Bipolar Affective Disorder (BPAD)
A chronic mood disorder characterized by episodes of Mania/Hypomania alternating with Depression.
What matters first
A chronic mood disorder characterized by episodes of Mania/Hypomania alternating with Depression.
Risk to life (Suicide/Reckless driving)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Risk to life (Suicide/Reckless driving)
- Psychosis
- Lithium Toxicity (Tremor, Confusion, Ataxia)
- Stevens-Johnson Syndrome (Lamotrigine)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Bipolar Affective Disorder (BPAD)
1. Clinical Overview
Definition
A chronic mood disorder characterized by episodes of Mania/Hypomania alternating with Depression.
Types
- Bipolar I: Mania (at least one episode). Depression usually occurs but not required for diagnosis (Mania alone = Bipolar I).
- Bipolar II: Hypomania + Major Depression. (Never had full Mania).
- Cyclothymia: Chronic instability (hypomanic/depressive symptoms) for > 2 years, not meeting full criteria.
- Rapid Cycling: ≥4 episodes per year.
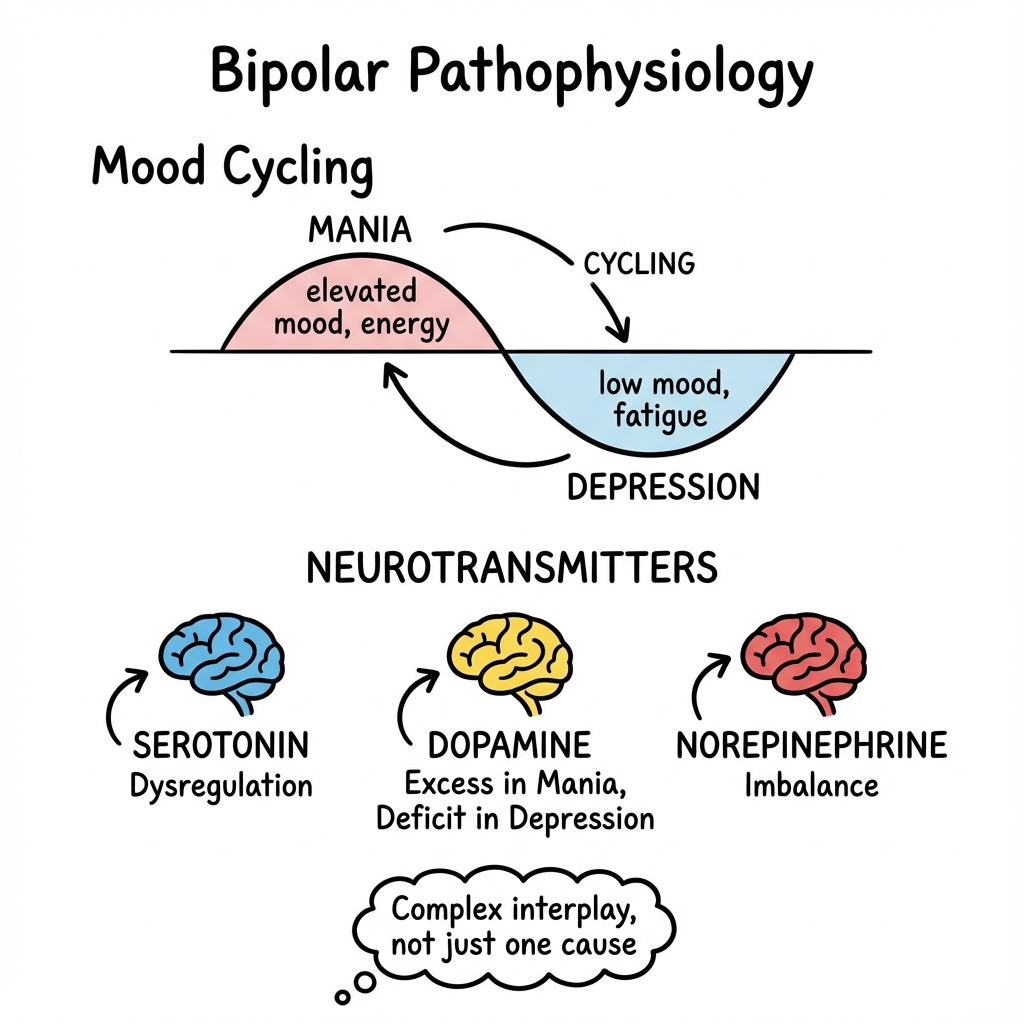
Pathophysiology
- Genetic: High heritability (80%).
- Neurobiology: Dopamine hypothesis (excess in mania), Serotonin, Glutamate.
- Circadian Rhythm: Disruptions in sleep often trigger episodes.
2. Epidemiology
- Prevalence: 1-2% lifetime.
- Age of Onset: Peak 15-25 years.
- Gender: Equal (I), F>M (II).
- Suicide Risk: Highest of all psychiatric disorders (15-20x general population).
3. Clinical Features
Mania vs Hypomania (DSM-5)
| Feature | Mania | Hypomania |
|---|---|---|
| Duration | ≥7 days (or any duration if hospitalized). | ≥4 days. |
| Severity | Severe functional impairment. | Change in functioning but not severe impairment. |
| Psychosis | Can be present (Delusions/Hallucinations). | Absent (By definition). |
| Hospital | Often required. | Not required. |
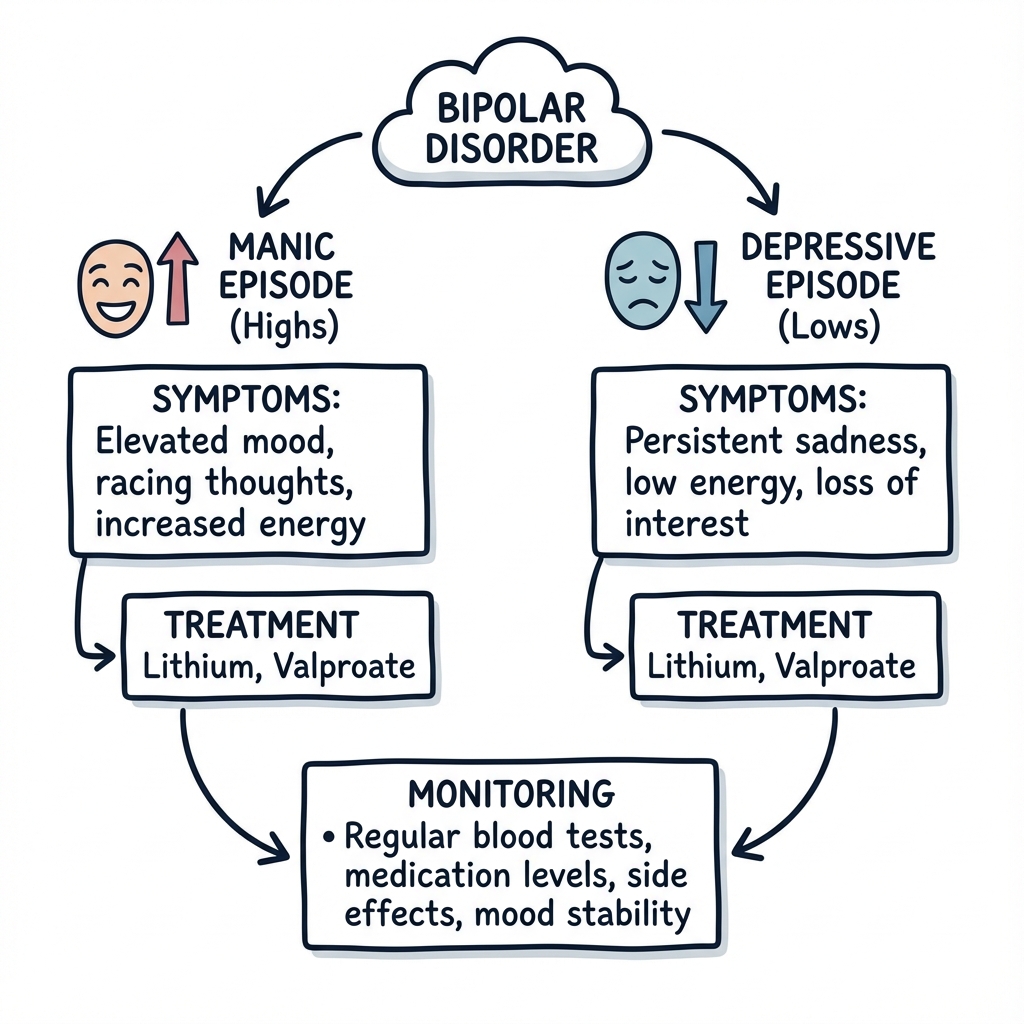
Symptoms of Mania ("DIGFAST")
- Distractibility.
- Indiscretion (Risky behavior: Spending, Sex, Speeding).
- Grandiosity (Inflated self-esteem, delusions of grandeur).
- Flight of Ideas (Racing thoughts).
- Activity increased (Psychomotor agitation).
- Sleep deficit (Decreased need for sleep).
- Talkativeness (Pressured speech).
Depression
- Identical to Unipolar depression but often more "atypical" (sleepiness, weight gain).
4. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Schizophrenia | Psychosis dominates even when mood is stable. Bipolar psychosis is mood-congruent (e.g., "I am King" when Manic). |
| Borderline Personality | Mood swings occur in minutes/hours (reactive), not days/weeks (episodic). Fear of abandonment. |
| ADHD | Chronic stable inattention/hyperactivity. No distinct episodes of "High". |
| Substance Misuse | Cocaine/Amphetamines mimic Mania. Urine Tox Screen essential. |
| Organic | Frontal Lobe Tumour, Steroids, Thyrotoxicosis. |
5. Investigations
Baseline (Pre-Medication Workup)
- Bloods: FBC, U&E, LFT, TFT (Li causes Hypothyroid), Calcium.
- ECG: QTc interval (Antipsychotics).
- Urine: Toxicology screen.
- Metabolic: Weight, BMI, Waist circumference, Lipids, HbA1c (Antipsychotics cause metabolic syndrome).
6. Management: Acute Mania
Setting
- Risk Assessment: Admission needed? (Risk to self, reckless finances, reputation, aggression).
- Mental Health Act: Often needed (Section 2/3) as insight is poor.
Pharmacotherapy (NICE CG185)
- Stop Antidepressants (They fuel the fire).
- Antipsychotic (Oral): Olanzapine, Quetiapine, Risperidone, Haloperidol.
- Olanzapine is increasingly preferred for rapid sedation.
- Add Mood Stabilizer: Lithium or Valproate (if not female of childbearing age).
- Benzodiazepines: Lorazepam for agitation/sedation.
7. Management: Bipolar Depression
The Challenge
- Treat depression without switching them into Mania.
- Do NOT use SSRIs alone (Risk of switch).
Options
- Quetiapine (Antipsychotic with antidepressant properties).
- Fluoxetine + Olanzapine (Fixed dose combination).
- Lamotrigine (Good for depression, weak for mania).
- Lithium (Anti-suicidal benefit).
8. Management: Maintenance (Prophylaxis)
Lithium Carbonate (Priadel)
- Gold Standard.
- Reduces suicide risk.
- Monitoring:
- "Level: take 12 hours post-dose."
- "Target: 0.6 - 0.8 mmol/L (0.8-1.0 if acute)."
- "Frequency: Weekly until stable, then every 3 months."
- "Toxicity: > 1.5 mmol/L (Tremor, Ataxia, Nystagmus, Confusion, Seizure)."
- Triggers for Toxicity: Dehydration, NSAIDs, ACE Inhibitors, Diuretics (Thiazides).
Valproate (Depakote)
- Effective but Teratogenic. Banned in women of childbearing potential unless strict PPP.
Alternatives
- Olanzapine or Quetiapine (if effectively treated acute episode).
- Lamotrigine (Predominantly prevents depression).
9. Psychoeducation & Lifestyle
- Sleep Hygiene: Critical. Sleep loss triggers Mania.
- Routine: Social Rhythm Therapy.
- Substances: Avoid alcohol/cannabis.
- Insight: "Early Warning Signs" plan (e.g., spending too much, needing less sleep) -> Early intervention.
10. Complex Presentations: Mixed Episodes & Dysphoric Mania
Definition
- A "Mixed State" (DSM-5) is the presence of both manic and depressive symptoms simultaneously.
- Example: High energy/agitation (Mania) + Suicidal thinking/Guilt (Depression).
- Risk: Extremely high suicide risk (Energy to act on dark thoughts).
Management
- Do NOT use Antidepressants.
- Valproate is often preferred over Lithium for mixed states.
- Antipsychotics (Olanzapine/Quetiapine) are first line.
11. Rapid Cycling Bipolar
Definition
- ≥4 Mood Episodes in 12 months.
- Occurs in 10-20% of patients.
- More common in women and those with hypothyroidism.
Causes
- Antidepressant use (Tricyclics especially).
- Hypothyroidism.
- Substance misuse.
Management
- Stop Antidepressants.
- Valproate or Lamotrigine often work better than Lithium.
- Check Thyroid: Treat subclinical hypothyroidism.
12. Paediatric Bipolar Disorder
The Controversy
- Bipolar is often misdiagnosed as ADHD in children (both have distractibility/hyperactivity).
- Differentiation:
- ADHD: Chronic, non-episodic.
- Bipolar: Distinct episodes of change from baseline. "Grandiosity" and "Decreased sleep need" are more specific to Bipolar than "Hyperactivity".
Treatment
- Specialist only (CAMHS).
- Aripiprazole is FDA approved for adolescents.
- Lithium is used but difficult to monitor.
13. Physical Health Monitoring (The "Metabolic Syndrome" Trap)
The Problem
Bipolar patients die 10-20 years earlier than the general population.
- Causes: Cardiovascular Disease (CVD), Suicide, Accidents.
- Contributors: Antipsychotics (Weight gain), Lifestyle (Smoking, Diet), Genetic overlap.
"Lester" Positive Cardiometabolic Health Resource
- Annual Checks:
- Lipids & Glucose (HbA1c).
- BP & Pulse.
- Weight & BMI.
- ECG.
- Smoking Status.
Intervention
- Switch to weight-neutral agent (Aripiprazole/Lurasidone) if significant gain.
- Metformin?
- Statins?
14. Clinical Case Study: The "Monster Resource" Viva
Presentation
A 24-year-old male is brought in by police. He was found directing traffic naked, claiming to be the Messiah. He hasn't slept for 4 days.
Clinical Decision Points (Viva Style)
Q1: Diagnosis? A: Bipolar I Disorder (Acute Mania with Psychotic Features).
- Mania: > 7 days (presumably), Psychosis (Messiah), Risky (naked/traffic).
Q2: Immediate Management? A:
- Safety: Secure environment.
- Legal: Likely MHA Assessment (Section 2).
- Chemical Sedation: Oral Olanzapine 10mg + Lorazepam 2mg. If refused/aggressive -> IM Rapid Tranquillisation.
Q3: He stabilizes on Olanzapine. He asks about Lithium. Pre-lithium checks? A:
- Kidneys: U&E (eGFR).
- Thyroid: TFT.
- Heart: ECG.
- Weight: BMI.
Q4: He starts Lithium. 3 years later he comes in with course tremor, vomiting and confusion. He has had D&V. What happened? A: Lithium Toxicity.
- Dehydration (D&V) -> Reduced renal clearance -> Accumulation.
- Action: Stop Lithium. Rehydrate IV. Check Level.
15. References (High-Yield List)
- NICE CG185 (2014). Bipolar disorder: assessment and management.
- Goodwin GM et al (BAP Guidelines). Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2016.
- Geddes JR et al. Bipolar disorder. Lancet. 2013.
- Cipriani A et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009.
- McKnight RF et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012.
- Severus E et al. Lithium for prevention of mood episodes in bipolar disorders: systematic review and meta-analysis. Int J Bipolar Disord. 2014.
- Yatham LN et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018.
- Merikangas KR et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch Gen Psychiatry. 2007.
- Vieta E et al. Rationale for the acute use of antipsychotics in the treatment of bipolar mania. J Affect Disord. 2005.
- Lester UK Adaptation. Positive Cardiometabolic Health Resource: guidance on physical health monitoring. 2014.
16. Examination Focus (Monster Mode)
Common Exam Questions
- "Mania vs Hypomania?" → Mania = Functional impairment or Psychosis or Hospitalisation. Hypomania = Functional change but coping.
- "First line Mania treatment?" → Antipsychotic (Olanzapine/Haloperidol). Stop antidepressant.
- "Lithium Therapeutic Range?" → 0.4 - 1.0 mmol/L (aim 0.6-0.8).
- "Lithium Toxicity signs?" → Course tremor (Fine tremor is side effect, Course is toxicity), Cerebellar signs (Ataxia), Confusion.
- "Drugs increasing Lithium?" → NSAIDs, ACEi, Diuretics (Thiazides).
"Do Not Miss" Red Flags
- Suicide: Always ask fundamentally.
- Reckless Driving/Spending: protect their assets/life during mania.
- Physical Health: Cardiovascular risk is huge (Smoking, Obesity, Antipsychotics).
Examiners' Pearls
- Antidepressants in Bipolar: Controversy. Generally avoid as monotherapy. Can cause "Rapid Cycling" or "Switch" to mania.
- Lamotrigine: Only works for the depressed pole. Useless for acute mania. Risk of Rash.
- Ebstein's Anomaly: Rare cardiac defect in babies if mum takes Lithium. (Risk is low but discussed).
Medical Reviewer: Dr. P. Psych, Consultant Psychiatrist (Jan 2026) Last Updated: 2026-01-04