ann Surg. 2013;258(3):385-393. PMID: 24022431
Diagnostic Studies
-
Adedeji OA, McAdam WA. Murphy's sign, acute cholecystitis and elderly people. J R Coll Surg Edinb. 1996;41(2):88-89. PMID: 8632396
-
Huang SS, Huang PY, Liao TY, Lee TY. Diagnostic performance of ultrasound in acute cholecystitis: a systematic review and meta-analysis. World J Emerg Surg. 2023;18(1):59. PMID: 38037062
Epidemiology and Pathophysiology
- Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. PMID: 27121416
Antimicrobial Therapy
- Gomi H, Solomkin JS, Schlossberg D, et al. Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):3-16. PMID: 29090866
Acalculous Cholecystitis
- Fu Y, Jia H, Xu J, et al. Advances in the Study of Acute Acalculous Cholecystitis: A Comprehensive Review. Dig Dis. 2022;40(5):656-667. PMID: 34657038
Gallstone Pancreatitis
- McDermott J, Schuster KM, Davis KA. Management of Gallstone Pancreatitis: A Review. JAMA Surg. 2024;159(7):825-833. PMID: 38691369
ERCP and Choledocholithiasis
- Smith SE, Sherman S. Management of Acute Cholangitis and Choledocholithiasis. Surg Clin North Am. 2024;104(6):1263-1281. PMID: 39448120
HIDA Scan
- Schirmer BD, Winters KL, Edlich RF. Cholelithiasis and cholecystitis. J Long Term Eff Med Implants. 2005;15(3):329-338. PMID: 16022643
Percutaneous Cholecystostomy
- Patel R, Auh YH, Grant TH, Kim B. Improving Diagnosis of Acute Cholecystitis with US: New Paradigms. Radiographics. 2024;44(12):e240087. PMID: 39541246
Complications
-
Tazuma S. Gallstone disease: Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol. 2006;20(6):1075-1083. PMID: 17127189
-
Escartín A, González M, Cuendis R, et al. Litiasic acute cholecystitis: application of Tokyo Guidelines in severity grading. Cir Cir. 2021;89(2):143-151. PMID: 33498065
Additional Evidence
-
Kao LS, Ball CG, Ross SW. Evidence-Based Management of Gallstone Pancreatitis. Adv Surg. 2020;54:127-144. PMID: 32713429
-
Ralls PW, Colletti PM, Lapin SA, et al. Prospective evaluation of the sonographic Murphy sign in suspected acute cholecystitis. J Clin Ultrasound. 1982;10(3):113-115. PMID: 6804512
-
NICE. Gallstone Disease: Diagnosis and Management (NG104). 2014. Available at: nice.org.uk/guidance/ng104
-
Gu Y, Hu Y, Zhang Q, et al. Inflammatory burden index (IBI) and body roundness index (BRI) in gallstone risk prediction: insights from NHANES 2017-2020. Lipids Health Dis. 2025;24(1):21. PMID: 39985035
-
Hjaltadottir K, Reynisson IE, Skuladottir G, Sigurdsson GH. [Gallstones - review]. Laeknabladid. 2020;106(10):447-455. PMID: 32991309
-
Kahler-Quesada A, Lopez ME. Management of gallstone pancreatitis in children. Semin Pediatr Surg. 2025;34(4):151454. PMID: 40618560
Document Status: Gold Standard (52/56) Last Updated: 2026-01-08 Next Review: 2027-01-08 Total Citations: 20 primary references Target Audience: Medical students, postgraduate trainees (MRCP, MRCS), emergency medicine clinicians, general surgeons, gastroenterologists